
Abstract
Botulinum toxin A is produced by anaerobic spore-forming bacteria and is used for various therapeutic and cosmetic purposes. Botulinum toxin A injections are the most popular nonsurgical procedure worldwide. Despite an increased demand for botulinum toxin A injections, the clinical pharmacology and differences in formulation of commonly available products are poorly understood. The various products available in the market are unique and vary in terms of units, chemical properties, biological activities, and weight, and are therefore not interchangeable. For safe clinical practice and to achieve optimal results, the practitioners need to understand the clinical issues of potency, conversion ratio, and safety issues (toxin spread and immunogenicity). In this paper, the basic clinical pharmacology of botulinum toxin A and differences between onabotulinum toxin A, abobotulinum toxin A, and incobotulinum toxin A are discussed.
Video abstract
Point your SmartPhone at the code above. If you have a QR code reader the video abstract will appear. Or use:
Introduction
Botulinum toxin is produced by the anaerobic spore-forming bacteria of the genus Clostridium. It consists of a complex mixture of proteins containing botulinum neurotoxin (BoNT) and several nontoxic proteins. BoNTs are the most potent toxins known to mankind and can cause botulism.Citation1 There are eight distinct BoNT serotypes (A–G) produced by different strains of Clostridium botulinum.Citation2,Citation3 The human nervous system is susceptible to BoNT-A, B, C, E, F, and G and unaffected by D.Citation1,Citation4–Citation6 Recent advances have resulted in the discovery of genes encoding for many new BoNTs that may be grouped within an existing serotype but with various amino acid sequences. In addition, there are some chimeric BoNTs, for example, BoNT-DC. All serotypes have a similar molecular architecture.Citation7 Only serotypes A and B are widely used for clinical applications as their effect is longer lasting than other serotypes.Citation8 BoNTs differ with each other in terms of protein size of the neurotoxin complex, the amount of neurotoxin in the activated or nicked form, potency, and intracellular protein target. These properties vary among different preparations of the same serotype.Citation9
BoNTs enter peripheral cholinergic nerve terminals where they cleave one or two of the three core proteins of the neuroexocytosis apparatus. This results in temporary and reversible inhibition of neurotransmitter release.Citation10 Paresis occurs 2–5 days after injection, reaches its maximal point at 5–6 weeks, and lasts for approximately 2–3 months.Citation8,Citation11 BoNT seems to be preferentially taken up by hyperactive nerve terminals. Nerve stimulation has been reported to increase the rapidity of BoNT poisoning.Citation10 The recovery of muscle contraction happens gradually and in two stages:Citation12
Stage 1 involves the return of exocytosis: reappearance of vesicle turnover in the sprouts and functional recovery of the neurones
Stage 2 involves the return of the vesicle turnover in the original terminals and regression of the sprouts.
The initial functional recovery is mediated by the terminal sprouts followed by reestablishment of the original terminals.Citation12 Rogozhin et al reported that the new synaptic contacts play a relatively minor role in functional recovery. The original neuromuscular junction is reported to play a more significant role than previously thought.Citation13
The specificity of action of BoNT has made this neurotoxin a useful therapeutic agent. The range of clinical application of BoNT is vast and fast growing with some of the clinical uses summarized in . BoNT-A is extensively used for aesthetic purposes worldwide and has been shown to have direct analgesic effects, mediated through blockade of substance P, glutamate, and calcitonin gene-related peptide.Citation11 The basis of popular use of BoNT is its potency, neurospecificity, and complete reversibility.Citation10
Table 1 Some of the clinical uses of botulinum toxin A
BoNT-A formulations
There are several BoNT-A-containing products available on the market, and they vary in terms of the following:Citation1,Citation8,Citation14
Composition
Amount of neurotoxin
Units
Toxin complex size
Molecular weight
Chemical properties
Biological activity
pH
Storage
Risk of antigenicity
Indication of use
Geographic distribution.
The three botulinum toxin formulations that have been approved by the US Food and Drug Administration and are well known in the Western hemisphere are as follows:
Onabotulinum toxin A (ONA; Botox®/Vistabel®; Allergan Inc., Dublin, Ireland)
Abobotulinum toxin A (ABO; Dysport®/Azzalure®; Ipsen, Paris, France/Galderma, Lausanne, Switzerland)
Incobotulinum toxin A (INCO; Xeomin®/Bocouture®, NT 201; Merz Pharmaceuticals GmbH, Frankfurt, Germany)
Each of these products are approved for various and limited indications in various countries. However, companies are evolving, and approved indications in various countries are constantly changing. Despite having similar efficacies, there is an ongoing debate regarding the comparability of these various preparations.Citation3 Each of these neurotoxins is formulated differently, has a different manufacturing process, and demonstrates unique characteristics, and subsequently, these products are not interchangeable ().Citation15 For safe clinical practice and achieving optimal results for a given indication, the practitioners need to understand the clinical issues of potency, conversion ratio, and safety (toxin spread and immunogenicity). A correct and optimal treatment plan and procedure requires an in-depth knowledge of the product(s) used, anatomy, and injection technique.Citation8
Table 2 Properties of different therapeutic botulinum toxin preparationsCitation5,Citation58,Citation59,Citation114,Citation123,Citation124
The effect of BoNT depends on the administered location, concentration, and volume which are in turn relative to the location, depth, and size of the target muscle.Citation1 Numerous published studies compare the characteristics of these products. However, when reviewing the literature on efficacy, diffusion, and spread of various products and in comparison to each other, it is important to take into consideration all the possible contributing factors including the following:Citation16
Intrinsic properties of the toxins available
◦ Protein load
Muscle selection
◦ Muscle activity pattern
◦ Muscle architecture
◦ Fascial planes
Injection technique
◦ Dilutions
◦ Volumes
◦ Doses.
Molecular architecture
BoNT-A is synthesized as macromolecular protein complexes in nature.Citation9 The progenitor toxins are known as protein complexes and consist of nontoxic accessory proteins (NAPs). The BoNT-A protein has a molecular weight of 150 kDa, and the NAP is associated to this active neurotoxin. The NAP composition of different products varies.Citation3
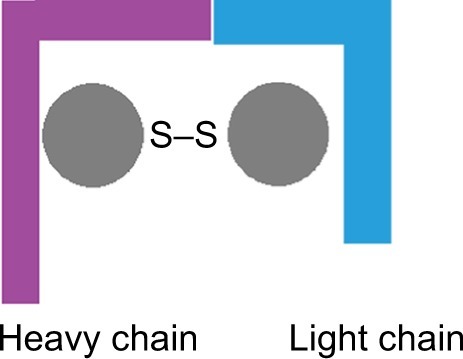
There is amino acid sequence variability and immunogenic differences between various serotypes. However, they all have a similar molecular structure and architecture. The BoNTs are produced as a single-chain polypeptide (150 kDa) that is inactive. Proteases nick the polypeptide chain resulting in a toxin that is pharmacologically active and consists of two chains: a heavy chain (100 kDa) and a light chain (50 kDa) connected together by a disulfide bond. In addition, there are noncovalent interactions, and the N terminus of the heavy chain encircles the globular light domain.Citation7,Citation17,Citation18 The heavy chain has two 50 kDa domains with two terminal parts, the amino- and the carboxy-terminal parts.Citation7 Each of these chains has different functions in the mechanism of action of the neurotoxin ().Citation19 The single disulfide bridge and its integrity play an integral role in biological activity of BoNT, making it highly fragile to various environmental variations and influences.Citation20
Figure 1 Botulinum neurotoxin consists of two amino acid chains connected by a disulfide bridge: a heavy amino acid chain with a molecular weight of 100 kDa and a light amino acid chain with a molecular weight of 50 kDa.Citation20
Composition
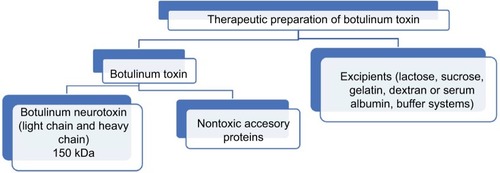
The therapeutic preparations of botulinum toxin consist of the following ():Citation8,Citation20
BoNT
NAPs
Excipients (lactose, sucrose, gelatin, dextran or serum albumin [for stabilization], buffer systems [for pH calibration]).
Figure 2 Simplified contents of therapeutic botulinum toxin preparations.
It has been reported that in all mentioned products (ONA, ABO, INCO), the neurotoxin is derived from the identical Hall strain of C. botulinum type A.Citation21,Citation22 However, there is evidence that Hall strains are different to each other, and the strain information for the products apart from ONA (Allergan Botox®) is unknown.Citation23–Citation25
The molecular weight of the BoNT-A progenitor toxins varies between 300 and 900 kDa. This weight variation depends on the composition of NAPs and the manufacturing process.Citation20 INCO contains only the 150 kDa neurotoxin and does not include complexing proteins.Citation20,Citation21 The 150 kDa neurotoxin is part of a complex with other proteins (complexing proteins) in ONA and ABO.Citation21 ONA is composed of a 900 kDa complex,Citation26 and the size of the ABO complex is unknown.Citation27
After dilution, drying, and reconstitution of the product, the neurotoxin rapidly dissociates from the complexing proteins. As such, it has been debated that molecular weight (protein complex size) does not influence the biological activity and pharmacological properties of BoNT.Citation28,Citation29 Complexing proteins do not contribute toward diffusion properties, seem not to contribute to the therapeutic effect, and are not required for the stabilization of the neurotoxin in the pharmaceutical formulation.Citation30 However, more studies are required to assess if the complexing proteins increase formation of antibodies against botulinum toxin type A.
Mode of action, pharmacology, and clinical assessment
The mechanism of action of BoNT on the nerve terminals can be summarized into five main steps: 1) binding of the BoNT to the peripheral cholinergic nerve terminals with high affinity and specificity, 2) internalization of the BoNT, 3) translocation (the light chain is translocated across the vesicle membrane), 4) release of the light chain and dissociation of the disulfide bond, and 5) cleavage of the SNARE proteins (the light chain cleaves SNAP-25) resulting in blockade of neurotransmitter release and therefore neuroparalysis.Citation2,Citation7,Citation31 This inhibits synaptic exocytosis and incapacitates neural transmission resulting in blockage of the release of acetylcholine at the neuromuscular junction and hence blocking the muscle contraction.Citation32
BoNT-elicited inhibition of neuroexocytosis depends on various factors including the toxin serotype, dose used, type of cholinergic nerve terminal affected, and also the animal species.Citation10,Citation33 Size of the denervation field of BoNT is determined by dose and volume of the solution injection. Clinical observation, wrinkle severity scales, area of anhidrotic effect, and electromyography evaluations are some of the methods used to examine the size of denervation field of different products. However, when evaluating such studies, the difference between the potency and dose equivalences of different preparations should be taken into consideration. Shaari and Sanders reported that in comparison to volume, the dose injected was a stronger predictor of area of paralysis.Citation34 The proximity of the injections to the motor end plates plays a key role.Citation34
Direct and indirect effects
BoNT has been reported to have direct and indirect effects. The direct effects include inhibition or blockage of the cholinergic neuromuscular or the cholinergic autonomic innervation of exocrine glands and smooth muscles.Citation20 Presence of BoNT in the peripheral blood at measurable levels, after intramuscular or intradermal injection at the recommended doses, is not expected and has not been reported.Citation8 The indirect effects include effects on the central nervous system such as the following:Citation11
Reflex inhibition
Normalization of reciprocal inhibition
Intracortical inhibition
Somatosensory evoked potentials.
The long-distance effects of BoNT do not happen by passive spread, but by an active retroaxonal transport.Citation35,Citation36 BoNT-A can retrotransport to the central nervous system. This was studied by tracing the cleavage of the SNARE proteins within the central nervous system neurons post peripheral injection of BoNT.Citation35,Citation37–Citation39 Retrograde transport of BoNT-A has been reported via sensory neurons.Citation36 There is evidence for antinociceptive activity of BoNT-A; however, no other associated symptoms due to BoNT acting within the central nervous system post peripheral injection have been reported.Citation39,Citation40 The direct and indirect effects are advantageous depending on the purpose of administration and the injection target. For example, the central action can contribute to functional improvements in spastic gait and can be beneficial in pain management.Citation39
Duration of action
The duration of persistence of the clinical results (eg, elimination of the wrinkles) is one of the key measures for BoNT efficacy. This has been reported to have significant influence on patient satisfaction in cosmetic patients and may be related to individual patient’s genetics and the target muscle (mass, size, thickness, and depth below the skin and structure).Citation41,Citation42 The specific administered dose of BoNT influences the efficacy and duration of effect.Citation43
The methods for assessment of onset of action in the clinic are not universal or fully validated and rely on reduced or diminished muscle activity assessed by the practitioner or reported by the patient. The onset of effect is different for different formulations. There is lack of consensus in the literature on the reason for this.Citation44
Studying and understanding the onset of action requires further comprehension and needs to be clearly defined. Onset of action of BoNT could be explained on a molecular level or as the presentation of the molecular events that take place (the biological effects). On a molecular level, the onset of action happens as soon as BoNT is injected into the muscle:Citation45,Citation46
Resides in the extracellular space (toxin uptake only takes place by the nerve terminals at the endplate)
◦ In the muscle for a short time (minutes or at most a few hours) and the uptake is rapid
◦ Binds to the surface of plasma membranes
Receptor-mediated endocytosis
pH-induced translocation across the endosome membrane
In the presynaptic terminal, cleavage of the SNARE proteins (SNAP-25) – essential for exocytosis
Blockade of transmitter release
Paralysis.
As such, the time taken for the toxin to be taken up and the time for the clinical response to become evident differ considerably.Citation45
When discussing the time interval of onset to response, it is once again important to explain what is meant by “response”:
Partial elimination of the lines and wrinkles/reduced lines and wrinkles
Complete elimination of the lines and wrinkles
Agonist muscle(s) action affected
Antagonist muscle action affected
The desired balance between the agonist and antagonist muscles achieved.
The mentioned events happen at different times and may not be fully achieved by the time patients are reviewed after injections which is normally in 7–14 days after injections.
Paresis occurs after 2–5 days post injection of BoNT into a striate muscle. This effect lasts 2–3 months before wearing off gradually as the original nerve terminals recover.Citation11,Citation13 Three studies conducted with ONA reported mean or median duration of effect for various doses to be approximately 4.5 months.Citation47 Examination of the literature has shown that patients treated with BoNT-A for aesthetic purposes can expect their results to last at least 3 months. However, the results can last 4–5 months depending on the area treated, the dose, and the formulation used.Citation48 Although the mechanism is not fully understood, the results may last longer for some patients, especially after repeated treatment.Citation49–Citation51 Muscle atrophy and reduced number of BoNT-A targets available are thought to be related to the prolonged effect.Citation44 Dolly and Aoki reported that there is no atrophy of the nerve endings upon blockade of neurotransmitter.Citation52 Rogozhin et al reported that repeated exposure to BoNT-A results in delayed restoration of neuromuscular transmission back to normal. In addition, it results in profound abnormalities in the structure of the neuromuscular junction and the intramuscular nerve.Citation13
In a randomized, double-blind study, Rappl et al reported that in female subjects, the onset of treatment effect happened earlier and the treatment effect duration was longer when a similar dose was applied. In their study, the onset of treatment effect was seen earlier in both sexes for INCO compared to ONA and ABO. The duration of treatment effect (the time taken for the glabellar muscle activity to return to the baseline level) was reported to be longer for INCO in comparison to the other two products.Citation53 Glogau et al studied duration of effect of aesthetic treatments with BoNT using data obtained from four Phase III clinical trials with similar designs and a total of 625 subjects treated with ONA. They reported that there was sustained clinical effect for 4 months (in more than 50% of subjects) after treatment of glabellar lines with 20 units of ONA.Citation54
Poor response to the treatment could be due to insufficient or incorrect dosing, errors in drug handling during preparation or storage or administration, and anatomical variations.Citation44
Dose–effect correlation
The extent of provoked paresis is correlated to the amount of BoNT administered. Dressler and Rothwell studied the relationship between the dose of BoNT-A and induced reduction of the maximal electromyographic amplitude in the sternocleidomastoid muscle. They reported a dose–effect relationship.Citation55 In a prospective multicenter placebo-controlled double-blind dose-ranging study, Poewe et al reported that higher doses of ABO resulted in greater magnitude and duration of improvement in patients with rotational torticollis. They recommended lower starting does as higher doses used resulted in significantly more adverse events.Citation56 Dressler et al reported that relatively low BoNT doses produce substantial paresis.Citation11 The dose–effect correlation can be used for optimization of BoNT treatment.Citation11,Citation55
Dose–duration correlation
Duration of effect of treatments is an important factor as it influences treatment intervals and determines patient satisfaction to some extent.Citation57 When lower doses of BoNT are used, the duration of its action is correlated to the amount injected. However, the duration of action is thought to saturate on approximately 3 months when higher BoNT doses are used.Citation11 Carruthers and Carruthers, in a prospective, double-blind, randomized, parallel-group, dose-ranging study, reported that the higher doses of BoNT were more effective (duration, peak response rate, improvement from baseline) in reducing glabellar lines in men. A dose-dependent increase was reported in the duration of effect, as well as the response rate at maximum frown with no increase in incidence of adverse effects. They also reported that their participants reported a dose-dependent reduction in frowning, and enhanced feelings of attractiveness, confidence, and satisfaction.Citation43 In another study, Carruthers et al reported that lower units of BoNT-A (10 units) were less effective than higher doses in treating glabellar rhytids and the relapse rate was significantly higher at 4 months.Citation58
Muscle atrophy
BoNT induces paresis of striate muscle which in turn produces muscle atrophy and reduction of the diameter of the target muscle.Citation11 Muscle atrophy caused by BoNT injection can be the aim of the treatment and hence a desirable effect or an unintended and undesirable effect. Injection of masseter muscles to reduce the appearance of square lower face and for facial contouring is highly prevalent is Asia.Citation59–Citation61 Evident reduction in size of masseter muscles has been reported in as little as 2 weeks, with maximal reduction in approximately 6–8 weeks.Citation62 The “hourglass deformity” due to temporalis atrophy caused by repeated treatment of BoNT-A was described by Guyuron et al in patients treated for migraine and reported to resolve in all patients several months after recovery of muscle function.Citation63
Potency
The biological potency of BoNT formulations is based on the median lethal dose of the neurotoxin after intraperitoneal injection in female Swiss-Webster mice and is also known as median lethal dose (LD50) assay. Potency used to be explained by the quantity of toxin required to achieve a median lethal dose (LD50) unit. Therefore, 1 unit of toxin (1 mouse LD50) is the dose of toxin or neurotoxin that can kill 50% of a group of mice. During the production process, potency and stability testings are required at several stages, and at the final stage, a large number of animals are used. A cell-based potency assay is a new modality for assessment of units in BoNTA and has resulted in elimination of the LD50 assay in some laboratories.Citation64 This method uses a specific cell line and can carry out evaluation of all four phases of botulinum toxin action (binding, internalization, translocation, and SNAP-25 cleavage). This method is superior as it reduces the need for animal testing, has been successfully cross-validated with the LD50 assay, and is appropriate to be used in a high-capacity and in a highly quality-controlled environment.Citation8 In addition, it has been reported to be more accurate and reproducible.Citation65 Allergan Inc. (produces ONA) has developed a cell-based potency assay for potency testing, which has received regulatory approval.Citation65,Citation66 In 2014, Merz Pharmaceuticals GmbH (produces INCO) also completed the validation of cell culture-based assay for INCO.Citation67
The dose of product for treating patients is determined by each manufacturer’s result of LD50 or cell-based potency assay. This is dependent on multiple variables including mouse strain, sex, age, volume, route of injection, time of examination after injection, delivery vehicle, and reconstituting buffer. These are not standardized across manufacturers.Citation3 The standards and in-house diluents for these LD50 potency assays are different for each manufacturer, and therefore, the unit of measurement for the three commercially available BoNT-A preparations is proprietary to each manufacturer. As such, the direct comparisons of potency between products are not valid.Citation23,Citation29,Citation67–Citation70 The specific potency explained as the potency per unit weight of toxin protein means the level of protein administered per injection.Citation25
The toxin moiety (the 150 kDa neurotoxin) is the same in all abovementioned pharmaceutical preparations. Potency of a product depends on the amount of active toxin available.Citation3 In order for the neurotoxin to be activated, the single-chain 150 kDa neurotoxin must be cleaved into a dichain molecule which must dissociate from the NAPs. Apart from INCO, all commercially available formulations are composed of the 150 kDa neurotoxin with NAPs.Citation3 The molecular weight of the BoNT-A progenitor toxins varies (300–900 kDa) depending on the composition of NAPs and the manufacturing process.Citation20 From a clinical point of view, this means that the potency and therapeutic profiles can be affected by different forms of the complex despite the same active molecule.Citation3
Reconstitution
All the above products are in powder form and need to be reconstituted prior to application. There is debate with regard to reconstitution with normal saline with no preservatives and preserved (0.9% benzyl alcohol) saline. The manufacturer’s suggested diluent is normal saline with no preservatives. Several authors have reported equivalent clinical effectiveness with BoNT-A diluted with preserved saline. However, there is a debate on whether the preservatives in the saline deactivate the toxin partially.Citation71,Citation72 Alam et al, in a double-blind, randomized controlled trial, reported that preserved saline containing benzyl alcohol used in reconstitution of ONA did not affect its potency or clinical outcome and made the injections less painful.Citation73 This was confirmed by two other studies.Citation74,Citation75
It has been traditionally believed that shaking, bubbling, and storing the vial for a long period of time reduces the efficacy of BoNT. However, a few clinical studies have contradicted this. Trindade De Almeida et al compared muscle paralysis in a split-face study. They injected gently reconstituted ONA without foam formation on one side of the face and rapidly reconstituted ONA with foam formation “with as many bubbles as possible” on the other side. They reported that the potency and the short- or long-term effects of the product were not affected by foaming during the reconstitution process.Citation76 This was supported by a prospective, double-blinded, randomized study carried out by Kazim and Black who used a Vortex Touch Model 232 at maximum speed for 30 seconds (vigorous reconstitution of ONA).Citation77 The 2004 consensus panel has reported that the fragility of BoNT-A is not as previously reported.Citation78 It is now understood that a lot of the precautions, mainly recommended by the manufacturers, are “too restrictive”. Studies and the literature show that BoNT may be less fragile and more resistant to degradation than previously thought.Citation79
It is paramount to remember that suboptimal reconstitution of BoNT preparations can reduce or diminish their efficacy.Citation80,Citation81 Inaccurate reconstitution could result in inaccuracy of actual units injected and therefore compromised treatment.Citation80
Niamtu has shown that conventional methods of reconstitution can result in an average loss of 5 units.Citation81 The size of needle plays a key role in loss of volume/units of product. A 30 G needle results in loss of 0.03 mL of the product in the dead space. Use of no dead space needles could ensure minimal to no loss of solution. In addition, new devices/syringes (eg, 3Dose Vlow Medical) with a triangular plunger help reduce/eliminate loss of solution and are easy to use and read number of units for different dilutions.
Use of fixed needles to syringes is less advisable. Upon drawing the product into the syringe, the needle goes through the silicone rubber stopper; hence, the needle becomes blunt, injections might be more painful, and there will be molecules of silicone in the needle. The silicone molecules will end up as foreign bodies in the muscle or skin. In addition, some insulin syringes have a silicone-coated needle.Citation82 There has been reported cases of silicone granulomas and siliconoma with acupuncture needles and in diabetic patients due to repeated use of silicone oil-coated needles.Citation83–Citation85
Dose equivalence
Numerous studies have proved that all three mentioned products are effective. However, the practitioners need to understand the differences to be able to have a comparable clinical outcome. The debate on conversion ratios might have been emphasized, understandably, from a commercial point of view.
There are different amounts of the 150 kDa toxin (and NAPs)/LD50 unit for different formulations of BoNT-A. Therefore, it is important for the clinicians to understand the equivalence ratio of the dose.
Clinical and preclinical analyses have demonstrated a clinical conversion ratio between ONA and INCO very close to 1:1.Citation86,Citation87 Prager et al reported that both these products had no statistically significant differences between them and showed high efficacy and good tolerability with a dose ratio of 1:1.Citation88 Kane et al carried out a prospective, randomized, double-blinded, parallel-group study where a single treatment with INCO or ONA was carried out in 250 females. This was followed by a 4-month observational period. They reported clinical equivalence with similar safety and efficacy profiles and patient-reported outcomes.Citation89
A number of studies have reported an ONA/INCO:ABO conversion factor of 1:3. However, this dose conversion is a topic of debate, and studies have reported ranges from 1:1 to as high as 1:11.Citation90–Citation93 The clinical and preclinical data available suggest a conversion ratio of 1:3 or 1:2.5. A higher conversion ratio may lead to the following:
Excessive dose
Increased incidence of adverse events
Underdosing when switching ABO to ONA.Citation3
Identical potency labeling between ONA and INCO allows easy exchange of these two drugs in clinical settings, and direct comparison of the efficacy, adverse effects, and costs. In summary, ABO and ONA have been reported to have nonparallel dose–response curves, and therefore differ in their relative potencies.Citation94 The presumed clinical effect of 1 unit of BoNT is not interchangeable between formulations.Citation95
Toxin spread
One of the factors contributing to remarkable safety record of BoNT therapy is the ability of the toxin to remain relatively localized at the site of injection.Citation96–Citation99 However, the effect of BoNT on areas away from the injection site is known as the toxin spread or field of effect.Citation3 Toxin spread to unwanted areas can be undesirable as it may increase the risk of adverse effects and complications. This is of particular importance when treating the face with BoNT as the injection sites and target muscles are very close to untargeted muscles. Therefore, to minimize unwanted effects, it is important that the toxin does not spread and affect the adjacent untargeted muscles. For example, eyelid ptosis is a serious complication and can be devastating for patients who have BoNT injections to improve their appearance. It can happen post BoNT-A treatment in the periorbital area due to unintended spread of the product to the levator palpebrae superioris muscle and consequently its reduced activity. The levator palpebrae superioris muscle is adjacent to the target muscles and injection sites recommended for the treatment of the upper face rhytides using BoNT. These include the following ():
Procerus
Depressor supercilii
Corrugator
Orbicularis oculi muscle.Citation22
Figure 3 Glabellar complex muscles and position of levator palpebrae superioris muscle.
There is a lack of consistency and much confusion about the terminology used regarding spread of the toxin (). Spread is an actual physical phenomenon that depends on several variables which are related to the injection done. It is a mechanistic effect and describes the physical movement of toxin from the original site of injection.
Table 3 Correct definitions to apply to botulinum toxin products for clinical administration
Diffusion is a passive phenomenon, and indicates the kinetic dispersion of the toxin outside its original injection site.Citation27 The effect of dose on diffusion is thought to be significant.Citation100 Arezzo exhibited a dose-dependent spread of biological activity to adjacent non-injected muscles.Citation101 Carruthers et al injected 30 units of ONA at different volumes used to reconstitute the vials for the treatment of glabellar lines. They reported that although there was no obvious relationship between the actual volume injected and response, higher dilutions can result in greater areas of “diffusion” and hence greater incidence of adverse effects.Citation102 Hsu et al reported in their prospective, randomized, controlled study that the area affected by the BoNT-A injection was 50% greater in the side with the larger volume with equivalent units of BoNT-A.Citation103
Migration is the distal effect, or the “retrograde transport” phenomena via the nerves (neuroaxonal transport) or by blood (hematogenous transport).Citation27,Citation104 Two phenomena take place after injection and rapid dissociation of the complex:Citation27
Diffusion: passive function, occurs from a very high to low concentration
Spread: physically driven, occurs active and fast.
Fick’s law of diffusion explains diffusion related to molecular weight. As such, the spread of neurotoxin into adjacent tissue is reported to be slower with the high-molecular-weight complex in comparison to the lower-molecular weight or free neurotoxin.Citation12,Citation28 However, this is debatable, and further clinical studies are required. Kerscher et al have demonstrated that ONA with complexing proteins and a molecular weight of 900 kDa and INCO without complexing proteins and a molecular weight 150 kDa have a comparable spread.Citation22 In addition, progenitor toxin size may be irrelevant with this regard as progenitor complexes are thought to dissociate in the vial on reconstitution with normal saline and under physiological conditions.Citation27,Citation28 Molecular weight and the presence of complexing proteins do not seem to affect spread or diffusion of the product.Citation28
Complexing proteins are believed to aid in the uptake and transcytosis of BoNT through the intestinal epithelium (protection from gastric pH extremes, resistance against stomach and intestinal proteases, and transportation across the intestinal epithelium) when ingested orally.Citation105,Citation106 However, in cosmetic and therapeutic setting where BoNT is not taken orally, the mentioned functions of the complexing proteins are not relevant to clinical efficacy.Citation30
A few studies have reported that both ONA and INCO have comparable spread.Citation22 Hexsel et al reported that similar action halos (muscular and sweat gland activity) were observed with standardized injections (equivalence ratio, same volume, depth, and technique) of ONA and ABO. However, ABO has been reported to have significantly greater spread than ONA/INCO.Citation107,Citation108
Several factors are thought to affect the potential for spread of BoNT, which include the following:Citation27,Citation109,Citation110
Clinical dose
Solution
Concentration
Injection technique
Type of target site
Post-injection massage
Location of injection within the muscle
Level of muscle hyperactivity
Depth of injection.
Immunogenicity
The ability of a protein product to elicit antibody formation is known as immunogenicity. Secondary nonresponse and primary nonresponse are different from immunogenicity (). BoNT preparations available commercially, excluding the excipient albumin, contain nonhuman proteins. These may act as antigens and elicit antibody formation when injected into a patient.Citation111 Botulinum toxin has the potential to induce an immune response, similar to other therapeutic proteins, and is regarded as foreign by the host. This is particularly true with repeated administration. Immunogenicity can result in development of neutralizing antibodies, which in turn may or may not result in secondary treatment failure.Citation29 Antibodies can be produced against the 150 kDa neurotoxin itself or the nontoxic complexing proteins (40–60% of treated patients) or both. The antibodies produced against the nontoxic complexing proteins are non-neutralizing antibodies and do not affect the neurotoxin activity. When antibodies are produced against the neurotoxin itself, the pharmacological effect of the neurotoxin is blocked. The rate of secondary treatment failure could potentially be reduced using purified neurotoxin preparations (INCO). Inactivated or nonactivated neurotoxins influence antibody formation and increase the risk of formation of neutralizing antibodies.Citation8
Table 4 Immunogenicity vs primary nonresponse vs secondary nonresponse
BoNT-A products have shown to exhibit lower clinically detectable levels of antibodies in comparison to other approved biological products.Citation111 Antibodies that may develop as a result of BoNT administration are not likely to cross-react with endogenous proteins; however, it is possible that the therapeutic response is lost.Citation111 Factors that impact the immunogenicity of BoNTs include the following:Citation111
Product-related factors
| |||||||||||||||||||||||||||||||||||||||||||||||||||||
Treatment-related factors | |||||||||||||||||||||||||||||||||||||||||||||||||||||
| ◦ | Dose: the overall toxin dose | ||||||||||||||||||||||||||||||||||||||||||||||||||||
| ◦ | Treatment intervals/booster injections
| ||||||||||||||||||||||||||||||||||||||||||||||||||||
| ◦ | Prior exposure
| ||||||||||||||||||||||||||||||||||||||||||||||||||||
Storage
ONA and ABO need to be stored under special temperatures, and this is critical. INCO can be stored at room temperature.Citation20 The manufacturers for the products recommend optimal storage condition for their products. The manufacturers recommend that BoNT-A should only be used within the first 4 hours after reconstitution of ONACitation117,Citation130 or within 1 hour after reconstitution of ABO.Citation113 The recommendation is for the reconstituted product to be kept at 2°C–8°C and administered within 24 hours after reconstitution. It also explains that the product should be used immediately considering a microbiological point of view.Citation114
Studies have shown that there is no alteration in potency of ONA even when it is refrigerated or refrozen for up to 1 weekCitation120 or for up to 2 weeks after reconstitution.Citation116–Citation118 Although warned about sterility issues, Park and Ahn reported no degradation of the potency of reconstituted ONA by refrigeration for 4 weeks.Citation119,Citation120 Hexsel et al reported that with correct sterile handling and storage under refrigeration, ONA within up to 6 weeks after reconstitution did not result in a significant alteration in the detectable clinical response from both patient’s and the observer’s point of view.Citation121 Soares et al studied the efficacy of INCO after prolonged storage (7 days) at room temperature (25°C) for treatment of dynamic lateral canthus lines. Their study was a randomized, double-blinded, split-face study, and evaluation was carried out over a 4-month period. They reported that prolonged storage at room temperature did not significantly alter its efficacy or longevity.Citation122
Adverse effects
The distant effect of BoNT is of concern as it can cause local or systemic adverse effects. Systemic adverse effects are due to the effect of BoNT on the tissues distant from the injection site and are due to transport within the blood.Citation20
The associated adverse effects are generally of three types:
Adverse effects related to expected effects of the BoNT, for example, excessive local muscle weakness
Adverse effects due to the spread of the BoNT to the surrounding muscles that were not injected or the target
Adverse effects due to systemic distribution of the toxin.Citation125
An increased frequency of local adverse effects with ABO compared to ONA has been reported when used for treating cervical dystonia.Citation126 Although the reason for this is unclear, this could be due to increased spread as demonstrated by animal studies or incorrect conversion factors.Citation20
The most effective dose at the smallest volume will achieve maximal dose response and minimal side effects. This means for targeted treatment, small volumes and high doses are effective and superior to large injection volume and low dose. The combination of small volume and high dose localizes the toxin, in addition to containing the biological effect of the toxin (muscle paralysis).Citation1,Citation127 Large volume and low dose weaken the muscle and may not result in complete muscle paralysis, resulting in an overall smoothing effect with an associated risk of toxin spread to adjacent untargeted muscles.Citation128,Citation129
Conclusion
Botulinum toxin products are used for therapeutic and cosmetic purposes, and their injections have been reported as the most popular noninvasive cosmetic procedure requested and carried out. The popularity of BoNT as a therapeutic and aesthetic agent is due to its potency, neurospecificity, efficacy, safety, complete reversibility, and a low rate of antibody formation. BoNT blocks presynaptic acetylcholine release resulting in reduced or diminished muscle contraction. It is used to temporarily treat wrinkles that are the result of muscle contraction and normal facial movement. This results in temporary improvement in the appearance of the areas affected by lines and wrinkles, for facial contouring, reducing sweating, and improving the skin. The different products available in the market vary in terms of units, chemical properties, biological activities, and weight and hence are not interchangeable. The products’ manufacturing process is different. Manufacturing process and conditions such as pH, temperature, formulation, and concentration are extremely crucial. Alterations in these process and conditions can increase the likelihood of formation of inactivated toxoid proteins, which in turn may be immunogenic. For safe clinical practice, and to achieve optimal results, the practitioners need to understand the clinical issues of potency, conversion ratio, and safety issues (toxin spread and immunogenicity). All three FDA-approved and popular preparations (ONA, INCO, ABO) are similar. The efficacy of ONA is comparable, and ONA and INCO have a 1:1 conversion ratio. These products are reported to have therapeutic equivalence in different indications. The conversation ratio of ABO is different from the other two preparations. The ratio is reported to be approximately 1:2.5. It is important to keep in mind that these products are not interchangeable. To reduce and minimize potential antibody resistance, the smallest effective dose should be used, treatment intervals should be less than 2–3 months, and booster injections should be avoided. The key factors affecting the clinical response to BoNT injections are individual anatomy, toxin preparation, dose–response relationship, reconstitution, length of storage after reconstitution, and immunogenicity. Injection patterns, techniques, dilutions, diffusion, and injection volumes of a particular formulation of BoNT are not interchangeable with other formulations. Understanding of clinical pharmacology of BoNT-A therapy will be useful for standardizing techniques used and achieving consistent and optimal therapeutic results. In addition, products and procedures must be selected and prescribed according to individual needs and aims of treatment.
Disclosure
The authors report no conflicts of interest in this work.
References
- HuangWFosterJARogachefskyASPharmacology of botulinum toxinJ Am Acad Dermatol200043224925910906647
- RossettoOPirazziniMMontecuccoCBotulinum neurotoxins: genetic, structural and mechanistic insightsNat Rev Microbiol201412853554924975322
- ScaglioneFConversion ratio between Botox®, Dysport®, and Xeo-min® in clinical practiceToxins (Basel)201683
- CoffieldJABakryNZhangRDCarlsonJGomellaLGSimpsonLLIn vitro characterization of botulinum toxin types A, C and D action on human tissues: combined electrophysiologic, pharmacologic and molecular biologic approachesJ Pharmacol Exp Ther19972803148914989067339
- EleopraRTugnoliVQuatraleRRossettoOMontecuccoCDifferent types of botulinum toxin in humansMov Disord200419Suppl 8S53S5915027055
- EleopraRTugnoliVQuatraleRRossettoOMontecuccoCDresslerDClinical use of non-A botulinum toxins: botulinum toxin type C and botulinum toxin type FNeurotox Res200692–312713116785109
- PirazziniMRossettoOEleopraRMontecuccoCBotulinum neurotoxins: biology, pharmacology, and toxicologyPharmacol Rev201769220023528356439
- BooneBBotulinum Toxin in Aesthetic Medicine European Handbook of Dermatological TreatmentsSpringerBerlin Heidelberg201510891106
- AokiKRGuyerBBotulinum toxin type A and other botulinum toxin serotypes: a comparative review of biochemical and pharmacological actionsEur J Neurol20018Suppl 5212911851731
- MontecuccoCMolgóJBotulinal neurotoxins: revival of an old killerCurr Opin Pharmacol20055327427915907915
- DresslerDSaberiFABarbosaERBotulinum toxin: mechanisms of actionArq Neuropsiquiatr200563118018515830090
- de PaivaAMeunierFAMolgóJAokiKRDollyJOFunctional repair of motor endplates after botulinum neurotoxin type A poisoning: biphasic switch of synaptic activity between nerve sprouts and their parent terminalsProc Natl Acad Sci U S A19999663200320510077661
- RogozhinAAPangKKBukharaevaEYoungCSlaterCRRecovery of mouse neuromuscular junctions from single and repeated injections of botulinum neurotoxin AJ Physiol2008586133163318218467364
- MatarassoSLComparison of botulinum toxin types A and B: a bilateral and double-blind randomized evaluation in the treatment of canthal rhytidesDermatol Surg2003291713 discussion 1312534505
- WilsonAJChangBTaglientiAJA quantitative analysis of OnabotulinumtoxinA, AbobotulinumtoxinA, and IncobotulinumtoxinA: a randomized, double-blind, prospective clinical trial of comparative dynamic strain reductionPlast Reconstr Surg201613751424143327119918
- RosalesRLBigalkeHDresslerDPharmacology of botulinum toxin: differences between type A preparationsEur J Neurol200613Suppl 1210
- SwaminathanSEswaramoorthySStructural analysis of the catalytic and binding sites of Clostridium botulinum neurotoxin BNat Struct Biol20007869369910932256
- MontalMBotulinum neurotoxin: a marvel of protein designAnnu Rev Biochem20107959161720233039
- RossettoOMorbiatoLCaccinPRigoniMMontecuccoCPresynaptic enzymatic neurotoxinsJ Neurochem20069761534154516805767
- DresslerDBeneckeRPharmacology of therapeutic botulinum toxin preparationsDisabil Rehabil200729231761176818033601
- FrevertJContent of botulinum neurotoxin in botox®/vistabel®, dysport®/azzalure®, and xeomin®/bocouture®Drugs R D2010102677320698714
- KerscherMRollSBeckerAWigger-AlbertiWComparison of the spread of three botulinum toxin type A preparationsArch Dermatol Res2012304215516122002325
- PickettAConsistent biochemical data are essential for comparability of botulinum toxin type A productsDrugs R D20111119798 author reply 98–9921410299
- FangPKRaphaelBHMaslankaSECaiSSinghBRAnalysis of genomic differences among Clostridium botulinum type A1 strainsBMC Genomics20101172521182778
- PanjwaniNO’KeeffeRPickettABiochemical, functional and potency characteristics of type A botulinum toxin in clinical useBotulinum J200811153166
- SchantzEJJohnsonEAProperties and use of botulinum toxin and other microbial neurotoxins in medicineMicrobiol Rev199256180991579114
- PickettADysport: pharmacological properties and factors that influence toxin actionToxicon200954568368919332087
- EiseleKHFinkKVeyMTaylorHVStudies on the dissociation of botulinum neurotoxin type A complexesToxicon201157455556521195107
- FrevertJPharmaceutical, biological, and clinical properties of botulinum neurotoxin type A productsDrugs R D20151511925559581
- FrevertJDresslerDComplexing proteins in botulinum toxin type A drugs: a help or a hindrance?Biologics2010432533221209727
- RummelAThe long journey of botulinum neurotoxins into the synapseToxicon2015107Pt A92426363288
- WheelerASmithHSBotulinum toxins: mechanisms of action, anti-nociception and clinical applicationsToxicology201330612414623435179
- ForanPGMohammedNLiskGOEvaluation of the therapeutic usefulness of botulinum neurotoxin B, C1, E, and F compared with the long lasting type A. Basis for distinct durations of inhibition of exocytosis in central neuronsJ Biol Chem200327821363137112381720
- ShaariCMSandersIQuantifying how location and dose of botulinum toxin injections affect muscle paralysisMuscle Nerve19931699649698355728
- AntonucciFRossiCGianfranceschiLRossettoOCaleoMLong-distance retrograde effects of botulinum neurotoxin AJ Neurosci200828143689369618385327
- MatakIBach-RojeckyLFilipovićBLackovićZBehavioral and immunohistochemical evidence for central antinociceptive activity of botulinum toxin ANeuroscience201118620120721539899
- MatakIRiedererPLackovićZBotulinum toxin’s axonal transport from periphery to the spinal cordNeurochem Int201261223623922580329
- RestaniLAntonucciFGianfranceschiLRossiCRossettoOCaleoMEvidence for anterograde transport and transcytosis of botulinum neurotoxin A (BoNT/A)J Neurosci20113144156501565922049408
- MazzocchioRCaleoMMore than at the neuromuscular synapse: actions of botulinum neurotoxin A in the central nervous systemNeuroscientist2015211446124576870
- MatakILackovićZBotulinum toxin A, brain and painProg Neurobiol2014119–1203959
- LeeHHKimSTLeeKJBaikHSEffect of a second injection of botulinum toxin on lower facial contouring, as evaluated using 3-dimensional laser scanningDermatol Surg201541443944425775445
- KeaneyTCAlsterTSBotulinum toxin in men: review of relevant anatomy and clinical trial dataDermatol Surg201339101434144324090254
- CarruthersACarruthersJProspective, double-blind, randomized, parallel-group, dose-ranging study of botulinum toxin type A in men with glabellar rhytidsDermatol Surg200531101297130316188182
- NestorMAblonGPickettAKey parameters for the use of abobotulinumtoxinA in aesthetics: onset and durationAesthet Surg J201737suppl_1S20S3128388717
- HallettMExplanation of timing of botulinum neurotoxin effects, onset and duration, and clinical ways of influencing themToxicon2015107Pt A646726220801
- SimpsonLLIdentification of the major steps in botulinum toxin actionAnnu Rev Pharmacol Toxicol20044416719314744243
- HankinsCLStrimlingRRogersGSBotulinum A toxin for glabellar wrinklesDermatol Surg19982411118111839834736
- FlynnTCBotulinum toxinAm J Clin Dermatol201011318319920369902
- CarruthersACarruthersJLoweNJOne-year, randomised, multicenter, two-period study of the safety and efficacy of repeated treatments with botulinum toxin type A in patients with glabellar linesJ Drug Assess2004726386
- MichaelsBMCsankGARybGEEkoFNRubinAProspective randomized comparison of onabotulinumtoxinA (Botox) and abobotulinumtoxinA (Dysport) in the treatment of forehead, glabellar, and periorbital wrinklesAesthet Surg J20123219610222231417
- SmallRBotulinum toxin injection for facial wrinklesAm Fam Physician201490316817525077722
- DollyJOAokiKRThe structure and mode of action of different botulinum toxinsEur J Neurol200613Suppl 41917112344
- RapplTParviziDFriedlHOnset and duration of effect of incobotulinumtoxinA, onabotulinumtoxinA, and abobotulinumtoxinA in the treatment of glabellar frown lines: a randomized, double-blind studyClin Cosmet Investig Dermatol20136211219
- GlogauRKaneMBeddingfieldFOnabotulinumtoxinA: a meta-analysis of duration of effect in the treatment of glabellar linesDermatol Surg201238111794180323106853
- DresslerDRothwellJCElectromyographic quantification of the paralysing effect of botulinum toxin in the sternocleidomastoid muscleEur Neurol2000431131610798896
- PoeweWDeuschlGNebeAWhat is the optimal dose of botulinum toxin A in the treatment of cervical dystonia? Results of a double blind, placebo controlled, dose ranging study using Dysport. German Dystonia Study GroupJ Neurol Neurosurg Psychiatry199864113179436721
- FlynnTCBotulinum toxin: examining duration of effect in facial aesthetic applicationsAm J Clin Dermatol201011318319920369902
- CarruthersACarruthersJSaidSDose-ranging study of botulinum toxin type A in the treatment of glabellar rhytids in femalesDermatol Surg2005314414422 discussion 42215871316
- KimNHChungJHParkRHParkJBThe use of botulinum toxin type A in aesthetic mandibular contouringPlast Reconstr Surg2005115391993015731696
- ParkMYAhnKYJungDSBotulinum toxin type A treatment for contouring of the lower faceDermatol Surg2003295477483 discussion 48312752514
- AhnJHornCBlitzerABotulinum toxin for masseter reduction in Asian patientsArch Facial Plast Surg20046318819115148129
- SmythAGBotulinum toxin treatment of bilateral masseteric hypertrophyBr J Oral Maxillofac Surg199432129338136335
- GuyuronBRoseKKrieglerJSTuckerTHourglass deformity after botulinum toxin type A injectionHeadache200444326226415012666
- SesardicDDasRGAlternatives to the LD50 assay for botulinum toxin potency testing: strategies and progress towards refinement, reduction and replacement. Proc. 6th World Congress on Alternatives and Animal Use in the Life Sciences, Tokyo, Japan, 21–25 August 2007AATEX200714Special Issue581585
- Fernández-SalasEWangJMolinaYNelsonJBJackyBPAokiKRBotulinum neurotoxin serotype A specific cell-based potency assay to replace the mouse bioassayPLoS One2012711e4951623185348
- Business WireAllergan receives FDA approval for first-of-its-kind, fully in vitro, cell-based assay for BOTOX® and BOTOX® cosmetic (onabotulinumtoxinA)2011 Available from: http://www.busi-nesswire.com/news/home/20110624005918/en/Allergan-Receives-FDA-Approval-First-of-Its-Kind-Fully-vitroAccessed February 2018
- AdlerSBickerGBigalkeHThe current scientific and legal status of alternative methods to the LD50 test for botulinum neurotoxin potency testing. The report and recommendations of a ZEBET Expert MeetingAltern Lab Anim201038431533020822324
- HambletonPPickettAMPotency equivalence of botulinum toxin preparationsJ R Soc Med19948711719
- SesardicDIs it possible to accurately determine content of botulinum neurotoxin type A in drug products?Drugs R D2010102919220698717
- HuntTClarkeKPotency evaluation of a formulated drug product containing 150-kd botulinum neurotoxin type AClin Neuropharma-col20093212831
- CarruthersJDCarruthersJATreatment of glabellar frown lines with C. botulinum-A exotoxinJ Dermatol Surg Oncol199218117211740562
- KleinAWDilution and storage of botulinum toxinDermatol Surg19982411117911809834735
- AlamMDoverJSArndtKAPain associated with injection of botulinum A exotoxin reconstituted using isotonic sodium chloride with and without preservative: a double-blind, randomized controlled trialArch Dermatol2002138451051411939813
- KwiatDMBersaniTABersaniAIncreased patient comfort utilizing botulinum toxin type A reconstituted with preserved versus nonpre-served salineOphthal Plast Reconstr Surg2004203186189
- SarifakiogluNSarifakiogluEEvaluating effects of preservative-containing saline solution on pain perception during botulinum toxin type-a injections at different locations: a prospective, single-blinded, randomized controlled trialAesthetic Plast Surg200529211311515815811
- Trindade De AlmeidaARKaduncBVDi ChiacchioNNetoDRFoam during reconstitution does not affect the potency of botulinum toxin type ADermatol Surg2003295530531 discussion 53212752523
- KazimNABlackEHBotox: shaken, not stirredOphthal Plast Reconstr Surg20082411012
- CarruthersJFagienSMatarassoSLConsensus recommendations on the use of botulinum toxin type A in facial aestheticsOphthal Plast Reconstr Surg2005212165
- Trindade De AlmeidaARSeccoLCCarruthersAHandling botulinum toxins: an updated literature reviewDermatol Surg201137111553156521777338
- CareyWDIncorrect reconstitution of incobotulinumtoxinA leads to loss of neurotoxinJ Drugs Dermatol201413673573824918566
- NiamtuJ3rdNeurotoxin waste from drawing product through the vial stopperJ Clin Aesthet Dermatol201476333725013537
- FlynnTCCarruthersACarruthersJSurgical pearl: the use of the Ultra-Fine II short needle 0.3-cc insulin syringe for botulinum toxin injectionsJ Am Acad Dermatol200246693193312063494
- YanagiharaMFujiiTWakamatuNIshizakiHTakeharaTNawateKSilicone granuloma on the entry points of acupuncture, venepuncture and surgical needlesJ Cutan Pathol200027630130510885407
- BaldwinRNContamination of insulin by silicone oil: a potential hazard of plastic insulin syringesDiabet Med1988587897902975573
- TschetterAJHochwaltPCColleranEStoneMSSilicone granulomas in the setting of acupuncture with silicone-coated needlesJ Clin Investig Dermatol2014212
- DresslerDManderGFinkKMeasuring the potency labelling of onabotulinumtoxinA (Botox®) and incobotulinumtoxinA (Xeomin®) in an LD50 assayJ Neural Transm (Vienna)20121191131521971766
- AokiKRRanouxDWisselJUsing translational medicine to understand clinical differences between botulinum toxin formulationsEur J Neurol200613Suppl 41019
- PragerWWissmüllerEKollhorstBWilliamsSZschockeIComparison of two botulinum toxin type A preparations for treating crow’s feet: a split-face, double-blind, proof-of-concept studyDermatol Surg201036Suppl 42155216021134046
- KaneMAGoldMHColemanWP3rdA randomized, double-blind trial to investigate the equivalence of IncobotulinumtoxinA and OnabotulinumtoxinA for glabellar frown linesDermatol Surg201541111310131926509943
- MarchettiAMagarRFindleyLRetrospective evaluation of the dose of Dysport and BOTOX in the management of cervical dystonia and blepharospasm: the REAL DOSE studyMov Disord200520893794415810022
- WohlfarthKGöschelHFrevertJDenglerRBigalkeHBotulinum A toxins: units versus unitsNaunyn Schmiedebergs Arch Pharmacol199735533353409089663
- RanouxDGuryCFondaraiJMasJLZuberMRespective potencies of Botox and Dysport: a double blind, randomised, crossover study in cervical dystoniaJ Neurol Neurosurg Psychiatry200272445946211909903
- YunJYKimJWKimHTDysport and Botox at a ratio of 2.5:1 units in cervical dystonia: a double-blind, randomized studyMov Disord201530220621325476727
- De BoulleKFagienSSommerBGlogauRTreating glabellar lines with botulinum toxin type A-hemagglutinin complex: a review of the science, the clinical data, and patient satisfactionClin Interv Aging2010510111820458348
- AokiKRIrvineRGallagherCRe: Botox produces functional weakness in non-injected muscles adjacent to the target muscleJ Biomech20084192066206718508061
- BentivoglioARFasanoAIalongoTSoletiFLo FermoSAlbaneseAFifteen-year experience in treating blepharospasm with Botox or Dysport: same toxin, two drugsNeurotox Res200915322423119384595
- CillinoSRaimondiGGuépratteNLong-term efficacy of botulinum toxin A for treatment of blepharospasm, hemifacial spasm, and spastic entropion: a multicentre study using two drug-dose escalation indexesEye (Lond)201024460060719648904
- JankovicJBotulinum toxin therapy for cervical dystoniaNeurotox Res200692–314514816785112
- LunguCKarpBIAlterKZolbrodRHallettMLong-term followup of botulinum toxin therapy for focal hand dystonia: outcome at 10 years or moreMov Disord201126475075321506157
- KaneMAMonheitGThe practical use of AbobotulinumtoxinA in aestheticsAesthet Surg J201737Suppl_1S12S1928388719
- ArezzoJCNeuroBloc®/Myobloc®: unique features and findingsToxicon200954569069619286001
- CarruthersACarruthersJCohenJDilution volume of botulinum toxin type A for the treatment of glabellar rhytides: does it matter?Dermatol Surg2007331 Spec NoS97S10417241422
- HsuTSDoverJSArndtKAEffect of volume and concentration on the diffusion of botulinum exotoxin AArch Dermatol2004140111351135415545544
- Ramirez-CastanedaJJankovicJComellaCDashtipourKFernandezHHMariZDiffusion, spread, and migration of botulinum toxinMov Disord201328131775178323868503
- JinYTakegaharaYSugawaraYMatsumuraTFujinagaYDisruption of the epithelial barrier by botulinum haemagglutinin (HA) proteins – differences in cell tropism and the mechanism of action between HA proteins of types A or B, and HA proteins of type CMicrobiology2009155Pt 1354519118344
- FujinagaYTransport of bacterial toxins into target cells: pathways followed by cholera toxin and botulinum progenitor toxinJ Biochem2006140215516016954533
- HexselDBrumCdo PradoDZField effect of two commercial preparations of botulinum toxin type A: a prospective, double-blind, randomized clinical trialJ Am Acad Dermatol201267222623222041253
- Trindade de AlmeidaARMarquesEde AlmeidaJCunhaTBorasoRPilot study comparing the diffusion of two formulations of botulinum toxin type A in patients with forehead hyperhidrosisDermatol Surg2007331 Spec NoS37S4317241413
- BrodskyMASwopeDMGrimesDDiffusion of botulinum toxinsTremor Other Hyperkinet Mov (N Y)20122 tre-02-85-417-1
- RocheNSchnitzlerAGenêtFFDurandMCBensmailDUndesirable distant effects following botulinum toxin type a injectionClin Neuropharmacol200831527228018836345
- NaumannMBooLMAckermanAHGallagherCJImmunogenicity of botulinum toxinsJ Neural Transm (Vienna)2013120227529023008029
- BOTOX® [package insert]Irvine, CAAllergan, Inc2002
- Dysport® [package insert]MaidenheadIpsen Products2002
- Package leaflet: Information for the user – BOCOUTURE 50 units powder for solution for injection2016
- MarkeyACBotulinum A exotoxin in cosmetic dermatologyClin Exp Dermatol200025317317510844487
- SloopRRColeBAEscutinROReconstituted botulinum toxin type A does not lose potency in humans if it is refrozen or refrigerated for 2 weeks before useNeurology19974812492539008526
- FrankelASBotox for rejuvenation of the periorbital regionFacial Plast Surg199915325526211816088
- CarruthersACarruthersJToxins 99, new information about the botulinum neurotoxinsDermatol Surg2000263174176
- ParkMYAhnKYEffect of the refrigerator storage time on the potency of botox for human extensor digitorum brevis muscle paralysisJ Clin Neurol20139315716423894239
- YangGCChiuRJGillmanGSQuestioning the need to use Botox within 4 hours of reconstitution: a study of fresh vs 2-week-old BotoxArch Facial Plast Surg200810427327918645097
- HexselDMDe AlmeidaATRutowitschMMulticenter, double-blind study of the efficacy of injections with botulinum toxin type A reconstituted up to six consecutive weeks before applicationDermatol Surg200329552352912752522
- SoaresDJDejosephLMZulianiGFLiebertzDJPatelVSImpact of postreconstitution room temperature storage on the efficacy of incobotulinumtoxinA treatment of dynamic lateral canthus linesDermatol Surg201541671271725973563
- DYSPORT® (abobotulinumtoxinA) for injection [prescribing information]Basking Ridge, NJIpsen Biopharmaceuticals, Inc2017
- MEDICATION GUIDE, BOTOX® BOTOX®, Cosmetic (Boetox), (onabotulinumtoxinA) for Injection Available from: https://www.aller-gan.com/miscellaneous-pages/allergan-pdf-files/botox_med_guideAccessed February 2018
- FosterKABigalkeHAokiKRBotulinum neurotoxin - from laboratory to bedsideNeurotox Res200692–313314016785110
- DresslerDDysport produces intrinsically more swallowing problems than Botox: unexpected results from a conversion factor study in cervical dystoniaJ Neurol Neurosurg Psychiatry2002735604 author reply 604
- BorodicGEPearceLBSmithKJosephMBotulinum a toxin for spasmodic torticollis: multiple vs single injection points per muscleHead Neck199214133371624292
- GarciaAFultonJEJrCosmetic denervation of the muscles of facial expression with botulinum toxin. A dose-response studyDermatol Surg199622139438556256
- EdelsteinCShorrNJacobsJBalchKGoldbergROculoplastic experience with the cosmetic use of botulinum A exotoxinDermatol Surg19982411120812129834740
- Highlights of prescribing information, BOTOX Cosmetic (onabotulinumtoxinA) for injection, for intramuscular use, Initial U.S. Approval: 1989 Revised 10/2017 [cited 2018; Available from: https://www.allergan.com/assets/pdf/botox_cosmetic_pi.pdf