
Abstract
Background
Patients >60 years suffering from non-unions are often unable to perform activities of daily living and often become dependent on nursing care. Evidence regarding treatment options and outcome is nonexistent. This study sought to determine the clinical effectiveness and safety of one- or two-step non-union therapy in elderly patients.
Methods
This study was a single-site retrospective database analysis of older adults with long bone non-unions treated via “diamond concept”. All medical records of patients receiving surgical treatment of non-unions between 01/01/2010 and 31/12/2016 were reviewed. Clinical and radiological outcome subsequent to non-union therapy were evaluated.
Results
A total of 76 patients (37 patients were treated with one-step and 39 patients with Masquelet therapy) suffering from a non-union older than 60 years treated between 01/01/2010 and 31/12/2016 in our institution were included into the current study. Bone consolidation was achieved in 91.9% after one-step and 76.9% after the Masquelet therapy. Analysis of age as a risk factor in the outcome of non-union therapy revealed no significant differences in patients treated with the one-step procedure according to the “diamond concept”. On the contrary, age had a significant negative influence on the outcome of the Masquelet therapy (p = 0.027).
Conclusion
Non-union therapy according to the “diamond concept” is an effective and reliable treatment option in elderly patients. According to findings of the current study, older adults suffering from an infected non-union benefit from a two-stage procedure, whereas in patients suffering from a non-infected non-union, a one-step surgical treatment is beneficial.
Introduction
Fractures of long bones are common in elderly patients (>60 years).Citation1 Patients aged 60 and older have a residual lifetime fracture risk of 29% in males and 56% in females,Citation2 therefore, long bone fractures in older adults are frequent and the prevalence of age-related fractures will increase over the next decades.Citation3 Increasing age leads to substantial physiological changes on a molecular, cellular and systemic level,Citation3 predisposing elderly patients to fractures and subsequent healing complications.Citation3
The prevalence of delayed or non-union is up to 30% in long bone fractures and such healing complications are a burden for both the patient and the healthcare system.Citation1 Older adults have a lower capacity for mesenchymal progenitor stem cell division and differentiation, impaired angiogenesis, and reduced levels of growth factors predisposing them to delayed fracture healing.Citation1,Citation3 Non-union of a fracture results in prolongation of the necessary treatment and significant limitations in the patients’ quality of life.Citation4 Several studies have reported that these complications are more common in the elderly.Citation5,Citation6 Therefore, treatment of non-unions is particularly challenging for surgeons in elderly patients.Citation1,Citation7 Principles in revision surgery are based on the “diamond concept” and may involve one or two stages.Citation7,Citation11 In general, the “diamond concept” states factors that are mandatory for successful bone healing. It was postulated by Giannoudis et al in 2007Citation12 and since then it has been established also for its principles in non-union therapy.Citation13 In particular, the “diamond concept” gives mechanical stability and biological environment equal importance during the successful bone repair responseCitation14 and mandatory factors that have to be provided for a successful non-union therapy are vascularity, osteoinductive factors, osteogenic cells, osteoconductive matrix, and mechanical stability.Citation14 Several studies have shown good clinical results in non-unions treated with the “diamond concept” in various long bones.Citation15,Citation17 However, most of the clinical evidence available so far investigated the clinical outcome of non-union therapy in younger patients. Hence, in this study we sought to determine the clinical effectiveness of one- or two-step non-union therapy based on the “diamond concept” in older adults, and assessed relevant risk factors influencing the outcome of non-union therapy. Therefore, the current study utilized a retrospective database analysis of patients older than 60 that suffered from a non-union of a long bone and were surgically treated. Clinical and radiological outcome of the treatment were evaluated and possible risk factors analyzed.
Materials and Methods
Study Design
This study was designed as a retrospective clinical database study. After obtaining approval from the ethics committee of the University of Heidelberg (S-262/2017), which, due to the nature of the study design and complete anonymization of patient data by physicians, allowed for review of medical records without signed patient consent, all records, operative notes, lab data and radiological imaging of patients that received surgical treatment of non-unions between 01/01/2010 and 31/12/2016 were reviewed regarding patient characteristics, performed surgical procedure, post-operative pain, post-operative weight bearing, mechanical stability, history of infection, and radiological signs of consolidation. The current study was performed in concordance with the Declaration of Helsinki. Patients 60 years or older suffering from non-union of a long bone who underwent surgical treatment in our hospital and participated in our standardized follow-up program for at least 12 months were included in the current study. The cut-off of 60 years of age was in accordance with current WHO guidelines as to what defines an “elderly patient”. Exclusion criteria were the existence of systemic diseases such as hypo- or hyperthyroidism, diabetes mellitus, advanced liver disease, chronic inflammatory diseases, malignancy as well as long-term use of immunosuppressive drugs. Subsequently, patient demographics were stratified to age, sex, BMI, method of osteosynthesis, surgical treatment, anatomical localization, and smoking status. Patients were then assigned to a total of two groups. Specifically, patients that were treated with a one-step surgery were assigned to the first group and patients that were treated with a two-step surgery were assigned to the second group.
Surgical Treatment
Prior to surgical treatment, the type of non-union (atrophic or hypertrophic, based on the local biological microenvironment), defect size, and likelihood of infection were evaluated. While the type of surgery was generally performed at the discretion of the responsible surgeon, smaller aseptic atrophic non-unions (<2 cm in defect size) and hypertrophic non-unions were generally treated with the one-step procedure while larger aseptic atrophic non-unions (>2 cm in defect size) and infected non-unions were treated with the induced membrane or Masquelet therapy.Citation9 During each surgery multiple tissue samples were harvested and analyzed for any type of microbial infection. One-step treatment consists of debridement of the non-union and surrounding avital tissue, de-novo osteosynthesis with a suitable and biomechanically stable implant, filling of the osseous defect with autologous bone graft and occasional application of additional growth factors such as bone morphogenic protein 2 or 7 (3.3 mg BMP-7 or 4 mg BMP-2).Citation18,Citation19
Typically, Masquelet therapy consists of two surgical procedures or steps; however, if an infection is detected the first step is repeated until asepsis is achieved. In detail, the individual steps involve the following aspects:
Step I: removal of any surgical implant, radical debridement of the non-union and surrounding avital soft tissue, filling of the bone defect with a polymethyl-methacrylate (PMMA) spacer impregnated with gentamycin and/or vancomycin,Citation15 de-novo osteosynthesis with a suitable and biomechanically stable implant if asepsis is guaranteed or temporary use of external fixators if any infection is suspected.
Step II: the spacer is left in-situ for 6 weeks to guarantee a fully grown Masquelet-membrane.Citation9 During the second step the spacer is removed carefully while leaving the Masquelet-membrane unimpaired, the bone defect grafted with autologous bone graft, application of growth factors analog to the first step. If an external fixator was used during the first step, it is removed and replaced with a suitable internal implant.
Follow-Up
In order to assess clinical outcome and healing complications, we developed a distinguished follow-up program. In particular, follow-up included radiological and clinical examination postoperatively at 1 and 6 weeks, as well as 3, 6, 12, 24, and 36 months. Follow-up consisted of X-rays and CT-scans (based on medical indication), as well as clinical evaluation of mechanical stability, weight bearing, postoperative pain, and signs of infection by two independent and experienced trauma surgeons. Inclusion in the current study required meticulous participation for a minimum of one year following the last surgical treatment.
Analysis of Radiological and Clinical Outcome
Radiological outcome of non-union therapy was assessed based on available X-rays and CT-scans 12 months subsequent to the final surgical non-union therapy. Available X-rays and CT-scans (only if medically indicated) were evaluated independently by two different experienced and blinded trauma surgeons and non-unions were evaluated as consolidated based on bridging of 3 out of 4 cortices. Clinical evaluation during follow-up comprised clinical examination regarding pain associated with weight bearing and clinical sign of mechanical stability as well as subjective patient history. In addition, risk factors that might influence outcome of non-union therapy (sex, age, history of infection, additional use of growth factors, localization, BMI, and method of osteosynthesis) were assessed using patient history and available clinical data. Pain associated with weight bearing was stratified into 5 categories (no pain associated with weight bearing, pain associated with high physical strain, pain associated with medium physical strain, pain associated with low physical strain, constant pain without physical strain). Generated data were imported into a database for further statistical analysis.
Statistics
Data entry was done with MS Excel, and statistical analysis was performed using SPSS for Windows 10 (SPSS Inc., Chicago, IL, USA). Categorical variables were evaluated using the Chi-squared test and Pearson’s Chi-squared test to assess statistically significant differences in-between groups. Non-parametric test methods were assessed to investigate location shifts between groups (Mann–Whitney U-test). The Wilcoxon signed rank test for paired samples was used to recognize significant changes within both groups. Continuous variables were expressed as absolute mean concentrations ± SD (standard deviation) and the level of significance (α) was set at 5%.
Results
Patient Characteristics
Between 01/01/2010 and 31/12/2016, 264 patients suffering from a non-union older than 60 years were treated in our institution. According to the exclusion criteria, 188 patients had to be excluded from the current study (161 due to missing follow-up, 22 patients were treated with a joint replacement, 5 patients were treated with cortisone) resulting in 76 suitable patients (37 patients were treated with one-step and 39 patients were treated with the Masquelet therapy). Additional data concerning the patient characteristics can be found in .
Table 1 Patient Demographics of All Patients Included in the Study
Analysis of the Outcome of Applied Non-Union Therapy
One year after the one-step procedure 34 patients (91.9%) showed proper consolidation, whereas 3 patients (8.1%) showed no consolidation. Patients that failed to respond to the revision surgery were suffering from tibial (2 patients) and femoral (1 patients) non-unions. In contrast, one year after the Masquelet therapy 30 patients (76.9%) had proper bone healing compared to 9 patients (23.1%) that did not. In particular, patients failing to heal suffered from femoral (7 patients) and tibial (2 patients) non-unions. Differences regarding the outcome between groups were at a non-significant level (p > 0.05) ( and ). Clinical outcome of the applied non-union therapy regarding pain associated with weight bearing showed significant correlation with the radiological consolidation regardless of the utilized treatment (p = 0.015). In particular, patients that were radiologically rated as consolidated had less pain compared to patients with persistent non-unions. The method of non-union therapy had no influence on postoperative pain.
Table 2 Patient Demographics of Non-Responders to the Therapy
Evaluation of Age as Risk Factor
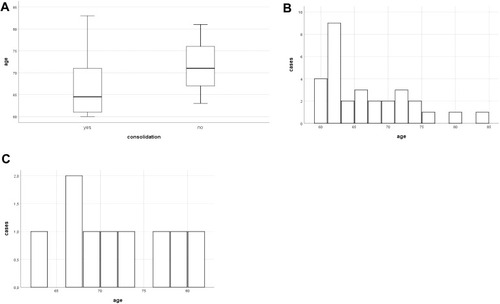
Analysis of age as a risk factor in the outcome of non-union therapy revealed no statistically significant differences in patients treated with the one-step procedure according to the “diamond concept” (). In contrast, age had a significant influence on the outcome of the Masquelet therapy (p = 0.027). In particular, increasing age of patients was associated with a higher risk for failure of the applied Masquelet therapy (). Patients that responded favorably to the Masquelet therapy were an average of 66.23 ± 6.27 years old, whereas patients that did not respond were an average of 71.33 ± 6 years old. These results were further corroborated by a binary regression analysis confirming that age had a significant negative impact (p=0.05) on the outcome of the Masquelet therapy but not the one-step treatment ().
Table 3 Binary Regression Analysis of Impact of Age on Type of Therapy
Figure 1 Outcome of one-step non-union treatment in respect to patient age.
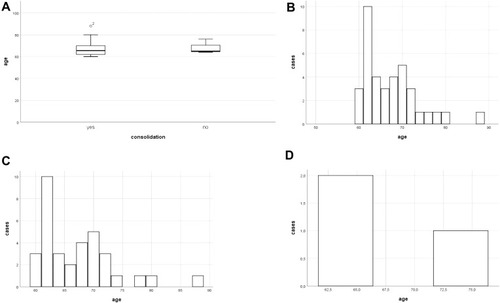
Figure 2 Outcome of the Masquelet therapy in respect to patient age.
Evaluation of Anatomical Localization as Risk Factor
Analysis of the affected long bone as risk factor for persisting non-union was applied in the two most common and relevant anatomical locations (tibia and femur). In particular, statistical analysis revealed no differences regarding the outcome of non-union therapy of the femur between both groups. However, patients with non-unions of the femur that were treated with the Masquelet therapy showed lower rates of unions (63.2%) compared to patients treated with one-step surgery (88.9%) at a non-significant extent. In contrast, patients suffering from a non-union of the metaphyseal tibia that was treated with the Masquelet therapy had a significantly better outcome compared to the one-step surgery (p = 0.047). Masquelet-treatment of non-unions of the remaining tibia shaft showed similar union rates compared to the one-step surgery (89.5% vs 87.5%, respectively).
Evaluation of Infection as Risk Factor
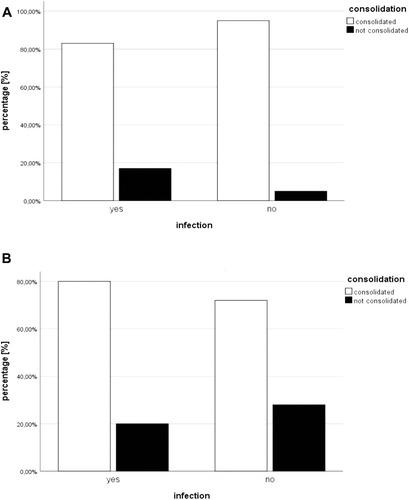
Analysis revealed a non-significant influence of infection on the outcome of one-step non-union therapy. However, patients suffering from an infected non-union showed the tendency toward an inferior outcome compared to patients that did not. In contrast, presence of an infection did not influence the outcome of the Masquelet therapy ().
Figure 3 Evaluation of local infection as risk factor.
Evaluation of the Method of Osteosynthesis, Smoking Status, Sex, and BMI as Risk Factor
Statistical analysis revealed no influence of BMI, sex, smoking status or method of osteosynthesis in context with the outcome of non-union therapy.
Discussion
Complex physiological changes on a cellular, molecular and systemic level lead to degenerative functional outcomes in an aging patient.Citation3 Initially, age-related changes were postulated to be constructive and conducive to maximize survivability,Citation3 however these changes have a profound impact on patients, predisposing them to fractures.Citation20 Older adults suffering from non-unions are often unable to perform activities of daily living and are at risk of becoming dependent on nursing care.Citation1 Therefore adequate, efficient, and beneficial treatment options are necessary in this demanding group of patients.
Clinical Effectiveness of Non-Union Therapy in Older Adults
Animal studies have shown that cartilage and bone formation are delayed in elderly animals, furthermore, inclusion of minerals into the callus is reduced by increased age.Citation5 Molecular studies have shown that the onset of expression of osteogenic factors is delayed in correlation with increasing age,Citation5 and older adults (>60 years) have a lower capacity for mesenchymal progenitor stem cell division and differentiation, impaired angiogenesis, and reduced levels of growth factors, predisposing them to delayed fracture healing.Citation1,Citation3 The period of convalescence required for non-union healing or fracture repair is crucial in older adults due to post-traumatic morbidity and mortalityCitation5 and therefore adequate, efficient, and beneficial treatment options are necessary in this demanding group of patients. Established treatment options inducing bone regeneration according to the “diamond concept” consist of one or two surgical procedures. One-stage treatment consists of optimization of stability, improvement of vascularization and the use of osteoconductive as well as osteoinductive materials (autologous bone graft).Citation11 Advantages of this treatment option are the necessity of a single surgical procedure, therefore reduced perioperative risks and the decreased duration of immobility, whereas infected non-unions and non-unions with a large osseous defect are limiting factors to this treatment option. Therefore, the induced membrane- or Masquelet-technique was established.Citation7,Citation11 The Masquelet-technique is a two-staged procedure: during the first step a vascularized membrane is induced, containing growth factors and supporting the proliferation of human bone marrow stromal cells,Citation8 subsequently the membranous tube is grafted by autologous bone graft due to its osteogenic and osteoconductive potential. Advantages of this treatment are effective reduction of infections and induction of bone regeneration, whereas multiple surgical treatments increase the perioperative risk as well as the duration of convalescence.
Despite substantial evidence demonstrating the effectiveness of non-union therapy applied according to the “diamond concept”,Citation9,Citation11,Citation17,Citation21 data evaluating the clinical effectiveness of non-union therapy in older adults remain scarce. The findings of the current study confirmed previous findings in younger patients and showed good clinical outcome after one-step (91.9%) and two-step (76.9%) therapy. Evidence regarding a higher risk of older patients developing delayed union or non-union remains controversial.Citation1 In particular, some studies have found no connection between age and healing complicationsCitation22 whereas others have found a higher risk of delayed union and union in older adults.Citation1 Foulke et al concluded that further studies are needed to discern whether age alone plays a significant role in the development of non-unions.Citation1 The findings of our study revealed no connection between age and applied one-stage treatment of non-unions. In contrast, the current study showed a significant negative correlation between increased age and clinical outcome of the Masquelet therapy. In particular, patients averaging 71 years were more likely to have a poor clinical outcome than patients averaging 66 years. Despite overall good clinical outcome subsequent to non-union therapy, current data indicated relevant differences regarding treatment of non-unions of particular anatomical regions. Here we were able to show that patients suffering from a non-union of the femur showed higher rates of union once a one-stage treatment was applied; whereas patients suffering from non-union of the metaphyseal tibia had significantly better outcome when treated with the Masquelet therapy. Infected non-union is a known risk factor regarding the outcome of non-union therapy.Citation11,Citation17 The data from the current study indicated that patients suffering from an infected non-union that was treated with a one-stage surgery had an inferior outcome compared to patients that had no infection. Interestingly, infection did not influence the outcome of Masquelet therapy. This finding is in concordance with previously published reports,Citation9,Citation23 since the Masquelet therapy eradicates potentially infected tissue during the first step. In addition, we could show that pain associated with weight bearing following non-union therapy is associated with the radiological consolidation regardless of the type of applied non-union therapy.
Risk Factors Influencing Non-Union Therapy
Smoking is known to cause various health complications; among them is delayed or inhibited fracture healing.Citation1 Studies have shown that smokers have a high risk of developing atherosclerosis and low oxygen levels leading to poor perfusion and the deposition of fibrous tissue instead of bone at the fracture side.Citation24 Interestingly, in our study, smoking status had no influence on the outcome of non-union therapy. This might be caused by an already altered biology and a diminished potential for angiogenesis due to increased age. Nonetheless, caregivers should advise cessation of smoking due to known health complications.
Studies have shown higher risk for wound infection in morbidly obese patients,Citation25 furthermore, Fischer et al have shown that non-unions in patients with lower BMI are more likely to consolidate than in obese patients.Citation21 However, in older adults it has been shown that obesity may improve outcome after cardiovascular surgery due to greater metabolic reserve and certain protective effects of fat-derived cytokines.Citation26 In addition, studies have shown protective effects regarding functionality and mortality for pre-obese patients (BMI 25–30 kg/m2) and therefore advised patients to stay in this range.Citation27,Citation28 The data of our study have shown no negative correlation of increased BMI with the outcome of non-union therapy. Average BMI in the current study was below 30 kg/m2; therefore the beneficial effects of being mildly overweight might have outweighed detrimental effects of morbid obesity. The data of our study suggest that patients may benefit from non-union therapy regardless of their BMI.
Gender-specific differences regarding fracture healing in younger patients might be due to an unequal distribution of high-risk sports and car accidents.Citation21 In particular, men more often than females suffer from open fractures, which are associated with impaired healing. In the current study, sex had no influence on the outcome of non-union therapy. This might be caused by an alignment of lifestyle in older adults and therefore equal distribution of injuries.
In the current study the method of osteosynthesis did not influence the outcome of applied non-union therapy. As shown before, comparison of plate osteosynthesis and intramedullary nailing of the tibia showed a similar responder rate, development of non-unions and number of following surgeries.Citation29 Based on our data, the method of osteosynthesis in older adults should be chosen based on the experience of the surgeon and the anatomical localization.
Limitations
Non-unions are a serious and debilitating complication, however occurrence of non-unions remains infrequent, therefore clinical studies concerning non-union therapy are complex, which explains the small size of our patient collective. Despite the large patient collective, only a small number of patients could be included in the study due to our strict inclusion and exclusion criteria. Caregivers should be aware that elderly patients’ willingness to adhere to follow-up protocol might be hampered for numerous reasons. Differences in radiological consolidation might have been influenced by the rater, however, two independent and blinded experienced trauma surgeons assessed radiological consolidation, thereby reducing possible biases. This study was able to identify important risk factors and furthermore rebut previously established risk factors; therefore, we believe that these findings add important knowledge to the literature in the field.
Conclusion
Treatment of non-unions is particularly challenging for caregivers of older adults.Citation1,Citation7 Based on the findings of the current study, non-union therapy according to the “diamond concept” is an effective and reliable treatment option in older adults. However, caregivers should be aware of the limitations of the one-stage and two-stage treatment.
In particular, when deciding in favor of a particular treatment option caregivers should take into account the age of a patient, anatomical localization, and the possibility of an infection. Patients benefit from non-union therapy regardless of their BMI or sex and the method of osteosynthesis in older adults should be chosen based on the experience of the surgeon and the anatomical localization. According to findings of the current study, we believe that older adults suffering from an infected non-union benefit from a two-stage procedure, whereas in patients suffering from a non-infected non-union a one-step surgical treatment is beneficial.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Acknowledgments
The authors acknowledge financial support by the Baden-Württemberg Ministry of Science, Research and the Arts and by Ruprecht-Karls-Universität Heidelberg.
Disclosure
The authors report no conflicts of interest in this work.
References
- Foulke BA, Kendal AR, Murray DW, Pandit H. Fracture healing in the elderly: a review. Maturitas. 2016;92:49–55. doi:10.1016/j.maturitas.2016.07.01427621238
- Jones G, Nguyen T, Sambrook PN, Kelly PJ, Gilbert C, Eisman JA. Symptomatic fracture incidence in elderly men and women: the Dubbo Osteoporosis Epidemiology Study (DOES). Osteoporos Int. 1994;4(5):277–282. doi:10.1007/BF16233527812076
- Gruber R, Koch H, Doll BA, Tegtmeier F, Einhorn TA, Hollinger JO. Fracture healing in the elderly patient. Exp Gerontol. 2006;41(11):1080–1093. doi:10.1016/j.exger.2006.09.00817092679
- Moghaddam A, Zimmermann G, Hammer K, Bruckner T, Grutzner PA, von Recum J. Cigarette smoking influences the clinical and occupational outcome of patients with tibial shaft fractures. Injury. 2011;42(12):1435–1442. doi:10.1016/j.injury.2011.05.01121665205
- Lu C, Miclau T, Hu D, et al. Cellular basis for age-related changes in fracture repair. J Orthop Res. 2005;23(6):1300–1307. doi:10.1016/j.orthres.2005.04.003.110023061015936915
- Egol KA, Koval KJ, Zuckerman JD. Functional recovery following hip fracture in the elderly. J Orthop Trauma. 1997;11(8):594–599. doi:10.1097/00005131-199711000-000099415867
- Karger C, Kishi T, Schneider L, Fitoussi F, Masquelet AC. Treatment of posttraumatic bone defects by the induced membrane technique. Orthop Traumatol Surg Res. 2012;98(1):97–102. doi:10.1016/j.otsr.2011.11.00122244249
- Bosemark P, Perdikouri C, Pelkonen M, Isaksson H, Tagil M. The masquelet induced membrane technique with BMP and a synthetic scaffold can heal a rat femoral critical size defect. J Orthop Res. 2015;33(4):488–495. doi:10.1002/jor.2281525639666
- Masquelet AC, Begue T. The concept of induced membrane for reconstruction of long bone defects. Orthop Clin North Am. 2010;41(1):27–37. doi:10.1016/j.ocl.2009.07.01119931050
- Pelissier P, Masquelet AC, Bareille R, Pelissier SM, Amedee J. Induced membranes secrete growth factors including vascular and osteoinductive factors and could stimulate bone regeneration. J Orthop Res. 2004;22(1):73–79. doi:10.1016/S0736-0266(03)00165-714656662
- Moghaddam A, Zietzschmann S, Bruckner T, Schmidmaier G. Treatment of atrophic tibia non-unions according to ‘diamond concept’: results of one- and two-step treatment. Injury. 2015;46(Suppl 4):S39–50. doi:10.1016/S0020-1383(15)30017-6
- Giannoudis PV, Einhorn TA, Marsh D. Fracture healing: the diamond concept. Injury. 2007;38(Suppl 4):S3–6. doi:10.1016/S0020-1383(08)70003-2
- Tanner M, Vlachopoulos W, Findeisen S, et al. Does age influence the outcome of lower limb non-union treatment? A matched pair analysis. J Clin Med. 2019;8(9):1276. doi:10.3390/jcm8091276
- Andrzejowski P, Giannoudis PV. The ‘diamond concept’ for long bone non-union management. J Orthop Traumatol. 2019;20(1):21. doi:10.1186/s10195-019-0528-030976944
- Schmidmaier G, Moghaddam A. [Long Bone Nonunion]. Z Orthop Unfall. 2015;153(6):659–674. German. doi:10.1055/s-0035-155825926670151
- Miska M, Findeisen S, Tanner M, et al. Treatment of nonunions in fractures of the humeral shaft according to the Diamond Concept. Bone Joint J. 2016;98-B(1):81–87. doi:10.1302/0301-620X.98B1.35682
- Moghaddam A, Thaler B, Bruckner T, Tanner M, Schmidmaier G. Treatment of atrophic femoral non-unions according to the diamond concept: results of one- and two-step surgical procedure. J Orthop. 2017;14(1):123–133. doi:10.1016/j.jor.2016.10.00327843223
- Haubruck P, Tanner MC, Vlachopoulos W, et al. Comparison of the clinical effectiveness of Bone Morphogenic Protein (BMP) −2 and −7 in the adjunct treatment of lower limb nonunions. Orthop Traumatol Surg Res. 2018;104(8):1241–1248. doi:10.1016/j.otsr.2018.08.00830293748
- Haubruck P, Kammerer A, Korff S, et al. The treatment of nonunions with application of BMP-7 increases the expression pattern for angiogenic and inflammable cytokines: a matched pair analysis. J Inflamm Res. 2016;9:155–165. doi:10.2147/JIR.S11062127703392
- Manolagas SC. Birth and death of bone cells: basic regulatory mechanisms and implications for the pathogenesis and treatment of osteoporosis. Endocr Rev. 2000;21(2):115–137. doi:10.1210/edrv.21.2.039510782361
- Fischer C, Nissen M, Schmidmaier G, Bruckner T, Kauczor HU, Weber MA. Dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI) for the prediction of non-union consolidation. Injury. 2017;48(2):357–363. doi:10.1016/j.injury.2017.01.02128088373
- Hernandez RK, Do TP, Critchlow CW, Dent RE, Jick SS. Patient-related risk factors for fracture-healing complications in the United Kingdom General Practice Research Database. Acta Orthop. 2012;83(6):653–660. doi:10.3109/17453674.2012.74705423140093
- Masquelet AC, Obert L. [Induced membrane technique for bone defects in the hand and wrist]. Chir Main. 2010;29(Suppl 1):S221–224. French. doi:10.1016/j.main.2010.10.00721084208
- Toksvig-Larsen AWD, Toksvig-Larsen S. Cigarette smoking delays bone healing: a prospective study of 200 patients operated on by the hemicallotasis technique. Acta Orthop Scand. 2004;75(3):347–351. doi:10.1080/0001647041000130315260429
- Floerkemeier S, Staubli AE, Schroeter S, Goldhahn S, Lobenhoffer P. Does obesity and nicotine abuse influence the outcome and complication rate after open-wedge high tibial osteotomy? A retrospective evaluation of five hundred and thirty three patients. Int Orthop. 2014;38(1):55–60. doi:10.1007/s00264-013-2082-324022738
- Chapman IM. Obesity in old age. Front Horm Res. 2008;36:97–106.18230897
- Wojzischke J, Diekmann R, Bauer JM. [Obesity in old age and its importance for functionality and frailty]. Z Gerontol Geriatr. 2016;49(7):573–580. German. doi:10.1007/s00391-016-1133-y27637579
- Mathus-Vliegen EM. Obesity and the elderly. J Clin Gastroenterol. 2012;46(7):533–544. doi:10.1097/MCG.0b013e31825692ce22772735
- Vallier HA, Cureton BA, Patterson BM. Randomized, prospective comparison of plate versus intramedullary nail fixation for distal tibia shaft fractures. J Orthop Trauma. 2011;25(12):736–741. doi:10.1097/BOT.0b013e318213f70921904230