
Abstract
While there have been advances in treatment options for those with advanced non-small-cell lung cancer, unmet medical needs remain, partly due to the heterogeneity of treatment effect observed among patients. The goals of this literature review were to provide updated information to complement past reviews and to identify a comprehensive set of nongenetic prognostic and predictive baseline factors that may account for heterogeneity of outcomes in advanced non-small-cell lung cancer. A review of the literature between 2000 and 2010 was performed using PubMed, Embase, and Cochrane Library. All relevant studies that met the inclusion criteria were selected and data elements were abstracted. A classification system was developed to evaluate the level of evidence for each study. A total of 54 studies were selected for inclusion. Patient-related factors (eg, performance status, sex, and age) were the most extensively researched nongenetic prognostic factors, followed by disease stage and histology. Moderately researched prognostic factors were weight-related variables and number or site of metastases, and the least studied were comorbidities, previous therapy, smoking status, hemoglobin level, and health-related quality of life/symptom severity. The prognostic factors with the most consistently demonstrated associations with outcomes were performance status, number or site of metastases, previous therapy, smoking status, and health-related quality of life. Of the small number of studies that assessed predictive factors, those that were found to be significantly predictive of outcomes were performance status, age, disease stage, previous therapy, race, smoking status, sex, and histology. These results provide a comprehensive overview of nongenetic prognostic and predictive factors assessed in advanced non-small-cell lung cancer over the last decade. This information can be used to inform the design of future clinical trials by suggesting additional subgroups based on nongenetic factors that may be analyzed to further investigate potential prognostic and predictive factors.
Introduction
Lung cancer has the highest mortality rate of any cancer type worldwide.Citation1 While there have been advances in therapeutic options for those with advanced (stage III/IV) non-small-cell lung cancer (NSCLC), particularly for subgroups of patients who qualify for treatment with newer targeted agents, a significant unmet medical need remains. There have been small gains in NSCLC survival rates; however, the significance of these gains and the benefits to patients with a variety of characteristics are unclear.Citation2,Citation3
Previous research identified several elements, including age, sex, comorbidities, and health care resource utilization, which are associated with differential treatment response and/or outcomes in NSCLC.Citation4 Prognostic factors are those variables that are associated with a clinical outcome (prognosis) that is independent of a given therapy.Citation5,Citation6 Prognostic factor information is important for the stratification of patients in clinical trial protocols and for the individualization of a patient care plan.Citation4 By contrast, predictive factors provide a probability that a patient will respond more favorably to a particular therapy. Predictive factors are important to consider when selecting patients likely to respond to a particular therapy and when evaluating multiple treatment options that are available for a particular patient.Citation4,Citation6
Heterogeneity of treatment effect (HTE) describes the differences in treatment outcomes observed within and outside clinical trials.Citation7,Citation8 Some patients will benefit more or less than the average patients reported in the clinical trial literature; understanding HTE is necessary to individualize treatment and optimize patient outcomes.Citation9 Prognostic and predictive factors influence HTE;Citation5,Citation6 therefore, identifying these factors and accounting for HTE in the development of new therapies will provide valuable information to evidence-based decision makers, while potentially improving clinical outcomes and health-related quality of life (HRQoL) for patients.
While much of the current research in NSCLC has focused on the identification of genetic prognostic and predictive factors, there is also value in understanding nongenetic factors or patient-related factors that are associated with HTE but are not related to known genetic markers. In the recent past, nongenetic factors have identified subgroups that have later been established as clinical correlates of genetic markers. For example, early studies found that subgroups of patients with NSCLC who were female, Asian, and nonsmokers or former light smokers and had tumors with adenocarcinoma histology were more likely to respond to epidermal growth factor receptor (EGFR) inhibitors than were patients without these characteristics.Citation10 It was later determined that patient subgroups whose tumors had activating EGFR mutations were the most responsive to EGFR inhibitors and that the clinical factors identified to predict response were associated with the target gene mutations in the NSCLC population.Citation10 This early characterization of patients helped to predict which patients might benefit more from EGFR inhibitors before the underlying genetic marker was identified.
In general, prognostic factors for all types of advanced-stage cancer include performance status (PS), clinical signs and symptoms (eg, related to anorexia, weight loss, dyspnea, and dysphagia), and biological factors (eg, leukocytosis, lymphocytopenia, and C-reactive protein).Citation11 A 2002 literature review identified 169 tumor- or patient-related prognostic factors, and identified those prognostic factors for patients with advanced NSCLC that were essential for decision making (ie, stage of disease, hypercalcemia, superior vena cava obstruction, weight loss, and PS).Citation12 New and emerging factors at the time of the 2002 review included items such as HRQoL, marital status, depressed mood, and various molecular biological markers.Citation12 Brundage et al noted that individual studies in the review were repeatedly underpowered and narrowly focused and had highly variable results.Citation12
In addition, a 2003 review identified prognostic factors that should be used when selecting stage IV NSCLC patients for systemic chemotherapy.Citation13 Prior chemotherapy was consistently identified as an important prognostic factor, and PS at the time of diagnosis was deemed a powerful indicator of survival.Citation13 Disease stage is one of the most well-established prognostic factors in NSCLC.Citation12,Citation13 Pretreatment weight loss was identified as a negative factor for survival, whereas high HRQoL scores, high levels of albumin, low levels of alkaline phosphatase, and expression of neuroendocrine markers were associated with positive outcomes.Citation13 Histologic subtype was reported to be an unreliable prognostic factor, and age was deemed a possible indicator as some studies suggest that elderly patients with advanced NSCLC have poorer outcomes.Citation13
The goals of this literature review were to provide updated information to complement past reviews and to focus on the identification of a comprehensive set of nongenetic prognostic and predictive baseline tumor- and patient-related factors that identify subpopulations of advanced-stage NSCLC patients with differential treatment response and outcomes.
Materials and methods
Search strategy
Three key databases were used for this search: PubMed, Embase, and Cochrane Library. The database searches were limited to studies published in English between January 2000 and November 2010. Published materials from the 2010 annual meeting of the American Society of Clinical Oncology were also reviewed. Conceptually, the inclusion criteria of the search strategy focused on stage III/IV NSCLC, Phase III or IV clinical trials, observational studies, meta-analyses, and systematic reviews. The search strategy developed for PubMed and adapted for use in the other databases is presented in .
Table 1 PubMed search strategyTable Footnotea for heterogeneity in advanced non-small-cell lung cancer
Definitions
In this review, prognostic factors were defined as tumor- or patient-related factors that provided risk information about achieving a specific clinical outcome (progression-free survival [PFS], overall survival [OS], time to progression [TTP], or response rate [RR]), independent of treatment.Citation5 Predictive factors were defined as factors that identified patients who had a different probability of achieving a specific outcome (ie, PFS, OS, TTP, or RR) only when treated with a specific therapy.Citation5 The direction of the association between factors and outcomes was also examined.
Study classification system
A classification system specific to studies that assessed prognostic or predictive factors was developed for this review, in order to differentiate among studies based on the rigor of the methods used to assess prognostic or predictive ability and to analyze the strength of evidence for the factors explored in these studies. Based on the classification system, all studies were assigned a qualitative evidence rating by one author that was verified by a second author. The classification system reflects that higher quality prognostic and predictive studies were those with greater internal validity (eg, data analyzed were from randomized controlled trials versus observational studies), with larger versus smaller sample sizes, and with multivariate versus univariate analyses. The clinical trial sample sizes in the classification categories were selected arbitrarily, based on the sizes of the trials in the identified studies. According to these criteria, studies were rated on a scale of one to five. The highest rating possible for a prognostic study was PROG-1 and the lowest rating was PROG-5. Meta-analyses, systematic reviews, and multiple clinical trials were assigned level one, the highest ranking. Single larger clinical trial studies (n≥200 for a two-arm study; n≥300 for a three-arm study) were assigned level two. Single smaller clinical trial studies (n<200 for a two-arm study; n<300 for a three-arm study) were assigned level three. Observational studies were assigned level four. Studies with no regression model or only univariate models were assigned a level five ranking, the lowest quality ranking.
Similarly, the highest possible rating for a predictive study was PRED-1 and the lowest possible rating was PRED-5. Factor validation studies prospectively designed to assess a predictive factor were assigned level one. The presence of a formal statistical interaction test, regardless of the size or number of trials, was assigned level two. Analyses of clinical trial(s) with a multivariate model without a formal test of interaction were assigned level three. Analyses of observational studies with or without a formal test of interaction were assigned level four. Predictive studies with no regression model or only univariate models were assigned a level five ranking, the lowest quality ranking. If a study presented data for both prognostic and predictive factors, the study was rated separately on each scale. Only the highest ranked studies were retained for this review; therefore, those studies assigned level PROG-5 and PRED-5 ratings were excluded.
Results
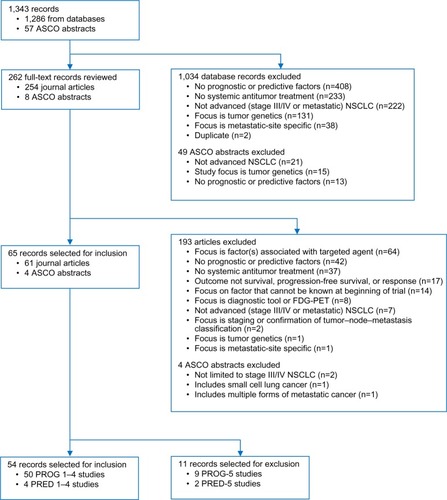
All evaluated studies were retrospective analyses of randomized controlled trials or observational study data. The literature review identified 1,856 records. After duplicates were removed, there were 1,286 unique journal articles (PubMed 1,030, Embase 243, and Cochrane 13). The American Society of Clinical Oncology search identified 57 records (36 prognostic and 21 predictive factors). Of the 1,343 records that were initially identified and screened, 65 studies focused on prognostic factors or predictive factors and were reviewed and abstracted. Ultimately, only the highest ranked studies were retained; therefore, eleven studies (nine prognostic and two predictive) with the lowest ranking in the study classification system (PROG-5 and PRED-5) were excluded (). A total of 54 studies were selected for final inclusion in the literature review; 50 studies focused on prognostic factors (six of which included both prognostic and predictive factors) and four studies focused exclusively on predictive factors ().
Table 2 Summary of study classification system
Figure 1 Flowchart of advanced non-small-cell lung cancer patient heterogeneity reference review.
Note: PROG-1–5 and PRED-1–5 represent a rating system for prognostic and predictive studies, respectively, where one is high and five is low.
Abbreviations: ASCO, American Society of Clinical Oncology; FDG-PET, fluorodeoxyglucose positron emission tomography; NSCLC, non-small-cell lung cancer.
Prognostic factors
Prognostic factor studies are summarized in , and the directionality of evidence for the prognostic factors is presented in .
Table 3 Summary of quality classification PROG-1 to PROG-4 studies of prognostic factors in advanced non-small-cell lung cancer
Figure 2 Directional evidence of prognostic factors in advanced non-small-cell lung cancer.
Notes: All associations are statistically significant, as specified in each study. aStudies that assessed response in second-line or later treatment populations.
Abbreviations: BMI, body mass index; HRQoL, health-related quality of life.
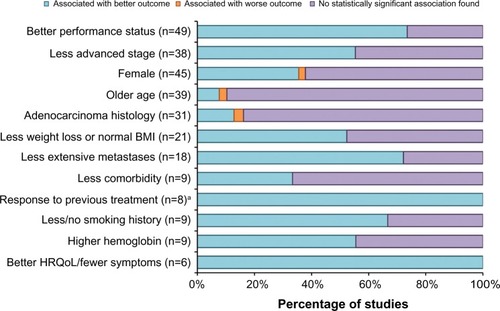
PS was one of the most consistently explored factors. Most studies categorized PS with the Eastern Cooperative Oncology Group PS scale as PS 0/1 versus PS 2 (or PS ≥2). The other scale used was the Karnofsky Performance Status (KPS) scale, most often categorized as KPS <70 versus KPS ≥80. There were 49 studies that evaluated PS as a prognostic factor, with 73% (n=36) reporting a significant association. Eleven (85%) of the 13 PROG-1 studies reported a significant association with outcomes, including tumor response or survival, as did 89% of the nine PROG-2 studies, 82% of the eleven PROG-3 studies, and 50% of the 16 PROG-4 studies. In the 36 studies that reported a significant association between outcomes (tumor response or survival) and PS, a better PS (lower Eastern Cooperative Oncology Group PS score or higher KPS score) was associated with a better outcome.Citation14–Citation49
The majority of the studies that assessed disease stage compared stage IIIB NSCLC with stage IV. There were 38 studies that evaluated disease stage as a prognostic factor, with 55% (n=21) reporting a significant association between disease stage and response or survival. Seven (70%) of the ten PROG-1 studies reported that disease stage is a significant prognostic factor, as did 33% of the nine PROG-2 studies, 29% of the seven PROG-3 studies, and 75% of the 12 PROG-4 studies. In the 21 studies that reported a significant association between disease stage and response or survival, less advanced disease stage was associated with a better outcome in all studies.Citation14,Citation15,Citation17,Citation20–Citation22,Citation24,Citation26,Citation31,Citation32,Citation35,Citation37,Citation42–Citation44,Citation47,Citation48,Citation50–Citation53
Sex was a frequently evaluated factor – there were 45 studies that assessed sex as a prognostic factor, with a total of 17 (38%) studies reporting a significant finding. Six (46%) of the 13 PROG-1 studies reported a significant association between sex and outcomes, as did 56% of the nine PROG-2 studies, 38% of the eight PROG-3 studies, and 20% of the 15 PROG-4 studies. In all cases, female sex was associated with better outcomes.Citation15,Citation16,Citation19,Citation23–Citation25,Citation28,Citation31,Citation32,Citation35,Citation36,Citation38,Citation42,Citation47,Citation51,Citation54,Citation55
Age was most commonly dichotomized using the cutoff of 65 or 70 years. Thirty-nine of the studies examined the relationship between age and survival, with four (10%) reporting a significant finding. Among the four studiesCitation37,Citation40,Citation42,Citation43 in which age was a significant prognostic factor, the evidence was inconsistent – older age appeared to be associated with better outcomes in three of the reviewed studiesCitation37,Citation40,Citation42 and associated with a worse outcome in one reviewed study.Citation43
Histology was most frequently dichotomized as adenocarcinoma versus other (nonadenocarcinoma, squamous) or nonsquamous versus squamous. Histology was evaluated in 31 studies and was found to be a significant prognostic factor in five studies (16%). Of these five studiesCitation15,Citation28,Citation46,Citation52,Citation56 that reported a significant association between histology and survival, adenocarcinoma histology appeared to be associated with better outcomes for four of these studies.Citation15,Citation46,Citation52,Citation56
Weight loss was often categorized in the literature by the percentage of body weight lost, although the time frames over which the weight loss occurred were often not well defined. Body mass index (BMI) was also used to classify patients (underweight: BMI <18.5; normal: 18.5≤ BMI <25; overweight: 25≤ BMI <30; obese: BMI ≥30) and to compare different BMI categories. Twenty-one studies assessed weight loss and/or BMI, and eleven studies (52%) reported a significant association with survival (four PROG-1 studies, one PROG-2 study, two PROG-3 studies, and four PROG-4 studies). In these studies reporting a significant association, less weight loss or a normal BMI at baseline was associated with better outcomes in all the studies.Citation19,Citation21,Citation23,Citation31,Citation37,Citation43,Citation48,Citation51,Citation57–Citation59
Various metastatic features were examined as potential prognostic factors. The presence or extent of metastases was evaluated in 18 studies, and a significant association was identified in 13 (72%) of the total assessed studies.Citation18–Citation20,Citation23,Citation26–Citation28,Citation30,Citation42,Citation43,Citation45,Citation51,Citation60 Seven of the 13 studies assessed the number of metastatic sites,Citation18–Citation20,Citation27,Citation28,Citation42,Citation45 and six of these studies found a significant association between a larger number of sites and worse OS or TTP.Citation18,Citation19,Citation27,Citation28,Citation42,Citation45 In addition, six studies assessed the presence of liver metastases, five of which found a significant association between the presence of liver metastases and worse OS.Citation18–Citation20,Citation30,Citation45,Citation51 Overall, when a significant association was identified, less extensive metastases were associated with better outcomes in all situations.
In the reviewed studies, comorbidity was defined and categorized by dichotomous groupings of the Charlson Comorbidity Index score, number of comorbid conditions, presence or absence of a specific comorbidity, or dichotomous groupings of the Simplified Comorbidity Score. Comorbidity was evaluated in nine studies, and three of these studies (33%) reported a significant association. Of the three studies that reported a significant association, two studies examined the number of comorbid conditions (less than two versus two or more)Citation60,Citation61 and one study examined comorbidity as Simplified Comorbidity Score (nine or less versus more than nine) and Charlson Comorbidity Index score (less than three versus three or more).Citation53 In the three studies that reported comorbidity as a statistically significant prognostic determinant of response, less comorbidity was associated with better outcomes.Citation53,Citation60,Citation61
Aspects of previous therapy that were examined as potential prognostic factors included type of therapy, response to previous therapy, and interval between first-line and second-line or later therapy. Previous therapy was assessed as a possible prognostic factor in nine studies. Among these studies, eight studies (89%) that assessed the prognostic significance of previous therapy in patients receiving second-line or later therapy reported statistically significant associations between response to previous treatment and outcomes.Citation15,Citation17,Citation32,Citation43,Citation47,Citation52,Citation58,Citation62 One study assessed previous radiotherapy in a first-line advanced NSCLC treatment population and reported that no previous radiotherapy was significantly associated with better survival and TTP.Citation38 In the majority of studies assessing response to previous therapy, responding to prior treatment was associated with better outcomes.
Smoking status was evaluated as a prognostic factor for survival or response in nine of the evaluated studies, with six studies (67%) reporting a significant association. Both PROG-2 studies reported a significant association between smoking status and outcomes, as did four of the six PROG-4 studies. Of the studies that found a significant association, less or no smoking was associated with favorable outcomes in all cases.Citation28,Citation30,Citation43,Citation44,Citation52,Citation56
Blood hemoglobin concentration was assessed as a potential prognostic factor in nine studies, and five of these studies (56%) reported a significant association. All five of these studies found that a higher hemoglobin level was associated with better outcomes.Citation21,Citation46,Citation53,Citation55,Citation58 Laboratory values other than hemoglobin were considered as potential prognostic factors in several studies. Explored laboratory values included albumin, alkaline phosphatase, C-reactive protein, lactate dehydrogenase, interleukin-2, and interleukin-10, and several studies assessed multiple laboratory values. Serum albumin was significantly associated with OS (four studies) or PFS (one study), and lower albumin levels were associated with worse outcomes.Citation20,Citation37,Citation45,Citation46,Citation60 Lactate dehydrogenase was significantly associated with survival in three studies, with elevated lactate dehydrogenase associated with shorter survival.Citation30,Citation50,Citation60 Serum neuron-specific enolase was significantly associated with survival in three studies.Citation20,Citation37,Citation53 In two studies, the direction of the association was reported, and in these studies, higher neuron-specific enolase levels were associated with worse survival.Citation20,Citation53
Pretreatment HRQoL or patient-reported symptoms were evaluated in six studies and were found to be significant in all six (100%) of the studies. In these studies, a variety of assessment tools were used and significant findings were reported for associations between various HRQoL or symptom severity measures and outcomes, including better HRQoL, better physical wellbeing and functioning, and less pain, dysphagia, severe symptoms, and coughing. Of the six studies that reported HRQoL to be a significant prognostic factor, better HRQoL and less symptom burden were associated with better outcomes.Citation25–Citation27,Citation49,Citation53,Citation57
Predictive factors
The distribution of predictive factor studies presented in and summarizes study-specific results for those with significant associations of achieving a specific outcome (ie, PFS, OS, TTP, or RR) when treated with a specific therapy. Overall, ten studies reported information for predictive factors, six studies included both prognostic and predictive factors,Citation28,Citation30,Citation31,Citation41,Citation52,Citation62 and four studies focused exclusively on predictive factors.Citation63–Citation66 Of the ten studies that assessed predictive factors, half found no significant results. All four of the exclusively predictive studies were classified as level two (PRED-2),Citation63–Citation66 and some of these studies reported on multiple predictive factors, particularly one of the PRED-2 studies.Citation66 Overall, two studies reported PS to be a significant predictive factor (borderline significant in Soria et al’s study),Citation65,Citation66 two reported age to be significant,Citation41,Citation66 one reported disease stage to be significant,Citation66 and one reported previous therapy to be significant.Citation62 Of the two studies that reported race, one found race to be significant.Citation66 One of two studies reported smoking status to be significant,Citation66 and one of two studies reported sex to be significant.Citation41 Four studies examined histology and two found histology to be significant.Citation63,Citation66
Table 4 Summary of quality classification for studies of predictive factors in advanced non-small-cell lung cancer
Table 5 Summary of statistically significant predictive factor findings in advanced non-small-cell lung cancer
Discussion
This comprehensive review of the published literature was conducted to assess nongenetic prognostic and predictive factors related to heterogeneity of response and outcomes in patients with advanced NSCLC in order to identify subpopulations that experience differential outcomes. This review provides an overview of prognostic and predictive factors assessed over the last decade and complements past literature reviews by providing updated information from studies published since 2000.Citation12,Citation67 Both patient- and tumor-related factors that were significantly associated with response or survival were identified.
Patient-related factors (eg, PS, sex, and age) were the most extensively researched prognostic factors, followed by disease stage and histology (both tumor-related variables). Moderately researched prognostic factors were weight-related variables and number or site of metastases, and the least studied nongenetic prognostic factors were comorbidities, previous therapy, smoking status, hemoglobin level, and HRQoL/symptom severity. The prognostic factors with the most consistently demonstrated associations with outcomes were PS, number or site of metastases, previous therapy, smoking status, and HRQoL.
This review demonstrated that better PS (lower Eastern Cooperative Oncology Group PS score or higher KPS score) was prognostic for better outcomes (tumor response or survival) in 73% of studies evaluating PS, adding to the extensive evidence that supports the prognostic importance of PS across multiple studies, patient populations, and treatments. Clinicians have long regarded PS as a reliable measure of functional independence, and it is a strong prognostic determinant of survival and of the incidence and severity of adverse events, with the majority of Phase III trials stratifying patients according to PS (PS 0/1 versus PS 2).Citation68 While this finding is consistent with previous literature,Citation12,Citation67,Citation69 it remains remarkable that PS is such a strong factor given the subjective nature of PS measures, the use of different scales, and considerable intraobserver and interobserver variation. Further research might focus on whether the prognostic ability of PS can be improved by using a composite measure with the addition of other nongenetic prognostic factors and by developing more specific standardized criteria.
Of the studies evaluating the following factors, the majority of these studies found that a larger number of metastatic sites and presence of liver metastases were associated with worse survival or TTP, response to previous therapy was prognostic for better outcomes, less or no smoking was prognostic for better survival or response, and better HRQoL was prognostic for better outcomes. The absolute number of studies supporting metastatic features, previous therapy, smoking status, and HRQoL as prognostic factors was limited. While these prognostic factors consistently demonstrated associations with outcomes, the number of studies with statistically significant associations was low compared to the number of studies evaluating other prognostic factors found in this review. Prognostic values cannot be established by a limited number of studies.
Disease stage is a well-established prognostic factor in NSCLC;Citation12 however, only 55% of the studies in this review assessing disease stage found that less advanced disease was prognostic for patient outcomes (tumor response or survival). Among the studies with the most robust designs, 70% reported a statistically significant association of disease stage with outcomes. The studies in this review were limited to advanced NSCLC, that is patients’ tumors of stage IIIB and stage IV comprise a relatively narrow range within the continuum of tumor staging.Citation70 Nonetheless, patients with advanced NSCLC, which usually includes stages IIIB and IV,Citation71 generally constitute the population frequently studied in clinical trials.
In a review by Hirsch et al, significant associations between histology and outcomes were observed, and adenocarcinoma was associated with superior survival in patients with advanced NSCLC.Citation67 The review by Hirsch et al identified 32 studies that found a statistically significant association between histology and one or more efficacy endpoints.Citation67 However, only five of 31 (16%) prognostic studies identified in the current review found an association between histology and outcomes. In four of the five studies, adenocarcinoma was prognostic for better survival. Two studies included in the current review overlap with studies included in Hirsch et al’s review which included studies conducted between 1982 and 2007.
The current review identified only ten studies that evaluated predictive factors, and among these only half reported statistically significant results, with most significant factors occurring in only one or two studies each. Four of the ten studies examined histology, and two of these found histology to be predictive of achieving a specific outcome (ie, PFS, OS, TTP, or RR) when treated with a specific therapy, which supports recent literature findings.Citation67,Citation72,Citation73 In the 2007 meta-analysis of nine trials, cisplatin-based chemotherapy prolonged survival versus carboplatin for patients with squamous histology.Citation63 A 2010 retrospective analysis of a Phase III randomized controlled trial of 1,725 stage IIIB and IV patients who received first-line therapy (cisplatin plus pemetrexed versus cisplatin plus gemcitabine) confirmed that histology was the only predictive factor of superior survival for cisplatin plus pemetrexed versus cisplatin plus gemcitabine in patients with nonsquamous NSCLC and shorter survival for cisplatin plus pemetrexed in patients with squamous cell carcinoma.Citation66 Predictive studies for newer targeted therapies, such as EGFR inhibitors and anaplastic lymphoma kinase inhibitors, have focused on selected molecular subgroups of NSCLC and have shown predictive biomarkers for these therapies; however, these studies were not included in this review because the mutations/biomarkers are genetic factors.
One limitation of this review is the heterogeneous nature of the identified studies. The reviewed studies varied in study quality; study populations; statistical analyses; factors included in models and analyses; methods used to define, measure, and classify the factors; laboratory techniques; and treatments received. The classification system reflects that higher ranked prognostic and predictive studies were those with greater internal validity (eg, data analyzed were from randomized controlled trials versus observational studies), with larger versus smaller sample sizes, and with multivariate versus univariate analyses. The reviewed studies were not prospectively designed; they may not be powered to assess statistical significance. Thus, the individual findings of this review should be interpreted in the context of the many factors evaluated. Discrepancies found in the results could reduce the ability to identify the true influence of prognostic and predictive factors. Publication bias may be present because those studies exploring prognostic and predictive factors that did not find significant associations may be less likely to be published. An additional limitation of this review is the time frame captured in this study. Studies published between 2000 and 2010 were reviewed. This could be an important limitation if more recently published studies have found results that are markedly different from those evaluated here.
Conclusion
This review provides an overview of nongenetic prognostic and predictive factors assessed over the last decade and complements past literature reviews by providing updated information from studies published since 2000. This literature review identified several factors, including PS, number or site of metastases, previous therapy, smoking status, and HRQoL, that may account for HTE and outcomes in advanced NSCLC. The findings in this review that are related to the prognostic ability of these factors generally support current clinical decision making. However, treatment implications of the predictive factors were limited because, for the most part, the interaction of a specific treatment with patient factors was examined in a single study, and only half of the reviewed predictive studies failed to demonstrate significant findings. This comprehensive review of the nongenetic patient factors that have been evaluated in advanced NSCLC can be used to complement information on genetic factors to inform the design of future clinical trials by suggesting additional subgroups of patients with differential treatment response and outcomes.
Acknowledgments
This study was funded by Eli Lilly and Company. The authors would like to thank Teri Tucker of inVentiv Health Clinical for her editorial contributions and Rebecca McCracken of inVentiv Health Clinical for assistance in preparing the manuscript.
Disclosure
GCC, AML, KBW, and WJJ are employees and stockholders of Eli Lilly and Company. AMB and JAK report no conflicts of interest in this work.
References
- American Cancer SocietyCancer Facts and Figures 2012Atlanta, GAAmerican Cancer Society2012 Available from: http://www.cancer.org/acs/groups/content/@epidemiologysurveilance/documents/document/acspc-031941.pdfAccessed July 29, 2012
- FuJBKauTYSeversonRKKalemkerianGPLung cancer in women: analysis of the national Surveillance, Epidemiology, and End Results databaseChest2005127376877715764756
- MorgenszternDWaqarSSubramanianJGaoFGovindanRImproving survival for stage IV non-small cell lung cancer: a Surveillance, Epidemiology, and End Results survey from 1990 to 2005J Thorac Oncol20094121524152919752759
- AlatorreCICarterGCChenCA comprehensive review of predictive and prognostic composite factors implicated in the heterogeneity of treatment response and outcome across disease areasInt J Clin Pract201165883184721718398
- SargentDJConleyBAAllegraCColletteLClinical trial designs for predictive marker validation in cancer treatment trialsJ Clin Oncol20052392020202715774793
- YipDHarperPGPredictive and prognostic factors in small cell lung cancer: current statusLung Cancer200028317318510812187
- Fernandez y GarciaENguyenHDuanNGablerNBKravitzRLAssessing heterogeneity of treatment effects: are authors misinterpreting their results?Health Serv Res2010451283301
- KentDMRothwellPMIoannidisJPAltmanDGHaywardRAAssessing and reporting heterogeneity in treatment effects in clinical trials: a proposalTrials2010118520704705
- GablerNBDuanNLiaoDElmoreJGGaniatsTGKravitzRLDealing with heterogeneity of treatment effects: is the literature up to the challenge?Trials2009104319545379
- MokTSWuYLThongprasertSGefitinib or carboplatin– paclitaxel in pulmonary adenocarcinomaN Engl J Med20093611094795719692680
- MaltoniMCaraceniABrunelliCPrognostic factors in advanced cancer patients: evidence-based clinical recommendations – a study by the Steering Committee of the European Association for Palliative CareJ Clin Oncol200523256240624816135490
- BrundageMDDaviesDMackillopWJPrognostic factors in non-small cell lung cancer: a decade of progressChest200212231037105712226051
- SocinskiMAMorrisDEMastersGALilenbaumRChemotherapeutic management of stage IV non-small cell lung cancerChest2003123Suppl 1226S243S12527582
- ComellaPGambardellaAFrasciGAvalloneACostanzoRComparison of the safety and efficacy of paclitaxel plus gemcitabine combination in young and elderly patients with locally advanced or metastatic non-small cell lung cancer. A retrospective analysis of the Southern Italy Cooperative Oncology Group trialsCrit Rev Oncol Hematol200865216417117702595
- Di MaioMLamaNMorabitoAClinical assessment of patients with advanced non-small-cell lung cancer eligible for second-line chemotherapy: a prognostic score from individual data of nine randomized trialsEur J Cancer201046473574320045311
- Di MaioMMorabitoABarberaSEducation level as prognostic factor of patients (pts) with advanced non-small cell lung cancer (NSCLC) enrolled in clinical trials [abstract]J Clin Oncol201028Suppl 15 abstract 6124
- HatzidakiDAgelakiSMavroudisDVlachonikolisIAlegakisAGeorgouliasVA retrospective analysis of second-line chemotherapy or best supportive care in patients with advanced-stage non-small-cell lung cancerClin Lung Cancer200681495516870046
- HoangTXuRSchillerJHBonomiPJohnsonDHClinical model to predict survival in chemonaive patients with advanced non-small-cell lung cancer treated with third-generation chemotherapy regimens based on Eastern Cooperative Oncology Group dataJ Clin Oncol200523117518315625371
- JeremicBMilicicBDagovicAAleksandrovicJNikolicNPretreatment clinical prognostic factors in patients with stage IV non-small cell lung cancer (NSCLC) treated with chemotherapyJ Cancer Res Clin Oncol2003129211412212669236
- MaedaTUeokaHTabataMPrognostic factors in advanced non-small cell lung cancer: elevated serum levels of neuron specific enolase indicate poor prognosisJpn J Clin Oncol2000301253454111210162
- MandrekarSJSchildSEHillmanSLA prognostic model for advanced stage nonsmall cell lung cancer. Pooled analysis of North Central Cancer Treatment Group trialsCancer2006107478179216847887
- PallisAGPolyzosABoukovinasIPooled analysis of elderly patients with non-small cell lung cancer treated with front line docetaxel/gemcitabine regimen: the Hellenic Oncology Research Group experienceJ Thorac Oncol20083550551018449003
- WakeleeHABernardoPJohnsonDHSchillerJHChanges in the natural history of nonsmall cell lung cancer (NSCLC) – comparison of outcomes and characteristics in patients with advanced NSCLC entered in Eastern Cooperative Oncology Group trials before and after 1990Cancer2006106102208221716604529
- Wheatley-PricePBlackhallFLeeSMThe influence of sex and histology on outcomes in non-small-cell lung cancer: a pooled analysis of five randomized trialsAnn Oncol201021102023202820332134
- EfficaceFBottomleyASmitEFIs a patient’s self-reported health-related quality of life a prognostic factor for survival in non-small-cell lung cancer patients? A multivariate analysis of prognostic factors of EORTC study 08975Ann Oncol200617111698170416968876
- EtonDTFaircloughDLCellaDYountSEBonomiPJohnsonDHEarly change in patient-reported health during lung cancer chemotherapy predicts clinical outcomes beyond those predicted by baseline report: results from Eastern Cooperative Oncology Group Study 5592J Clin Oncol20032181536154312697878
- MaionePPerroneFGalloCPretreatment quality of life and functional status assessment significantly predict survival of elderly patients with advanced non-small-cell lung cancer receiving chemotherapy: a prognostic analysis of the multicenter Italian lung cancer in the elderly studyJ Clin Oncol200523286865687216192578
- ScagliottiGVDe MarinisFRinaldiMThe role of histology with common first-line regimens for advanced non-small cell lung cancer: a brief report of the retrospective analysis of a three-arm randomized trialJ Thorac Oncol20094121568157120009911
- SederholmCHillerdalGLambergKPhase III trial of gemcitabine plus carboplatin versus single-agent gemcitabine in the treatment of locally advanced or metastatic non-small-cell lung cancer: the Swedish Lung Cancer Study GroupJ Clin Oncol200523338380838816293868
- TeramukaiSKitanoTKishidaYPretreatment neutrophil count as an independent prognostic factor in advanced non-small-cell lung cancer: an analysis of Japan Multinational Trial Organization LC00-03Eur J Cancer200945111950195819231158
- WakeleeHAWangWSchillerJHSurvival differences by sex for patients with advanced non-small cell lung cancer on Eastern Cooperative Oncology Group trial 1594J Thorac Oncol20061544144617409897
- WeissGJRosellRFossellaFThe impact of induction chemotherapy on the outcome of second-line therapy with pemetrexed or docetaxel in patients with advanced non-small-cell lung cancerAnn Oncol200718345346017322539
- ComellaPFrasciGCarnicelliPGemcitabine with either paclitaxel or vinorelbine vs paclitaxel or gemcitabine alone for elderly or unfit advanced non-small-cell lung cancer patientsBr J Cancer200491348949715266334
- GeorgouliasVAgelidouASyrigosKSecond-line treatment with irinotecan plus cisplatin vs cisplatin of patients with advanced non-small-cell lung cancer pretreated with taxanes and gemcitabine: a multicenter randomized Phase II studyBr J Cancer200593776376916175189
- HanJYLimHSLeeDHRandomized Phase II study of two opposite administration sequences of irinotecan and cisplatin in patients with advanced nonsmall cell lung carcinomaCancer2006106487388016411223
- HelbekkmoNAaseboUSundstromSHvon PlessenCBrunsvigPFBremnesRMTreatment outcome in performance status two advanced NSCLC patients administered platinum-based combination chemotherapyLung Cancer200862225326018417246
- KodaniTUeokaHKiuraKA Phase III randomized trial comparing vindesine and cisplatin with or without ifosfamide in patients with advanced non-small-cell lung cancer: long-term follow-up results and analysis of prognostic factorsLung Cancer200236331331912009244
- KosmidisPMylonakisNSkarlosDPaclitaxel (175 mg/m2) plus carboplatin (6 AUC) versus paclitaxel (225 mg/m2) plus carboplatin (6 AUC) in advanced non-small-cell lung cancer (NSCLC): a multicenter randomized trial. Hellenic Cooperative Oncology Group (HeCOG)Ann Oncol200011779980510997806
- MoscettiLNelliFPadalinoDSperdutiIGiannarelliDPolleraCFGemcitabine and cisplatin in the treatment of elderly patients with advanced non-small cell lung cancer: impact of comorbidities on safety and efficacy outcomeJ Chemother200517668569216433202
- NgeowJLeongSSGaoFImpact of comorbidities on clinical outcomes in non-small cell lung cancer patients who are elderly and/or have poor performance statusCrit Rev Oncol Hematol2010761536019939700
- SculierJPLafitteJJLecomteJA three-arm Phase III randomized trial comparing combinations of platinum derivatives, ifosfamide, and/or gemcitabine in stage IV non-small-cell lung cancerAnn Oncol200213687488212123332
- BischoffHGvan den BorneBPimentelFLObservation of the treatment and outcomes of patients receiving chemotherapy for advanced NSCLC in Europe (ACTION study)Curr Med Res Opin20102661461147020394472
- GirardNJacouletPGainetMThird-line chemotherapy in advanced non-small cell lung cancer: identifying the candidates for routine practiceJ Thorac Oncol20094121544154919884862
- KochAFohlinHSorensonSPrognostic significance of C-reactive protein and smoking in patients with advanced non-small cell lung cancer treated with first-line palliative chemotherapyJ Thorac Oncol20094332633219155996
- ParalkarVRLiTLangerCJPopulation characteristics and prognostic factors in metastatic non-small-cell lung cancer: a Fox Chase Cancer Center retrospectiveClin Lung Cancer20089211612118501099
- ProvencioMCoboMVazquez-EstevezSAnalysis of prognostic factors in patients with advanced non-small cell lung cancer (NSCLC) who are candidates to receive a second-line treatment [abstract]J Clin Oncol201028suppl 15 abstract e18109
- ScartozziMMazzantiPGiampieriRClinical predictive factors for advanced non-small cell lung cancer (NSCLC) patients receiving third-line therapy: selecting the unselectable?Lung Cancer201068343343719664842
- TohCKWongEHLimWTThe impact of smoking status on the behavior and survival outcome of patients with advanced non-small cell lung cancer: a retrospective analysisChest200412661750175615596669
- WangXSShiQLuCPrognostic value of symptom burden for overall survival in patients receiving chemotherapy for advanced nonsmall cell lung cancerCancer2010116113714519852033
- AkechiTOkamuraHOkuyamaTFurukawaTANishiwakiYUchitomiYPsychosocial factors and survival after diagnosis of inoperable non-small cell lung cancerPsychooncology2009181232918484649
- ChuDTKimSWHsuHKPatient attitudes towards chemotherapy and survival: a prospective observational study in advanced non-small cell lung cancerLung Cancer200966225025619264374
- ItayaTYamaotoNAndoMInfluence of histological type, smoking history, and chemotherapy on survival after first-line therapy in patients with advanced non-small cell lung cancerCancer Sci200798222623017233840
- JacotWColinetBBertrandDQuality of life and comorbidity score as prognostic determinants in non-small-cell lung cancer patientsAnn Oncol20081981458146418356134
- ShepherdFAAbrattRCrinoLThe influence of gemcitabine and cisplatin schedule on response and survival in advanced non-small cell lung cancerLung Cancer200030211712511086205
- SculierJPLafitteJJLecomteJA Phase III randomized trial comparing sequential chemotherapy using cisplatin-based regimen and paclitaxel to cisplatin-based chemotherapy alone in advanced non-small-cell lung cancerAnn Oncol20071861037104217404152
- KogureYAndoMChibaYImpact of histology and smoking status on survival outcome of patients with advanced non-small cell lung cancer (NSCLC): West Japan Oncology Group (WJOG) study 3906L [abstract]J Clin Oncol201028Suppl 15 abstract e18013
- QiYSchildSEMandrekarSJPretreatment quality of life is an independent prognostic factor for overall survival in patients with advanced stage non-small cell lung cancerJ Thorac Oncol2009491075108219546817
- BerghmansTLafitteJJLecomteJSecond-line paclitaxel in non-small cell lung cancer initially treated with cisplatin: a study by the European Lung Cancer Working PartyBr J Cancer200796111644164917473825
- TartariRFAbreu NunesCMoreiraJThe mid-arm muscle circumference measurement and the prognosis of stage IV non-small cell lung cancer patients [abstract]J Clin Oncol201028Suppl 15 abstract e18058
- LilenbaumRVillaflorVMLangerCSingle-agent versus combination chemotherapy in patients with advanced non-small cell lung cancer and a performance status of two: prognostic factors and treatment selection based on two large randomized clinical trialsJ Thorac Oncol20094786987419487960
- LiJChenPDaiCHLiXQBaoQLPrognostic factors in elderly patients with advanced non-small cell lung cancer treated with chemotherapyOncology200976535536219321963
- GotoYSekineIYamadaKInfluence of previous chemotherapy on the efficacy of subsequent docetaxel therapy in advanced non-small cell lung cancer patientsJ Thorac Oncol20083441241618379361
- ArdizzoniABoniLTiseoMCisplatin- versus carboplatin-based chemotherapy in first-line treatment of advanced non-small-cell lung cancer: an individual patient data meta-analysisJ Natl Cancer Inst2007991184785717551145
- ObasajuCKAnsariRHSocinskiMAA comparison of white and African American outcomes from a three-arm, randomized, Phase III multicenter trial of advanced or metastatic non-small cell lung cancerJ Thorac Oncol201057993100020593535
- SoriaJCBrisgandDLe ChevalierTDo all patients with advanced non-small-cell lung cancer benefit from cisplatin-based combination therapy?Ann Oncol200112121667167011843242
- SyrigosKNVansteenkisteJParikhPPrognostic and predictive factors in a randomized Phase III trial comparing cisplatin–pemetrexed versus cisplatin–gemcitabine in advanced non-small-cell lung cancerAnn Oncol201021355656119828561
- HirschFRSpreaficoANovelloSWoodMDSimmsLPapottiMThe prognostic and predictive role of histology in advanced non-small cell lung cancer: a literature reviewJ Thorac Oncol20083121468148119057275
- GebbiaVGalettaDDe MarinisFNon small cell lung cancer patients with ECOG PS2: unsolved questions and lessons from clinical trialsAnn Oncol200516Suppl 4iv123iv13115923412
- BerghmansTPaesmansMSculierJPPrognostic factors in stage III non-small cell lung cancer: a review of conventional, metabolic, and new biological variablesTher Adv Med Oncol20113312713821904576
- JemalASiegelRWardECancer statistics, 2008CA Cancer J Clin2008582719618287387
- EdgeSBByrdDRComptonCCFritzAGGreeneFLTrottiAAJCC Cancer Staging Manual7th edNew York, NYSpringer2010
- ScagliottiGBrodowiczTShepherdFTreatment-by-histology interaction analyses in three Phase III trials show superiority of pemetrexed in nonsquamous non-small cell lung cancerJ Thorac Oncol201161647021119545
- SandlerAYiJDahlbergSTreatment outcomes by tumor histology in Eastern Cooperative Group Study E4599 of bevacizumab with paclitaxel/carboplatin for advanced non-small cell lung cancerJ Thorac Oncol2010591416142320686429
- OrdituraMRomanoCDe VitaFBehavior of interleukin-2 serum levels in advanced non-small-cell lung cancer patients: relationship with response to therapy and survivalCancer Immunol Immunother2000491053053611129323