
Abstract
The exclusion of collateral ventilation (CV) and other factors affect the clinical success of endoscopic lung volume reduction (ELVR). However, despite its benefits, the outcome of ELVR remains difficult to predict. We investigated whether clinical success could be predicted by emphysema distribution assessed by computed tomography scan and baseline perfusion assessed by perfusion scintigraphy. Data from 57 patients with no CV in the target lobe (TL) were retrospectively analyzed after ELVR with valves. Pulmonary function tests (PFT), St George’s Respiratory Questionnaire (SGRQ), and 6-minute walk tests (6MWT) were performed on patients at baseline. The sample was grouped into high and low levels at the median of TL perfusion, ipsilateral nontarget lobe (INL) perfusion, and heterogeneity index (HI). These groups were analyzed for association with changes in outcome parameters from baseline to 3 months follow-up. Compared to baseline, patients showed significant improvements in PFT, SGRQ, and 6MWT (all P≤0.001). TL perfusion was not associated with changes in the outcome. High INL perfusion was significantly associated with increases in 6MWT (P=0.014), and high HI was associated with increases in forced expiratory volume in 1 second (FEV1), (P=0.012). Likewise, there were significant correlations for INL perfusion and improvement of 6MWT (r=0.35, P=0.03) and for HI and improvement in FEV1 (r=0.45, P=0.001). This study reveals new attributes that associate with positive outcomes for patient selection prior to ELVR. Patients with high perfusions in INL demonstrated greater improvements in 6MWT, while patients with high HI were more likely to respond in FEV1.
Introduction
Endoscopic lung volume reduction (ELVR) with valves has been shown to improve lung function, exercise capacity, and quality of life in selected patients with severe lung emphysema.Citation1–Citation5 However, a large spectrum of clinical treatment responses has been observed, emphasizing the importance of patient selection prior to treatment.Citation1 Although the selection criteria for ELVR have recently improved, it remains a challenge for clinicians to identify those patients with the highest benefit–risk ratio.
The development of target lobe (TL) atelectasis is an important surrogate marker for clinical response.Citation6,Citation7 A TL volume reduction of >350 mL has been defined in several studies as indicative of significant lobe volume reduction associated with clinical benefits.Citation8 Recent post hoc analyses of large studies have identified complete lobular occlusion by valves and the exclusion of interlobar collateral ventilation (CV) as important predictive factors.Citation9–Citation12 CV is defined as the ventilation between lobes that bypasses the normal airways.Citation13 The importance of CV to the outcome of ELVR was recently demonstrated by a prospective sham-controlled randomized trial.Citation2 It has become clinical routine to assess interlobar CV by the analysis of fissure integrity from computed tomography (CT) scans or by endobronchial in vivo measurement using the Chartis system. Both techniques have shown comparable accuracies.Citation14–Citation16
CT scans and ventilation/perfusion scintigraphy are routinely performed to better characterize COPD lungs prior to ELVR.Citation1,Citation16–Citation18 While emphysema heterogeneity is widely used as a selection criterion for ELVR treatment, its role is currently under discussion: in the original North American VENT study cohort, heterogeneous emphysema distribution predicted improvement in the 6-minute walk test (6MWT) and in the forced expiratory volume in 1 second (FEV1).Citation1 In contrast, the European VENT cohort and two recent studies did not find a difference in outcome parameters for homogenous or heterogeneous emphysema distribution.Citation6,Citation9,Citation16
Low perfusion of the upper lobes, as assessed by ventilation/perfusion scans, was shown to associate with less mortalityCitation19 following lung volume reduction surgery, the surgical equivalent of ELVR. When lung perfusion was taken into consideration for ELVR, a recent study suggested that patients with low perfusion of the TL demonstrated more improvement in exercise capacity after ELVR than patients with high perfusion in the TL.Citation17
In the context that CT and ventilation/perfusion scans are important tools for assessing COPD patients prior to ELVR, we investigated whether emphysema distribution and baseline perfusion of lung lobes help to predict the clinical outcome of ELVR with valves.
Materials and methods
Patients
We retrospectively analyzed 57 patients treated with ELVR between September 2011 and July 2014 at the Charité Hospital in Berlin, Germany. The study design was approved by the ethics committee of the Charité Universitätsmedizin Berlin (EA1/064/12). All patients provided written informed consent. Inclusion criteria for ELVR were age over 40 years, diagnosis of COPD with FEV1 below 45% predicted, and nonsmoker status for at least 3 months proven by HbCO below 2.0%. No ELVR was performed on patients with signs of an infection, myocardial infarction in the past 6 months, and severe comorbidities (malignant disease, severe bronchiectasis, asthma, pulmonary hypertension, and lung fibrosis). For the retrospective analysis, we further excluded patients with α1 antitrypsin deficiency, CV in the TL as detected by the Chartis system, and implantation of valves in the middle lobe, and missing follow-up examination.
Prior to ELVR, all patients underwent pulmonary function tests (PFT) for FEV1, vital capacity (VC), residual volume (RV), diffusing capacity of the lung for carbon monoxide (corrected for lung volume) (KCO), as well as 6MWT and St George’s Respiratory Questionnaire (SGRQ), which ranges from 0 to 100, with higher scores associating with lower quality of life. Low-dose CT under deep inspiration and ventilation/perfusion scintigraphy was performed on patients to assess emphysema distribution and lobe perfusion in the lung. Patients without contraindications for ELVR from these evaluations further received a Chartis assessment (Pulmonx, Redwood City, CA, USA) to exclude possible CV. A team of pneumologists and radiologists defined the primary and alternative TL according to the most emphysematous lobes in the CT scan. If multiple lobes showed a high degree of emphysema, lobes with less perfusion in the scintigraphy were preferred. The perfusion of the ipsilateral adjacent lobe was not considered for TL selection. Finally, the primary or alternative TL was chosen for treatment if no CV was detected in the Chartis assessment. The patients were hospitalized for the ELVR valve treatment. Endobronchial one-way silicone valves (Zephyr, Pulmonx) were implanted in the bronchus via a flexible delivery catheter, and the TL was completely occluded with valves. Follow-up assessment of the patients 3 months later included another CT scan, PFT, 6MWT, and SGRQ. The data were compared to baseline values.
Because left lungs were found to be more frequently negative for CV, ELVR was more often performed in the left lung: right upper lobe (RUL; n=7), right lower lobe (RLL; n=4), left upper lobe (LUL; n=13), and left lower lobe (LLL; n=33).
Perfusion scintigraphy
Lung perfusion was assessed using a combined single-photon emission computed tomography (SPECT) and CT system. Technical details of the procedure are available in the supplementary material. Only the posterior-to-anterior planar views were analyzed due to the lack of software-based quantification tools for SPECT. Each lung perfusion scintigram was split craniocaudally into three regions to quantify the distribution of the tracer in the lungs. The perfusion was calculated as the percentage of tracer activity in the upper, middle, and lower regions of the right and left lung. The upper region perfusion was used as a surrogate for upper lobe perfusion, and the lower region perfusion was used as a surrogate for lower lobe perfusion, as recently described.Citation17 The perfusion of the middle region was not considered for further analyses. shows examples of different perfusion scintigrams. Three patients had no ventilation and perfusion scintigraphies and were excluded from the analyses of TL and ipsilateral nontarget lobe (INL) perfusion.
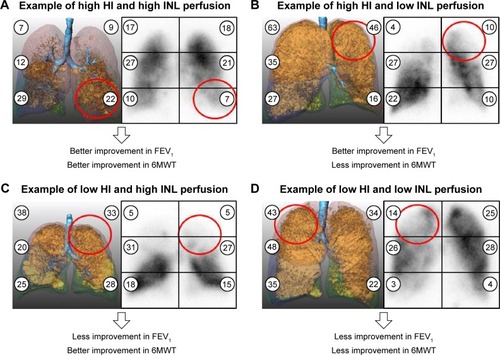
Figure 1 Quantification of baseline CT and perfusion scintigrams prior to ELVR with valves.
Abbreviations: CT, computed tomograms; ELVR, endoscopic lung volume reduction; FEV1, forced expiratory volume in 1 second; 6MWT, 6-minute walk test; HI, heterogeneity index; TL, target lobe; INL, ipsilateral nontarget lobe.
Low-dose CT scans
Patients underwent a CT scan for TL selection and emphysema evaluation at baseline and 3 months after endoscopic valve implantation as follow-up. All patients were examined using the same CT scanner (General Electric LightSpeed Ultra 8, General Electric Inc, Milwaukee, WI, USA) and the same scanning protocol (continuous helical scan of the whole lung in deep inspiratory breath hold, no intravenous contrast agent, primary slice thickness 1.25 mm, 100 kV voltage, and 100 mA current). Reconstruction of the raw CT data was performed using a “standard” (soft tissue) kernel. Quantitative analysis of lung parenchyma from CT data was performed semiautomatically using the MeVisPULMO3D software (v3.42, Fraunhofer MeVis, Bremen, Germany). The software was able to evaluate the distribution of emphysema by calculating the pixel index, defined as the ratio of lung voxels with a density <−950 Hounsfield units to the total number of voxels in the lung per lobe, which also is the emphysema score per lobe. The heterogeneity index (HI) was defined as the difference in emphysema score between TL and ipsilateral nontarget upper or lower lobe, as previously reported.Citation1,Citation9,Citation20 The middle lobe was not considered for further analyses. shows examples of different emphysema distributions. TL volume reduction was calculated as the difference between TL volume at baseline and TL volume at follow-up. Three patients had no baseline CT data and were excluded from the heterogeneity analysis.
Statistics
First, patients were grouped into high and low levels at 1) the median of TL perfusion (Table S1), 2) the median of INL perfusion (), and 3) the median of HI (). Between these groups, the changes in the outcome parameters (PFT, SGRQ, and 6MWT) were compared. Next, correlations were calculated between TL perfusion, INL perfusion, HI, and the changes in the outcome parameters. The chi-square test and the Fisher’s exact test were used for the statistical analysis of categorical variables. The Mann–Whitney U-test was used for continuous variables. The Wilcoxon test was used for paired samples, eg, changes in the outcome parameters from baseline to follow-up. Correlations were assessed by Pearson’s correlation coefficient and Student’s t-test. All tests were two-tailed. SPSS Statistics Version 22 (IBM Corporation, Armonk, NY, USA) was used for all analyses. The data are presented as mean ± standard deviation. A P-value <0.05 was considered statistically significant.
Table 1 Patient baseline characteristics and clinical outcome with respect to baseline INL perfusion
Table 2 Patient baseline characteristics and clinical outcome with respect to baseline HI
Results
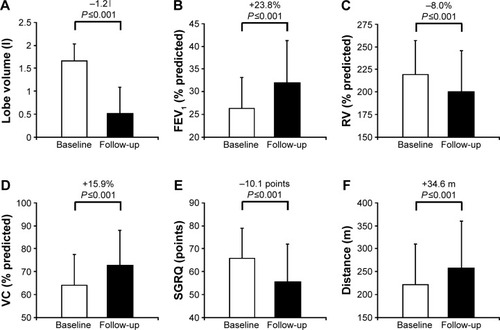
Fifty-seven patients, assessed to be negative for CV by Chartis, were treated with endobronchial valves. Compared to baseline, all patients demonstrated at follow-up a mean volume reduction in the TL of 1<184±577 mL, an improvement in FEV1 of 23.8%±24.9%, RV of −8.0%±17.3%, VC of 15.9%±23.2%, SGRQ of −10.1±14.0 points, and 6MWT of 34.6±62.3 m (all P≤0.001, ). Further details are listed in Table S2.
Figure 2 Clinical outcomes of patients after ELVR with valves.
Abbreviations: ELVR, endoscopic lung volume reduction; TLV, target lobe volume; FEV1, forced expiratory volume in 1 second; RV, residual volume; VC, vital capacity; SGRQ, St George’s Respiratory Questionnaire; 6MWT, 6-minute walk test.
The baseline characteristics and outcome data for TL perfusion, INL perfusion, and HI groups are listed in , and S1. The TL perfusion ranged from 1.8% to 19.9% with a median of 8.11% (Table S1), the INL perfusion ranged from 3.4% to 25.7% with a median of 14.7% (), and HI ranged from 0.6% to 32.8% with a median of 12.2% (). The median perfusion was lowest in LLL (8.8%), compared to LUL (14.7%), RLL (13.4%), and RUL (13.4%). With respect to HI, 27 patients were categorized in the homogeneous emphysema group and 27 patients were in the heterogeneous emphysema group (cutoff 12.2%).
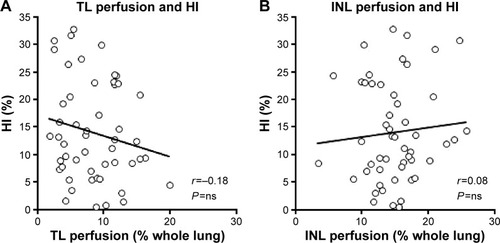
There were no significant correlations between TL perfusion and HI as well as INL perfusion and HI (). Likewise, the distribution of patients into the four group combinations of low or high TL perfusion and low or high HI was not significantly different (P=0.58, Table S3). The same was observed for the groups of low and high INL perfusion and low or high HI (P=1.0, Table S3).
Figure 3 Correlation between lung perfusion and HI.
Abbreviations: HI, heterogeneity index; TL, target lobe; INL, ipsilateral nontarget lobe; r, Pearson’s correlation coefficient; ns, not significant.
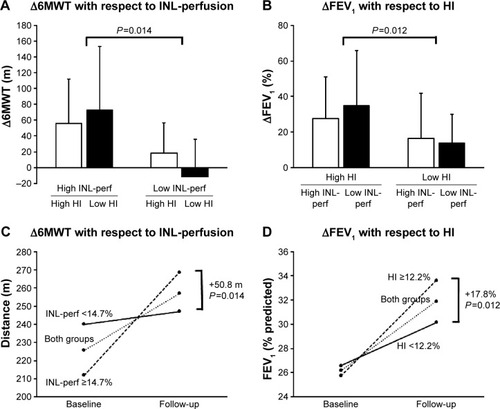
Comparing TL perfusion, INL perfusion, and HI to outcome parameters, low vs high TL perfusion was not associated with any outcome indices (Table S1). In contrast, patients with INL perfusion >14.7% demonstrated a higher increase in 6MWT than patients with INL perfusion below 14.7% (P=0.014), while the other outcome parameters were similar for both groups (). Likewise, patients with HI >12.2% had a higher improvement in FEV1 than patients with HI <12.2% (P=0.012), while the other outcome parameters were similar for both groups ().
To confirm these results, TL perfusion, INL perfusion, and HI were tested for correlation with the outcome parameters. Likewise, no significant correlation was identified between TL perfusion and any change in clinical outcome (Figure S1). Again, INL perfusion was significantly correlated only with changes in the 6MWT between baseline and follow-up (r=0.35, P=0.03; ), and not with changes in TL volume (r=−0.05, P=not significant [ns]), FEV1 (r=0.01, P=ns), RV (r=−0.10, P=ns), VC (r=0.07, P=ns), KCO (r=−0.08, P=ns), and SGRQ (r=−0.11, P=ns; Figure S2). Similarly, HI demonstrated a significant correlation only with changes in FEV1 (r=0.45, P=0.001; ), but not with changes in TL volume (r=−0.09, P=ns), RV (r=−0.12, P=ns), VC (r=0.14, P=ns), SGRQ (r=−0.15, P=ns), KCO (r=−0.05, P=ns), and 6MWT (r=0.05, P=ns; Figure S3). Interestingly, improvement of 6MWT of 50.8 m among patients with high INH perfusion compared to low INL perfusion was independent of the HI (), and, likewise, improvement of FEV1 of 17.8% among patients with high HI compared to low HI was not associated with INL perfusion ().
Figure 4 Correlations between perfusion of the INL, HI and outcome parameters.
Notes: P-values were calculated using the Student’s t-test. (A) Correlation between INL perfusion and change in Δ6MWT after ELVR. (B) Correlation between HI and ΔFEV1 after ELVR.
Abbreviations: INL, ipsilateral nontarget lobe; HI, heterogeneity index; 6MWT, 6-minute walk test; ELVR, endoscopic lung volume reduction; FEV1, forced expiratory volume in 1 second; r, Pearson’s correlation coefficient; Δ, change from baseline to follow-up.
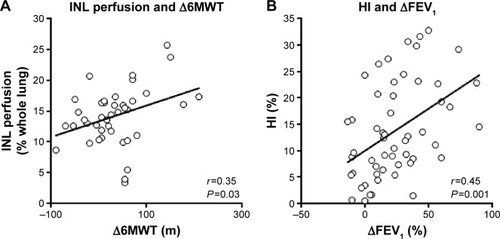
Figure 5 Clinical outcome according to baseline percentage perfusion of the INL and the HI.
Abbreviations: INL, ipsilateral nontarget lobe; HI, heterogeneity index; 6MWT, six-minute walk test; FEV1, forced expiratory volume in 1 second; perf, perfusion; TL, target lobe; INL, ipsilateral nontarget lobe; Δ, change from baseline to follow-up.
Discussion
In this study, we found a significant correlation between high INL perfusion and larger improvement in the 6MWT and between a high HI and larger improvement in FEV1. Analyzing subgroups, patients with high INL perfusion (cutoff 14.7%) benefited from a greater improvement of 50.8 m in the 6MWT compared to those with low INL perfusion, while patients with a heterogeneous emphysema distribution (cutoff 12.2% HI) showed a higher increase in FEV1 of 17.8% compared to those with low HI.
Important factors were recently characterized to predict the clinical success of ELVR. Several studies suggest that ELVR is an effective treatment option if complete lobar occlusion with valves is achieved.Citation2,Citation8–Citation10 In line, other studies have shown valve treatment to be less efficient, if valves were placed in both lungs without the goal of lobar occlusion.Citation11,Citation12 A post hoc analysis of the US- and Euro-VENT studies identified a subset of patients who had no CV and who achieved higher lung volume reduction and greater clinical response.Citation1,Citation9 The importance of the absence of CV to the outcome was recently confirmed by the BeLieVeR-HIFi study in a randomized, sham-controlled study design.Citation2 Subsequently, it has become routine practice to assess interlobar CV by analysis of fissure integrity on high-resolution CT scan or by real-time endobronchial in vivo measurement with the Chartis system.Citation3,Citation4,Citation8,Citation14
This study suggests that INL lung perfusion significantly predicts the improvement of the 6MWT after ELVR. Consequently, perfusion scintigraphy seems to be an important criterion for baseline evaluation of patients prior to ELVR. Among COPD patients, we observed a large variability of TL and INL perfusions ranging from very high to extreme low, which supports the concept of COPD heterogeneity.Citation21,Citation22 In this context, it is important to note that the perfusion of TL or INL is calculated as a percentage of the perfusion of the total lung. Therefore, a seemingly homogeneously perfused COPD lung might be severely impaired due to homogeneous parenchymal destructions of the lung. Similar to other authors, we found an association between perfusion and emphysema score (Figure S4).Citation23 Interestingly, however, we also identified severe hypoperfused regions irrespective of the emphysematic changes, suggesting other pulmonary vascular abnormalities such as local vascular inflammation with remodeling to be relevant to these COPD lungs.Citation24,Citation25
It remains unclear how perfusion affects improvements in the 6MWT after ELVR. The 6MWT is a predictor of mortality in patients with severe emphysema and has been established in the evaluation of COPD patients.Citation26–Citation28 It reflects the exercise capacity of patients based on the pulmonary, cardiovascular, and muscular systems. Chung et alCitation29 first examined perfusion in patients treated with ELVR and reported that perfusion decreased in the treated lung, while it increased in the contralateral lung. This was confirmed by other studies, which specified that after the treated lobe was reduced in volume, the perfusion and volume was redirected to the INL and to the contralateral lung.Citation18,Citation30,Citation31 This interesting finding suggests that both the INL and contralateral lung take over functionality after development of an atelectasis of the TL, which explains the importance of the INL.Citation32
However, while we did not find an effect of TL perfusion on the 6MWT, a recent study by Argula et alCitation17 reports a better 6MWT performance in patients with low TL perfusion. This may be due to the fact that we mostly treated the lower lobes of patients, which were already associated with less perfusion, while Argula et alCitation17 mostly treated the upper lobes of patients. Moreover, Argula et al’sCitation17 data also consisted of a slightly higher proportion of patients with heterogeneous lung emphysema in comparison to our study group. Nevertheless, high INL perfusion seems to be an indicator of a relatively healthier functional lobe, while low TL perfusion probably indicates a more damaged lobe. We hypothesize that the findings of improved 6MWT in low TL perfusion and high INL perfusion may together represent an optimal setting for ELVR: a more functional INL with high perfusion and a more damaged TL with low perfusion.
Recent studies suggest that each lung lobe contributes differently to the pulmonary function; the lower lobes demonstrated a higher association to the FEV1 than the upper lobes.Citation33,Citation34 In this study, mostly the LLL was treated, which might be another explanation why the changes in lung function were greater than in previous studies like the VENT study. However, because the lower lobes in general, and especially the LLL, were treated more often in this cohort, we cannot evaluate this effect due to the small number of patients in whom the upper lobes were treated. A small study by Eberhardt et alCitation35 found no difference for the treatment of upper vs lower lobes with valves. Nevertheless, future studies with an equal distribution of the TL are needed to test for a different outcome of ELVR for each specific TL. Moreover, the recent interesting studies by Matsuo et alCitation33 and Kitano et alCitation34 used the normal lobar volume and the collapsibility index as CT-derived indices to analyze lobar physiology and function. These indices might be useful in the future to evaluate lung lobes prior to ELVR.
Another important finding of this study is the correlation of improvement in FEV1 after ELVR to the baseline HI, suggesting a greater improvement of FEV1 in patients with higher differences in the emphysema distribution between TL and the ipsilateral nontarget upper or lower lobe (middle lobes were not considered for HI calculations). There are several possible explanations for this observation: in lungs with heterogeneous emphysema, the TL consists of more bullae and cysts compared to the INL, while in homogeneous emphysema, both are more evenly distributed. Because these bullae and cysts are the main contributors to the hyperinflation, ELVR of the TL in a high heterogeneity lung may lead to a more significant reduction hyperinflation and consequently improve respiratory mechanics and air trapping. Moreover, compressed areas of the better-preserved adjacent lobes can reinflate to increase the surface of the lung to improve the gas exchange. This finding is in agreement with the North American VENT cohort reporting better clinical results in patients with heterogeneous compared to homogeneous emphysema.Citation1 However, some other studies have not observed these associations of emphysema distribution and outcome changes;Citation6,Citation9,Citation16 therefore, further studies are urgently needed for clarification. Currently, a prospective randomized trial is studying the effect of ELVR in patients with homogeneous and heterogeneous lung emphysema and no CV.Citation36
A standardized definition of how to distinguish between heterogeneous and homogeneous lung emphysema is still lacking. In clinical routine and some other studies, heterogeneity is visually assessed on native CT scans,Citation2,Citation37,Citation38 which is observer dependent and therefore highly variable. Software-based quantification tools allow investigators to quantify precisely the severity of emphysema in the lobes. Some studies converted the quantified emphysema score to a Likert scale to determine the HI.Citation39,Citation40 This study used the definition of the VENT study, which defined the HI as the difference in emphysema score between the target and the ipsilateral adjacent lobe.Citation1 The median HI was 15% in the VENT study, which was used to split patients into low and high HI subgroups. The 15% median was suggested as an arbitrary cutoff marker for homogeneous and heterogeneous emphysema. Applying the same method, we split the patients into a low and high heterogeneity group at the median HI in this study. The median of 12.2% suggests a higher fraction of patients with homogeneous emphysema compared to the VENT. Nevertheless, there was a significant correlation between HI and FEV1 improvement, indicating the predictive value of the HI regardless of a cutoff.
It is interesting to note that baseline HI was the main contributor of FEV1 improvement, while INL perfusion was almost only associated with increases of 6MWT after ELVR. This suggess that morphologic changes of emphysematous damaged lobes are more likely to influence breathing mechanics, while INL perfusion shows higher correlations to exercise capacity. On the basis of the findings for INL perfusion and HI, we distinguished four COPD patient groups according to their baseline perfusion and HI in the TL: 1) patients with HI and high INL perfusion who were more likely to improve in FEV1 and 6MWT; 2) patients with high HI and low INL perfusion who demonstrated better improvements in FEV1, but less in 6MWT; 3) patients with low HI and high INL perfusion who showed less improvement in FEV1 but higher 6MWT changes; and 4) patients with low HI and low INL who were less likely to respond in FEV1 and 6MWT. Especially the last patient group might be a new subgroup to show limited response to ELVR even though this patient group fulfilled the other factors relevant to clinical success (significant hyperinflation in PFT, negative CV in TL, and complete lobar occlusion with valves).
Several possible limitations of this study should be considered. The division of planar perfusion scintigrams into thirds is only a rough estimation of lung perfusion and reduces the accuracy of the data. This limitation could be addressed in the future by software-based quantification tools for SPECT, which analyze the perfusion for each anatomical lung lobe. These tools showed impressive initial results, but are not yet widely used.Citation41,Citation42 Consequently, future studies should be performed using software-based quantification tools for SPECT to reassess the role of pulmonary perfusion for ELVR patient selection. However, because perfusion scintigraphy is already widely used prior to ELVR, the findings of this study are still highly relevant despite the limitations of planar perfusion imaging until SPECT is established in the clinical routine.
This is a retrospective analysis without blinding or patient randomization, and baseline characteristics are not evenly distributed, and so a selection bias cannot be excluded. CT scan and perfusion scintigraphy were also used for TL selection, which might bias the results. Therefore, prospective studies with well-matched and larger cohorts are urgently needed to confirm these results. Correlation analyses need careful interpretation due to the possible role of confounding variables, which might not have been considered. The only data that were evaluated were those in patients’ files, as a consequence of the retrospective study design. We used the medians to discriminate between low and high INL perfusion and low and high HI; however, there might be better cutoff values for discriminating between the patient subgroups. To better understand the improvements in exercise capacity, other exercise tests, such as spiroergometry, are needed.
In summary, patient selection remains critical in ELVR because it bears the risk of severe complications.Citation43 Baseline HI and lobe perfusion may help to identify patients who benefit most from ELVR treatment. While patients with heterogeneous emphysema are more likely to profit from improved breathing mechanics, patients with high INL perfusion might benefit from improved exercise capacity. These predictors could be helpful in selecting both the patient and the TL for ELVR.
Acknowledgments
We thank Melanie Wegemund for her excellent assistance in data collection. This work is part of the doctoral thesis of Christian Thomsen.
Supplementary materials
Online supplement
Technical details of perfusion scintigraphy
Ventilation and perfusion were assessed using a hybrid dual-head Siemens Symbia TruePoint T6 SPECT/CT system (Siemens Medical Solutions, Erlangen, Germany), which has a crystal thickness of 9.5 mm, and a 53.3 cm axial by 38.7 cm diameter single-photon emission computed tomography (SPECT) field of view. The scans were performed following a 1-day standard protocol: 128×128 acquisition matrix, zoom 1.0, pixel size 4.8 mm, and noncircular orbit (autocontour) with 30 projections over 180° (continuous acquisition). A low-energy high-resolution collimator was used with dual-energy windowing, and a lower scatter energy window (10% width) for scatter estimation. Thirty samples, each of 15 seconds duration, were used for both the ventilation and the perfusion study. The total acquisition time was approximately 20 minutes. The seated patient inhaled about 60 MBq Tc-99m Technegas (Tema 10,000, Cyclomedica GmbH, Salzgitter, Germany) and the ventilation SPECT was performed. After the ventilation SPECT was performed, 100–120 MBq of 99 mTc-labeled human albumin macroaggregates (Mallinckrodt Medical BV, Petten, the Netherlands) were slowly injected intravenously while the patient took deep breaths. Perfusion tomography was then performed on the patient who was lying down. Only posterior-to-anterior planar views were used for further analyses due to the lack of software-based quantification tools for SPECT.
This study protocol was already described by the coauthors in another study using the same patients and procedure.Citation1
Figure S1 Correlations with baseline percentage perfusion of the TL.
Notes: P-values were calculated using the Student’s t-test. (A) Correlation between TL perfusion and ΔTLV. (B) Correlation between TL perfusion and ΔFEV1. (C) Correlation between TL perfusion and ΔRV. (D) Correlation between TL perfusion and ΔVC. (E) Correlation between TL perfusion and ΔSGRQ. (F) Correlation between TL perfusion and Δ6MWT.
Abbreviations: TL, target lobe; Δ, change from baseline to follow-up; TLV, target lobe volume; r, Pearson’s correlation coefficient; ns, not significant; FEV1, forced expiratory volume in 1 second; RV, residual volume; SGRQ, St George’s Respiratory Questionnaire; 6MWT, 6-minute walk test distance; VC, vital capacity.
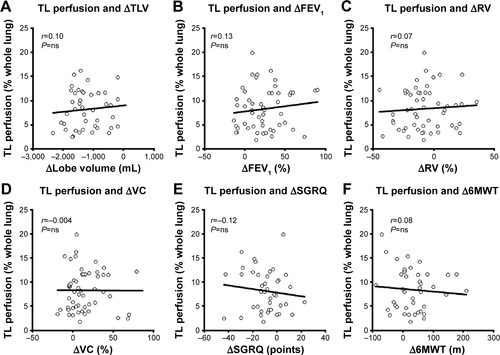
Figure S2 Correlations with baseline percentage perfusion of the INL.
Notes: P-values were calculated using the Student’s t-test. (A) Correlation between INL perfusion and ΔTLV. (B) Correlation between INL perfusion and ΔFEV1. (C) Correlation between INL perfusion and ΔRV. (D) Correlation between INL perfusion and ΔVC. (E) Correlation between INL perfusion and ΔSGRQ. (F) Correlation between INL perfusion and Δ6MWT.
Abbreviations: INL, ipsilateral nontarget lobe; Δ, change from baseline to follow-up; TLV, target lobe volume; r, Pearson’s correlation coefficient; ns, not significant; FEV1, forced expiratory volume in 1 second; RV, residual volume; SGRQ, St George’s Respiratory Questionnaire; 6MWT, 6-minute walk test distance; VC, vital capacity.
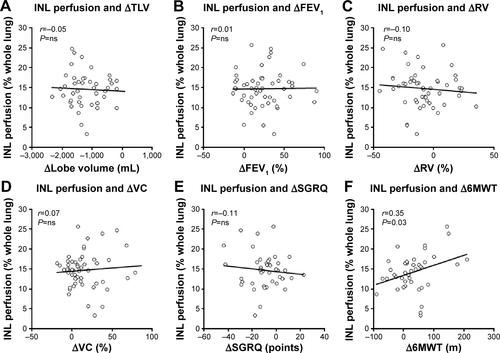
Figure S3 Correlations with baseline HI.
Notes: HI is the difference in emphysema scores between the potential TL and the ipsilateral lobe. P-values were calculated using the Student’s t-test. (A) Correlation between HI and ΔTLV. (B) Correlation between HI and ΔFEV1. (C) Correlation between HI and ΔRV. (D) Correlation between HI and ΔVC. (E) Correlation between HI and ΔSGRQ. (F) Correlation between HI and Δ6MWT.
Abbreviations: HI, heterogeneity index; TL, target lobe; Δ, change from baseline to follow-up; TLV, target lobe volume; r, Pearson’s correlation coefficient; ns, not significant; FEV1, forced expiratory volume in 1 second; RV, residual volume; SGRQ, St George’s Respiratory Questionnaire; 6MWT, 6-minute walk test distance; VC, vital capacity.
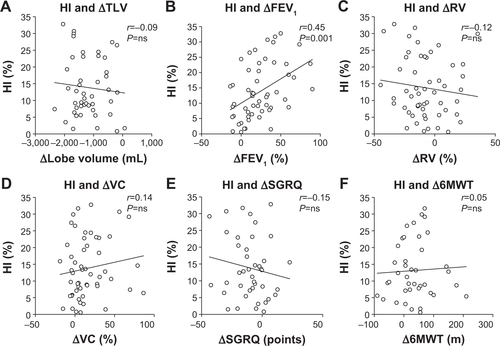
Figure S4 Correlations between baseline perfusion and ES for each lung lobe.
Notes: P-values were calculated using the Student’s t-test. (A) Correlation between baseline perfusion and ES for the RUL. (B) Correlation between baseline perfusion and ES for the LUL. (C) Correlation between baseline perfusion and ES for the RLL. (D) Correlation between baseline perfusion and ES for the LLL.
Abbreviations: ES, emphysema score; RUL, right upper lobe; LUL, left upper lobe; RLL, right lower lobe; LLL, left lower lobe; r, Pearson’s correlation coefficient.
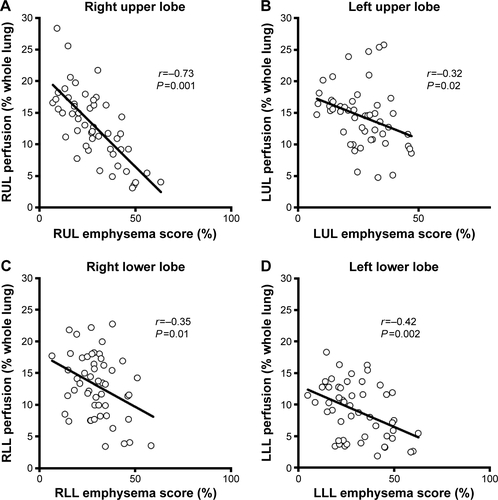
Table S1 Patient baseline characteristics and clinical outcome with respect to baseline TL perfusion
Table S2 Clinical outcome after ELVR
Table S3 Patient groups with respect to perfusion and emphysema heterogeneity
Reference
- FroelingVHeimannUHuebnerR-HVentilation/perfusion SPECT or SPECT/CT for lung function imaging in patients with pulmonary emphysema?Ann Nucl Med201529652853425939639
Disclosure
Ralf-Harto Hubner has received lecture fees for educational activities and consulting fees from Pulmonx. The other authors have declared no conflict of interest in this work.
References
- SciurbaFCErnstAHerthFJFA randomized study of endobronchial valves for advanced emphysemaN Engl J Med2010363131233124420860505
- DaveyCZoumotZJordanSBronchoscopic lung volume reduction with endobronchial valves for patients with heterogeneous emphysema and intact interlobar fissures (the BeLieVeR-HIFi study): a randomised controlled trialLancet201538699981066107326116485
- ShahPLHerthFJFCurrent status of bronchoscopic lung volume reduction with endobronchial valvesThorax201469328028624008689
- HerzogDDöllingerFTemmesfeld-WollbrückBHübnerR-HInterventionelle bronchologische Therapie [Interventional bronchoscopic therapy]Pneumologe2014112135143 German
- ParkTSHongYLeeJSBronchoscopic lung volume reduction by endobronchial valve in advanced emphysema: the first Asian reportInt J Chron Obstruct Pulmon Dis20151011501151126251590
- ValipourAHerthFJFBurghuberOCTarget lobe volume reduction and COPD outcome measures after endobronchial valve therapyEur Respir J201443238739623845721
- HopkinsonNSKempSVTomaTPAtelectasis and survival after bronchoscopic lung volume reduction for COPDEur Respir J20113761346135120947683
- HerthFJFEberhardtRGompelmannDRadiological and clinical outcomes of using Chartis™ to plan endobronchial valve treatmentEur Respir J201341230230822556025
- HerthFJFNoppenMValipourAEfficacy predictors of lung volume reduction with Zephyr valves in a European cohortEur Respir J20123961334134222282552
- KoegelenbergCFNSlebosD-JShahPLTime for the global rollout of endoscopic lung volume reductionRespiration201590543044026393503
- NinaneVGeltnerCBezziMMulticentre European study for the treatment of advanced emphysema with bronchial valvesEur Respir J20123961319132522654006
- EberhardtRGompelmannDSchuhmannMHeusselCPHerthFJComplete unilateral vs partial bilateral endoscopic lung volume reduction in patients with bilateral lung emphysemaChest2012142490090822459779
- GompelmannDEberhardtRHerthFJFCollateral ventilationRespiration201385651552023485627
- GompelmannDEberhardtRSlebosD-JDiagnostic performance comparison of the Chartis system and high-resolution computerized tomography fissure analysis for planning endoscopic lung volume reductionRespirology201419452453024612306
- DoellingerFHuebnerRHKuhnigkJMPoellingerALung volume reduction in pulmonary emphysema from the radiologist’s perspectiveRofo2015187866267526062174
- SchuhmannMRaffyPYinYComputed tomography predictors of response to endobronchial valve lung reduction treatment: comparison with ChartisAm J Respir Crit Care Med2015191776777425635349
- ArgulaRGStrangeCRamakrishnanVGoldinJBaseline regional perfusion impacts exercise response to endobronchial valve therapy in advanced pulmonary emphysemaChest201314451578158623828481
- PizarroCAhmadzadehfarHEsslerMFimmersRNickenigGSkowaschDVolumetric and scintigraphic changes following endoscopic lung volume reductionEur Respir J201545126226525359337
- ChandraDLipsonDAHoffmanEAPerfusion scintigraphy and patient selection for lung volume reduction surgeryAm J Respir Crit Care Med2010182793794620538961
- ValipourAShahPLGesierichWPatterns of emphysema heterogeneityRespiration201590540241126430783
- AgustiAGeaJFanerRBiomarkers, the control panel and personalized COPD medicineRespirology2016211243326172306
- AgustiACalverleyPMCelliBCharacterisation of COPD heterogeneity in the ECLIPSE cohortRespir Res201011112220831787
- HueperKVogel-ClaussenJParikhMAPulmonary microvascular blood flow in mild chronic obstructive pulmonary disease and emphysema. The MESA COPD StudyAm J Respir Crit Care Med2015192557058026067761
- HarknessLMKanabarVSharmaHSWestergren-ThorssonGLarsson-CallerfeltA-KPulmonary vascular changes in asthma and COPDPulm Pharmacol Ther201429214415525316209
- SantosSPeinadoVIRamírezJCharacterization of pulmonary vascular remodelling in smokers and patients with mild COPDEur Respir J200219463263811998991
- Pinto-PlataVMCoteCCabralHTaylorJCelliBRThe 6-min walk distance: change over time and value as a predictor of survival in severe COPDEur Respir J2004231283314738227
- CasanovaCCoteCMarinJMDistance and oxygen desaturation during the 6-min walk test as predictors of long-term mortality in patients with COPDChest2008134474675218625667
- TakigawaNTadaASodaRDistance and oxygen desaturation in 6-min walk test predict prognosis in COPD patientsRespir Med2007101356156716899358
- ChungSCSPetersMJChenSEmmettLIngAJEffect of unilateral endobronchial valve insertion on pulmonary ventilation and perfusion: a pilot studyRespirology20101571079108320636308
- PizarroCAhmadzadehfarHEsslerMEffect of endobronchial valve therapy on pulmonary perfusion and ventilation distributionPLoS One2015103e011897625822624
- BrownMSKimHJAbtinFGEmphysema lung lobe volume reduction: effects on the ipsilateral and contralateral lobesEur Radiol20122271547155522466511
- KotloffRMHansen-FlaschenJLipsonDAApical perfusion fraction as a predictor of short-term functional outcome following bilateral lung volume reduction surgeryChest200112051609161511713142
- MatsuoKIwanoSOkadaTKoikeWNaganawaS3D-CT lung volumetry using multidetector row computed tomography: pulmonary function of each anatomic lobeJ Thorac Imaging201227316417021873909
- KitanoMIwanoSHashimotoNMatsuoKHasegawaYNaganawaSLobar analysis of collapsibility indices to assess functional lung volumes in COPD patientsInt J Chron Obstruct Pulmon Dis2014911347135625525352
- EberhardtRHerthFJFRadhakrishnanSGompelmannDComparing clinical outcomes in upper versus lower lobe endobronchial valve treatment in severe emphysemaRespiration201590431432026340540
- ValipourABurghuberOCAn update on the efficacy of endobronchial valve therapy in the management of hyperinflation in patients with chronic obstructive pulmonary diseaseTher Adv Respir Dis20159629430126294417
- FishmanAMartinezFNaunheimKNational Emphysema Treatment Trial Research GroupA randomized trial comparing lung-volume–reduction surgery with medical therapy for severe emphysemaN Engl J Med2003348212059207312759479
- BandyopadhyaySHenneEGuptaASegmental approach to lung volume reduction therapy for emphysema patientsRespiration2015891768125500669
- TsuzukuAAsanoFMiyazawaTCT assessment of lobar heterogenity and fissure integrity in pulmonary emphysema for bronchoscopic lung volume reduction with valveEur Respir J201546Suppl 59PA763
- ShahPSlebosD-JCardosoPBronchoscopic lung-volume reduction with Exhale airway stents for emphysema (EASE trial): randomised, sham-controlled, multicentre trialLancet20113789795997100521907863
- SchreiterVSteffenIHuebnerHVentilation/perfusion SPECT/CT in patients with pulmonary emphysema. Evaluation of software-based analysingNuklearmedizin2015541313525683108
- HeWZhaiWHAvondoJBertlingSThe clinical value of novel hybrid 3D lobar quantification SPECT lung ventilation/perfusion scan in predicting remaining lung function for lobectomy lung cancer patientsJ Nucl Med201455Suppl 1536
- HerzogDPoellingerADoellingerFModifying post-operative medical care after EBV implant may reduce pneumothorax incidencePLoS One2015105e012809726010886