
Abstract
Introduction
Research in mice showed that vitamin D receptor deficiency was correlated with an increased rate of non-melanoma skin cancer. Therapeutic supplemental vitamin D has also been reported to reduce cell growth in both melanoma and non-melanoma skin cancer. This paper aims to describe the existing research studies that discuss the potential and role of vitamin D in the management of skin cancer.
Methods
Articles were searched from three databases (PubMed, ScienceDirect, Scopus) and manual search. 18 articles were included. These were further divided into in vivo and in vitro studies. The literature search was based on the following Patients, Intervention, Control, and Outcome (PICO) criteria: Patients with any types of skin cancer; Vitamin D and their derivates as the intervention; placebo or standard regimen as control, and survival rate or response rate as primary outcome.
Results
From the three databases, we obtained 802 studies. Prior to screening of the literature obtained, several studies were excluded. In the eligibility assessment, seven studies were excluded due to their outcomes being not eligible for analysis, and two studies were excluded due to inaccessible full texts. The remaining 18 studies were included. Five studies had a clinical research design (randomized controlled trial or interventional study), which use vitamin D3 as vitamin D derivatives and the results showed that the administration of vitamin D3 reduces the proliferation of skin cancer cells. Similar results were also reported in studies with pre-clinical research designs, either in vivo or in vitro, where six were in vivo studies and nine studies were in vitro studies.
Conclusion
Our literature review revealed that that vitamin D derivatives, such as 1,25(OH)2D3 or 20(OH)D3 can effectively reduce the proliferation of skin cancer cells by contributing in the inhibition of cell growth and development, highlighting vitamin D’s role as good prognostic factor.
Introduction
Laboratory and animal studies have shown the potential of vitamin D in preventing the progression of carcinogenesis and slow the growth of tumor cells, where the known mechanisms include promoting cell differentiation, preventing cancer cell proliferation, and effects on cancer cells such as anti-inflammatory, immunomodulatory, antiangiogenic and proapoptotic effects through autophagy.Citation1 Skin cancer is the most prevalent malignancy in the United States, with more than 1 million incidence annually.Citation2 For more than 40 years, there has been a rapid increase in the incidence of skin cancer, both non-melanoma and melanoma skin cancer, especially in female population.Citation3 The rising case might be explained by the increasing sunray and ultraviolet exposure with poor sun-protective behavior, compounded with ozone depletion and particular tan-seeking behaviour in western societies.Citation4,Citation5 Similar trend has also been observed in various regions, such as Australia as the highest country with skin cancer incidence rate. The increasing incidence happens in both squamous cell or non-squamous cell carcinoma.Citation4,Citation5
Numerous studies have discussed the morbidity and mortality of skin cancer in advanced stages, and the identification of chemopreventive agents, especially for skin cancer, needs to be reviewed further; As of now, only nicotinamide is demonstrated to have chemopreventive property for skin cancer.Citation6 Recently, interest in the chemopreventive effects of the vitamin D has revealed its potential D in reducing the risk of several cancers such as colon, prostate and breast cancers. A randomized controlled trial (RCT) showed a significant reduction on the overall incidence of all cancer types with calcium and vitamin D supplementation.Citation7 Vitamin D is a fat-soluble vitamin, which could be obtained from daily diet and can be produced by the skin, mediated by ultraviolet B ray from sun exposure.Citation7,Citation8 Also, a precursor of steroid hormones, vitamin D undergoes two stages of metabolism in the liver and kidneys which eventually produces calcitriol.Citation8 Calcitriol will bind to vitamin D receptors and activate the physiological functions of vitamin D.Citation8 The general physiological function of vitamin D is to maintain or control the metabolism of both calcium and phosphate, which can be utilized for bone remodeling. However, current studies have found that low sunlight exposure and vitamin D deficiency are correlated with the increase of various risk factors for diseases outside the musculoskeletal system, one of which is cancer.Citation8 A review of various studies suggested that vitamin D could regulate all processes from tumor cell formation, initiation of metastasis, as well as interactions between cells and their environment. One of these mechanisms is the control of cell behavior, such as proliferation, differentiation, apoptosis, autophagy, epithelial mesenchymal transition (EMT) as well as the modulation of cell–microenvironment interactions, such as angiogenesis, antioxidants, inflammation and the regulation of immune system of cancer cells.Citation8
Research in mice had shown that vitamin D receptor deficiency was correlated with an increased rate of non-melanoma skin cancer.Citation7 Vitamin D supplementation also reduced the growth of both non-melanoma and melanoma skin cancer cells.Citation7 A human study reported the association between a high vitamin D level with a reduced risk of non-melanoma skin cancer, thinner melanoma, and increased survival of skin cancer patients.Citation7 Although it is known from the WHO data that vitamin D has anti-cancer properties, the evidence for its effect on skin cancer is still limited, especially in humans.Citation7 Exposure to ultraviolet from sunlight is a major environmental risk factor for melanoma and non-melanoma skin cancer.Citation9 Several studies have observed that the formation of vitamin D may protect against the risk of developing non-melanoma skin cancer, however the optimal dose and use of vitamin D in the prevention of skin cancer has not been widely confirmed.Citation10 There is also an evidence from experimental studies showing that vitamin D can protect the skin from ultraviolet radiation that induces DNA damage, thereby preventing the proliferation of skin cancer cells. Vitamin D is also reported to prevent the formation or growth of melanoma cell lines.Citation1,Citation11,Citation12 This paper aims to describe existing research studies that discuss the potential of vitamin D in the management of patients with skin cancer.
Method
Literature Search and Screening Process
The systematic review adhered to the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines. The review process started with a literature search through three scientific databases, including PubMed, Scopus, and ScienceDirect. The literatures were searched based on Patients, Intervention, Control, and Outcome (PICO) criteria, as follows: Patients with any types of skin cancer; calciferol as intervention; placebo or standard regimen as control, and survival rate or response rate as primary outcome.
The PICO criteria of the study () were then translated into several queries and keywords as follows: (Skin cancer, basal cell carcinoma, squamous cell carcinoma, melanoma) and (“Calciferol” or “Vitamin D3”). MeSH-Terms were utilized if available in the mentioned databases. Literatures were then selected against the predetermined inclusion and exclusion criteria. Studies were included with the following criteria: Studies on the effects of calciferol on skin cancer, published within the last 10 years (2012–2022), written or available in English, and being original studies such as RCT or case series. Studies were excluded if they were review articles, letters, or correspondences and if there was no complete data to retrieve.
Table 1 PICO Criteria of the Study
Data Extraction
Data extraction was conducted to summarize the included studies’ characteristics, including the year of publication, trial location, trial design, intervention used on the study, and the cancer population used on the study. The outcomes of included studies were also summarized as shown in .
Table 2 Main Characteristics of the in vitro Studies
Table 3 Main Characteristics of the in vivo Studies
Table 4 Main Characteristics of the Clinical Studies
Results
Literature Search and Papers Selection
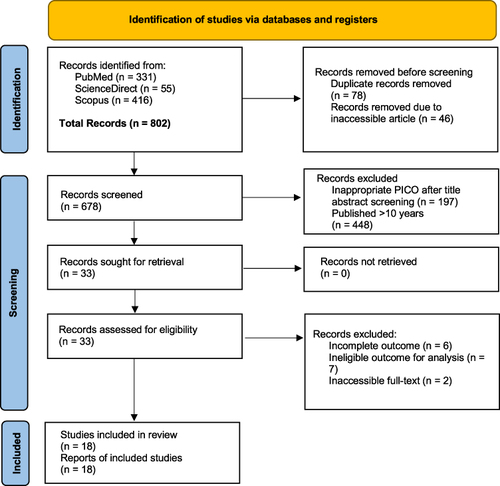
The present literature search was planned, conducted and reported according to the PRISMA guidelines. On July 1, 2022, we searched for relevant literatures in three databases, namely PubMed, ScienceDirect and Scopus with the following keywords: (Skin cancer, basal cell carcinoma, squamous cell carcinoma, melanoma) AND (“Calciferol” OR “Vitamin D3”) to ensure that the literatures obtained were in accordance with the predetermined PICO criteria. We obtained 802 studies, including 331 studies from PubMed, 55 studies from ScienceDirect and 416 studies from Scopus. Prior to the literature screening, there were several studies that were excluded, including 78 studies due to duplication and 46 studies due to the fact that those studies were inaccessible. The remaining 678 studies were screened. A total of 197 studies were then excluded because the titles and abstracts did not match the specified PICO. A total of 448 studies were further excluded because they had been published more than 10 years prior, leaving 33 studies to be assessed for eligibility. From the eligibility assessment, seven studies were excluded because the outcomes were not eligible for analysis, and two studies were excluded due to the full-texts being inaccessible. After the eligibility assessment, the remaining 18 studies were included in the review ().
Figure 1 Article selection for the systematic review on the potential role of calciferol for optimizing cancer therapy.
Main Characteristics of the in vitro Studies
Nine studies published the results in the form of in vitro preclinical studies. One study was from Indonesia, six studies were from Europe, mostly from Poland, and two studies were from the Americas. Five studies investigated melanoma cell lines, two studied malignant-type melanoma cells, and another two investigated hamster cell lines. Only a study by Spath et al described an observation period of around 6 weeks. Seven studies used calcitriol (1,25(OH)2D3) as a vitamin D derivative, one study used 1,25-dihydroxyvitamin D2 (1,25(OH) analogue), and one study used 20(OH)D3. Most studies employing calcitriol as a vitamin D derivative used around 100 nM concentrations. In the studies employing 20(OH)D3, the dose was around 30 g/day. In the studies employing 1,25-dihydroxyvitamin D2 (1,25(OH)2D2), the dose was around 100–1000 nM. However, a study conducted by Piotrowska et al did not provide dose information. Nearly all studies seeded the vitamin D into each well. The study by Sutedja et al in Indonesia, reported significant results by presenting 1,25(OH)2D3 on the growth inhibition of melanoma cell lines at a dose of about 0.244 nM. These results are almost similar to those of Piotrowska et al in Poland, in which the growth inhibition of melanoma cell lines was at the dose range of 0.274 nM to 5.3 nM. Another study conducted by Piotrowska in a different year (2016) showed similar results with inhibition of melanoma cell lines using 1,25(OH)2D2 at a dose of around 0.036 nM. Piotrowska et al also reported significant results on the growth inhibition of melanoma cell lines in their newest study in 2020. These results were relatively different from a study conducted by Pogdorska et al in 2018 in which the calcitriol was found to be able to inhibit the profiling of human melanoma cells at a dose of 10 nM. A study conducted by Wasiewicz et al in 2015 reported a decrease in the growth rate and colony formation in all forms of vitamin D analogues. A study conducted by Spath et al in 2017 also showed that vitamin D3 decreased the proliferation and viability of tumor cells with permanent effects. Meanwhile, a study by Skobowiat et al reported that the administration of 20(OH)D3 had a higher efficacy in the absolute inhibition percentage compared to the inhibition by 1,25(OH)2D3 (56.0% vs 17.0%). Furthermore, a study conducted by Slominski et al in 2012 reported that all compounds caused comparable inhibition in the human melanoma cell lines ().
Main Characteristics of the in vivo Studies
We obtained six in vivo studies, most of which were conducted in areas outside of Asia, two from the USA, 3 from Europe and only one study from Asia, specifically South Korea. Only two studies were conducted research human cells, namely the studies conducted by Skobowiat et al and Spath et al in 2017, although the study recruited mice subjects too. The other five studies were on mice. Two studies did not report their sample size. The study by Kim et al had 35 samples, which was different from the other two studies, namely the study by Pommergard et al in 2013 and 2014, in which each had a fairly larger sample size of approximately 160 and 96 samples. Two studies also did not report the time of observation. The study conducted by Spath et al observed the subjects for 6 weeks, similar to the study conducted by Pommergard et al with 17 weeks observation and the study by Kim et al with 26 weeks observation. Almost all of these studies used vitamin D3 in the form of calcitriol. The study by Skobowiat et al used 20(OH)D3 as vitamin D derivative. Four studies used topical vitamin D, while other two studies used vitamin D seeded into each well. The dose varied between the six studies; the study by Makarova and Kim used a dose of approximately 3 µg, in contrast to the study conducted by Pommergard which used a dose of approximately 0.166 ug/week. The study by Spath et al used doses of approximately 4 and 12 IU, whereas the study by Skobowiat et al used 20(OH)D3 at a dose of 30 g/day. The study by Makarova et al which used high dose (3.8 g) topical vitamin D showed reduction of BCC from 3 ± 1.1 to 0.9 ± 0.5 BCCs/mm skin. The study by Skobowiat et al showed 20(OH)D3 had higher absolute percentage of inhibition compared to inhibition by 1,25(OH)2D3. The studies by Spath and Kim et al also reported similar results of significant tumor cell growth inhibition ().
Main Characteristics of the Clinical Studies
There are five clinical studies, comprising four RCTs and one prospective interventional study. Only one study was conducted in Asia, namely in Turkey, two studies were in the USA and two others were in Europe. Two studies tested the effectiveness of vitamin D in basal cell carcinoma patients. The other two studies also examined patients with skin malignancies. One study conducted by Rosenberg et al tested the effectiveness of vitamin D in actinic keratosis patients. The sample size varied between studies. Three studies had less than 150 subjects, while the other two studies had 496 and 2259 subjects, respectively. Three studies had an average observation time of 30 months, one study only observed for 8 weeks, and one study had a fairly long period of time with a median observation time of approximately 96 months. All studies used vitamin D3 derivatives, with two studies using Cholecalciferol, one study using calcitriol, and the other one using calcipotriol. Two studies used topical administration, while the remaining three studies used oral administration (pill). The study by Johansson et al showed that the serum level of 25-OH-D rose sharply after 4 months of vitamin D supplementation (median of 33 ng/mL) compared to the placebo (median of 19 ng/mL). In their study on basal cell carcinoma patients, Passarelli et al showed a lower incidence rate in the vitamin D group compared to placebo. Meanwhile, a study by Ince et al in 2019 showed that the mean 25-OH vitamin D3 level in the patients with BCC recurrence was 10.1 ng/mL at the second stage. A study by Brinkhuizen et al that tested calcitriol combined with diclofenac in basal cell carcinoma patients showed a significant reduction, whereas single calcitriol therapy did not induce tumor regression sufficiently ().
Discussion
We included a total of 18 studies discussing the potential of vitamin D in skin cancer therapy. The studies were divided into 3 groups based on the study design, namely clinical study and preclinical study which was further divided into in vivo and in vitro studies. In the clinical studies, most subjects had malignant cancer while only one study recruited actinic keratosis subjects, and almost all of them used calcitriol as vitamin D derivatives. Most of these clinical studies concluded that vitamin D3 can reduce the risk of skin cancer, whether used alone or in combination with other components, such as diclofenac or calcium.
The biological mechanism on how vitamin D can be a protective factor for primary melanoma cancer cells is mediated by the 1,25-dihydroxyvitamin D as the vitamin D active form at the intranuclear vitamin D receptor (VDR). VDRs are widely expressed in the human body, where the receptor can trigger several hormones in the body, and are correlated with various diseases. One study found that VDR dysfunction was associated with increased epidermal carcinogenesis.Citation31 Furthermore, this high level of VDR was found in less aggressive cancer cells and correlated with a good prognosis.Citation32
In the in vitro preclinical studies,Citation13–21 most of the samples were melanoma cell lines, either from humans or animals (mice). Most of these in vitro studies concluded that vitamin D derivatives, one of which was calcitriol, could increase the inhibition of melanoma cell proliferation, thereby reducing the growth of these tumor cells. Even the study conducted by Wasiewicz et al in Poland concluded that the administration of all types of vitamin D analogues could reduce the rate of growth and formation of melanoma skin cancer cells,Citation20 although some types of vitamin D analogues, such as 20(OH)D3, could exert greater growth inhibition of cancer cell on several types of cell lines compared to 1,25(OH)2D3, like the results of a study conducted by Slominski et al in 2012.Citation21
This was also in line with the findings of a study conducted by Lim et al,Citation32 in which there was a statistically significant relationship between vitamin D level and tumor thickness as assessed using Breslow thickness (p=0.045). The mean serum vitamin D level was found to be higher in patients with a thin tumor (<1mm) and vitamin D deficiency increased the tumor cell thickness up to 3 mm (p=0.044). Breslow thickness is the most significant indicator for assessing the prognosis of primary melanoma. In addition to using the Breslow thickness indicator, Lim et al also used two traditional indicators for assessing the prognosis of melanoma, namely ulceration and mitosis, which yielded statistically significant results that both indicators were also better in cancer cells with higher vitamin D mean.Citation32 These results indicated that serum vitamin D level was a protective factor for primary melanoma cancer cells. The results of the study by Lim et al were also in line with the study by Wyatt et al which concluded that vitamin D deficiency was associated with increasing tumor cells thickness, leading to poorer prognosis.Citation33 The study also reported that ensuring vitamin D level at 50 nmol/L or more could potentially reduce tumor thickness up to less than 0.75 mm when assessed with the Breslow thickness.Citation33
For in vivo studies,Citation17,Citation18,Citation22–25 the samples were taken from various types of human skin cancer cells and from animals (mice), one study used basal cell carcinoma cell types, two studies used melanoma skin cancer cells and two studies, conducted by the same author, used squamous cell carcinoma cells. The study by Makarova et al showed that the use of high doses of topical vitamin D3 (3.8 ug) had greater effectiveness in reducing the growth of basal cell carcinoma,Citation22 while the study by Skobowiat et al reported that the use of the vitamin D analogue 20(OH)D3 reduced the cancer cell growth significantly greater compared to other vitamin D analogues such as 1,25(OH)2D3.Citation17 The study by Kim et al,Citation23 showed that statistically, the smaller the tumor size, the faster the regression experienced after calcitriol administration at a dose of 3 µg/g.
A study by Bagatini et al reported that 1,25(OH)2D3 increased CD39 enzymatic expression and decreased CD73 enzymatic expression, which if not prevented, it would later develop into melanoma.Citation34 A study conducted by Pawlowska et al concluded that vitamin D had a dose-dependent growth inhibition of melanoma cells.Citation35 This occurs not only in skin cancer cells but also in those of breast cancer, colon cancer, and prostate cancer cells. The study conducted by Dzhandzhugazyan et al also showed that CD39 was a major ectonucleotidase in human melanocytes and melanoma cell lines.Citation36 The results of our study are supported by the study by Nanzer et al in which there was an increase in CD39 expression after treatment with 1,25(OH)2D3.Citation37 Vitamin D has antiproliferative properties in normal cells and cancer cells expressing VDR, where a high dose of vitamin D3 can stop the G0/G1 cell cycle in these cells. The study by Bagatini et al concluded that 1,25(OH)2D3 could increase CD39 and reduce CD73 enzyme expression and activity, which was highly dependent on the dose of vitamin D.Citation34 Such regulation suggests a mechanism to regulate the production of adenosine in the cutaneous melanoma cells treated with the active form of vitamin D.Citation37
Another mechanism on how vitamin D can be a potential therapy in skin cancer cells is related to the concept of autophagy in cancer cells. The concept of autophagy in cancer has been known to be a “double-edged knife”, which can both inhibit or induce the growth of cancer cells and metastasis.Citation38 Apoptosis works by both intrinsic and extrinsic signaling pathway. The intrinsic apoptosis pathway is induced by several intracellular stimuli, such as DNA damage, growth factor depravation, and oxidative stress, which form the apoptosome complex. Meanwhile, autophagy has a pro-metastatic role, despite the original intention of cell regulation. In the early cancer stage, autophagy would help as a suppressor through tumor necrosis restriction and inflammatory cells infiltration; while in the later stage, autophagy promotes extracellular matrix (ECM)-detached metastatic survival in remote site.Citation39
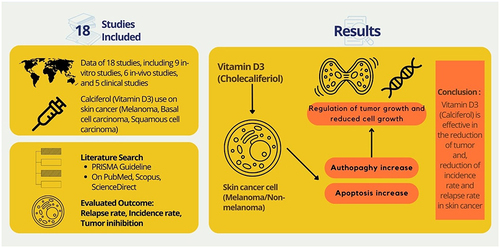
Vitamin D elicits anti-cancer properties by inhibiting tumor promotion through autophagy and apoptosis processes. Inhibition of mTOR signal by vitamin D may cause the induction of autophagy. This vitamin also has the ability to convert the function of autophagy from cytoprotective to cytotoxic which can be a benefit for the treatment of melanoma. Caspase-3 and caspase-9 activation has been said to be critically important in apoptosis. Vitamin D can induce cleavage of both procaspase-3 and procaspase-9 to their active forms. This vitamin can also control the production of reactive oxygen species (ROS) which can inhibit cell proliferation and induce apoptosis significantly.Citation40 Studies by Wu and Sun et al previously discussed the potential mechanism of vitamin D in inducing antitumor activity by modulation of apoptosis and autophagy process. Vitamin D3 might be a major controller of calcium metabolism. The increase of circulating vitamin D enacts VDR, driving to expand the intestinal calcium absorption. In the target cells, calcium is discharged from the sarcoplasmic or endoplasmic reticulum (ER) to actuate calcium-dependent kinases and phosphatases, in this manner controlling various cellular forms, counting autophagy.Citation41,Citation42 ER calcium actuates autophagy when fortified by vitamin D. This process is hindered by mTOR, a negative controller of autophagy, which actuates gigantic collection of autophagosomes in a beclin-1- and ATG7-dependent way as they are not intertwined with lysosomes. Vitamin D also reduces the expression of mTOR protein, hence actuating autophagy by repressing the mTORC1 complex. Additionally, VDR directs autophagy through p19INK4D, a cyclin-dependent kinase inhibitor. Vitamin D actuates the expression of p19INK4D in SCC25 cells, thus protecting cells from autophagy-induced passing.Citation43 Based on the studies included in this review, vitamin D supplementation may be a promising candidate for adjuvant treatment of melanoma through the induction of autophagy and apoptosis. The schematic role of vitamin D in skin cancer is summarized in .
Figure 2 Role of vitamin D in skin cancer.
Conclusion
Vitamin D has been associated with its potential effect as chemopreventive agent on skin cancer therapy. This systematic review with a total of 18 studies has revealed the tremendous potential of vitamin D in the management of skin cancer, including melanoma, squamous cell carcinoma, or basal cell carcinoma. The vitamin D as in various forms, such as 1,25(OH)2D3 or 20(OH)D3 has inhibited the proliferation of cancer cells and thus proving its capability as anticancer therapy. Various mechanism might explain the vitamin D anticancer properties, such as autophagy and apoptosis inducing property through the control of ROS and hinders proapoptotic cytokines, also in controlling the VDR expression and prometastatic gene expression. Vitamin D might be potential to be fully studied with further research on its potential as skin cancer therapy.
Author Contributions
All authors made substantial contributions to the conceptualization and study design, acquisition of data, as well as data analysis and interpretation; and in drafting the article and performing critical revision for important intellectual content. All authors have agreed to submit to the current journal with final approval for publication. All authors will be accountable for all aspects of this manuscript.
Disclosure
The authors declared no conflicts of interest related to this work.
Acknowledgment
The authors would like to thank the Department of Dermatology and Venereology, Faculty of Medicine, Universitas Padjadjaran, Bandung, West Java, Indonesia for the support in the preparation of this manuscript. The authors would also like to extend their gratitude to all authors of the included studies.
Additional information
Funding
References
- Mason RS, Reichrath J. Sunlight vitamin D and skin cancer. Anticancer Agents Med Chem. 2013;13(1):83–97. doi:10.2174/187152013804487272
- Purdue MP, Freeman LE, Anderson WF, et al. Recent trends in incidence of cutaneous melanoma among US Caucasian young adults. J Invest Dermatol. 2008;128:2905–2908. doi:10.1038/jid.2008.159
- Linos E, Swetter SM, Cockburn MG, et al. Increasing burden of melanoma in the United States. J Invest Dermatol. 2009;129:1666–1674. doi:10.1038/jid.2008.423
- Memon A, Bannister P, Rogers I, et al. Changing epidemiology and age-specific incidence of cutaneous malignant melanoma in England: an analysis of the national cancer registration data by age, gender and anatomical site, 1981–2018. Lancet Reg Health Eur. 2021;2:100024. doi:10.1016/j.lanepe.2021.100024
- Apalla Z, Lallas A, Sotiriou E, et al. Epidemiological trends in skin cancer. Dermatol Pract Concept. 2017;7(2):1–6. doi:10.5826/dpc.0702a01
- Giacalone S, Spigariolo CB, Bortoluzzi P, et al. Oral nicotinamide: the role in skin cancer chemoprevention. Dermatol Ther. 2021;34(3):e14892. doi:10.1111/dth.14892
- Chen JG, Fleischer AB, Smith ED, et al. Cost of nonmelanoma skin cancer treatment in the United States. Dermatol Surg. 2001;27:1035–1038. doi:10.1046/j.1524-4725.2001.01004.x
- Jeon SM, Shin EA. Exploring vitamin D metabolism and function in cancer. Exp Mol Med. 2018;50(4):1–14. doi:10.1038/s12276-018-0038-9
- Asgari MM, Tang J, Warton ME, et al. Association of prediagnostic serum vitamin D levels with the development of basal cell carcinoma. J Invest Dermatol. 2010;130:1438–1443. doi:10.1038/jid.2009.402
- Bikle DD. Vitamin D receptor, UVR, and skin cancer: a potential protective mechanism. J Invest Dermatol. 2008;128:2357–2361. doi:10.1038/jid.2008.249
- Binkley N, Ramamurthy R, Krueger D. Low vitamin D status: definition, prevalence, consequences, and correction. Rheum Dis Clin North Am. 2012;38:45–59. doi:10.1016/j.rdc.2012.03.006
- Shariev A, Painter N, Reeve VE, et al. PTEN: a novel target for vitamin D in melanoma. J Steroid Biochem Mol Biol. 2022;218:106059. doi:10.1016/j.jsbmb.2022
- Sutedja EK, Amarassaphira D, Goenawan H, et al. Calcitriol inhibits proliferation and potentially induces apoptosis in B16-F10 cells. Med Sci Monit Basic Res. 2022;28:e935139. doi:10.12659/MSMBR.935139
- Piotrowska A, Wierzbicka J, Kwiatkowska K, Chodyński M, Kutner A, Żmijewski MA. Antiproliferative activity of side-chain truncated vitamin D analogs (PRI-1203 and PRI-1204) against human malignant melanoma cell lines. Eur J Pharmacol. 2020;881:173170. doi:10.1016/j.ejphar.2020.173170
- Piotrowska A, Wierzbicka J, Rybarczyk A, Tuckey RC, Slominski AT, Żmijewski MA. Vitamin D and its low calcemic analogs modulate the anticancer properties of cisplatin and dacarbazine in the human melanoma A375 cell line. Int J Oncol. 2019;54(4):1481–1495. doi:10.3892/ijo.2019.4725
- Podgorska E, Drzal A, Matuszak Z, et al. Calcitriol and calcidiol can sensitize melanoma cells to low⁻LET proton beam irradiation. Int J Mol Sci. 2018;19(8):2236. doi:10.3390/ijms19082236
- Skobowiat C, Oak AS, Kim TK, et al. Noncalcemic 20-hydroxyvitamin D3 inhibits human melanoma growth in in vitro and in vivo models. Oncotarget. 2017;8(6):9823–9834. doi:10.18632/oncotarget.14193
- Spath L, Ulivieri A, Lavra L, et al. Antiproliferative effects of 1α-OH-vitD3 in malignant melanoma: potential therapeutic implications. Sci Rep. 2017;7:40370. doi:10.1038/srep40370
- Piotrowska A, Wierzbicka J, Nadkarni S, Brown G, Kutner A, Żmijewski MA. Antiproliferative activity of double point modified analogs of 1,25-Dihydroxyvitamin D2 against human malignant melanoma cell lines. Int J Mol Sci. 2016;17(1):76. doi:10.3390/ijms17010076
- Wasiewicz T, Szyszka P, Cichorek M, et al. Antitumor effects of vitamin D analogs on hamster and mouse melanoma cell lines in relation to melanin pigmentation. Int J Mol Sci. 2015;16(4):6645–6667. doi:10.3390/ijms16046645
- Slominski AT, Janjetovic Z, Kim TK, et al. Novel vitamin D hydroxyderivatives inhibit melanoma growth and show differential effects on normal melanocytes. Anticancer Res. 2012;32(9):3733–3742. doi:10.1016/j.mce.2012.04.001
- Makarova A, Wang G, Dolorito JA, Kc S, Libove E, Epstein EH. Vitamin D3 produced by skin exposure to UVR inhibits murine basal cell carcinoma carcinogenesis. J Invest Dermatol. 2017;137(12):2613–2619. doi:10.1016/j.jid.2017.05.037
- Kim JS, Jung M, Yoo J, et al. Protective effect of topical vitamin D3 against photocarcinogenesis in a murine model. Ann Dermatol. 2016;28(3):304–313. doi:10.5021/ad.2016.28.3.304
- Pommergaard HC, Burcharth J, Rosenberg J, Raskov H. Topical combination of diclofenac, calcipotriol, and difluoromethylornithine has beneficial effects comparable to 5-fluorouracil for the treatment of non-melanoma skin cancer in mice. J Chemother. 2014;26(2):105–110. doi:10.1179/1973947813Y.0000000117
- Pommergaard HC, Burcharth J, Rosenberg J, Raskov H. Combination chemoprevention with diclofenac, calcipotriol and difluoromethylornithine inhibits development of non-melanoma skin cancer in mice. Anticancer Res. 2013;33(8):3033–3039.
- Johansson H, Spadola G, Tosti G, et al. Vitamin D supplementation and disease-free survival in stage II melanoma: a randomized placebo controlled trial. Nutrients. 2021;13(6):1931. doi:10.3390/nu13061931
- Passarelli MN, Karagas MR, Mott LA, Rees JR, Barry EL, Baron JA. Risk of keratinocyte carcinomas with vitamin D and calcium supplementation: a secondary analysis of a randomized clinical trial. Am J Clin Nutr. 2020;112(6):1532–1539. doi:10.1093/ajcn/nqaa267
- Ince B, Yildirim MEC, Dadaci M. Assessing the effect of vitamin D replacement on basal cell carcinoma occurrence and recurrence rates in patients with vitamin D deficiency. Horm Cancer. 2019;10(4–6):145–149. doi:10.1007/s12672-019-00365-2
- Rosenberg AR, Tabacchi M, Ngo KH, et al. Skin cancer precursor immunotherapy for squamous cell carcinoma prevention. JCI Insight. 2019;4(6):e125476. doi:10.1172/jci.insight.125476
- Brinkhuizen T, Frencken KJ, Nelemans PJ, et al. The effect of topical diclofenac 3% and calcitriol 3 μg/g on superficial basal cell carcinoma (sBCC) and nodular basal cell carcinoma (nBCC): a Phase II, randomized controlled trial. J Am Acad Dermatol. 2016;75(1):126–134. doi:10.1016/j.jaad.2016.01.050
- Caini S, Boniol M, Tosti G, et al. Vitamin D and melanoma and non-melanoma skin cancer risk and prognosis: a comprehensive review and meta-analysis. Eur J Cancer. 2014;50:2649–2658. doi:10.1016/j.ejca.2014.06.024
- Lim A, Shayan R, Varigos G. High serum vitamin D level correlates with better prognostic indicators in primary melanoma: a pilot study. Australas J Dermatol. 2018;59(3):182–187. doi:10.1111/ajd.12648
- Wyatt C, Lucas RM, Hurst C, Kimlin MG. Vitamin D deficiency at melanoma diagnosis is associated with higher Breslow thickness. PLoS One. 2015;10(5). doi:10.1371/journal.pone.0126394
- Bagatini MD, Bertolin K, Bridi A, et al. 1α, 25-Dihydroxyvitamin D3 alters ectonucleotidase expression and activity in human cutaneous melanoma cells. J Cell Biochem. 2019;120(6):9992–10000. doi:10.1002/jcb.28281
- Pawlowska E, Wysokinski D, Blasiak J. Nucleotide excision repair and vitamin D—relevance for skin cancer therapy. Int J Mol Sci. 2016;17(4):1‐21. doi:10.3390/ijms17040372
- Dzhandzhugazyan KN, Kirkin AF, Thor Straten P, Zeuthen J. Ecto‐ATP diphosphohydrolase/CD39 is overexpressed in differentiated human melanomas. FEBS Lett. 1998;430:227‐230. doi:10.1016/S0014-5793(98)00603-6
- Nanzer AM, Chambers ES, Ryanna K, et al. Enhanced production of IL‐17A in patients with severe asthma is inhibited by 1α,25‐dihydroxyvitamin D3 in a glucocorticoid‐independent fashion. J Allergy Clin Immunol. 2013;132(2):297‐304.e3. doi:10.1016/j.jaci.2013.03.037
- Su M, Mei Y, Sinha S. Role of the crosstalk between autophagy and apoptosis in cancer. J Oncol. 2013;2013:102735. doi:10.1155/2013/102735
- Su Z, Yang Z, Xu Y, Chen Y, Yu Q. Apoptosis, autophagy, necroptosis, and cancer metastasis. Mol Cancer. 2015;14(1):48. doi:10.1186/s12943-015-0321-5
- Gunadi JW, Welliangan AS, Soetadji RS, Jasaputra DK, Lesmana R. The role of autophagy modulated by exercise in cancer cachexia. Life. 2021;11:781. doi:10.3390/life11080781
- Wu S, Sun J. Vitamin D, vitamin D receptor, and macroautophagy in inflammation and infection. Discov Med. 2011;11(59):325–335.
- Abdel-Mohsen MA, El-Braky AA, Ghazal AAE, Shamseya MM. Autophagy, apoptosis, vitamin D, and vitamin D receptor in hepatocellular carcinoma associated with hepatitis C virus. Medicine. 2018;97(12):e0172. doi:10.1097/MD.0000000000010172
- Tavera-Mendoza L, Wang TT, Lallemant B, et al. Convergence of vitamin D and retinoic acid signaling at a common hormone response element. EMBO Rep. 2006;7(2):180–185. doi:10.1038/sj.embor.7400594