Abstract
Background:
Environmental factors, including socioeconomic status, may affect inflammatory bowel disease (IBD). There is a paucity of data on the epidemiology of IBD among patients of low socioeconomic status.
Aim:
To examine the epidemiologic features of IBD among African-American, Hispanic, and Caucasian patients from a county hospital, where the majority of the patients are socioeconomically disadvantaged.
Methods:
A retrospective study was conducted on a cohort of patients diagnosed with IBD based on clinical, radiologic, endoscopic, and histological data. We reviewed charts of adults aged 20–70 years diagnosed with IBD between 2000 and 2006. Demographic data, disease subtype, and phenotypic features of IBD were recorded based on the Montreal Classification. The data were analyzed using the chi-square, Fisher exact, Wilcoxon rank-sum, and Student’s t-tests.
Results:
The study cohort included 273 patients, with 54% female, 30% Caucasian, 44% African-American, and 26% Hispanic. Over half (54%) of the patients had Crohn’s disease (CD), and 46% had ulcerative colitis (UC). The mean age at diagnosis was 40 ± 14 years with no significant difference between CD and UC (age 43 ± 13 versus 44.5 ± 14, respectively; P = 0.5). Females were diagnosed at a significantly later age than males (46 ± 13 years versus 40 ± 13, respectively; P = 0.001). This trend remained significant for females with CD and UC, and across each racial/ethnic group. Hispanic patients were diagnosed with UC more often than Caucasian patients (64% versus 34%; odds ratio [OR] 3.5; 95% confidence interval [CI]: 1.8–6.5, P = 0.0003) or African-Americans (64% versus 43%; OR 2.3; 95% CI: 1.3–4.3, P = 0.005). Among the 147 patients with CD, 54% had fistulizing and/or stricturing disease. The prevalence of fistulizing, stricturing, and inflammatory CD was similar across all age, gender, and racial/ethnic groups.
Conclusions:
Within an indigent population, UC was diagnosed more often in Hispanics than CD. Females were diagnosed at a significantly older age than males across all racial/ethnic groups. There was no difference in the CD phenotypes between the three ethnic groups. Understanding the epidemiology of IBD will require examination of the interactions between gender, race/ethnicity, and environmental factors.
Keywords:
Introduction
The term inflammatory bowel disease (IBD) includes Crohn’s disease (CD) and ulcerative colitis (UC) and is ranked among the five most prevalent gastrointestinal diseases in the United States.Citation1 IBD is estimated to affect over one million patients in the United States and be responsible for annual health care costs exceeding US$1.7 billion.Citation1–Citation4 The etiology and the natural history of IBD are both influenced by environmental and genetic factors. IBD is considered a complex polygenic disorder in which the genotypic profile influences the disease characteristics.Citation5–Citation6 Environmental exposures such as cultural background, socioeconomic status, and diet are also important, although data concerning environmental–genetic interactions are sparse.Citation5
Our current understanding of the epidemiology, prognosis, and treatment of IBD is currently based primarily on studies conducted in Caucasian populations,Citation7–Citation9 despite the fact that over the last two decades the incidence of hospitalizations for IBD among African-Americans has begun to approach that of Caucasians.Citation10–Citation12 Our aim was to examine the epidemiologic features of IBD among multiethnic patients in a county hospital that primarily serves patients of low socioeconomic status. We also evaluated these patients for differences in IBD phenotype between racial/ethnic groups.
Materials and methods
Study design
We performed a cross-sectional study of all patients with IBD treated in the Harris County Hospital District (HCHD) between 2000 and 2006. Patients with IBD were identified using diagnostic codes from the International Classification of Disease (ICD) 9th (555.x [CD] and 556.x [UC]) and 10th editions (K50.x [CD] and K51.x [UC]). Primary medical record review was performed by a gastroenterologist (JKH) using a standardized abstraction form.
The diagnosis of IBD was confirmed based on findings consistent with current practice criteria. Patients with a history of bowel resection prior to seeking care within the HCHD were eligible for inclusion without histologic confirmation. Perianal surgery included fistulotomy, abscess drainage, or seton placement. Patients with a non-IBD diagnosis on follow-up (infection, ischemia, or malignancy) or indeterminate colitis were excluded, as were patients under the age of 18 years.
Study setting
HCHD comprises three inpatient facilities and 13 outpatient clinics and serves the residents of the third most populous county in the United States. Over 40,000 hospital admissions and more than 900,000 clinic visits occurred in the HCHD between 2000 and 2006.Citation14 Sixty percent of the patients are charity/self-pay and nearly 60% are Hispanic. More than half of the patients in the HCHD are female (HCHD internal data source). This study was conducted with the approval of the Baylor College of Medicine and HCHD Institutional Review Boards.
Data collection
The HCHD uses the EpicWeb (Epic Systems Incorporated, Wisconsin, MN, USA) electronic medical record (EMR) system. This EMR contains laboratory, endoscopy, radiology, and pathology reports; limited inpatient records (admission history and physical and discharge summaries); and ambulatory care records.
Demographic data including age, gender, and race/ethnicity were recorded for each study patient. Race/ethnicity was based on patient self-report in the medical record. Only data involving African-American, Caucasian, and Hispanic patients were included in this study due to the small sample size of the other ethnic groups.
IBD characteristics were recorded for each study patient. CD and UC location and phenotype were classified according to the Montreal Classification. The extent of UC was determined based on evidence of endoscopic or histological activity. The phenotype of CD was identified as fistulizing, stricturing, or inflammatory disease based on available data.
Statistical analysis
Categorical variables were compared using chi-square and ANOVA tests. Continuous variables were compared using Wilcoxon rank-sum and Student’s t-tests. Age was analyzed as a continuous variable and was also categorized into five groups by each decade. Statistical analysis was performed using SAS version 4.0 Software.Citation13
Results
The study cohort included 273 patients with 54% female, 30% Caucasian, 44% African-American, and 26% Hispanic. Over half of the patients had CD and 46% had UC (). The mean age at diagnosis was 40 ± 14 years with no significant difference between CD and UC (age 43 ± 13 versus 44.5 ± 14, respectively; P = 0.5). Female patients with IBD were diagnosed at a significantly later age than male patients, and this trend was consistent for both CD and UC. Although this trend was seen among all three racial/ethnic groups, it was significant among the African-American patients. Hispanic patients were diagnosed with UC more often than Caucasian (64% versus 34%; odds ratio [OR] 3.5; 95% confidence interval [CI]: 1.8–6.5, P = 0.0003) or African-American patients (64% versus 43%; OR 2.3; 95% CI: 1.3–4.3, P = 0.005). Caucasians were diagnosed with CD more often than UC ().
Figure 1 The CD:UC ratio among the total study population by race/ethnicity. Hispanics were diagnosed more often with UC than with CD, Caucasians were diagnosed more often with CD than with UC, and African-Americans were diagnosed more often with CD than with UC, but the difference was not significant.
Abbreviations: IBD; inflammatory bowel disease; CD, Crohn’s disease; UC, ulcerative colitis.
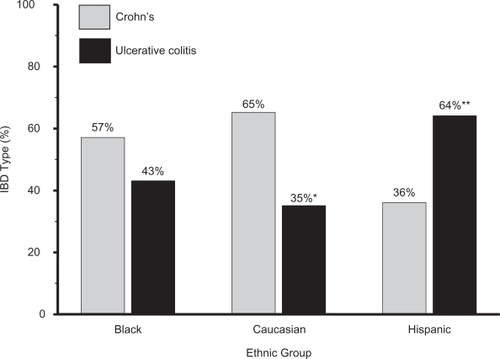
Table 1 The mean age of diagnosis/presentation of inflammatory bowel disease by gender among the 273 adults in the study
Crohn’s disease characteristics
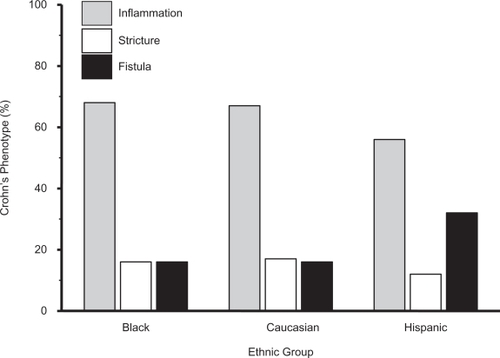
The prevalence of the inflammatory phenotype was significantly greater than stricturing disease (65% versus 16%, OR 4.1, 95% CI: 2.5–7.0, P = 001) or fistulizing disease (65% versus 19%, OR 3.4, 95% CI: 2.1–5.5, P = 0.001). The fistulizing phenotype was seen twice as often in Hispanics than Caucasians or African-Americans, although this did not reach statistical significance, possibly due to the small sample size (32% versus 17%, OR 2.0, 95% CI: 0.7–5.5, P = 0.20, versus 16%, OR 2.2, 95% CI: 0.7–5.2, P = 0.18, respectively) (). The overall rate of fistulizing, stricturing, and inflammatory CD was similar across all age groups and between male and female patients.
Figure 2 The distribution rates of Crohn’s disease (CD) phenotype by race/ethnicity among the 147 patients with CD. Hispanics have twice the rate of fistualzing disease than African-Americans or Caucasians. There were no significant differences in the distribution rates of inflammation and strictures between the three ethnic groups.
Ulcerative colitis characteristics
The majority of the patients (62%) with UC had pancolitis, 27% had left-sided colitis, and 11% had proctitis. This distribution was similar across all racial/ethnic groups. The mean age of patients with left-sided colitis was significantly higher than those with pancolitis or proctitis (age 50 ± 14.1 versus 41.5 ± 14.4, 41.2 ± 13.4, respectively; P = 0.05). Females had a significantly higher rate of left colitis than males (30% versus 13%, OR 2.1, 95% CI: 1.1–5.4, P = 0.001). Males had a higher rate of pancolitis than females, but that difference was not significant (56% versus 42%, OR 1.3, 95% CI: 0.6–2.1, P = 0.60).
Discussion
Although IBD has been reported worldwide, most studies have focused on the Caucasian populations, and there is still a paucity of literature on the epidemiologic aspects of the disease in Hispanics and African-Americans. Moreover, IBD has not previously been studied in populations of low socioeconomic status. In this study of a multiethnic IBD population of predominantly low socioeconomic status, we found that Hispanics were diagnosed with UC more than CD. Our findings are consistent with the results reported from Puerto Rico that showed that a higher proportion of study patients were diagnosed with UC than with CD.Citation13–Citation15 This finding was also reported in another United States study in which Mexican-Americans predominantly had UC, compared with Caucasians and African-Americans, who predominantly had CD.Citation16 An earlier study from a health maintenance organization database in California found that Hispanics had a lower prevalence of CD compared with both African-Americans and Caucasians.Citation17 A systematic review of 28 publications encompassing 1272 Hispanic and 547 African-American patients with IBD found that a greater proportion of Hispanic patients were diagnosed with UC than with CD compared with African-American patients.Citation18 On the contrary, Nguyen et al reported a higher frequency of CD compared with UC among a Puerto Rican population.Citation11 This dissimilarity in the study results could be due to differences in the study design, the characteristics of the study population, or the differences in the genetic and environmental exposure(s) of the studied population.
The difference in the distribution rate of CD and UC across the three racial/ethnic groups emphasizes the potential role of genetics and environmental interaction on the etiology of IBD. A recent study reported that African-American and Hispanic CD patients, but not UC patients, had a lower prevalence of family history of IBD than their Caucasian counterparts, concluding that racial differences may reflect underlying genetic variations.Citation11 It is also worth pointing out that differences in diet and hygiene are changing over time and could play a role in the etiology of IBD. The high-fat intake diet among the African-American population could possibly contribute to the etiology of CD. A study from the United States among urban African-Americans found 77% of the study population had a diet that is very high in fat.Citation19
The second novel finding of our study is the difference in the mean age of diagnosis between females and males. Female patients with IBD were diagnosed at a significantly older age than males. Although this trend was consistent among the three ethnic groups for UC, it was reversed among Caucasians diagnosed with CD, as males were diagnosed later than females. This observation was not previously reported, and the clear reason for that difference is unknown. This finding could be due to true gender differences or because women had sought medical care for their symptoms later than men. It is less likely to be due to a high proportion of women treated in the studied hospital because, based on an HCHD internal source (unpublished data), 59% of the patients treated between 2008 and 2009 were females. Nevertheless, IBD is a complex disease that is controlled by multiple risk factors,Citation20 and the difference in age of diagnosis between genders deserves to be further studied.
Our results revealed similar rates of fistualizing disease in African-Americans and Caucasians with CD. This finding contradicts the concept that African-Americans diagnosed with CD have a more severe disease course than CaucasiansCitation21–Citation22 but is in agreement with Deveaux et al, who reported that there was no difference in disease presentation between African-American and Caucasian patients who required surgery for CD.Citation23 Another study by Mahid et al has recently published a systemic review on the comparison of the course of IBD between African-Americans and Caucasians among over 2000 cases of IBD and reported similar findings to our results.Citation12 Of interest, we found that the rate of fistulizing CD among Hispanics was double that of the other two ethnic groups. Because there are few published data on distribution and manifestation of IBD in Hispanics, we were not able to make a comparison with this finding in the literature. The Mid-Atlantic Crohn’s Disease Study Group conducted a multicenter survey of African-American and Caucasian patients with CD who were matched by age, gender, and practice type (teaching versus private practice setting) and reported that African-American and Caucasian patients have similar disease course presentations.Citation24
The utilization of data for constructing the current cross-sectional study has some shortcomings. First, the retrospective nature of the data collection may be limited by incomplete documentation. However, the HCHD has a comprehensive system that details all radiology, endoscopy, pathology, and laboratory reports – data that are essential in the diagnosis and management of patients with IBD. The second limitation of the study is that we were not able to examine the effect of other races due to their small sample size. However, our study is the largest study comparing African-Americans, Hispanics, and Caucasians with IBD in the United States to date. In the 2000 Census, nearly 60% of the Hispanic population in the United States was of Mexican descent, which is similar to the majority of the Hispanic population of Harris County. Therefore, our data reflect the findings of a predominantly Mexican-American patient population with IBD. Our results could be more representative of the overall indigent Hispanic population in the United States. We also found that the three studied ethnic groups underwent similar rates of diagnostic testing during the study period. Finally, all patients within the HCHD have equal access to physicians, hospital facilities, and the pharmacy, thus eliminating potential provider or patient bias that may delay the diagnosis.
In conclusion, our study demonstrates clear evidence of the importance of the effect of ethnicity on the presentation and manifestation of IBD. Hispanics were diagnosed more frequently with UC, whereas African-Americans and Caucasians were diagnosed more frequently with CD. Females were diagnosed with IBD at an older age than males, and the difference was consistent for the three racial/ethnic groups. Understanding the epidemiology of IBD requires better understanding of the interactions between environment, ethnic group, age, and socioeconomic conditions.
Disclosure
The authors report no conflicts of interest in this work.
References
- SandlerRSEverhartJEDonowitzMThe burden of selected digestive diseases in the United StatesGastroenterology20021221500151111984534
- BaldassanoRNPiccoliDAInflammatory bowel disease in pediatric and adolescent patientsGastroenterol Clin North Am19992844545810372276
- MarxGSeidmanEGMartinSRDeslandresCOutcome of Crohn’s disease diagnosed before two years of ageJ Pediatr200214047047312006965
- LoftusEVJrClinical epidemiology of inflammatory bowel disease: incidence, prevalence, and environmental influencesGastroenterology20041261504151715168363
- WeersmaRKStokkersPCCleynenIConfirmation of multiple Crohn’s disease susceptibility loci in a large Dutch-Belgian cohortAm J Gastroenterol200910463063819174780
- SuCLichtensteinGRRecent developments in inflammatory bowel diseaseMed Clin North Am2002861497152312510462
- LoftusEVJrSilversteinMDSandbornWJTremaineWJHarmsenWSZinsmeisterARUlcerative colitis in Olmsted County, Minnesota, 1940–1993: incidence, prevalence, and survivalGut20004633634310673294
- LoftusEVJrSilversteinMDSandbornWJTremaineWJHarmsenWSZinsmeisterARCrohn’s disease in Olmsted County, Minnesota, 1940–1993: incidence, prevalence, and survivalGastroenterology1998114116111689609752
- VindIRiisLJessTfor the DCCD study groupIncreasing incidences of inflammatory bowel disease and decreasing surgery rates in Copenhagen City and County, 2003–2005: a population-based study from the Danish Crohn colitis databaseAm J Gastroenterol20061011274128216771949
- FinlayDGBasuDSellinJHEffect of race and ethnicity on perceptions of inflammatory bowel diseaseInflamm Bowel Dis20061250350716775495
- NguyenGCTorresEARegueiroMInflammatory bowel disease characteristics among African Americans, Hispanics, and non-Hispanic Whites: characterization of a large North American cohortAm J Gastroenterol20061011012102316696785
- MahidSSMulhallAMGholsonRDEichenbergerMRGalandiukSInflammatory bowel disease and African Americans: a systematic reviewInflamm Bowel Dis20081496096718266229
- MorenoJMRubioCETorresEAInflammatory disease of the gastrointestinal tract at the University Hospital, Medical Center, Puerto Rico. 1980–1987 [in Spanish]Bol Asoc Med P R1989812142182765040
- TorresEAde JesúsRPérezCMPrevalence of inflammatory bowel disease in an insured population in Puerto Rico during 1996P R Health Sci J20032225325814619451
- AppleyardCBHernándezGRios-BedoyaCFBasic epidemiology of inflammatory bowel disease in Puerto RicoInflamm Bowel Dis20041010611115168809
- BasuDLopezIKulkarniAImpact of race and ethnicity on inflammatory bowel diseaseAm J Gastroenterol20051002254226116181378
- KurataJHKantor-FishSFranklHGodbyPVadheimCMCrohn’s disease among ethnic groups in a large health maintenance organizationGastroenterology1992102194019481587413
- HouJKEl-SeragHThirumurthiSDistribution and manifestations of inflammatory bowel disease in Asians, Hispanics, and African Americans: a systematic reviewAm J Gastroenterol20091042100210919471256
- di NoiaJSchinkeSPContentoIRDietary fat intake among urban, African American adolescentsEat Behav2008925125618329605
- KugathasanSAmreDInflammatory bowel disease – environmental modification and genetic determinantsPediatr Clin North Am20065372774916873002
- SonnenbergAMcCartyDJJacobsenSJGeographic variation of inflammatory bowel disease within the United StatesGastroenterology19911001431491983816
- AgrezMVValenteRMPierceWMeltonLJ3rdvan HeerdenJABeartRWJrSurgical history of Crohn’s disease in a well-defined populationMayo Clin Proc1982577477527144254
- DeveauxPGKimberlingJGalandiukSCrohn’s disease: presentation and severity compared between black patients and white patientsDis Colon Rectum2005481404140915906124
- StrausWLEisenGMSandlerRSMurraySCSessionsJTCrohn’s disease: does race matter? The Mid-Atlantic Crohn’s Disease Study GroupAm J Gastroenterol20009547948310685754