Abstract
Lenalidomide is an amino-substituted derivative of thalidomide with direct antiproliferative and cytotoxic effects on the myeloma tumor cell, as well as antiangiogenic activity and immunomodulatory effects. Together with the introduction of bortezomib and thalidomide, lenalidomide has significantly improved the survival of patients with relapsed and refractory myeloma. The most common adverse events associated with lenalidomide include fatigue, skin rash, thrombocytopenia, and neutropenia. In addition, when lenalidomide is combined with dexamethasone or other conventional cytotoxic agents, there is an increase in the incidence of venous thromboembolic events. There is now evidence that continued treatment with lenalidomide has a significant impact on survival by improving the depth and duration of response. This highlights the value of adverse event management and appropriate dose adjustments to prevent toxicity, and of allowing continued treatment until disease progression. In this review, we will discuss the different lenalidomide-based treatment regimens for patients with relapsed/refractory myeloma. This is accompanied by recommendations of how to manage and prevent adverse events associated with lenalidomide-based therapy.
Introduction
Lenalidomide and pomalidomide, as more potent derivatives of thalidomide, have been found to be less toxic and more active than their parent drug in the treatment of multiple myeloma (MM).Citation1–Citation4 Because of the structural similarities between thalidomide and its derivative immunomodulatory drugs (IMiDs), these agents have similar modes of action with both direct antitumor activity and indirect immunomodulatory and antiangiogenic effects (). IMiDs directly kill MM cells by the induction of cell cycle arrest and caspase-dependent apoptosis.Citation5–Citation7 In addition, we have shown that IMiDs target a subpopulation of MM cells with stem cell-like features (ie, side-population cells).Citation8 Recently, it has been demonstrated that cereblon, the primary target for thalidomide teratogenicity,Citation9 is required for the cytotoxic effects of thalidomide, lenalidomide, and pomalidomide.Citation10
Figure 1 The proposed mechanisms of action of lenalidomide in multiple myeloma include immune modulation (A); interference with tumor microenvironment interactions (B); and direct antitumor effects (C). (A) Immunomodulation by lenalidomide includes T cell co-stimulation, suppression of Tregs, increased production of Th1 cytokines, and activation of NK and NKT cells. (B) Lenalidomide mediates disruption of myeloma cell-microenvironment interactions via several mechanisms including antiangiogenesis, anti-inflammatory effects, antiosteoclastogenic properties, modulation of cytokine production, and downregulation of adhesion molecules. (C) IMiDs also exert direct effects on myeloma cells via cell cycle arrest and induction of apoptosis.
Abbreviations: T reg, regulatory T cell; BMSCs, bone marrow stromal cells; APC, antigen-presenting cell; NK cells, natural killer cells; NKT cells, natural killer T cells; ICAM-1, intercellular adhesion molecule 1; VCAM-1, vascular cell adhesion molecule 1; VEGF, vascular endothelial growth factor; RANKL, receptor activator of nuclear factor kappa-B ligand; bFGF, basic fibroblast growth factor; TGF-β, transforming growth factor-β; IGF-1, insulin-like growth factor 1; TNF-α, tumor necrosis factor α; IL-6, interleukin-6.
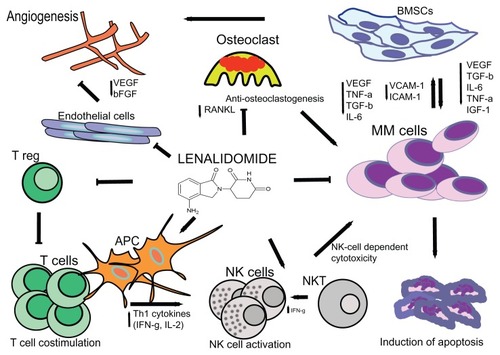
In addition, lenalidomide also impairs MM cell survival and proliferation through interference with the protective properties of bone marrow stromal cells, including the down-regulation of adhesion molecules such as VCAM-1 and ICAM-1,Citation11,Citation12 and inhibition of the production of cytokines like IL-6 and TNF-α.Citation13 Furthermore, IMiDs inhibit angiogenesis by downregulation of vascular endothelial growth factor and β–fibroblast growth factorCitation14,Citation15 and impair osteoclastogenesis by reducing RANKL levels.Citation16 IMiDs also have immunomodulatory effects including stimulation of T cell proliferation, increased production of IL-2 and IFNγ,Citation13 and enhancement of cytotoxic T lymphocyte, natural killer T, and natural killer effector cell activity against MM cells.Citation17,Citation18 Lenalidomide is more potent than thalidomide in both stimulating T cell proliferation via the T cell receptor and in enhancing IL-2 and IFNγ production. IMiDs also decrease the development of regulatory T cells in MM.Citation19 In addition, lenalidomide inhibits myeloid cell-mediated inflammatory function by decreasing the secretion of IL-6, TNFα, and IL-10.Citation20 We have demonstrated that IMiDs induce immune effector cell activation by triggering positive costimulatory molecule CD28 signaling in T cells,Citation17,Citation21 as well as regulate cytokine signaling by downregulating the suppressor of cytokine signaling (SOCS)1 in immune effector cells in MM, thereby inducing IL-2 and IFNγ production.Citation22
In this review, we will discuss the clinical activity and optimal use of lenalidomide and lenalidomide-based combinations in the management of relapsed and refractory MM.
Single-agent lenalidomide in relapsed/refractory MM
Single-agent lenalidomide was shown to be effective and well tolerated in relapsed/refractory MM patients who had received a median of three prior regimens as part of a Phase I trial in which the maximum tolerated dose (MTD) was found to be 25 mg daily, and 29% of the patients obtained at least a partial response (PR).Citation4 Importantly, no significant somnolence, constipation, or neuropathy was observed. The most common adverse events included fatigue, skin rash, thrombocytopenia, and neutropenia, which proved manageable with dose-reduction and granulocyte colony stimulating factor (G-CSF) support.Citation4 Single-agent lenalidomide did not significantly increase the risk of venous thromboembolism (VTE).Citation4 Other studies have since confirmed that single-agent lenalidomide has a favorable tolerability and promising efficacy, even after prior treatment with thalidomide, bortezomib, and/or high-dose melphalan with autologous stem cell rescue.Citation23,Citation24
Lenalidomide plus dexamethasone in relapsed/refractory MM
In vitro studies demonstrated that dexamethasone enhances the anti-MM effects of lenalidomide.Citation5,Citation6 Based on these preclinical and early phase clinical trial data suggesting that response rates can be markedly enhanced by the addition of dexamethasone, two randomized Phase III trials (MM-009 and MM-010) compared lenalidomide (25 mg on days 1–21 of a 28-day cycle) plus dexamethasone (40 mg on days 1–4, 9–12, and 17–20 for the first four cycles, and 40 mg on days 1–4 thereafter) with placebo plus dexamethasone in relapsed/refractory MM patients who had received a median of two previous therapies (). Dimopoloulos et alCitation25 demonstrated the superior efficacy of lenalidomide-dexamethasone compared with placebo plus dexamethasone in terms of higher overall response rate (complete response (CR) + PR; 60.2% vs 24.0%; P < 0.001) and CR rate (15.9% vs 3.4%; P < 0.001). The authors also noted that lenalidomide-dexamethasone exhibited a longer median time to progression (TTP) (11.3 vs 4.7 months; P < 0.001) and median overall survival (OS) (not reached and 20.6 months; P = 0.03) when compared with placebo plus dexamethasone. In the study of Weber et al,Citation26 comparable results were reported with a superior response rate (≥PR: 61.0% vs 19.9%; P < 0.001), CR rate (14.1% vs 0.6%; P < 0.001), median TTP (11.1 vs 4.7 months; P < 0.001), and median OS (29.6 vs 20.2 months; P < 0.001) in the lenalidomide-dexamethasone group when compared to the placebo-dexamethasone group. Adverse events associated with lenalidomide therapy were neutropenia, thrombocytopenia, and thromboembolic complications in both studies.Citation25,Citation26 There was a non-significant trend toward increased grade 3 or 4 infections in lenalidomide recipients.Citation25,Citation26
Table 1 Results from the two Phase III studies evaluating lenalidomide plus dexamethasone versus placebo plus dexamethasone
Pooled analysis of both randomized Phase III trials with an extended median follow-up of 48 months demonstrated a continued prolongation of overall survival for the lenalidomide-dexamethasone group (38.0 months) versus the dexamethasone single-agent group (31.6 months), despite a crossover of 48% of the patients to either lenalidomide or lenalidomide plus dexamethasone as subsequent salvage therapies.Citation27
Response to lenalidomide plus dexamethasone improved over time, with better quality of response associated with improved clinical outcomes. Median TTP and OS were longer in patients who achieved CR/very good partial response (VGPR) compared to patients who obtained a PR (TTP: 27.7 vs 12.0 months; OS: not yet reached vs 44.2 months).Citation28 San Miguel et al showed that patients who participated in MM-009 or MM-010 who achieved PR or better and continued therapy had an overall survival of 50.9 months, compared to 35.0 months in patients who discontinued lenalidomide-dexamethasone due to adverse events, withdrawal of consent, or other reasons.Citation29,Citation30 This suggests that continued treatment has a significant impact on survival, possibly by improving the depth of response.
Preliminary results from another pooled analysis of both Phase III studies showed that patients whose dexamethasone dose was reduced because of toxicity had a better outcome compared with patients who continued on high-dose dexamethasone.Citation31 In newly diagnosed MM, lenalidomide combined with low-dose dexamethasone was also associated with lower toxicity and better overall survival than lenalidomide with high-dose dexamethasone;Citation32 this has been widely adopted, even in the relapsed/refractory MM setting. An appropriate approach to minimize treatment-related toxicity in case of an aggressive relapse (eg, with hypercalcemia or renal failure) is to start with high-dose dexamethasone for rapid disease control, which can be followed by low-dose dexamethasone in case of response. Another subanalysis showed that patients with progression-free survival (PFS) ≥12 months who had dose reductions of lenalidomide after ≥12 months had better PFS than those who had earlier dose reductions or no dose reductions.Citation33 This suggests that it is important to continue full-dose lenalidomide therapy for at least 12 months in patients who tolerate the treatment, and after this time, the dose can be reduced without compromising treatment efficacy. Overall, these studies highlight the value of adverse event management and appropriate dose adjustments to prevent toxicity, thereby allowing continued treatment until disease progression.
Efficacy of lenalidomide plus dexamethasone and previous treatment
Stadtmauer et alCitation34 showed in a subset analysis of both Phase III trials that lenalidomide-dexamethasone was more effective in terms of response, TTP, PFS, and OS in patients who had one prior therapy when compared to those who had two or more earlier therapies, indicating that the greatest benefit occurs with early use of lenalidomide-dexamethasone in relapsed/refractory MM. Another pooled analysis of all patients that participated in these randomized trials showed that lenalidomide-dexamethasone was more effective than dexamethasone alone in both thalidomide-exposed and naïve patients.Citation35 However, higher efficacy in terms of overall response rate, TTP, and PFS of the combination of lenalidomide-dexamethasone or dexamethasone alone was observed in thalidomide-naïve patients compared to thalidomide-exposed patients, suggesting some degree of cross-resistance between thalidomide and lenalidomide. However, patients previously treated with thalidomide had significantly more prior lines of therapy compared with patients who were thalidomide naïve.Citation35 A French study showed similar results with inferior TTP and OS for patients that previously progressed on thalidomide.Citation36 In contrast, an Italian study showed that response, PFS, and OS were similar between thalidomide-resistant and thalidomide-sensitive patients.Citation37 A retrospective analysis performed in The Netherlands further showed that response rate was not influenced by previous thalidomide or bortezomib treatment.Citation38
In the MM-009 study, the response (≥PR) to lenalidomide-dexamethasone was 68% in bortezomib exposed and 60% in bortezomib naïve patients.Citation26 Results from the VISTA study also showed that lenalidomide-based therapy is equally effective in patients with or without previous bortezomib treatment.Citation39 In contrast, a French study highlighted that previous bortezomib exposure was associated with significantly shorter PFS and OS in patients treated with lenalidomide-dexamethasone when compared to patients with no earlier bortezomib treatment. However, patients who received bortezomib had a median of two additional lines of therapy, compared to patients who did not receive bortezomib.Citation36 Some other studies also suggest that prior bortezomib treatment is associated with lower efficacy of lenalidomide-dexamethasone.Citation40–Citation42 A retrospective single-center study showed that use of both thalidomide and bortezomib prior to lenalidomide-dexamethasone was associated with a significant reduction in TTP and OS.Citation41
Regimens with lenalidomide and conventional cytotoxic agents
Various other lenalidomide-based regimens have been studied to further improve the outcome of patients with relapsed/refractory MM (). Lenalidomide in combination with adriamycin and dexamethasone (RAD) in refractory and relapsed MM resulted in a high response rate of 73% (≥PR) including 15% CR and 45% VGPR, with hematologic toxicity and infections as the primary side effects.Citation43 Another lenalidomide and chemotherapy combination tested in the setting of relapsed/refractory MM was lenalidomide combined with pegylated liposomal doxorubicin, vincristine, and dexamethasone with an overall response rate (≥PR) of 75% including 29% CR or near CR.Citation44 Myelosuppression, neuropathy, muscle cramps, and rash were the most common adverse events. Median PFS was 12 months, and median OS had not been reached at the time of publication.
Table 2 Results from selected studies (n ≥ 30) in relapsed/refractory MM evaluating combinations of lenalidomide with conventional cytotoxic agents
Preliminary results from a phase I/II study show that the combination of lenalidomide with bendamustine and dexamethasone is effective and well tolerated.Citation45 Responses were also achieved in patients with prior exposure to lenalidomide. A variation on this regimen, bendamustine-lenalidomide plus prednisone followed by lenalidomide maintenance was evaluated in another Phase I trial. Preliminary results show that this combination was well tolerated and active in the setting of relapsed/refractory disease.Citation46
A retrospective study showed that the fully oral combination of lenalidomide (10 mg) with continuous low-dose cyclophosphamide (Endoxan, Baxter 100 mg orally [po]) and prednisone (REP) had a remarkably high activity with good tolerability in lenalidomide/dexamethasone-refractory MM (≥minimal response (MR): 64%; median PFS: 12.2 months).Citation47 The efficacy of cyclophosphamide combined with lenalidomide and corticosteroids has also been described by Morgan et al.Citation48 In a retrospective analysis, they treated relapsed lenalidomide-naïve MM patients with the combination of lenalidomide (25 mg; 21 days, followed by 1 week rest), cyclophosphamide (500 mg po; days 1, 8, 15, 21), and dexamethasone (40 mg po; days 1–4 and 12–15 of a 28-day cycle; RCD regimen) resulting in ≥MR in 75% of patients.Citation48 However, progression-free survival of 5.7 months seems inferior to REP (12.2 months). The prolonged progression-free survival of patients treated with the REP regimen may be attributed to the continuous exposure of tumor cells to antimyeloma agents in this regimen, which possibly prevents the emergence of resistant clones.
Based on the promising results from these retrospective studies, a prospective Phase I/II study of cyclophosphamide, lenalidomide, and dexamethasone was performed in relapsed/refractory lenalidomide-naïve MM with a median of three previous lines of therapy. The MTD was established at lenalidomide 25 mg on days 1–21, cyclophosphamide 600 mg on days 1 and 8, and dexamethasone 20 mg on days 1–4 and 8–11 of each 28-day cycle. Hematological toxicity could be easily managed by dose-reductions. Of all 31 evaluable patients, 81% achieved at least PR, including 29% CR.Citation49 The PFS at 2 years was 56%, and the OS at 30 months was 80%.Citation49 Another Phase I/II study is currently evaluating the combination of lenalidomide plus prednisone and cyclophosphamide, and has enrolled 32 lenalidomide-naïve patients.Citation50 Preliminary data show good tolerability with high efficacy.
Regimens with lenalidomide plus proteasome inhibitor
In vitro studies demonstrate that lenalidomide sensitizes MM cells to bortezomib-induced apoptosis, which provided the rationale for clinical studies evaluating this combination ().Citation6 A Phase I dose-escalation trial evaluated lenalidomide plus bortezomib in relapsed and refractory MM (median of five prior lines of therapy, including 87% of the patients with prior thalidomide, 55% with prior bortezomib, and 18% prior lenalidomide). Dexamethasone was added if the patient experienced progression after the second cycle. The MTD was lenalidomide 15 mg (days 1–14 of a 21-day cycle) and bortezomib 1.0 mg/m2 (days 1, 4, 8, 11).Citation51 MR or better was observed in 61% of the patients, which included 39% ≥ PR and 8% CR or near-CR. The most common treatment-related grade 3 to 4 toxicities included reversible neutropenia, thrombocytopenia, and anemia.Citation51 This study was followed by a Phase II trial, which evaluated the efficacy of this combination at the MTD in 64 patients with relapsed or refractory disease. Preliminary results show an impressive overall response rate (≥MR) of 78%, including 64% ≥ PR and 25% CR plus near-CR.Citation52
Table 3 Results from selected studies in relapsed/refractory MM evaluating combinations of lenalidomide with other novel agents (IMiDs and proteasome inhibitors)
Similar results were obtained in a Greek study, which demonstrated that the addition of bortezomib to lenalidomide-dexamethasone was associated with a high response rate of at least PR in 63% of patients (median of two previous lines of therapy).Citation53 Thalidomide-refractory disease was associated with an inferior response rate and survival.Citation53 Another study evaluated lenalidomide, bortezomib, and dexamethasone followed by lenalidomide-dexamethasone maintenance as treatment of first relapse after autologous stem cell transplantation. Preliminary data showed a promising response rate (≥PR: 71%; ≥VGPR: 43%) with a low toxicity profile.Citation54
The addition of pegylated doxorubicin to a modified schedule of lenalidomide-bortezomib-dexamethasone was evaluated in a Phase II study in relapsed/refractory MM. At least PR was achieved in 10 (56%) of 18 patients (median of four lines of prior therapy).Citation55
A dose-escalation study is investigating lenalidomide plus carfilzomib and dexamethasone in MM patients who have received a median of three previous therapies. Preliminary results show a response rate (≥PR) of 55% across all cohorts.Citation56 Responses were also observed in patients who had prior therapy with bortezomib or lenalidomide.
Lenalidomide-dexamethasone in combination with MLN9708, an oral, potent, reversible proteasome inhibitor, is currently being evaluated in newly diagnosed MM (NCT01217957 and NCT01383928). In addition, a phase III trial of weekly MLN9708, lenalidomide, and dexamethasone in patients with relapsed/refractory MM will soon be initiated (NCT01564537).
Regimens with lenalidomide and thalidomide
Based on a minimal overlapping side effect profile and different mechanisms of action between thalidomide (more antiangiogenic activity) and lenalidomide (more potent antiproliferative, cytotoxic, and immunomodulatory effects) in preclinical studies, the four-drug combination of lenalidomide, melphalan, prednisone, and thalidomide was tested in refractory/relapsed lenalidomide-naïve MM ().Citation57 A high response rate was observed, with 75% of the 44 patients achieving at least a PR, including 32% VGPR and 2% CR. Combining thalidomide with lenalidomide seems to increase the hematologic toxicity when compared to lenalidomide alone.
Another combination of both IMiDs is lenalidomide, thalidomide, and dexamethasoneCitation58 (). This combination was active, with at least PR in 12 out of 13 (92%) evaluable patients (median of three prior lines of therapy). Interestingly, seven of eight patients (88%) with lenalidomide-refractory disease achieved at least a PR, suggesting that thalidomide may modulate lenalidomide resistance.
Regimens with lenalidomide and new novel agents
mTor inhibitors
In vitro studies demonstrating synergistic antimyeloma activity between lenalidomide and mTor inhibitorsCitation59 provided the rationale for testing the combination of lenalidomide and temsirolimus in a Phase I trial in relapsed/refractory MM patients (n = 21, median of three previous lines of therapy including 19% lenalidomide). The maximum tolerated dose was lenalidomide 25 mg on days 1–21 of a 28-day cycle with 15 mg of temsirolimus weekly. Most common adverse events included fatigue, neutropenia, anemia, rash, and electrolyte abnormalities. The combination had modest activity, with PR in only two patients, and stable disease in 15 patients.Citation60
Another Phase I study evaluated RAD001 and lenalidomide in relapsed/refractory MM (28 patients with a median of four previous therapies, including 50% prior lenalidomide).Citation61 At least PR was obtained in 11% of patients.
Histone deacetylase inhibitors
A Phase I trial is evaluating vorinostat, lenalidomide plus dexamethasone in patients with relapsed/refractory MM.Citation62 Patients had received a median of four prior therapies including lenalidomide in 45%, thalidomide in 71%, and bortezomib in 65% cases. Fatigue, cytopenias, and diarrhea were the most common adverse events. At least PR was achieved in 53% of patients, including those previously exposed to lenalidomide. Median TTP was 5 months.
The combination of vorinostat, lenalidomide, and dexamethasone as a salvage therapy was also evaluated in 29 lenalidomide-dexamethasone-refractory MM patients with a median of four previous lines of therapy.Citation63 At least PR was achieved in 24% of patients, with a median duration of response of 4 months. Common toxicities included fatigue, myelosuppression, and diarrhea.
Akt inhibitor
Perifosine, an oral Akt inhibitor, was combined with lenalidomide and dexamethasone in a Phase I trial.Citation64 Patients had received a median of two prior lines of treatment, and patients refractory to lenalidomide plus dexamethasone were excluded. A total of 50% of the patients achieved at least PR, and median PFS was 10.8 months.
Lenalidomide and monoclonal antibody therapy
The ability of lenalidomide to activate multiple arms of the patient’s immune system including enhanced antibody-dependent cell-mediated cytotoxicity,Citation65,Citation66 coupled with its ability to modulate important signaling cascades in MM cells, forms the rationale to combine lenalidomide with monoclonal antibodies.Citation67 Preliminary results from ongoing trials show encouraging results with acceptable toxicity for lenalidomide combined with elotuzumab (anti-CS1 antibody),Citation68,Citation69 lorvotuzumab mertansine (anti-CD56 antibody conjugated to DM1),Citation70 and dacetuzumab (anti-CD40 antibody).Citation71
In vitro studies also demonstrated enhanced cytotoxicity of NK cells against MM cells of the combination of NK cell activating antibodies and lenalidomide, which also activates NK cells.Citation72 Based on these data, a Phase I/II trial is currently evaluating lenalidomide combined with 1-7F9, a fully human anti-KIR antibody, in relapsed/refractory MM.Citation72
Lenalidomide and cancer vaccines
Suppression of cytotoxic T cells by cytokines such as TGF-β, recruitment of regulatory T cells, and altered expression of immune suppressor molecules on MM cells or immune effector cells, contributes to immune evasion in MM. In addition, the function of dendritic cells and NK cells is severely impaired in MM. In a mouse model, a lymphoma vaccine in combination with lenalidomide improved survival when compared to vaccine or lenalidomide alone. Lenalidomide treatment was accompanied with enhanced cellular immunity and ameliorated immune suppression.Citation73 In vitro studies showed that lenalidomide also enhanced T cell activation in response to stimulation by a dendritic cell/MM fusion vaccine.Citation74 A recent clinical study in MM patients showed that lenalidomide augmented humoral and cellular responses to the polyvalent pneumococcal vaccine, Prevnar (Wyeth Pharmaceuticals, Inc, Madison, NJ; Pfizer Inc, New York, NY).Citation75 Altogether, these studies indicate that lenalidomide has the potential to improve immune dysfunction and can serve as an adjuvant for MM vaccines.
Increasing evidence also suggests that IMiDs enhance the graft-versus-myeloma effect mediated by donor T cells or donor NK cells after allogeneic stem cell transplantation or donor lymphocyte infusions.Citation76–Citation80 Unfortunately, use of IMiDs in this setting seems also to be associated with increased occurrence of graft-versus-host disease.Citation78,Citation79
Cytogenetics
Data from a Canadian study in relapsed or refractory MM suggest that lenalidomide-dexamethasone can overcome the poor prognosis conferred by del(13q) and t(4;14), but not del(17p) (all detected by fluorescence in situ hybridization).Citation40 However, results from a French multicenter study testing lenalidomide-dexamethasone in the relapsed setting showed an inferior PFS in patients with del(13q) and t(4;14).Citation36 Also, del(1p21) adversely affected the outcome of patients treated with lenalidomide-dexamethasone.Citation42
In other lenalidomide-based combinations, del(17p) remains a negative prognostic factor, with some combinations overcoming poor prognosis of both t(4;14) and del(13q). Response and TTP were identical in patients with or without del(13q) or t(4;14) following RAD treatment, but del(17p) remained associated with an inferior response rate and shortened TTP.Citation43 In addition, when bortezomib was added to lenalidomide-dexamethasone, del(17p) was still associated with an inferior response rate and survival. But bortezomib added to lenalidomide-dexamethasone overcame part of the adverse impact conferred by del(13q), ampl(1q21), and t(4;14).Citation53 The PFS of patients treated with lenalidomide, melphalan, prednisone and thalidomide was independent of the presence of del(13q), but was inferior in patients with t(4;14).Citation57
Lenalidomide treatment in frail or elderly patients with relapsed/refractory MM
More than half of all new cases of MM occur in patients 65 years of age or older,Citation81 whereas the proportion of elderly relapsed/refractory MM patients enrolled in clinical trials decreases with age, and no specific trials are currently available for unfit elderly MM patients. Furthermore, during the last decade, the improvement in survival was more pronounced in younger patients,Citation81 which is likely due to patient characteristics such as lower performance status and comorbidities in the elderly which strongly impact chemotherapy feasibility and tolerance. In addition, biologic differences between tumors may play a role. This highlights the need for further treatment innovations in this population.
Dose adjustments of lenalidomide and other components of the salvage regimen, such as dexamethasone, are needed to keep patients on therapy and prevent treatment discontinuation. Depending on the number of risk factors (such as age ≥ 75 years, frailty, and comorbidities), the starting dose of lenalidomide should be 25, 15, or 10 mg on days 1–21, and the starting dose of dexamethasone should be 40 mg, 20 mg, or 10 mg weekly.Citation82,Citation83 A Phase II trial in relapsed/refractory MM patients aged ≥60 years and/or with a creatinine clearance < 60 mL/min showed that lower doses of lenalidomide (15 mg) and dexamethasone reduced the incidence of hematological toxicities, infections, and VTE without compromising efficacy when compared to standard dose lenalidomide-dexamethasone (MM-010 and MM-009).Citation84 Another lenalidomide-containing salvage regimen with proven efficacy accompanied with mild toxicity, which may be beneficial to frail MM patients, includes dose-adjusted lenalidomide-cyclophosphamide-prednisone.Citation47 Careful monitoring of toxicity and prompt administration of supportive care such as G-CSF in case of neutropenia is important in this group of patients.
Renal impairment
Bortezomib clearance is independent of renal function and overcomes the adverse impact of renal dysfunction. Importantly, it also improves renal function to a higher degree than conventional chemotherapy or IMiD-based regimens. This suggests that relapsed/refractory patients presenting with renal insufficiency should receive bortezomib-based treatment. However, in case of bortezomib-refractory disease or intolerance to bortezomib, thalidomide or dose-adjusted lenalidomide-based regimens can be considered.Citation85
Lenalidomide is a renally metabolized drug, and without dose adjustments myelosuppression is more frequent in patients with renal impairment.Citation86–Citation88 In a subgroup analysis of MM-009 and MM-010 studies (starting dose of lenalidomide 25 mg for all patients), response and TTP was independent of renal function. Improvement of renal function was observed in the majority of patients with renal impairment. However, patients with severe renal impairment had a shorter OS.Citation87
With dosing of lenalidomide being administered according to creatinine clearance (), toxicity of lenalidomide was independent of renal function.Citation89 The response rate, PFS, and OS following lenalidomide-dexamethasone were identical between patients with and without renal impairment, and treatment was associated with improvement of renal function. However, a retrospective single center study from Germany with a starting dose of lenalidomide according to renal function showed that TTP following lenalidomide-dexamethasone was significantly shorter in the case of severe renal impairment, probably due to dose interruptions and reductions resulting from toxicity.Citation41
Table 4 Adjustment of lenalidomide dose in case of renal impairment
Adjusted dose lenalidomide-based therapy can also be administered to patients requiring dialysis, which is effective, but accompanied by a high incidence of neutropenia and infections.Citation90
Management of adverse events associated with lenalidomide
Neutropenia
Neutropenia increases the risk of bacterial and fungal infection, and is a common adverse event of lenalidomide treatment. The incidence of grade 3/4 neutropenia in the MM-009 and MM-010 studies was 41.2% and 29.5%, respectively, in lenalidomide plus dexamethasone-treated patients, whereas it was only 4.6% and 2.3%, respectively, in the placebo plus dexamethasone group.Citation25,Citation26 The risk of developing grade 3/4 neutropenia is higher when lenalidomide is combined with other chemotherapeutic agents such as alkylating drugs (eg, MPR) or doxorubicin (eg, RAD). Extensive previous treatment is also an important risk factor. Therapy-related toxicities including infections may lead to early treatment discontinuations, thereby negatively affecting outcomes.Citation91 When patients start with lenalidomide-based treatment, the blood counts should be monitored biweekly, but in case of pre-existing cytopenia, weekly monitoring is recommended. Growth factor support, and sometimes dose adjustments and dose interruptions, should be considered in case neutropenia develops (). Patients at high risk of developing neutropenia based on patient-, MM-, and treatment-related factors may benefit from primary prophylaxis with G-CSF.
Table 5 Supportive care for the management or prevention of adverse events associated with lenalidomide
Venous thromboembolism
Lenalidomide used as a single agent does not increase the risk of VTE. However, treatment with lenalidomide plus dexamethasone or cytotoxic agents results in a higher incidence of VTE.Citation25,Citation26,Citation48 In the MM-009 and MM-010 trials, the incidence of grade 3 and 4 thromboembolic events was 11.4% and 14.7%, respectively, in the lenalidomide plus dexamethasone group, which was significantly higher compared to 4.6% and 3.4%, respectively, in the placebo plus dexamethasone group.Citation25,Citation26 Importantly, in both studies thromboprophylaxis was not required. Risk factors for thromboembolic events associated with lenalidomide-dexamethasone treatment include high-dose dexamethasoneCitation32,Citation92–Citation94 and concomitant erythropoietin administration.Citation92,Citation94–Citation96 A subgroup analysis of the MM-009 and MM-010 trials showed an increased rate of VTE during lenalidomide-dexamethasone therapy in previously thalidomide-exposed patients when compared with thalidomide-naïve patients.Citation35 Interestingly, data suggest that the frequency of VTE may be markedly reduced when bortezomib is combined with IMiD-based regimens with high thrombogenic potential, even when no thromboprophylaxis was administered.Citation51,Citation97–Citation103
In addition, patient-related factors such as advanced age, history of VTE, immobilization, inherited thrombophilic disorders, and comorbidities such as diabetes mellitus and cardiac disease, contribute to the development of VTE during lenalidomide therapy. Patients treated with lenalidomide-dexamethasone who developed a VTE did not experience shorter OS or TTP.Citation104
Importantly, with thalidomide and lenalidomide-based combination therapies, prophylactic treatment with aspirin in patients at standard risk for VTE and low molecular weight heparin, or adjusted dose warfarin for high-risk patients reduces the frequency of VTE ().Citation93,Citation95,Citation96,Citation105,Citation106
Secondary malignancies
There have been recent concerns over the use of lenalidomide and the risk of developing second primary malignancies. There is an increased incidence of second primary malignancies in newly diagnosed MM patients receiving lenalidomide plus melphalan/prednisone (MPR).Citation107,Citation108 In the randomized Phase III, MM-015 study, the 3-year rate of invasive primary tumors was 7% in patients treated with MPR, 7% in patients treated with MPR followed by lenalidomide maintenance (MPR-R), but only 3% in the melphalan/prednisone group.Citation108 In addition, patients receiving lenalidomide maintenance following high-dose therapy with autologous stem cell rescue had a significantly higher incidence of second primary cancers.Citation109–Citation112 In the Intergroupe Francophone du Myelome trial, the incidence of second primary cancers was 3.1 per 100 patient-years in the lenalidomide group versus 1.2 per 100 patient-years in the placebo group.Citation111 In the CALGB study, 3.5% and 4.3% of the patients in the lenalidomide maintenance group developed new hematologic cancers and solid-tumor cancers (excluding nonmelanoma skin cancers), respectively.Citation112 The corresponding numbers are 0.4% and 2.2% in the placebo group.Citation112
A retrospective pooled analysis of 11 clinical trials of lenalidomide-based therapy has addressed this issue in the relapsed/refractory setting;Citation113 however, in the absence of prospective studies, conclusions regarding the incidence of second primary cancers are more difficult to draw. In a pooled analysis of 3846 relapsed/refractory MM patients treated with lenalidomide as a single agent (7%) or in combination with dexamethasone (93%), the incidence rate (events per 100 patient-years) of invasive second primary malignancies was 2.08, which is comparable to that expected according to the Surveillance, Epidemiology and End Results cancer registry (2.1).Citation113 The incidence rates (events per 100 patient-years) of second primary malignancies, excluding noninvasive skin cancers, in the MM-009 and MM-010 trials was 1.71 for lenalidomide plus dexamethasone, and 0.91 for placebo plus dexamethasone. This difference was not statistically significant, and it was also consistent with the expected incidence of invasive cancer in the general population.Citation113 However, there was an increased occurrence of noninvasive skin cancers in the lenalidomide plus dexamethasone group compared to the dexamethasone only group (incidence rate: 2.40 vs 0.91). Although there is an increased incidence of non-invasive skin cancers in this patient group, there remains a positive risk-benefit profile of lenalidomide plus dexamethasone in relapsed/refractory MM.Citation113
Other adverse events
Other common adverse events associated with lenalidomide treatment include thrombocytopenia, anemia, rash, and diarrhea. These toxicities can be managed with dose reductions or interruptions, as well as with the start of appropriate supportive care ().Citation114
Concluding remarks
Lenalidomide plus dexamethasone and other lenalidomide-based combinations are effective treatment options for relapsed/refractory MM patients. Several studies demonstrate that continued treatment with lenalidomide is associated with improved survival. Appropriate dose adjustments and institution of supportive care are therefore very important to enable patients to continue treatment with lenalidomide-based therapies until disease progression.
The introduction of the novel agents, thalidomide, lenalidomide, and bortezomib,Citation115 and the application of high-dose therapy with autologous stem cell rescue have improved the survival of MM patients. However, event-free and overall survival for patients that are refractory to both an IMiD and bortezomib is only 5 and 9 months, respectively,Citation116 indicating that new drugs are still needed for continued disease control. Novel agents are currently being evaluated in clinical trials, and include second generation IMiDs such as pomalidomide, and second generation proteasome inhibitors, such as carfilzomib, MLN 9708, and marizomib. Drugs belonging to other classes, such as histone deacetylase inhibitors, Akt inhibitors, mTor inhibitors, and several monoclonal antibodies including elotuzumab and daratumumab, hold promise for improving the outcome of patients with lenalidomide and bortezomib refractory disease.Citation67,Citation117 Incorporation of biomarker assessment (using techniques such as fluorescence in situ hybridization, gene expression profiling, array based comparative genomic hybridization, single nucleotide polymorphism array, microRNA array, or high throughput sequencing) in future studies in relapsed/refractory MM will help to evaluate the risk/benefit profile and tailor individualized therapeutic approaches. Altogether, this will hopefully translate to further improvement in outcomes for MM patients.
Acknowledgment
NWCJvdD was supported by the Dutch Cancer Society.
Notes
Conflict of interest disclosure
NWCJvdD has received research support from Celgene, and honoraria as a speaking fee from Johnson and Johnson and Celgene. CSM has received in the past honoraria from Millennium Pharmaceuticals, Novartis Pharmaceuticals, Bristol-Myers Squibb, Merck and Co, Celgene, licensing royalties from PharmaMar, and research funding from Amgen Pharmaceuticals, AVEO Pharma, EMD Serono, Sunesis, and Johnson and Johnson. HML has received research support from Celgene, Genmab, and Ortho-Biotech. PGR has served on the advisory board of Millennium Pharmaceuticals, Celgene Corporation, Novartis, Johnson and Johnson, and Bristol Myers Squibb. KCA is the scientific founder of Acetylon, and is on the advisory boards of Celgene, Millennium, Onyx, BMS, and Merck. GG, RWJG, JJ, TH, JPL, ISN, and RAR declare no competing financial interests.
References
- KotlaVGoelSNischalSMechanism of action of lenalidomide in hematological malignanciesJ Hematol Oncol200923619674465
- ValletSWitzens-HarigMJaegerDPodarKUpdate on immunomodulatory drugs (IMiDs) in hematologic and solid malignanciesExpert Opin Pharmacother201213447349422324734
- DaviesFBazRLenalidomide mode of action: linking bench and clinical findingsBlood Rev201024 Suppl 1S13S1921126632
- RichardsonPGSchlossmanRLWellerEImmunomodulatory drug CC-5013 overcomes drug resistance and is well tolerated in patients with relapsed multiple myelomaBlood200210093063306712384400
- HideshimaTChauhanDShimaYThalidomide and its analogs overcome drug resistance of human multiple myeloma cells to conventional therapyBlood20009692943295011049970
- MitsiadesNMitsiadesCSPoulakiVApoptotic signaling induced by immunomodulatory thalidomide analogs in human multiple myeloma cells: therapeutic implicationsBlood200299124525453012036884
- VerhelleDCorralLGWongKLenalidomide and CC-4047 inhibit the proliferation of malignant B cells while expanding normal CD34+ progenitor cellsCancer Res200767274675517234786
- JakubikovaJAdamiaSKost-AlimovaMLenalidomide targets clonogenic side population in multiple myeloma: pathophysiologic and clinical implicationsBlood2011117174409441921321360
- ItoTAndoHSuzukiTIdentification of a primary target of thalidomide teratogenicityScience201032759711345135020223979
- ZhuYXBraggioEShiCXCereblon expression is required for the antimyeloma activity of lenalidomide and pomalidomideBlood2011118184771477921860026
- GeitzHHandtSZwingenbergerKThalidomide selectively modulates the density of cell surface molecules involved in the adhesion cascadeImmunopharmacology1996312–32132218861747
- HideshimaTChauhanDSchlossmanRRichardsonPAndersonKCThe role of tumor necrosis factor alpha in the pathophysiology of human multiple myeloma: therapeutic applicationsOncogene200120334519452711494147
- CorralLGHaslettPAMullerGWDifferential cytokine modulation and T cell activation by two distinct classes of thalidomide analogues that are potent inhibitors of TNF-alphaJ Immunol1999163138038610384139
- GuptaDTreonSPShimaYAdherence of multiple myeloma cells to bone marrow stromal cells upregulates vascular endothelial growth factor secretion: therapeutic applicationsLeukemia200115121950196111753617
- De LuisiAFerrucciAColucciaAMLenalidomide restrains motility and overangiogenic potential of bone marrow endothelial cells in patients with active multiple myelomaClin Cancer Res20111771935194621307145
- BreitkreutzIRaabMSValletSLenalidomide inhibits osteoclastogenesis, survival factors and bone-remodeling markers in multiple myelomaLeukemia200822101925193218596740
- DaviesFERajeNHideshimaTThalidomide and immunomodulatory derivatives augment natural killer cell cytotoxicity in multiple myelomaBlood200198121021611418482
- ChangDHLiuNKlimekVEnhancement of ligand-dependent activation of human natural killer T cells by lenalidomide: therapeutic implicationsBlood2006108261862116569772
- GalustianCMeyerBLabartheMCThe anti-cancer agents lenalidomide and pomalidomide inhibit the proliferation and function of T regulatory cellsCancer Immunol Immunother20095871033104519009291
- MullerGWChenRHuangSYAmino-substituted thalidomide analogs: potent inhibitors of TNF-alpha productionBioorg Med Chem Lett19999111625163010386948
- LeBlancRHideshimaTCatleyLPImmunomodulatory drug costimulates T cells via the B7-CD28 pathwayBlood200410351787179014512311
- GorgunGCalabreseESoydanEImmunomodulatory effects of lenalidomide and pomalidomide on interaction of tumor and bone marrow accessory cells in multiple myelomaBlood2010116173227323720651070
- RichardsonPGBloodEMitsiadesCSA randomized phase 2 study of lenalidomide therapy for patients with relapsed or relapsed and refractory multiple myelomaBlood2006108103458346416840727
- RichardsonPJagannathSHusseinMSafety and efficacy of single-agent lenalidomide in patients with relapsed and refractory multiple myelomaBlood2009114477277819471019
- DimopoulosMSpencerAAttalMfor Multiple Myeloma (010) Study InvestigatorsLenalidomide plus dexamethasone for relapsed or refractory multiple myelomaN Engl J Med2007357212123213218032762
- WeberDMChenCNiesvizkyRfor Multiple Myeloma (009) Study InvestigatorsLenalidomide plus dexamethasone for relapsed multiple myeloma in North AmericaN Engl J Med2007357212133214218032763
- DimopoulosMAChenCSpencerALong-term follow-up on overall survival from the MM-009 and MM-010 phase III trials of lenalidomide plus dexamethasone in patients with relapsed or refractory multiple myelomaLeukemia200923112147215219626046
- HarousseauJLDimopoulosMAWangMBetter quality of response to lenalidomide plus dexamethasone is associated with improved clinical outcomes in patients with relapsed or refractory multiple myelomaHaematologica201095101738174420460639
- San-MiguelJFDimopoulosMAStadtmauerEAEffects of lenalidomide and dexamethasone treatment duration on survival in patients with relapsed or refractory multiple myeloma treated with lenalidomide and dexamethasoneClin Lymphoma Myeloma Leuk2011111384321273172
- San MiguelJDimopoulosMBravoMLWeberDLonger duration of treatment and maintenance of best response with lenalidomide + dexamethasone increases overall survival (OS) in patients with relapsed/refractory multiple myeloma [abstract]Haematologica200994Suppl 2382
- San MiguelJFDimopoulosMWeberDDexamethasone dose adjustments seem to result in better efficacy and improved tolerability in patients with relapsed/refractory multiple myeloma who are treated with lenalidomide/dexamethasone (MM009/010 sub-analysis) [abstract]Blood (ASH Annual Meeting Abstracts)2007110112712
- RajkumarSVJacobusSCallanderNSfor Eastern Cooperative Oncology GroupLenalidomide plus high-dose dexamethasone versus lenalidomide plus low-dose dexamethasone as initial therapy for newly diagnosed multiple myeloma: an open-label randomised controlled trialLancet Oncol2010111293719853510
- DimopoulosMAHusseinMSwernASWeberDImpact of lenalidomide dose on progression-free survival in patients with relapsed or refractory multiple myelomaLeukemia201125101620162621747400
- StadtmauerEAWeberDMNiesvizkyRLenalidomide in combination with dexamethasone at first relapse in comparison with its use as later salvage therapy in relapsed or refractory multiple myelomaEur J Haematol200982642643219302559
- WangMDimopoulosMAChenCLenalidomide plus dexamethasone is more effective than dexamethasone alone in patients with relapsed or refractory multiple myeloma regardless of prior thalidomide exposureBlood2008112124445445118799726
- Avet-LoiseauHSoulierJFermandJPfor IFM MAG groupsImpact of high-risk cytogenetics and prior therapy on outcomes in patients with advanced relapsed or refractory multiple myeloma treated with lenalidomide plus dexamethasoneLeukemia201024362362820072152
- GuglielmelliTBringhenSRrodheSPrevious thalidomide therapy may not affect lenalidomide response and outcome in relapse or refractory multiple myeloma patientsEur J Cancer201147681481821334196
- KneppersELokhorstHMEeltinkCMAnalysis of efficacy and prognostic factors of lenalidomide treatment as part of a Dutch compassionate use programClin Lymphoma Myeloma Leuk201010213814320371448
- MateosMVRichardsonPGSchlagRBortezomib plus melphalan and prednisone compared with melphalan and prednisone in previously untreated multiple myeloma: updated follow-up and impact of subsequent therapy in the phase III VISTA trialJ Clin Oncol201028132259226620368561
- ReeceDSongKWFuTInfluence of cytogenetics in patients with relapsed or refractory multiple myeloma treated with lenalidomide plus dexamethasone: adverse effect of deletion 17p13Blood2009114352252519332768
- KleinUNebenKHielscherTHeissCHoADGoldschmidtHLenalidomide in combination with dexamethasone: effective regimen in patients with relapsed or refractory multiple myeloma complicated by renal impairmentAnn Hematol201190442943920857112
- ChangHJiangAQiCTrieuYChenCReeceDImpact of genomic aberrations including chromosome 1 abnormalities on the outcome of patients with relapsed or refractory multiple myeloma treated with lenalidomide and dexamethasoneLeuk Lymphoma201051112084209120929319
- KnopSGereckeCLiebischPLenalidomide, adriamycin, and dexamethasone (RAD) in patients with relapsed and refractory multiple myeloma: a report from the German Myeloma Study Group DSMM (Deutsche Studiengruppe Multiples Myelom)Blood2009113184137414319182205
- BazRWalkerEKaramMALenalidomide and pegylated liposomal doxorubicin-based chemotherapy for relapsed or refractory multiple myeloma: safety and efficacyAnn Oncol200617121766177116980599
- LentzschSO’SullivanAKennedyRCombination of bendamustine, lenalidomide, and dexamethasone (BLD) in patients with refractory or relapsed multiple myeloma is safe and highly effective: results of phase I/II open-label, dose escalation study [abstract]Blood (ASH Annual Meeting Abstracts)201111821304
- PonischWHeynSWagnerICombined bendamustine, prednisolone and lenalidomide (RBP) in refractory or relapsed multiple myeloma. First results of a phase I clinical trial [abstract]Blood (ASH Annual Meeting Abstracts)2010116211971
- van de DonkNWWittebolSMinnemaMCLokhorstHMLenalidomide (Revlimid) combined with continuous oral cyclophosphamide (endoxan) and prednisone (REP) is effective in lenalidomide/dexamethasone-refractory myelomaBr J Haematol2010148233533720085583
- MorganGJScheySAWuPLenalidomide (Revlimid), in combination with cyclophosphamide and dexamethasone (RCD), is an effective and tolerated regimen for myeloma patientsBr J Haematol2007137326826917408469
- ScheySAMorganGJRamasamyKThe addition of cyclophosphamide to lenalidomide and dexamethasone in multiply relapsed/refractory myeloma patients; a phase I/II studyBr J Haematol2010150332633320553268
- ReeceDEMasih-KhanEKhanAPhase I-II trial of oral cyclophosphamide, prednisone and lenalidomide (Revlimid(R)) (CPR) for the treatment of patients with relapsed and refractory multiple myeloma [abstract]Blood (ASH Annual Meeting Abstracts)2010116213055
- RichardsonPGWellerEJagannathSMulticenter, phase I, dose-escalation trial of lenalidomide plus bortezomib for relapsed and relapsed/refractory multiple myelomaJ Clin Oncol200927345713571919786667
- RichardsonPGJagannathSJakubowiakAJPhase II trial of lenalidomide, bortezomib, and dexamethasone in patients (pts) with relapsed and relapsed/refractory multiple myeloma (MM): updated efficacy and safety data after >2 years of follow-up [abstract]Blood (ASH Annual Meeting Abstracts)2010116213049
- DimopoulosMAKastritisEChristoulasDTreatment of patients with relapsed/refractory multiple myeloma with lenalidomide and dexamethasone with or without bortezomib: prospective evaluation of the impact of cytogenetic abnormalities and of previous therapiesLeukemia201024101769177820739955
- BelhadjKAmraouiKSafarVLenalidomide plus bortezomib and dexamethasone (RVD) followed by lenalidomide plus dexamethasone as salvage treatment for myeloma patients in first relapse after autologous stem cell transplantation. Single institution experience [abstract]Blood (ASH Annual Meeting Abstracts)2011118215143
- BerensonJRYellinOCartmellADA phase II study of pegylated liposomal doxorubicin (PLD), bortezomib, dexamethasone and lenalidomide (DVD-R) for patients with relapsed/refractory (R/R) multiple myeloma (MM) [abstract]Blood (ASH Annual Meeting Abstracts)2010116213044
- NiesvizkyRWangLOrlowskiRZPhase Ib multicenter dose escalation study of carfilzomib plus lenalidomide and low dose dexamethasone (CRd) in relapsed and refractory multiple myeloma (MM) [abstract]Blood (ASH Annual Meeting Abstracts)1120200911422304
- PalumboALaroccaAFalcoPLenalidomide, melphalan, prednisone and thalidomide (RMPT) for relapsed/refractory multiple myelomaLeukemia20102451037104220376079
- ShahJJOrlowskiRZAlexanianRPhase I trial of the combination of lenalidomide, thalidomide and dexamethasone in relapsed/refractory multiple myeloma [abstract]Blood (ASH Annual Meeting Abstracts)2010116211948
- RajeNKumarSHideshimaTCombination of the mTOR inhibitor rapamycin and CC-5013 has synergistic activity in multiple myelomaBlood2004104134188419315319277
- HofmeisterCCYangXPichiorriFPhase I trial of lenalidomide and CCI-779 in patients with relapsed multiple myeloma: evidence for lenalidomide-CCI-779 interaction via P-glycoproteinJ Clin Oncol201129253427343421825263
- MahindraARichardsonPGHariPUpdated results of a phase I study of RAD001 in combination with lenalidomide in patients with relapsed or refractory multiple myeloma with pharmacodynamic and pharmacokinetic analysis [abstract]Blood (ASH Annual Meeting Abstracts)2010116213051
- RichardsonPWeberDMitsiadesCSA phase I study of vorinostat, lenalidomide, and dexamethasone in patients with relapsed or relapsed and refractory multiple myeloma: excellent tolerability and promising activity in a heavily pretreated population [abstract]Blood (ASH Annual Meeting Abstracts)2010116211951
- RichterJRBilottiEMcBrideLSalvage therapy with vorinostat, lenalidomide, and dexamethasone (ZRD) in lenalidomide/dexamethasone relapsed/refractory multiple myeloma [abstract]Blood (ASH Annual Meeting Abstracts)2011118213986
- JakubowiakAJRichardsonPGZimmermanTMFinal phase I results of perifosine in combination with lenalidomide and dexamethasone in patients with relapsed or refractory multiple myeloma (MM) [abstract]Blood (ASH Annual Meeting Abstracts)2010116213064
- QuachHRitchieDStewartAKMechanism of action of immunomodulatory drugs (IMiDS) in multiple myelomaLeukemia2010241223219907437
- HayashiTHideshimaTAkiyamaMMolecular mechanisms whereby immunomodulatory drugs activate natural killer cells: clinical applicationBr J Haematol2005128219220315638853
- van de DonkNWKampsSMutisTLokhorstHMMonoclonal antibody-based therapy as a new treatment strategy in multiple myelomaLeukemia201226219921321852787
- LonialSJakubowiakAJJagannathSA phase 2 study of elotuzumab in combination with lenalidomide and low-dose dexamethasone in patients with relapsed/refractory multiple myeloma [abstract]Blood (ASH Annual Meeting Abstracts)201111821303
- LonialSVijRHarousseauJLElotuzumab in combination with lenalidomide and low-dose dexamethasone in relapsed or refractory multiple myelomaJ Clin Oncol201230161953195922547589
- BerdejaJGAilawadhiSNiesvizkyRPhase I study of lorvotuzumab mertansine (IMGN901) in combination with lenalidomide and dexamethasone in patients with CD56-positive relapsed or relapsed/refractory multiple myeloma – a preliminary safety and efficacy analysis of the combination [abstract]Blood (ASH Annual Meeting Abstracts)2010116211934
- AguraENiesvizkyRMatousJDacetuzumab (SGN-40), lenalidomide, and weekly dexamethasone in relapsed or refractory multiple myeloma: multiple responses observed in a phase 1b study [abstract]Blood (ASH Annual Meeting Abstracts)2009114222870
- ZhangSLiangJChenLEnhanced NK cell mediated cytotoxicity against multiple myeloma (MM) cells by the combination of anti-KIR (1-7F9) monoclonal antibody (mAb) and lenalidomide [abstract]AACR Meeting Abstracts20092_Annual_Meeting3245
- SakamakiIKaplanBChaS-CQinHKwakLWPotent immunomodulatory effects of lenalidomide on effector T cells and Treg improve the effectiveness of a therapeutic lymphoma vaccine [abstract]Blood (ASH Annual Meeting Abstracts)201111821108
- LuptakovaKGlotzbeckerBMillsHLenalidomide decreases PD-1 expression, depletes regulatory T-cells and improves cellular response to a multiple myeloma/dendritic cell fusion vaccine in vitro [abstract]Blood (ASH Annual Meeting Abstracts)201011621492
- NoonanKRudrarajuLFergusonALenalidomide-induced immunomodulation in multiple myeloma: impact on vaccines and antitumor responsesClin Cancer Res20121851426143422241792
- van de DonkNWKrogerNHegenbartURemarkable activity of novel agents bortezomib and thalidomide in patients not responding to donor lymphocyte infusions following nonmyeloablative allogeneic stem cell transplantation in multiple myelomaBlood200610783415341616597603
- KrogerNBadbaranALioznovMPost-transplant immunotherapy with donor-lymphocyte infusion and novel agents to upgrade partial into complete and molecular remission in allografted patients with multiple myelomaExp Hematol200937779179819487069
- MinnemaMCvan der VeerMSAartsTEmmelotMMutisTLokhorstHMLenalidomide alone or in combination with dexamethasone is highly effective in patients with relapsed multiple myeloma following allogeneic stem cell transplantation and increases the frequency of CD4+Foxp3+ T cellsLeukemia200923360560718784738
- KneppersEvan der HoltBKerstenMJLenalidomide maintenance after nonmyeloablative allogeneic stem cell transplantation in multiple myeloma is not feasible: results of the HOVON 76 TrialBlood201111892413241921690556
- El-CheikhJCrocchioloRFurstSLenalidomide plus donor-lymphocytes infusion after allogeneic stem-cell transplantation with reduced-intensity conditioning in patients with high-risk multiple myelomaExp Hematol201240752152722446605
- KumarSKRajkumarSVDispenzieriAImproved survival in multiple myeloma and the impact of novel therapiesBlood200811152516252017975015
- PalumboAAndersonKMultiple myelomaN Engl J Med2011364111046106021410373
- PalumboABringhenSLudwigHPersonalized therapy in multiple myeloma according to patient age and vulnerability: a report of the European Myeloma Network (EMN)Blood2011118174519452921841166
- QuachHFernyhoughLHendersonRLower-dose lenalidomide and dexamethasone reduces toxicity without compromising efficacy in patients with relapsed/refractory myeloma, who are aged ≥60 years or have renal impairment: planned interim results of a prospective multicentre phase II trial [abstract]Blood (ASH Annual Meeting Abstracts)2010116211961
- DimopoulosMATerposEGoldschmidtHAlegreAMarkTNiesvizkyRTreatment with lenalidomide and dexamethasone in patients with multiple myeloma and renal impairmentCancer Treat Rev5182012 [Epub ahead of print.]
- NiesvizkyRNaibTChristosPJLenalidomide-induced myelosuppression is associated with renal dysfunction: adverse events evaluation of treatment-naive patients undergoing front-line lenalidomide and dexamethasone therapyBr J Haematol2007138564064317686058
- DimopoulosMAlegreAStadtmauerEAThe efficacy and safety of lenalidomide plus dexamethasone in relapsed and/or refractory multiple myeloma patients with impaired renal functionCancer2010116163807381420564094
- KleberMIhorstGUdiJKochBWaschREngelhardtMPrognostic risk factor evaluation in patients with relapsed or refractory multiple myeloma receiving lenalidomide treatment: analysis of renal function by eGFR and of additional comorbidities by comorbidity appraisalClin Lymphoma Myeloma Leuk2012121384822054851
- DimopoulosMAChristoulasDRoussouMLenalidomide and dexamethasone for the treatment of refractory/relapsed multiple myeloma: dosing of lenalidomide according to renal function and effect on renal impairmentEur J Haematol20108511520192988
- de la RubiaJRoigMIbanezAActivity and safety of lenalidomide and dexamethasone in patients with multiple myeloma requiring dialysis: a Spanish multicenter retrospective studyEur J Haematol201085436336520662900
- PalumboABladeJBoccadoroMHow to manage neutropenia in multiple myelomaClin Lymphoma Myeloma Leuk201212151122178143
- BennettCLAngelottaCYarnoldPRThalidomide- and lenalidomide-associated thromboembolism among patients with cancerJAMA2006296212558256017148721
- ZonderJABarlogieBDurieBGMcCoyJCrowleyJHusseinMAThrombotic complications in patients with newly diagnosed multiple myeloma treated with lenalidomide and dexamethasone: benefit of aspirin prophylaxisBlood20061081403 author reply 40416790586
- KnightRDeLapRJZeldisJBLenalidomide and venous thrombosis in multiple myelomaN Engl J Med2006354192079208016687729
- PalumboARajkumarSVDimopoulosMAfor International Myeloma Working GroupPrevention of thalidomide- and lenalidomide-associated thrombosis in myelomaLeukemia200822241442318094721
- LaroccaACavalloFBringhenSAspirin or enoxaparin thromboprophylaxis for patients with newly diagnosed multiple myeloma treated with lenalidomideBlood20121194933939 quiz 109321835953
- LonialSRichardsonPGSan MiguelJCharacterisation of haematological profiles and low risk of thromboembolic events with bortezomib in patients with relapsed multiple myelomaBr J Haematol2008143222222918713253
- Pineda-RomanMZangariMvan RheeFVTD combination therapy with bortezomib-thalidomide-dexamethasone is highly effective in advanced and refractory multiple myelomaLeukemia20082271419142718432260
- CiolliSLeoniFCasiniCBreschiCSantiniVBosiAThe addition of liposomal doxorubicin to bortezomib, thalidomide and dexamethasone significantly improves clinical outcome of advanced multiple myelomaBr J Haematol2008141681481918410447
- CiolliSLeoniFGigliFRigacciLBosiALow dose Velcade, thalidomide and dexamethasone (LD-VTD): an effective regimen for relapsed and refractory multiple myeloma patientsLeuk Lymphoma200647117117316321846
- PalumboAAmbrosiniMTBenevoloGfor Italian Multiple Myeloma Network, Gruppo Italiano Malattie Ematologicche dell’AdultoBortezomib, melphalan, prednisone, and thalidomide for relapsed multiple myelomaBlood200710972767277217148584
- TerposEKastritisERoussouMThe combination of bortezomib, melphalan, dexamethasone and intermittent thalidomide is an effective regimen for relapsed/refractory myeloma and is associated with improvement of abnormal bone metabolism and angiogenesisLeukemia200822122247225618769451
- ZangariMFinkLZhanFTricotGLow venous thromboembolic risk with bortezomib in multiple myeloma and potential protective effect with thalidomide/lenalidomide-based therapy: review of data from phase 3 trials and studies of novel combination regimensClin Lymphoma Myeloma Leuk201111222823621575928
- ZangariMTricotGPolavaramLSurvival effect of venous thromboembolism in patients with multiple myeloma treated with lenalidomide and high-dose dexamethasoneJ Clin Oncol201028113213519901114
- RajkumarSVHaymanSRLacyMQCombination therapy with lenalidomide plus dexamethasone (Rev/Dex) for newly diagnosed myelomaBlood2005106134050405316118317
- KleinUKoselyFHillengassJEffective prophylaxis of thromboembolic complications with low molecular weight heparin in relapsed multiple myeloma patients treated with lenalidomide and dexamethasoneAnn Hematol2009881677118668241
- PalumboADelforgeMCatalanoJA phase 3 study evaluating the efficacy and safety of lenalidomide combined with melphalan and prednisone In patients ≥ 65 years with newly diagnosed multiple myeloma (NDMM): continuous use of lenalidomide vs fixed-duration regimens [abstract]Blood (ASH Annual Meeting Abstracts)201011621622
- PalumboAHajekRDelforgeMfor MM-015 InvestigatorsContinuous lenalidomide treatment for newly diagnosed multiple myelomaN Engl J Med2012366191759176922571200
- AttalMLauwersVcMaritGMaintenance treatment with lenalidomide after transplantation for MYELOMA: final analysis of the IFM 2005–2002 [abstract]Blood (ASH Annual Meeting Abstracts)201011621310
- McCarthyPOwzarKAndersonKPhase III intergroup study of lenalidomide versus placebo maintenance therapy following single autologous stem cell transplant (ASCT) for multiple myeloma (MM): CALGB ECOG BMT-CTN 100104Haematologica201196s1S23
- AttalMLauwers-CancesVMaritGfor IFM InvestigatorsLenalidomide maintenance after stem-cell transplantation for multiple myelomaN Engl J Med2012366191782179122571202
- McCarthyPLOwzarKHofmeisterCCLenalidomide after stem-cell transplantation for multiple myelomaN Engl J Med2012366191770178122571201
- DimopoulosMARichardsonPGBrandenburgNA review of second primary malignancy in patients with relapsed or refractory multiple myeloma treated with lenalidomideBlood2012119122764276722323483
- DimopoulosMAPalumboAAttalMfor European Myeloma NetworkOptimizing the use of lenalidomide in relapsed or refractory multiple myeloma: consensus statementLeukemia201125574976021293488
- BarosiGMerliniGBillioASIE, SIES, GITMO evidence-based guidelines on novel agents (thalidomide, bortezomib, and lenalidomide) in the treatment of multiple myelomaAnn Hematol201291687588822476884
- KumarSKLeeJHLahuertaJJfor International Myeloma Working GroupRisk of progression and survival in multiple myeloma relapsing after therapy with IMiDs and bortezomib: a multicenter international myeloma working group studyLeukemia201226114915721799510
- van de DonkNWLokhorstHMDimopoulosMTreatment of relapsed and refractory multiple myeloma in the era of novel agentsCancer Treat Rev201137426628320863623