Abstract
Irritable bowel syndrome (IBS) is a multifactorial condition with principal symptoms of pain and altered bowel function. The kappa-opioid agonist asimadoline is being evaluated in Phase III as a potential treatment for IBS. Asimadoline, to date, has shown a good safety profile and the target Phase III population – diarrhea-predominant IBS patients with at least moderate pain – was iteratively determined in a prospective manner from a Phase II dose-ranging study. The clinical data in support of this population are reviewed in this article. Furthermore, the scientific rationale for the use of asimadoline in the treatment of IBS is reviewed. Considering the high patient and societal burdens of IBS, new treatments for IBS represent therapeutic advances.
Introduction
Irritable bowel syndrome (IBS) remains one of the most common disorders seen by gastroenterologists.Citation1–Citation3 Although IBS itself does not lead to a more sinister pathology, the magnitude and importance of the symptoms associated with IBS result in patients undergoing more surgical procedures in search of other etiologies to explain and treat their symptoms, reduced quality of life, increased health care expenditures, increased work absenteeism, reduced productivity while at work, and increased psychological disorders.Citation3–Citation11 Thus, the burden of IBS on the patient and in terms of societal costs is large. Considering this, finding new, safe, and efficacious treatments for IBS is of large importance both at the patient level and also to reduce the overall burden on the health care system.
IBS has been estimated to have a prevalence of approximately 6%–12% in Western countries.Citation9,Citation12–Citation14 Most studies show IBS to be a disorder predominantly in females, with a female-to-male ratio of 2–2.5 to 1. In many patients, symptoms begin in childhood or young adulthood, and often continue throughout their lives with an episodic course of exacerbations and remissions.
The principal symptoms of IBS are abdominal pain and altered bowel function.Citation15 The alterations in bowel function may manifest as diarrhea, constipation, or an alternation between the two bowel states. These abnormal bowel patterns have led to subtyping of IBS as diarrhea-predominant IBS (D-IBS), constipation-predominant IBS (C-IBS), and mixed or alternating IBS (A-IBS).Citation15 As discussed later in this review, the abdominal pain associated with IBS is a consequence of a state of heightened visceral nociception.Citation15
Effective treatments for IBS need to improve both abdominal pain and abnormal bowel patterns. To date, few contemporary agents have obtained regulatory approval for the treatment of IBS. In considering a reasonable profile for future IBS treatments, several features should be noted. First, there should not be the expectation that a single agent will be efficacious in more than one subtype of IBS. Present-day agents have been shown to be efficacious in only one IBS subtype, reflecting that improvement by the same agent for states of both diarrhea and constipation is unlikely. This presents challenges for the treatment of the A-IBS population. Some have proposed to study A-IBS patients in either their diarrhea or their constipated states, and then combine those populations with either D-IBS or C-IBS patients for indications of nonconstipated IBS patients or constipated IBS patients, respectively. We believe that to achieve these indications, it would be most appropriate to have completed long-term safety information both in D-IBS or C-IBS patients and in an all-comer population of A-IBS patients. A-IBS patients in their diarrheal phase will eventually alternate from their state of diarrhea to constipation; therefore, an all-comer A-IBS population should be used in safety studies. Second, effective IBS treatments must treat abdominal pain. Agents that treat only abnormal bowel function in IBS patients may be classified as laxatives or antidiarrheals, but are not IBS treatments just because they treat abnormal bowel function in IBS patients. Third, in evaluating datasets from randomized, placebo-controlled IBS studies, relevant subgroups should be considered. For all datasets in IBS patients, analyses should be conducted on patients stratified by gender and IBS subtype. Depending on the specific agent, other prespecified analyses may include efficacy by baseline pain. Finally, duration of action ideally should persist as long as treatment does. Some agents show a dissipation of effect with continued treatment. However, this latter point has not been and is not an absolute barrier to drug approval.
When evaluating currently available therapeutic options for the treatment of IBS, few drugs have regulatory approval. For D-IBS patients, alosetron remains the gold standard therapy with respect to drug efficacy. Alosetron shows excellent efficacy in the treatment of multiple symptoms of IBS in diarrhea-predominant patients.Citation16,Citation17 Most notably, improvement is seen on adequate relief of IBS pain and discomfort, urgency, stool consistency, and stool frequency. However, the potential use of alosetron will always be limited by its safety profile. With alosetron, significant constipation occurred in approximately 25% of the patients enrolled in clinical trials.Citation17 Constipation was responsible for the withdrawal of approximately 10% of patients from clinical trials,Citation17 and ischemic colitis was also reported in association with the use of alosetron.
The only other agent for which regulatory approval for D-IBS has been sought in contemporary time is rifaximin. Rifaximin shows marginal efficacy, with differences of rifaximin over placebo in the two pivotal studies of approximately 9% on the primary endpoint.Citation18,Citation19 Evaluation of abdominal pain also showed benefit of less than a 10% difference with rifaximin as compared with placebo. For several endpoints, efficacy with rifaximin dissipated over time in the 10-week observation period following 2 weeks of dosing. The initial new drug application (NDA) for rifaximin in the treatment of IBS was rejected due to lack of long-term safety or repeat-use data.
At the time of the writing of this manuscript, the kappa-opioid agonist asimadoline is in Phase III development for the treatment of D-IBS patients. The available data on asimadoline as a potential treatment for IBS are reviewed in this manuscript.
For the treatment of C-IBS, tegaserod showed benefit on multiple symptoms in C-IBS patients,Citation20,Citation21 but tegaserod was ultimately withdrawn from marketing because of cardiovascular safety concerns. Lubiprostone is indicated for the treatment of patients with C-IBS. Efficacy with lubiprostone is not robust, with differences on the primary endpoint as compared with placebo of 7.8% (17.9% vs 10.1%).Citation22 Evaluation of data during the individual months of treatment showed significance in one Phase III study only at month 2, and in the other study at months 2 and 3. Magnitudes of improvement in pain were not clinically relevant.
Based on the publicly available data, we believe that linaclotide for the treatment of C-IBS will achieve regulatory approval. Linaclotide shows statistically significant benefit on multiple endpoints including bowel movement frequency, pain, straining, bloating, and stool consistency.Citation23
Asimadoline: a peripherally restricted kappa-opioid receptor agonist
For a putative opioid agonist or antagonist, the importance of selectivity across opioid class receptors should not be underestimated. The effects and side effects of centrally active analgesic mu-opioid receptor agonists, such as euphoria, respiratory depression, tolerance, dependence, and withdrawal, can be significant, especially if agents are used as chronic treatments. Peripherally restricted mu-opioid receptor agonists (eg, loperamide) are powerful antidiarrheal agents but do not show convincing analgesic activity.Citation24 The kappa-opioid receptor agonist asimadoline, by contrast, produces both analgesic and antidiarrheal effects presumably via an action in the periphery. Activity in the central nervous system (CNS) is not necessary for efficacy of asimadoline in the treatment of IBS. When kappa-opioid agonists penetrate the CNS at sufficient levels, they do not produce the mu-like opioid side effects of respiratory depression or euphoria; however, kappa receptor activation in the CNS results in other undesirable adverse effects such as dysphoria, sedation, and diuresis.Citation25 In the study of IBS, low levels of asimadoline are used such that these side effects do not occur.
Receptor binding and functional assays performed with asimadoline reveal it to be a potent, full agonist at kappa-opioid receptors.Citation26 A half-maximum inhibitory concentration (IC50) of 1.2 nM (Ki, 0.6 nM) was determined in radioligand binding assays using human recombinant kappa-opioid receptors expressed in CHO cells. Studies in preclinical species revealed a similar high-affinity binding of asimadoline at guinea pig brain kappa receptors (IC50, 3–6 nM). Asimadoline is a potent, full agonist at kappa-opioid receptors in functional assays using rabbit vas deferens and guinea pig ileum.
Asimadoline is highly selective for kappa-opioid receptors, having approximately 400- to 500-fold lower affinity for recombinant human mu-opioid (IC50, 601 nM; Ki, 216 nM) or delta-opioid (IC50, 597 nM; Ki, 313 nM) receptors expressed in CHO cells.Citation26 Studies in preclinical species revealed a similar high degree of selectivity for kappa receptors. Asimadoline is also highly specific, demonstrating no affinity below the micromolar range for any other receptor tested. Although arylacetamide kappa-opioid receptor agonists have been shown to block sodium channels at high concentrations,Citation27 asimadoline is 500- to 1000-fold less potent in this activity than it is as a kappa-opioid receptor agonist,Citation28 which makes it highly unlikely that this activity has any relevance to the clinical effect of the drug at the IBS dose.
Following oral administration to rats, dogs, or monkeys, asimadoline is rapidly absorbed with a time to maximum plasma concentrations (Tmax) of 0.25 to 1 hour and an absolute oral bioavailability of 6%–20%.Citation26,Citation29 The drug is distributed with a half-life of 2–3 hours and has a terminal elimination half-life of 15–20 hours; steady state for twice-daily (bid) treatment occurs after 2–3 days (Tioga Pharmaceuticals, Inc, unpublished data). In humans following oral administration of single doses of 0.15–15 mg, bioavailability is approximately 50%; maximum plasma concentrations (Cmax) are seen after 0.8–1.4 hours, and both Cmax and area under the curve (AUC) increased in a dose-proportional manner (Tioga Pharmaceuticals, Inc, unpublished data).Citation30
Preclinical studiesCitation26,Citation29 demonstrate that the distribution of asimadoline into tissues and organs is rapid, with concentrations several-fold higher than plasma in the liver, kidney, and lung. In contrast, less than 1% of total tissue concentration was found in the brain 1 hour following either single intravenous or oral doses.Citation29 This very limited penetration of asimadoline into the CNS is in part due to its amphiphilic chemical structure, which limits its penetration across the blood-brain barrier, and in part because it is a substrate for P-glycoprotein (P-gp).Citation26,Citation29 Importantly, studies performed in nonclinical speciesCitation31 and in man (Tioga Pharmaceuticals, Inc, unpublished data) have shown only minor increases in asimadoline exposure in the presence of powerful P-gp inhibitors; therefore, the risk from drug-drug interactions with drugs that are P-gp inhibitors is considered negligible.
Clinical pharmacodynamic studies in healthy volunteers provide further strong evidence for the limited CNS penetration of asimadoline. Diuresis is a class effect of kappa agonists in animals and humans mediated via actions both within the blood-brain barrier at the hypothalamic-neurohypophyseal nerve terminal to inhibit release of antidiuretic hormone (ADH) and via a direct action in the kidney.Citation32–Citation35 In a placebo-controlled crossover studyCitation36 of the effect of asimadoline on renal function in healthy volunteers, 5 mg and 10 mg single doses of asimadoline led to an increase in free water excretion (150–200 mL over the 4-hour collection period post dose) without effect on urinary electrolytes. There was no concomitant inhibition of plasma ADH, suggesting that this aquaretic effect was not mediated centrally. However, under stimulated conditions of osmotic challenge, an inhibition of the enhanced plasma ADH was observed at the 10 mg dose, suggesting CNS activity of asimadoline at the 10 mg dose, 20-fold higher than the IBS dose.
A drug interaction study investigating the coadministration of asimadoline with the P-gp and CYP3A4 inhibitor ketoconazole was performed in healthy volunteers (Tioga Pharmaceuticals, Inc, unpublished data). Single (1.5 mg) and multiple (1.5 mg bid for 6 days) doses of asimadoline were administered in the presence of steady-state ketoconazole (200 mg bid for duration of a 10-day study). Assessment of potential CNS-mediated effects of asimadoline was made using several pharmacodynamic endpoints. A modest, two-to three-fold increase in AUC and Cmax of asimadoline was observed with concomitant administration of ketoconazole. However, even in the presence of this enhanced exposure, equivalent to eight times the Cmax reached during 0.5 mg bid dosing (the target IBS dose), there were no effects upon any of the measured CNS endpoints. It was concluded that the threshold for CNS effects of asimadoline is at least ten-fold higher than drug levels achieved in the IBS setting, in good agreement with the experience from clinical safety and efficacy studies performed to date.
Visceral analgesic and antihyperalgesic actions
Kappa-opioid receptors are members of the superfamily of inhibitory GTP-binding regulatory protein (G protein)- coupled receptors, which activate potassium channels, inhibit calcium channels, and inhibit adenylate cyclase activity, all resulting in an inhibition of neuronal excitability.Citation37–Citation39 Kappa-opioid receptors are thought to be located on the terminals of a variety of neurons, including those extrinsic visceral afferent neurons that transmit sensory signals from the gut to the CNS.Citation40–Citation45 A broad literatureCitation46 describes a peripherally mediated, visceral analgesic and antihyperalgesic activity of kappa-opioid receptor agonists.
The fundamental mechanism of action for production of the visceral analgesic effect of kappa-opioid receptor agonists is an inhibition of the excitability of visceral afferent nerve terminals in the gut wall, causing a reduction of action potential firing and neurotransmitter release from those sensory nerves.Citation46 An action in the CNS does not appear to be necessary for visceral analgesia with kappa-opioid receptor agonists.Citation41–Citation43 However, the presence of visceral hypersensitivity is thought to be important for optimum visceral analgesic effect of kappa-opioid receptor agonists.Citation45,Citation47,Citation48 The analgesic potency of asimadoline is increased in visceral pain models in the presence of visceral hypersensitivity.Citation47,Citation48 Previous studies in somatic pain models demonstrated that the potency of asimadoline’s analgesic effect is higher following the induction of hyperalgesia.Citation26 Such antihyperalgesic effects may be produced by asimadoline’s abilities to reduce expression of substance P and calcitonin gene-related peptide in dorsal root ganglia (DRG) neurons in chronic hyperalgesia and to inhibit plasma extravasation and the release of neurogenic inflammatory mediators.Citation26,Citation49,Citation50
Recently, data from studies of peripheral sensory nerves (trigeminal ganglion) in rats suggest that peripheral kappa-opioid receptors require stimuli associated with sensitization processes to become functional.Citation51 Such induction of “ functional competence” of kappa-opioid receptors by sensitizing agents (eg, bradykinin) involves the phospholipase C pathway, arachidonic acid metabolism, and membrane integrins. Earlier work described kappa-opioid receptors in peripheral sensory nerves as dormant “silent” receptors, showing that neuronal depolarization stimulates kappa-opioid receptor mRNA expression, axonal transport, and protein translation in DRG neurons.Citation52–Citation55 The authors described a membrane depolarization-induced de novo synthesis of kappa-opioid receptors in DRG that was mediated by a netrin-1-induced translocation of mRNA to the transcriptionally active polyribosomal fraction. The effect was dependent on calcium influx via L-type calcium channels, and Copb1-dependent trafficking of mRNA along axons was also demonstrated. Such neuronal activity-dependent and/or sensitization-dependent increases in kappa-opioid receptor expression and function may underlie the preferential efficacy of asimadoline in hypersensitive states both in animal models and in man.
Pharmacodynamic studies with asimadoline also suggest a preferential efficacy against visceral pain in patients with visceral hypersensitivity. Delvaux et alCitation45 evaluated asimadoline for potential analgesic activity in IBS patients with significant pain symptoms and demonstrated visceral hypersensitivity (pain threshold ≤32 mmHg). The crossover study design compared the effect of single doses of placebo with 0.5 mg asimadoline upon distensions over a range of pressures up to 45 mmHg. Asimadoline produced a significant reduction of the AUC of pain intensity (rated at each distension step) and a small but nonsignificant increase in pain threshold, compared with placebo. No effect on colonic compliance or perception of nonpainful distensions was observed. Delgado-Aros et alCitation56 performed similar barostat studies in healthy volunteers. The parallel-group study compared single doses of placebo with 0.15 mg, 0.5 mg, and 1.5 mg asimadoline. Colonic distensions at 8 mmHg, 16 mmHg, 24 mmHg, and 32 mmHg were rated for gas and pain perception scores using a 100 mm visual analogue scale (VAS). Although pain scores were lower in the 0.5 mg dose group at all distension levels, the differences were not statistically significant, including at the two higher pressure distension levels, which elicited pain scores of 40–50 mm on the VAS, suggesting that kappa receptor activation does not significantly inhibit moderate to high-level noxious sensations in health. Asimadoline at 0.5 mg and 1.5 mg had mixed inhibitory or excitatory effects on low-threshold gas and pain sensations in response to low pressure (8 mmHg and 16 mmHg) distension, which were scored below 35 mm on the VAS. This suggests a potential role for kappa receptors in modulation of less noxious sensations in the “nonsensitized” state of health. The findings from these two studies correlate with the clinical experience gained to date from efficacy and safety studies with asimadoline, in which efficacy against symptoms of IBS is greatest in patients with a higher symptom burden.Citation57
Antidiarrheal actions
Kappa receptors are found on cholinergic terminals of enteric neurons of the myenteric plexus where they inhibit cholinergic transmission and inhibit propulsive motility when studied in vitro.Citation58,Citation59 However, there is a paucity of data concerning any role of kappa-opioid receptors in gastrointestinal secretion. Immunohistochemistry studies in gastrointestinal tissues from pig,Citation60 rat,Citation61 and guinea pigCitation62 demonstrate a preferential distribution of kappa-opioid receptors in the myenteric plexus, with either low or no immunoreactivity found in submucous plexus neurons where mu-opioid receptors predominate. However, in mice the opposite distribution has been described for kappa-opioid receptors, along with an up-regulation of these receptors in the submucous plexus during inflammation.Citation63 Asimadoline has no effect on normal gastrointestinal transit in the small intestine in miceCitation26 or on colonic transit or postprandial motility in healthy normal volunteers,Citation56 but inhibits stress-induced fecal output in rats (Tioga Pharmaceuticals, Inc, unpublished data) and reduces diarrhea in D-IBS patients without producing constipation.Citation57 Thus, although kappa-opioid receptors are found in the ENS, they do not appear to be critical mediators of normal motility and secretory processes in the normal state. The lack of a constipating effect of kappa receptor agonists in D-IBS may be due to their preferential localization in the myenteric plexus such that secretory processes are not inhibited; in addition, their presynaptic localization may allow for a more subtle modulation of motility in contrast to the stronger inhibitory influence on both motility and secretion produced by the broader localization of mu-opioid receptors both presynaptically and on cell bodies of both myenteric and submucosal plexus neurons.Citation60–Citation62 In addition, a similar reliance upon a hypersensitizing stimulus for receptor functionality, as described above for peripheral sensory nerves, may exist in the ENS, especially in the submucous plexus.Citation63
It is also possible that the effect of asimadoline on sensitized gastrointestinal transit may also be mediated by a non-ENS site of action. Several studies have demonstrated altered postprandial motility and symptoms in functional bowel disorder patients. Of note in D-IBS patients are increased small bowel motility,Citation64 faster orocecal transit,Citation65 faster ileocolonic transit,Citation66 increased colonic motility index, greater number of high amplitude propagating contractions and shortened colonic transit time,Citation67 and increase in meal-related or postprandial symptoms.Citation68 Such enhanced “gastrocolic” responses may be the result of hypersensitivity in the extrinsic vagal and or spinal nerves that mediate these reflexes, and inhibition of these enhanced reflexes is an interesting potential mechanism of action for asimadoline in the reduction of diarrhea and other symptoms in these patients.
Clinical trials with asimadoline in the treatment of IBS
Based on the results of the barostat study in IBS patients,Citation45 a randomized, multicenter, placebo-controlled, dose-ranging IBS trial was conducted with asimadoline.Citation59,Citation69 This Phase IIb trial enrolled approximately 600 patients, including patients with all three IBS subtypes, as well as male and female IBS patients. Prospectively defined subgroup analyses were done by degree of baseline pain, as well as by gender and IBS subtype.
In the intent-to-treat population, asimadoline at doses of 0.15 mg, 0.5 mg, or 1.0 mg was given bid and no dose level distinguished itself from placebo (bid). Following the prospectively planned analysis scheme, numerically and statistically significant benefit was seen with all doses of asimadoline in patients with higher levels of baseline pain.Citation57,Citation69 One-third of the patients who entered the trial with the highest level of baseline pain showed excellent benefit on multiple endpoints. Similar benefit was seen in both genders, but efficacy was driven by D-IBS patients. Thus, the Phase IIb study identified a target population for progression into Phase III of male and female D-IBS patients who had more severe pain at baseline. For ease of recruitment into the Phase III program, the target population became D-IBS patients with at least moderate pain at baseline. Analyses of this population from the Phase IIb data yielded excellent efficacy results on pain scores (), stool frequency (), pain-free days, urgency, bloating, and adequate relief.Citation57
Figure 1 Effects of asimadoline on pain scores in D-IBS patients with at least moderate pain at baseline: asimadoline (asi) and placebo were administered twice daily for up to 12 weeks. Pain scores were collected daily and averaged numerically on a weekly basis. Week 0 represents the 2-week baseline period. As is apparent, with 0.5 mg and 1.0 mg dose levels, a substantial reduction in pain occurred, compared with placebo. Copyright © 2008. Reproduced with permission from Alimentary Pharmacology & Therapeutics. Mangel AW, Bornstein JD, Hamm LR, et al. Clinical trial: asimadoline in the treatment of patients with irritable bowel syndrome. Aliment Pharmacol Ther. 2008;28(2):239–249.
Abbreviation: D-IBS, diarrhea-predominant irritable bowel syndrome.
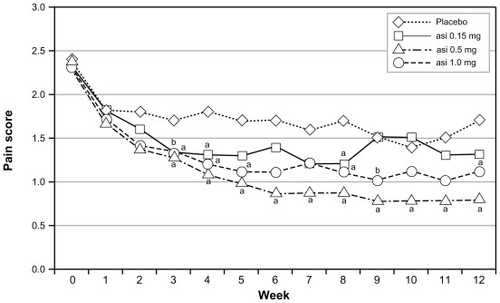
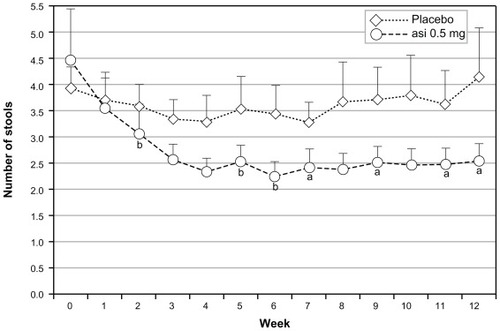
Figure 2 Effects of asimadoline (asi) on stool frequency in D-IBS patients with at least moderate pain at baseline: asimadoline (0.5 mg) and placebo were administered twice daily for up to 12 weeks. Stool frequency was collected daily and averaged numerically on a weekly basis. Week 0 represents the 2-week baseline period. As is apparent, with the 0.5 mg dose level a substantial reduction in stool frequency occurred, compared with placebo.
Abbreviation: D-IBS, diarrhea-predominant irritable bowel syndrome.
By contrast to the above study, a single-center study that analyzed data on the basis of on-demand or as-needed use did not show efficacy of asimadoline.Citation70 The reason for the lack of efficacy is unclear.
Asimadoline has an extensive safety database.Citation69,Citation71 More than 1000 humans have been exposed to asimadoline in clinical trials. Single doses of asimadoline as high as 15 mg and repeat doses up to 10 mg administered daily for up to 8 weeks have been evaluated in various Phase I and Phase II studies. With the dosage level being evaluated in the Phase III asimadoline program, 0.5 mg bid, a very good safety profile has been observed (). Significantly, for a drug intended to treat D-IBS patients, no increase in constipation was reported. The most common adverse events seen in the Phase IIb IBS trial are shown in for the efficacy population being evaluated in Phase III. Constipation is once again included, as it is a significant adverse event to consider in D-IBS patients. No safety signals were observed.
Table 1 Most common adverse events seen in nonirritable bowel syndrome asimadoline trials
Table 2 Most common adverse events in Phase IIb irritable bowel syndrome asimadoline trial among D-IBS patients with at least moderate pain at baseline
Conclusion
Treatment of patients with IBS remains a perplexing problem. Several confounding factors contribute to the difficulties in developing therapeutics. IBS is a multifactorial condition with principal symptoms of pain and altered bowel function. Pain is always a difficult symptom to treat. Furthermore, IBS is subtyped into three principal groups, and the likely scenario is that the same medication will not work for more than one subtype of patients because of the difference in the type of bowel dysfunction. Additionally, although there are pharmacodynamic models by which to study transit and pain, there is no true animal model of IBS against which candidate therapeutics can be tested.
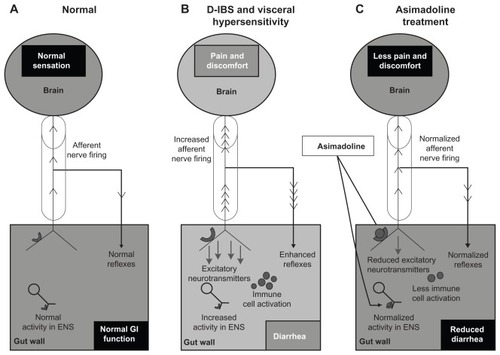
The kappa-opioid agonist asimadoline represents a potential treatment for IBS. Asimadoline, to date, has a good safety profile, and the target population showing strong efficacy was iteratively dissected from the Phase IIb data to optimize the likelihood of success in Phase III. There is a sound scientific basis for use of asimadoline in the treatment of IBS. Although an action of asimadoline in the ENS cannot be excluded, one potential mechanism of action that may explain all of the effects of asimadoline (on sensory and bowel function symptoms) in IBS is the activation of up-regulated kappa-opioid receptors on hypersensitive extrinsic afferent nerve terminals in the gut wall (). This may result in (1) reduced sensory output from the gut to the spinal cord and brain, thereby directly inhibiting sensory symptoms and reducing augmented local motility reflexes that may contribute to sensory symptoms and diarrhea, and (2) reduced neurotransmitter release in the gut wall, which may lead to reduced diarrhea and potentially to a reduced level of peripheral, and subsequently central, sensitization in the brain–gut axis.
Figure 3 Proposed mechanism of action of asimadoline in the treatment of D-IBS. (A) The “brain–gut” axis in the normal state (health). Sensory information is conveyed to the brain via the spinal cord (cylinder) by extrinsic VAN. Local reflexes and descending regulatory input from the CNS via autonomic efferent nerves (not shown) control overall gut function. Normal secretomotor function is coordinated by the ENS. (B) Visceral hypersensitivity in D-IBS drives increased activity in VAN resulting in increased sensory signaling to the brain and enhanced local reflexes, contributing to diarrhea. The accompanying transmitter release into the gut wall results in increased ENS activity (leading to diarrhea) and immune cell activation, which heightens sensitization. Kappa receptor expression on VAN terminals is up-regulated due to sensitization. (C) Asimadoline activates kappa-opioid receptors on VAN, leading to reduced sensory input to the brain, reduced local reflexes, and reduced transmitter release. Asimadoline also acts presynaptically to reduce neurotransmitter release in the ENS. Pain, diarrhea, and visceral hypersensitivity are reduced.
Disclosure
During the past year, A Mangel has participated in projects for the following sponsors: C-Path Institute, Tucson, AZ; Tioga Pharmaceuticals, San Diego, CA; Theravance, South San Francisco, CA; Novartis International AG, Basel, Switzerland; GlaxoSmithKline (GSK), London, UK; Pfizer, NY; and Boehringer, Binger Str, Ingelheim, Germany. A Mangel is an employee of RTI Health Solutions, Research Triangle Park, NC. RTI Health Solutions met the costs for preparation of this manuscript. G Hicks is an employee of Tioga Pharmaceuticals.
References
- EverhartJERenaultPFIrritable bowel syndrome in office-based practices in the United StatesGastroenterology1991100499810052001837
- RussoMWGaynesBNDrossmanDAA national survey of practice patterns of gastroenterologists with comparison to the past two decadesJ Clin Gastroenterol199229433934310599638
- MayerEAClinical practice. Irritable bowel syndromeN Engl J Med2008358161692169918420501
- WatsonMELaceyLKongSAlosetron improves quality of life in women with diarrhea-predominant irritable bowel syndromeAm J Gastroenterol200196245545911232690
- WellsNEHahnBAWhorwellPJClinical economics review: irritable bowel syndromeAliment Pharmacol Ther1997116101910309663824
- WhiteheadWEBurnettCKCookEWIIITaubEImpact of irritable bowel syndrome on quality of lifeDig Dis Sci19964111224822538943980
- CorneyRHStantonRPhysical symptom severity, psychological and social dysfunction in a series of outpatients with irritable bowel syndromeJ Psychosom Res19903454834912231481
- HahnBAYanSStrasselsSImpact of irritable bowel syndrome on quality of life and resource use in the United States and United KingdomDigestion199960177819892803
- AndrewsEBEatonSCHollisKAPrevalence and demographics of irritable bowel syndrome: results from a large web-based surveyAliment Pharmacol Ther2005221093594216268967
- PatelRPPetittaAFogelAPetersonEZarowitzBJThe economic impact of irritable bowel syndrome in a managed care settingJ Clin Gastroenterol2002351142012080220
- LevyRLVon KorffMWhiteheadWECosts of care for irritable bowel syndrome in a health maintenance organizationAm J Gastroenterol200196113122312911721759
- SandlerRSEpidemiology of irritable bowel syndrome in the United StatesGastroenterology19909924094152365191
- DrossmanDALiZAndruzziEU.S. householder survey of functional gastrointestinal disorders. Prevalence, sociodemography, and health impactDig Dis Sci1993389156915808359066
- HunginAPWhorwellPJTackJMearinFThe prevalence patterns and impact of irritable bowel syndrome: an international survey of 40,000 subjectsAliment Pharmacol Ther200317564365012641512
- LongstrethGFThompsonWGCheyWDHoughtonLAMearinFSpillerRCFunctional bowel disordersDrossmanDACorazziariEDelvauxMRome III: The Functional Gastrointestinal DisordersMcLean, VADegnon Associates Inc2006
- MangelAWNorthcuttARReview article: the safety and efficacy of alosetron, a 5-HT3 receptor antagonist, in female irritable bowel syndrome patientsAliment Pharmacol Ther199913Suppl 2778210429745
- CamilleriMCheyWYMayerEAA randomized controlled clinical trial of the serotonin type 3 receptor antagonist alosetron in women with diarrhea-predominant irritable bowel syndromeArch Int Med2001161141733174011485506
- PimentelMLemboACheyWDfor TARGET Study GroupRifaximin therapy for patients with irritable bowel syndrome without constipationN Eng J Med201136412232
- PimentelMLemboACheyWDfor TARGET Study GroupRifaximin therapy for patients with irritable bowel syndrome without constipationN Eng J Med20113641 Supplementary Appendix
- TackJMüller-LissnerSBytzerPA randomised controlled trial assessing the efficacy and safety of repeated tegaserod therapy in women with irritable bowel syndrome with constipationGut200554121707171316020489
- Müller-LissnerSAFumagalliIBardhanKDTegaserod, a 5-HT(4) receptor partial agonist, relieves symptoms in irritable bowel syndrome patients with abdominal pain, bloating and constipationAliment Pharmacol Ther200115101655166611564007
- DrossmanDACheyWDJohansonJFClinical trial: lubiprostone in patients with constipation-associated irritable bowel syndrome – results of two randomized, placebo-controlled studiesAliment Pharmacol Ther200929332934119006537
- JohnstonJMKurtzCBMacdougallJELinaclotide improves abdominal pain and bowel habits in a phase IIb study of patients with irritable bowel syndrome with constipationGastroenterology201013961877188620801122
- American College of Gastroenterology Task Force on Irritable Bowel SyndromeBrandtLJCheyWDFoxx-OrensteinAEAn evidence- based position statement on the management of irritable bowel syndromeAm J Gastroenterol2009104Suppl 1S1S3519521341
- WalshSLStrainECAbreuMEBigelowGEEnadoline, a selective kappa opioid agonist: comparison with butorphanol and hydromorphone in humansPsychopharmacology (Berl)2001157215116211594439
- BarberABartoszykGDBenderHMA pharmacological profile of the novel, peripherally-selective kappa-opioid receptor agonist, EMD 61753Br J Pharmacol19941134131713277889287
- SuXJoshiSKKardosSGebhartGFSodium channel blocking actions of the kappa-opioid receptor agonist U50,488 contribute to its visceral antinociceptive effectsJ Neurophysiol20028731271127911877501
- JoshiSKLambKBielefeldtKGebhartGFArylacetamide kappa-opioid receptor agonists produce a tonic- and use-dependent block of tetrodotoxin-sensitive and -resistant sodium currents in colon sensory neuronsJ Pharmacol Exp Ther2003307136737212954815
- JonkerJWWagenaarEvan DeemterLRole of blood-brain barrier P-glycoprotein in limiting brain accumulation and sedative side-effects of asimadoline, a peripherally acting analgesic drugBr J Pharmacol19991271435010369454
- BarberAGottschlichRNovel developments with selective, nonpeptidic kappa-opioid receptor agonistsExpert Opin Investig Drugs199761013511368
- BenderHMDasenbrockJBrain concentrations of asimadoline in mice: the influence of coadministration of various P-glycoprotein substratesInt J Clin Pharmacol Ther199836276799520149
- SlizgiGRLudensJHStudies on the nature and mechanism of the diuretic activity of the opioid analgesic ethylketocyclazocineJ Pharmacol Exp Ther198222035855916121047
- RimoyGHBhaskarNKWrightDMRubinPCMechanism of diuretic action of spiradoline (U-62066E) – a kappa-opioid receptor agonist in the humanBr J Clin Pharmacol19913256116151659438
- BrooksDPGiardinaGGellaiMOpiate receptors within the blood-brain barrier mediate kappa agonist-induced water diuresisJ Pharmacol Exp Ther199326611641718392549
- AshtonNBalmentRJBlackburnTPKappa-opioid-receptor agonists modulate the renal excretion of water and electrolytes in anaesthetized ratsBr J Pharmacol19909911811852158834
- KramerHJUhlWLadstetterBBäckerAInfluence of asimadoline, a new kappa-opioid receptor agonist, on tubular water absorption and vasopressin secretion in manBr J Clin Pharmacol200050322723510971307
- JordanBDeviLAMolecular mechanisms of opioid receptor signal transductionBr J Anaesth199881112199771268
- NorthRAOpioid receptor types and membrane ion channelsTrends Neurosci19869114117
- HerzAPeripheral opioid analgesia – facts and mechanismsProg Brain Res1996110951049000718
- DiopLRivièrePJPascaudXJunienJLPeripheral kappa-opioid receptors mediate the antinociceptive effect of fedotozine (correction of fetodozine) on the duodenal pain reflex in ratEur J Pharmacol1994271165717698213
- HaradaYNishiokaKKitahataLMNakataniKCollinsJGContrasting actions of intrathecal U50, 488H, morphine, or [D-Pen2, D-Pen5] enkephalin or intravenous U50, 488H on the visceromotor response to colorectal distension in the ratAnesthesiology19958323363437631956
- DanzebrinkRMGreenSAGebhartGFSpinal mu and delta, but not kappa, opioid-receptor agonists attenuate responses to noxious colorectal distension in the ratPain199563139478577489
- SenguptaJNSuXGebhartGFKappa, but not mu or delta, opioids attenuate responses to distention of afferent fibers innervating the rat colonGastroenterology199611149689808831591
- SuXSenguptaJNGebhartGFEffects of kappa-opioid receptor-selective agonists on responses of pelvic nerve afferents to noxious colorectal distensionJ Neurophysiol1997782100310129307130
- DelvauxMBeckAJacobJEffect of asimadoline, a kappa opioid agonist, on pain induced by colonic distension in patients with irritable bowel syndromeAliment Pharmacol Ther200420223724615233705
- RivièrePJPeripheral kappa-opioid agonists for visceral painBr J Pharmacol200414181331133415051626
- SenguptaJNSniderASuXGebhartGFEffects of kappa opioids in the inflamed rat colonPain1999792–317518510068163
- BurtonMBGebhartGFEffects of kappa-opioid receptor agonists on responses to colorectal distension in rats with and without acute colonic inflammationJ Pharmacol Exp Ther199828527077159580617
- WalkerJSScottCBushKAKirkhamBWEffects of the peripherally selective kappa-opioid asimadoline, on substance P and CGRP mRNA expression in chronic arthritis of the ratNeuropeptides2000343–419320211021980
- BinderWScottCWalkerJSInvolvement of substance P in the anti-inflammatory effects of the peripherally selective kappa-opioid asimadoline and the NK1 antagonist GR205171Eur J Neurosci19991162065207210336675
- BergKARowanMPSanchezTARegulation of κ-opioid receptor signaling in peripheral sensory neurons in vitro and in vivoJ Pharmacol Exp Ther20113381929921487072
- BiJTsaiNPLinYPLohHHWeiLNAxonal mRNA transport and localized translational regulation of kappa-opioid receptor in primary neurons of dorsal root gangliaProc Natl Acad Sci U S A200610352199191992417167054
- BiJTsaiNPLuHYLohHHWeiLNCopb1-facilitated axonal transport and translation of kappa opioid-receptor mRNAProc Natl Acad Sci U S A200710434138101381517698811
- TsaiNPBiJLohHHWeiLNNetrin-1 signaling regulates de novo protein synthesis of kappa opioid receptor by facilitating polysomal partition of its mRNAJ Neurosci200626389743974916988045
- TsaiNPBiJWeiLNThe adaptor Grb7 links netrin-1 signaling to regulation of mRNA translationEMBO J20072661522153117318180
- Delgado-ArosSChialHJCamilleriMEffects of a kappa-opioid agonist, asimadoline, on satiation and GI motor and sensory functions in humansAm J Physiol Gastrointest Liver Physiol20032844G558G56612631557
- MangelAWBornsteinJDHammLRClinical trial: asimadoline in the treatment of patients with irritable bowel syndromeAliment Pharmacol Ther200828223924918466359
- ChamouardPKleinAMartinEAdloffMAngelFRegulatory role of enteric kappa opioid receptors in human colonic motilityLife Sci19935314114911568103909
- GiulianiSLecciATramontanaMMaggiCARole of kappa opioid receptors in modulating cholinergic twitches in the circular muscle of guinea-pig colonBr J Pharmacol199611959859898922749
- PoonyachotiSKulkarni-NarlaABrownDRChemical coding of neurons expressing delta- and kappa-opioid receptor and type I vanilloid receptor immunoreactivities in the porcine ileumCell Tissue Res20023071233311810311
- BagnolDMansourAAkilHWatsonSJCellular localization and distribution of the cloned mu and kappa opioid receptors in rat gastrointestinal tractNeuroscience19978125795919300443
- SterniniCPatiernoSSelmerISKirchgessnerAThe opioid system in the gastrointestinal tractNeurogastroenterol Motil200416Suppl 231615357847
- PolOPalacioJRPuigMMThe expression of delta- and kappa-opioid receptor is enhanced during intestinal inflammation in miceJ Pharmacol Exp Ther2003306245546212724348
- KellowJEPhillipsSFAltered small bowel motility in irritable bowel syndrome is correlated with symptomsGastroenterology1987926188518933569764
- MarcianiLCoxEFHoadCLPostprandial changes in small bowel water content in healthy subjects and patients with irritable bowel syndromeGastroenterology2010138246947719909743
- DeiterenACamilleriMBurtonDMcKinzieSRaoAZinsmeisterAREffect of meal ingestion on ileocolonic and colonic transit in health and irritable bowel syndromeDig Dis Sci201055238439119949866
- CheyWYJinHOLeeMHSunSWLeeKYColonic motility abnormality in patients with irritable bowel syndrome exhibiting abdominal pain and diarrheaAm J Gastroenterol20019651499150611374689
- BouchouchaMDevroedeGRaynaudJJBonCBejouBBenamouzigRIs the colonic response to food different in IBS in contrast to simple constipation or diarrhea without abdominal pain?Dig Dis Sci201156102947295621479817
- MangelAWWilliamsVSAsimadoline in the treatment of irritable bowel syndromeExpert Opin Investig Drugs2010191012571264
- SzarkaLCamilleriMBurtonDEfficacy of on-demand asimadoline, a peripheral k-opioid agonist, in females with irritable bowel syndromeClin Gastroenterol Hepatol20075111268127517900994
- CamilleriMNovel pharmacology: asimadoline, a kappa-opioid agonist, and visceral sensationNeurogastroenterol Motil200820997197918715494