
Abstract
Purpose
This study is to investigate the risk prediction of severe or critical events of COVID-19 in older adults in China and provide the evidence to support the management of older adults with COVID-19.
Materials and Methods
The clinical data of older adults with COVID-19 admitted to the Shanghai Public Health Clinical Center during January 20, 2020 to March 16, 2020 were collected. The possible risk factors of severe or critical illness were investigated with Cox proportional hazards (PH) regression models for univariate and multivariate analyses to estimate hazard ratios (HRs) and 95% confidence intervals (CIs). For the prediction indicators, optimum cut-off points were determined by calculating Youden’s index. The efficacy of risk prediction of severe or critical illness was examined through the receiver operating characteristic (ROC) curve.
Results
A total of 110 older adults with COVID-19 were included, in which 21 (19.1%) patients had severe or critical illness of COVID-19. Multivariable regression analysis showed that CD4 cells and D-dimer were independent risk factors. D-dimer, CD4 cells, and CD cells/D-dimer ratio with cut-off values of 0.65 (mg/L), 268 (cell/µL) and 431 were in the prediction of severe or critical illness of older adults with COVID-19. The AUC value of D-dimer, CD4 cells, CD4 cells/D-dimer ratio, the tandem combination and the parallel combination to predict severe or critical illness of the older adults with COVID-19 were 0.703, 0.804, 0.794, 0.812 and 0.694, respectively.
Conclusion
D-dimer and CD4 cells either by themselves or in combination have demonstrated predictive value in risk stratification as well as established the prognosis of severe or critical illness in older adults with COVID-19.
Introduction
The disease burdens of coronavirus disease 2019 (COVID-19), caused by severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2), have been continuously increasing.Citation1 To date, there have been over 3.5 million confirmed patients and over 0.24 million deaths globally according to COVID-19 global data from Johns Hopkins University (JHU). Advance age has been reported as a significant predictor of morbidity and mortality in patients with COVID-19.Citation2 The mortality of older adult patients with COVID-19 is higher than that of young and middle-aged patients and older adult patients with COVID-19 are more likely to progress to severe disease.Citation2 A recent meta-analysis found that the case-fatality rate (CFR), proportion of severe cases and incidents of acute respiratory distress syndrome (ARDS) were significantly higher in studies with a high proportion of older adult patients.Citation3 Furthermore, previous studies showed that older adult patients with comorbidities and ARDS are at increased risk of death.Citation4,Citation5 Given a large aging population worldwide, it is important to understand the characteristics and the susceptibility on older adult patients with COVID-19. Up to now, there has been few reports on risk assessment of severe or critical illness of COVID-19 in older adults.Citation2,Citation5,Citation6 This study aims to provide a comprehensive understanding of clinical characteristics of older adult patients with COVID-19 and the determinants of prognosis.
Materials and Methods
Patients and Definitions
Patients with confirmed COVID-19 diagnosis admitted to the Shanghai Public Health Clinical Center from January 20, 2020 to March 16, 2020 were included. Confirmed cases diagnosis met the following criteria: the patients had epidemiological contact history or clinical manifestations, and positive nucleic acid of COVID-19 were confirmed with real-time fluorescence polymerase chain reaction (RT-PCR). Severe events of COVID-19 patients were defined as one of the following conditions: shortness of breath with respiratory rate (RR) ≥30 times/min; the oxygen saturation ≤93% at rest; the arterial partial oxygen pressure (PaO2)/fraction of inspired oxygen (FiO2) ≤ 300mmHg. Critical events of COVID-19 patients were defined as one of the following conditions: respiratory failure with the need for mechanical ventilation; shock; patients with other organ failures should be treated in ICU.Citation7 Older adults were defined as aged ≥ 60 years old in China. Severe or critical illness were defined as patients with COVID-19 who developed severe or critical events during hospitalization. The index date was set as the first day of hospitalization. The endpoint was the occurrence of severe or critical illness during hospitalization. The high-risk group was defined as older adults with COVID-19 who developed severe or critical events during hospitalization, and the control group was defined as older adults with COVID-19 who did not develop to severe or critical illness during hospitalization. We exclude patients who have other infectious complications.
Informed consent of patients was obtained for diagnosis, treatment, and their data being used for research. The study protocol was approved by the Ethics Committee of the Shanghai Public Health Clinical Center, the approval letter number of which was YJ-2020-S015-01. This study was also conducted in accordance with the Declaration of Helsinki.
Study Design and Indicators
A retrospective cohort study design was conducted to collect the demographic and clinical data from electronic medical record (EMR), including hospital information system (HIS), laboratory information system (LIS) and radiology information system (RIS) of the Shanghai Public Health Clinical Center. The demographic and clinical data included age and sex of the patients, pulmonary lobes affected by COVID-19, history of hypertension, diabetes, cardiovascular disease; laboratory testing results including alanine aminotransferase (ALT), aspartate aminotransferase (AST), creatine kinase (CK), lactate dehydrogenase (LDH), total bilirubin (TBIL), albumin (ALB), prealbumin (PA), total cholesterol (TC), triglyceride (TG), blood urea nitrogen (BUN), creatinine (Cr), high-density lipoprotein (HDL-C), low-density lipoprotein (LDL-C), activated partial thrombin time (APTT), fibrinogen (Fg), prothrombin time (PT), thrombin time (TT), D-dimer (D-D), white blood cell (WBC), neutrophil (Neu), lymphocyte (Lym), haemoglobin (Hgb), platelet (PLT), and CD4-positive T-lymphocytes (CD4, CD4 cells). All the above baseline characteristics were collected in the 24 hours after admission.
Statistical Analyses
Pearson’s chi-squared test was used for categorical data. The Kolmogorov–Smirnov test was used for the normality of continuous variables. Data with normal distribution were described as mean ± standard deviation. The median and interquartile range was used for non-parametric data. The difference between case and control groups was tested by Mann–Whitney U-test.
The possible risk factors of severe or critical illness were investigated with Cox proportional hazards (PH) regression models for univariate and multivariate analyses to estimate hazard ratios (HRs) and 95% confidence intervals (CIs). PH assumption was verified using Schoenfeld residuals. Potential confounders were identified and investigated in the analysis. For the prediction indicators, an optimum cut-off point can be determined by calculating Youden’s index. The cut-off point that achieves this maximum Youden’s index is referred to as the optimal cut-point. Youden Index is the main summary statistic of the receiver operating characteristic (ROC) curve used in the interpretation and evaluation of an indicator, which defines the maximum potential effectiveness of a diagnostic test. The area under curve (AUC) of ROC were compared using Delong test. The P value of two-sided less than 0.05 was considered as statistically significant. SPSS software version 16.0 (SPSS Inc. Chicago, IL, USA,) was used for statistical analysis of the data.
Results
Baseline Profile of COVID-19 in Older Adults
A total of 110 older adults with confirmed COVID-19 were included in this study, in which 52 were males (47.3%). Twenty-one patients (19.1%) were included in the high-risk group and 89 patients (80.9%) in the control group. The proportion of males, aspartate aminotransferase, creatine kinase, lactate dehydrogenase, total bilirubin, activated partial thrombin time, prothrombin time, creatinine, D-dimer, neutrophil count, neutrophil percentage and haemoglobin in the high-risk group were higher than those in the control group (P<0.05). The level of albumin, pre-albumin, lymphocytes and CD4 cells in the high-risk group were lower than those in the control group (P<0.05). The detailed information is shown in .
Table 1 Baseline Data of Older Adults with COVID-19
Risk Factors of COVID-19 Severe or Critical Illness Events in Older Adults
From the univariate Cox regression analysis, the HR of age, sex, CK, LDH, TBIL, ALB, PA, BUN, Cr, D-dimer, WBC, Neu count, Neu percentage, Lym, Hgb and CD4 were significant associated with the outcome (P< 0.05). Results from multivariate Cox regression analysis suggested that the level of D-dimer was a risk factor of occurrence of severe or critical events while the CD4 cells count was a protective factor, with HR of 1.577 (1.072–2.320) and 0.993 (0.986–0.999), respectively. The detailed Cox regression results are shown in .
Table 2 Analysis of Risk Events Indicators in the Older Adults with COVID-19
Predictive Efficacy of D-Dimer, CD4 Cells and Their Combination for Severe or Critical Illness in Older Adults with COVID-19
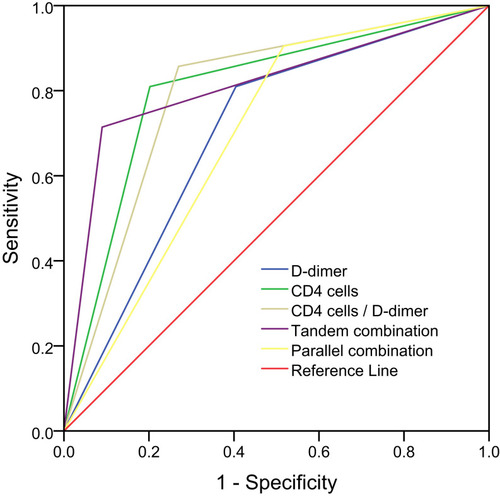
According to the Youden index maximization principle, the cut-off values of D-dimer, CD4 cells and CD4 cells/D-dimer ratio were 0.65 (mg/L), 268 (cell/µL) and 431 for the prediction of severe or critical events in older adults with COVID-19. In the tandem combination (D-dimer and CD4 cells), the D-dimer was higher than 0.65 mg/L and the CD4 cells were less than 268 cell/µL. In the parallel combination (D-dimer or CD4 cells), the D-dimer was higher than 0.65 mg/L, or the CD4 cells were less than 268 cell/µL. The AUC values of D-dimer, CD4 cells, CD4 cells/D-dimer ratio, the tandem combination and the parallel combination were 0.703, 0.804, 0.794, 0.812, and 0.694, respectively (P<0.05). and show the detailed information.
Table 3 Risk Prediction of D-Dimer, CD4 Cells and Their Combination in Older Adults with COVID-19
Figure 1 AUC curve of D-dimer, CD4 cells and their combination in the risk prediction of severe or critical illness in the older adult with COVID-19.
To evaluate the risk prediction efficacy of COVID-19 in older adults, the sensitivity, specificity, positive predictive value and negative predictive value of D-dimer, CD4 cells, CD4 cells/D-dimer ratio, tandem combination (D-dimer and CD4 cells) and parallel combination (D-dimer or CD4 cells) are shown in with detailed information.
Table 4 Evaluation of D-Dimer, CD4 Cells, and Their Combination in the Risk Prediction of Severe or Critical Illness in Older Adults with COVID-19
Discussion
SARS-CoV-2 is a member of the coronavirus family, which is derived from bats according to gene sequencing. It belongs to a de novo independent evolution branch of coronavirus, and has high homology with coronavirus related to severe acute respiratory syndrome (SARS) and coronavirus related to Middle East Respiratory Syndrome (MERS).Citation3,Citation8–13 The virus is mainly spread by droplets and contact, and there is the possibility of aerosol transmission. Patients during the incubation period and asymptomatic virus carriers are also infectious.Citation14 As SARS virus, through S protein and angiotensin conversion enzyme-Ⅱ-receptor, SARS-CoV-2 can be transmitted across species or human to human.Citation15–Citation17 Compared with the SARS virus, SARS-CoV-2 is less virulent but more infectious.Citation16,Citation17
Several global studies have investigated the characteristics and risk factors of COVID-19-related symptoms and deaths in Italy, Mexico and UK.Citation18–Citation20 Therefore, it is of great value to analyze the risk prediction indicators of COVID-19 in older adults in China. This study focuses on the analysis of risk factors for severe and critical illness in older adults with COVID-19 and their practical application. In this paper, the regression analysis was used to collect COVID-19 keywords from recent literature retrieval, and representative indicators were selected for statistical analysis based on clinical experience and practical value. To avoid the time difference between baseline data and severe or critical events in the course of the disease, Cox regression was used for progressive analysis to determine whether the study parameters were independent influencing factors. The ROC curve was used to deduce the warning value of risk factors.
The proportion of lung insult of COVID-19 in the early stage was generally extensive in the older adults, and the median of both the risk group and the control group was 5 lobes, showing no statistically significant difference between the two groups. Age and sex were the risk factors for COVID-19 severe or critical events in the older adults. The complications of hypertension, diabetes and cardiovascular disease did not significantly aggravate in the severe or critical cases. SARS-CoV-2 is a member of the coronavirus family. These imported cases (refers to people in other areas of China outside Shanghai who were diagnosed as COVID-19 cases when they pass by Shanghai) may have milder comorbidities; because the cases with severe comorbidities may be less likely to be infected due to the limited range of daily communication.
Subsequently, the sample size could be increased to stratify the severity and control of complications and further verify the risk ratio. However, the number of complications in the older adults is more than that in the younger population, and the complications of basic diseases in the older adults is significantly correlated with the occurrence of end-stage event.Citation2,Citation6 Alanine aminotransferase and aspartate aminotransferase had no effect on severe or critical events in older adults with COVID-19, which was consistent with earlier reports.Citation21 Early indicators such as creatine kinase, lactate dehydrogenase, bilirubin, urea, creatinine, albumin, prealbumin, white blood cells, neutrophils and hemoglobin were related factors influencing the severe or critical events of COVID-19 in older adults, rather than independent factors. It could be related to the basic metabolism, characteristics of infection, host immunity, or combinations of basic diseases and starting point set by the research in the older adults.
In this study, CD4 cells were independent factors affecting severe or critical events of COVID-19 in the older adults. Previous studies of SARS have also confirmed a decrease in the absolute count of CD4 cells, with characteristic changes throughout the pathogenesis, which is consistent with the characteristics of coronavirus family infection. Recent studies have reported that SARS-CoV-2 infection can induce decreased CD4 cells.Citation4,Citation22–24 Compared with the survival group, the absolute count level of CD4 cells count in the death group of viral pneumonia was significantly reduced, suggesting that a large number of T cells were activated and depleted during the antiviral process. All of the above supported the study results of CD4 cells; and CD4 cell count of < 268 cell/µL had a significant predictive effect on the occurrence of severe or critical COVID-19 events in the older adults, with high sensitivity (81.0%) and negative predictive value (94.7%).
As for the lymphocyte count, there was significant differences in the univariate analysis, but no significant differences in the multivariate analysis. Lymphocyte count was preliminarily determined to be a risk factor associated with COVID-19 severe or critical events in the older adults, rather than an independent factor. Recently, SARS-CoV-2 pneumonia has been reported to have a significant decrease in lymphocytes in the whole population;Citation16,Citation17 SARS-CoV-2 may act on lymphocytes via ACE2 receptor, causing lymphocytopenia or induce lymphocytopenia by TNF, interleukin-6, and other pro-inflammatory cytokines,Citation25–Citation27 which is also characteristic of coronavirus infection of immune cells. In this study, lymphocytes were indeed low in the older adults, with a lower value of 0.84±0.45 (10^9/L) in the risk group, but a normal range of 1.2–3.5 (10^9/L). However, the early count of lymphocytes was not an independent factor affecting severe or critical events, which might be related to the characteristics of the older adults. But, studies have suggested that the dynamic expression of lymphocyte percentage can predict the severity of COVID-19.Citation28 Later cases could be added, and lymphocyte counts at different stages were used to evaluate the severity of COVID-19 and verify whether there was a statistical difference.
D-dimer was also an independent factor affecting severe or critical events of COVID-19 in the older adults. In terms of this indicator, recent studies have reported that the significant increase of D-dimer is associated with the poor prognosis of severe coronavirus pneumonia.Citation29,Citation30 The death cases of COVID-19 had significant increase of plasma D-dimer.Citation30 Moreover, in adults with community-acquired pneumonia, increased plasma D-dimer was associated with increased inflammatory response, admission to intensive care and 30-day mortality, and was superior to C-reactive protein and procalcitonin in predicting admission to intensive care and 30-day mortality.Citation29 All of the above reflected the value of D-dimer and supported that the increase of D-dimer was an independent factor affecting the severe or critical events of COVID-19 in the older adults. Similarly, the severe or critical events of D-dimer>0.65 mg/L in older adults with COVID-19 were also evaluated by ROC curve with high predictive efficacy, showing high sensitivity (81.0%) and negative predictive value (93.0%), respectively.
In order to consider the effects of SARS-CoV-2 on immunity and coagulation in older adult patients, we can combine D-dimer level and CD4 cells count in conjunction to evaluate the occurrence of severe or critical events. The combination of the two had high inferential efficiency on the occurrence of risk events in the older adults with COVID-19. There were respective significant contributions on the evaluation index, with high sensitivity (90.5%), specificity (91.0%), positive predictive value (65.2%) or negative predictive value (95.6%).
Based on the results of this study and the close correlation between autoimmune disorders and coagulation abnormalities and thrombosis events in patients,Citation31 we propose a hypothesis: CD4 cells and D-dimer may trigger in the progression of the older adults with COVID-19; SARS-CoV-2 may act on CD4 cells through ACE2 receptor, and cause CD4 cells count reduction. Immune dysregulation and inflammatory response can increase the level of D-dimer and decrease CD4 cells. In the early stage of the disease, when the number of CD4 cells count decreases to a certain number and the D-dimer increase to a certain level, the risk event trend of COVID-19 will be continuously affected. To eliminate the bias, we exclude patients who have other infectious complications, which might greatly influence the CD4 cell count and D-dimer level. Therefore, the immune dysregulation, cytokine disorder and multi-organ damage can be continuously induced in the state of low cellular immunity and high coagulation to a certain extent, leading to the severe or critical events of COVID-19.
The highlight of this study was the older adults with COVID-19 as the research object, because the older adult population has its own characteristics with risk factors of severe or critical events.Citation2,Citation4,Citation6 It was found that D-dimer and CD4 cells were independent factors affecting the severe or critical events of COVID-19 in the older adults, and the indicators had important clinical application value. However, the proportion of comorbidities and their prognostic analysis were significantly different from the other studies,Citation5,Citation6 which would be related to the fact that the samples of this study were all imported domestic cases and regional prevention and control policies. The advantage of this study lay in the in-depth analysis of all the research data; the independent influencing factors of COVID-19 risk events in the older adults were identified, and the application value was evaluated.
This study has several limitations. First, the sample size of the older adults with COVID-19 was not large. Second, we did not collect the follow-up testing of D-dimer and CD4 cells to analyse the dynamic of the testing results, which will help to better determine the associations between the two parameters and the severity of COVID-19.
Conclusions and Implications
COVID-19 risk factors in older adults have their own characteristics. The decrease of CD4 cells count and the increase of D-dimer level in the early stage of the disease are independent influencing factors for the occurrence of severe or critical events. The application of D-dimer, CD4 cells and their combination have important risk prediction efficacy for the severe or critical illness of the older adults with COVID-19.
Ethical Approval
The study was approved by the Ethics Committee of the Shanghai Public Health Clinical Center Clinical Committee (approval letter number: YJ-2020-S015-01).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. These authors contributed equally to this work and should be considered co-first authors: Xiao-Yu Zhang and Lin Zhang.
Acknowledgments
The study was supported by the Shanghai Public Health Clinical Center for data access. Thanks Dr. Hai-Bing Wu for supporting the data input of the study. Thanks Dr. Wei-Xia Li, Dr. Zhi-Ping Qian, Dr. Yin-Peng Jin, Dr. Qing-Chun Fu, Dr. Xin-Yan Li, Dr. Yi Zhang and Dr. Yu-Xian Huang for providing comments for the study.
Disclosure
The authors declare no conflicts of interest.
References
- Epidemiology Working Group for NCIP Epidemic Response CCfDC, Prevention. The epidemiological characteristics of an outbreak of 2019 novel coronavirus diseases (COVID-19) in China. Chinese J Epidemiol. 2020;41(02):145–151.
- Li Q, Guan X, Wu P, et al. Early transmission dynamics in Wuhan, China, of Novel Coronavirus–Infected Pneumonia. New England J Med. 2020;382(13):1199–1207. doi:10.1056/NEJMoa200131631995857
- Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395(10223):497–506. doi:10.1016/S0140-6736(20)30183-531986264
- Zhou F, Yu T, Du R, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020;395(10229):1054–1062. doi:10.1016/S0140-6736(20)30566-332171076
- Guan WJ, Ni ZY, Hu Y, Liang WH, Zhong NS. Clinical characteristics of coronavirus disease 2019 in China. New England J Med. 2020;382:18. doi:10.1056/NEJMoa2002032
- Commission. CNH. Diagnosis and treatment protocol for Novel Coronavirus Pneumonia (Trial Version 7). Chin Med J. 2020;133(9):1087–1095. doi:10.1097/CM9.000000000000081932358325
- Chen N, Zhou M, Dong X, Qu J, Zhang L. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet. 2020;395:10223. doi:10.1016/S0140-6736(20)30211-7
- Xu X, Chen P, Wang J, et al. Evolution of the novel coronavirus from the ongoing Wuhan outbreak and modeling of its spike protein for risk of human transmission. Sci China Life Sci. 2020;63(3):457–460. doi:10.1007/s11427-020-1637-532009228
- Chen Y, Guo Y, Pan Y, Zhao ZJ. Structure analysis of the receptor binding of 2019-nCoV. Biochem Biophys Res Commun. 2020;525(1):135–140. doi:10.1016/j.bbrc.2020.02.071
- Ren -L-L, Wang Y-M, Wu Z-Q, et al. Identification of a novel coronavirus causing severe pneumonia in human. Chin Med J. 2020;133(9):1015–1024. doi:10.1097/CM9.000000000000072232004165
- Li R, Qiao S, Zhang G. Analysis of angiotensin-converting enzyme 2 (ACE2) from different species sheds some light on cross-species receptor usage of a novel coronavirus 2019-nCoV. J Infection. 2020;80(4):469–496.
- Zhang Y, Zheng L, Liu L, Zhao M, Xiao J, Zhao Q. Liver impairment in COVID-19 patients: A retrospective analysis of 115 cases from a single centre in Wuhan city, China. Liver Int. 2020;40(9):2095–2103. doi:10.1111/liv.1445532239796
- Zhou P, Yang X-L, Wang X-G, et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature. 2020;579(7798):270–273. doi:10.1038/s41586-020-2012-732015507
- Liu J, Zheng X, Tong Q, et al. Overlapping and discrete aspects of the pathology and pathogenesis of the emerging human pathogenic coronaviruses SARS‐CoV, MERS‐CoV, and 2019‐nCoV. J Med Virol. 2020;92(5):491–494. doi:10.1002/jmv.2570932056249
- Guo L, Wei D, Zhang X, Wu Y, Li Q. Clinical features predicting mortality risk in patients with viral pneumonia: the mulbsta score. Front Microbiol. 2019;10:2752. doi:10.3389/fmicb.2019.0275231849894
- Liu Y, Yang Y, Zhang C, et al. Clinical and biochemical indexes from 2019-nCoV infected patients linked to viral loads and lung injury. Nature Public Health Emergency Collection. 2020;63:3.
- Wang D, Hu B, Hu C, et al. Clinical characteristics of 138 hospitalized patients with 2019 Novel Coronavirus–Infected Pneumonia in Wuhan, China. JAMA. 2020;323(11):1061. doi:10.1001/jama.2020.158532031570
- Palmieri L, Vanacore N, Donfrancesco C, et al. Clinical characteristics of hospitalized individuals dying with COVID-19 by age group in Italy. J Gerontol. 2020;75(9):1796–1800. doi:10.1093/gerona/glaa146
- Bello-Chavolla OY, González-Díaz A, Antonio-Villa NE, et al. Unequal impact of structural health determinants and comorbidity on COVID-19 severity and lethality in older mexican adults: considerations beyond chronological aging. J Gerontol. 2020. doi:10.1093/gerona/glaa163
- Atkins JL, Masoli JAH, Delgado J, et al. Preexisting comorbidities predicting COVID-19 and mortality in the UK biobank community cohort. J Gerontol. 2020;75:2224–2230. doi:10.1093/gerona/glaa183
- Xu H, Zhong L, Deng J, Peng J, Chen Q. High expression of ACE2 receptor of 2019-nCoV on the epithelial cells of oral mucosa. Int J Oral Ence. 2020;12(1):8.
- Chen G, Wu D, Guo W, et al. Clinical and immunological features of severe and moderate coronavirus disease 2019. J Clin Invest. 2020;130(5):2620–2629. doi:10.1172/JCI13724432217835
- Zhang Y, Mo P, Ma Z, et al. Characteristics of peripheral lymphocyte subset alteration in COVID-19 Pneumonia. J Infect Dis. 2020;221(11):1762–1769. doi:10.1093/infdis/jiaa15032227123
- Wan S, Yi Q, Fan S, et al. Relationships among lymphocyte subsets, cytokines, and the pulmonary inflammation index in coronavirus (COVID‐19) infected patients. Br J Haematol. 2020;189(3):428–437. doi:10.1111/bjh.1665932297671
- Fung S-Y, Yuen K-S, Ye Z-W, Chan C-P, Jin D-Y. A tug-of-war between severe acute respiratory syndrome coronavirus 2 and host antiviral defence: lessons from other pathogenic viruses. Emerg Microbes Infect. 2020;9(1):558–570. doi:10.1080/22221751.2020.173664432172672
- Giamarellos-Bourboulis EJ, Netea MG, Rovina N, et al. Complex immune dysregulation in COVID-19 patients with severe respiratory failure. Cell Host Microbe. 2020;27(6):992–1000 e1003. doi:10.1016/j.chom.2020.04.00932320677
- Jamilloux Y, Henry T, Belot A, et al. Should we stimulate or suppress immune responses in COVID-19? Cytokine and anti-cytokine interventions. Autoimmun Rev. 2020;19(7):102567. doi:10.1016/j.autrev.2020.10256732376392
- Tan L, Wang Q, Zhang D, et al. Lymphopenia predicts disease severity of COVID-19: a descriptive and predictive study. Signal Transduction Targeted Therapy. 2020;5(1):33.32296069
- Ge YL, Liu CH, Wang N, et al. Elevated plasma d-dimer in adult community-acquired pneumonia patients is associated with an increased inflammatory reaction and lower survival. Clin Lab. 2019;65:1. doi:10.7754/Clin.Lab.2018.180720
- Zhang Y, Xiao M, Zhang S, et al. Coagulopathy and antiphospholipid antibodies in patients with Covid-19. N Engl J Med. 2020;382(17):e38. doi:10.1056/NEJMc200757532268022
- Leung C. Risk factors for predicting mortality in elderly patients with COVID-19: A review of clinical data in China. Mech Ageing Dev. 2020;188:111255. doi:10.1016/j.mad.2020.11125532353398