
Abstract
Background
This study was conducted to investigate whether point-of-care (POC) procalcitonin (PCT) measurement can reduce redundant antibiotic treatment in patients hospitalized with acute exacerbation of COPD (AECOPD).
Methods
One-hundred and twenty adult patients admitted with AECOPD were enrolled in this open-label randomized trial. Patients were allocated to either the POC PCT-guided intervention arm (n=62) or the control arm, in which antibiotic therapy followed local guidelines (n=58).
Results
The median duration of antibiotic exposure was 3.5 (interquartile range [IQR] 0–10) days in the PCT-arm vs 8.5 (IQR 1–11) days in the control arm (P=0.0169, Wilcoxon) for the intention-to-treat population. The proportion of patients using antibiotics for ≥5 days within the 28-day follow-up was 41.9% (PCT-arm) vs 67.2% (P=0.006, Fisher’s exact) in the intention-to-treat population. For the per-protocol population, the proportions were 21.1% (PCT-arm) vs 73.9% (P<0.00001, Fisher’s exact). Within 28-day follow-up, one patient died in the PCT-arm and two died in the control arm. A composite harm end point consisting of death, rehospitalization, or intensive care unit admission, all within 28 days, showed no apparent difference.
Conclusion
Our study shows that the implementation of a POC PCT-guided algorithm can be used to substantially reduce antibiotic exposure in patients hospitalized with AECOPD, with no apparent harm.
Introduction
Repeated exacerbations and comorbidities contribute to increased morbidity and mortality and affect the quality of life in patients suffering from COPD. Besides the standard treatment with oral corticosteroids and bronchodilators, acute exacerbations of COPD (AECOPD) are often treated with antibiotics, since this has shown to improve prognosis in patients with AECOPD and purulent sputum.Citation1,Citation2 However, only about half of all AECOPD cases are caused by infectious agents, among which viruses seem to be the leading cause.Citation3–Citation5 Thus, current recommendations may lead to preventable overuse of antibiotics, thereby increasing resistance rates and side effects.Citation6,Citation7
It can be challenging for the clinician to identify patients with bacterial AECOPD, as clinical signs, symptoms, and laboratory parameters are often inconclusive. Among other uncertainties, the clinician has to consider that 25%–50% of patients with stable COPD are chronically colonized with potentially pathogenic bacteria; however, these colonizing strains seem to play a minor role in the event of AECOPD.Citation8–Citation10
Procalcitonin (PCT) is the prehormone of calcitonin that is released by most types of parenchymal cells (except blood cells and neurons) through direct cytokine stimulation after bacterial infection,Citation11 and serum PCT levels increase with the severity of bacterial infection.Citation12,Citation13 PCT is released 2–6 hours after bacteria or parts of them are presented in the blood, which is faster than the release of C-reactive protein (CRP).Citation14 Furthermore, CRP appears to be less sensitive and specific than PCT for the detection of bacterial infection.Citation15 Finally, PCT is superior to CRP in the diagnosis of sepsis.Citation16
PCT has been used as a tool to reduce antibiotic exposure in patients with clinical signs of lower respiratory tract infections (LRTIs).Citation17–Citation19 Thus, PCT measurements have the potential to guide the physician in identifying patients with AECOPD who do not require antibiotic treatment.
However, rapid detection of PCT levels in the daily assessment of patients with AECOPD can be logistically and economically challenging and not all local biochemistry laboratories offer the test. Point-of-care (POC) measurements of PCT may increase awareness and availability of test results in a timely manner. POC PCT detection as a tool to reduce antibiotic exposure in patients admitted to hospital with AECOPD has not yet been evaluated in a randomized trial.
Furthermore, earlier studies evaluating PCT as a tool to reduce antibiotic prescription in LRTI were mainly conducted by a single Swiss research group, thus suggesting external validation of this strategy.
This study aimed to determine whether a POC PCT-guided antibiotic therapy could reduce the overall use of antibiotics among patients hospitalized for AECOPD in a population of Danish COPD patients.
Methods
Setting and study population
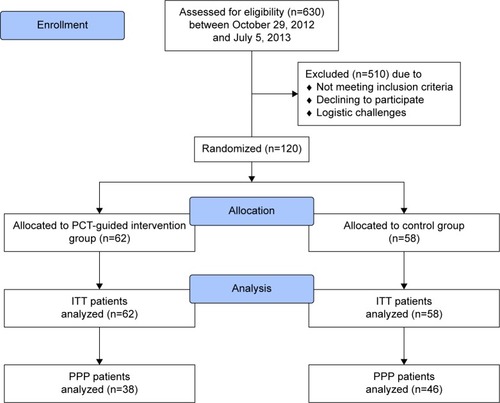
From October 29, 2012, to July 5, 2013, 630 patients admitted with AECOPD were screened at the emergency department at Copenhagen University Hospital Bispebjerg and 120 were found eligible to participate in the Procalcitonin To Reduce Antibiotics in Chronic Obstructive Lung Disease (ProToCOLD) study.
Patients were eligible for the intervention if they met the following criteria: 1) ≥18 years old and 2) admitted with an AECOPD (clinician’s diagnosis at admission), defined according to the Global Initiative for Chronic Obstructive Lung Disease (GOLD).Citation20 The exclusion criteria in the study were 1) patient unable to understand or respond to oral or written information; 2) previously been enrolled in the study; and 3) do not resuscitate order in place.
Written informed consent was obtained from all patients, and the study protocol was approved by the Research Ethics Committees of the Capital Region of Denmark, file number H-4-2012-057, and by the Danish Data Protection Agency, file number 2007-58-006. The trial is registered in ClinicalTrials.gov with the identifier no NCT1950936.
The flow of patients is summarized in . Patients were allocated according to the random part of the civil registration number in Denmark (Central Person Register [CPR] number). Randomness of the used part was confirmed by the legal department of the Danish CPR-administration upon inquiry by the authors. The randomization algorithm was concealed to treating clinicians and patients. Patients eligible for participation were allocated to either the PCT-guided intervention arm (PCT-arm) or the control arm. Blinding of allocation arm was not possible post-randomization, because PCT measurements could not be blinded in a reasonable manner.
Figure 1 CONSORT diagram showing patient flow.
All patients assessed as AECOPD underwent chest X-ray and were treated with systemic corticosteroids (37.5 mg prednisolone once-a-day [qd] for 10 days) and inhaled bronchodilators (short-acting muscarinic antagonists and/or short-acting β2-agonists).
In the control arm, antibiotic therapy followed treatment strategies for AECOPD according to GOLD.Citation20
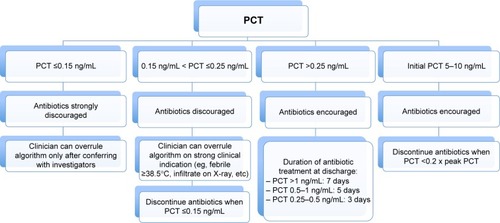
According to the PCT algorithm (), initiation or continuation of antibiotics was strongly discouraged if PCT was 0.15 ng/mL or lower and discouraged if levels were between 0.15 ng/mL and 0.25 ng/mL. Initiation or continuation of antibiotics was encouraged if PCT was >0.25 ng/mL. In patients with PCT over 5 ng/mL on admission, the algorithm recommended stopping antibiotics when PCT levels decreased by 80% of the peak value. Overruling of the PCT algorithm was possible by prespecified criteria, namely in case of respiratory or hemodynamic instability, infiltrate on chest X-ray, fever of ≥38.5°C, or after consulting with the ProToCOLD team. The reason for the latter was to achieve higher algorithm adherence among clinicians, however, giving the possibility to administer antibiotics in case of particular concern of the clinician despite low PCT values. The empiric first choice of antibiotic drug followed local guidelines in both groups, namely oral amoxicillin clavulanate in clinically stable patients and intravenous piperacillin/tazobactam in unstable patients. In case of allergy or intolerance, prescribed antibiotics were adapted. Similarly, antibiotics were adapted to antibiograms in case of relevant positive bacterial culture. The precise dose and regimen of the antibiotics (according to body mass index, renal function, liver function, etc) was left at the discretion of the treating clinicians.
Figure 2 PCT-guided antibiotic therapy – algorithm.
Blood samples for PCT measurements were collected within 24 hours of admission and on days 3, 5, and 7 of admission. CRP was routinely measured at admission, and subsequent measurements were left at the discretion of the treating clinicians, however mostly being measured once daily.
Per-protocol population
Per-protocol population (PPP) was defined as patients with confirmed AECOPD, not withdrawing from the study after enrollment, and being adherent to the treatment algorithm on day 1 of admission, in both arms, respectively. Treatment algorithm in the control arm was following GOLD treatment strategies for AECOPD,Citation20 furthermore consisted of antibiotic prescription in case of community-acquired pneumonia (CAP) and in patients with temperature of ≥38.5°C and/or CRP of ≥50 mg/L.
End points
The primary end point of this study was fraction of patients using antibiotics for ≥5 days within 28 days after inclusion, which was evaluated by overall antibiotic exposure. Secondary end points included 1) cumulative number of days with any antibiotic therapy within 28 days, 2) fraction of patients using antibiotics for a) ≥1 day, b) ≥3 days, c) ≥7 days, and finally 3) length of hospital stay and adverse events, which were evaluated by a composite end point of mortality, readmission, and intensive care unit admission, all within 28 days after inclusion. Mortality was not the primary end point, since the safety of PCT-guided antibiotic therapy in these patients has already been established in other studies.Citation17,Citation21
Data collection
POC PCT measurement required blood collection in lithium heparin tube, centrifugation at 3,900 rpm for 15 minutes, followed by fully automated analysis of 200 µL of plasma, using an enzyme-linked fluorescent assay system (mini VIDAS®; BioMérieux SA, Marcy d’Etoile, France) with a functional assay sensitivity of 0.09 ng/mL. Test kits contained all the required reagents. Assay time waŝ20 minutes, and results were routinely available within 1–2 hours. The equipment was placed at the Department of Respiratory Medicine (POC), and all measurements were performed by the department’s clinical staff after being properly trained.
Statistical analysis
Discrete variables are expressed as count (percentage), and continuous variables as median and interquartile range (IQR). Comparability of groups was analyzed by chi-square (χ2) test, two-sample t-test, and Mann–Whitney U-test, as appropriate. A P-value <0.05 was defined as significant. Data were analyzed using statistical software (SAS Version 9.1.3; SAS Institute Inc., Cary, NC, USA, PASW Version 18; Chicago, IL, USA, Excel 2010; Microsoft Corporation, Redmond, WA, USA, and SigmaPlot; Systat Software, Inc., San Jose, CA, USA).
Sample size calculation
Based on prior trials, we assumed that using a PCT-guided therapy algorithm in AECOPD could reduce antibiotic exposure by ~50%Citation18,Citation22 without influencing the proportion of adverse effects.Citation17,Citation21 A sample size of 60 patients in the PCT-arm and 60 in the control arm yielded a power of 0.80 to detect a significant difference using a two-tailed test with a 5% significance level.
Results
Baseline characteristics
Detailed baseline characteristics of the studied population are presented in . One-hundred and twenty patients were found eligible, of whom 62 were randomized to the PCT-arm and 58 to the control arm. Median age was 72 years (IQR 63–80), 39% were male. Ninety-six percent of the patients had a history of smoking with a median of 40 pack-years. Ninety-two percent of the patients had either a verified or a clinician’s diagnosis of COPD prior to enrollment in the study. Spirometry, either measured prior to hospitalization or at convalescence (ie, >6 weeks after discharge), showed severe airflow limitation (forced expiratory volume in 1 second 29%–53% predicted [IQR]), thus classified as high risk according to GOLD classification (classes C or D).Citation20 Spirometry could not be obtained from 12 patients (10%). Poor patient enrollment was due to busy emergency department at times.
Table 1 Baseline characteristics of the study population, overall and by randomization
Clinical findings and diagnoses
shows the details of clinical findings and diagnoses. Ninety-seven percent of the patients were diagnosed with AECOPD, and 25% of patients were additionally diagnosed with CAP, defined as the combination of infiltrate on X-ray interpreted by admitting clinician and CRP ≥50 mg/L.
Table 2 Clinical characteristics and final diagnoses of the study population, overall and by randomization
Median PCT in the intervention arm was 0.06 ng/mL, and median CRP was 42 mg/L in the PCT-arm vs 22 mg/L in the control arm.
Primary end point
Antibiotic exposure and prescription rates are presented in . Antibiotic exposure for ≥5 days was reduced from 67.2% to 41.9% of all patients (P=0.006) in the intention-to-treat (ITT) population and from 73.9% to 21.1% (P<0.0001) in the PPP. The relative risk in the PCT-arm to be exposed to antibiotics for ≥5 days was 0.62 (95% CI 0.44–0.88) in the ITT population. In the PPP, antibiotic prescription rate on day 5 was reduced from 100% to 54.5% (P=0.035) in the CAP-subgroup.
Table 3 Antibiotic exposure, antibiotic prescription rate, and length of hospital stay by randomization
Secondary end points
Results of secondary end points are presented in . The median duration of antibiotic exposure was 3.5 (IQR 0–10) days in the PCT group vs 8.5 (IQR 1–11) days in the control group (P=0.0169) for the ITT population.
In the PPP, the median number of days exposed to antibiotics was 0 (IQR 0–4) days in the PCT group vs 10 (IQR 5–12) days in the control group (P<0.0001).
The median duration of antibiotic treatment among patients with CAP in the PPP was 5 (IQR 2–9) days in the PCT group vs 10 (IQR 7–14) days for control patients (P=0.0143).
In the PPP group, the fraction of patients receiving antibiotics for 1 day, 3 days, 5 days, and 7 days was significantly reduced in the PCT group as compared with the control group. Similarly, for the ITT population, the fraction of patients on antibiotics on days 3, 5, and 7 was significantly smaller in the PCT group ( and ).
Figure 3 Antibiotic exposure in patients receiving antibiotic therapy, intention-to-treat.
Note: Red bars indicate primary endpoints of study.
Abbreviations: PCT, procalcitonin; d, days.
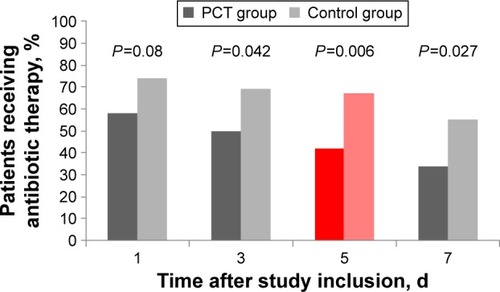
Figure 4 Antibiotic exposure in patients receiving antibiotic therapy, per-protocol population.
Abbreviations: PCT, procalcitonin; d, days.
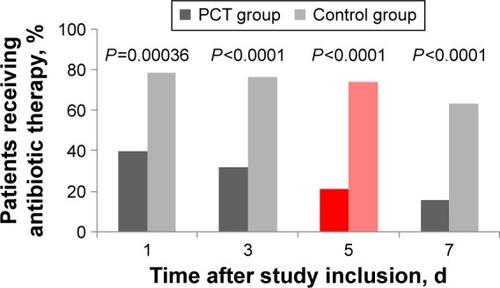
Initial prescription rate of antibiotics was reduced from 74% to 58% (P=0.08) in the ITT population and from 78% to 39% (P=0.0004) in the PPP. Length of hospital stay showed no significant differences between the groups.
addresses the adverse events. Here, we could not find significant differences, neither in the ITT nor in the PPP. Within 28 days after inclusion, two patients died in the control arm and one in the PCT-arm. For the latter, a 73-year-old woman, cause of death was respiratory arrest, 4 days after admission due to AECOPD. Chest X-ray assessment from the radiologist stated increased bronchovascular markings, suggesting either incipient pneumonia or exacerbation of chronic bronchitis. PCT at admission was 0.13 ng/mL and CRP was 55 mg/L, decreasing spontaneously to 0.1 ng/mL and 24 mg/L, respectively, on day 3, and no antibiotics were administered. In the control arm, one of the patients with fatal adverse events, a 66-year-old woman, showed not to have had AECOPD at admission and cause of death was multiple organ dysfunction syndrome as a consequence of septic shock in a patient with history of liver cirrhosis, 17 days after admission. The other patient, an 88-year-old woman, deceased 17 days after admission of acute respiratory failure as a consequence of AECOPD and pneumonia. The patient has been under broad-spectrum antibiotic therapy all 17 days.
Table 4 Rates of combined adverse outcomes and mortality by randomization group
Adherence with protocol algorithm
Total PPP consisted of 84 (70%) patients (). Thus, 38 patients (61%) in the PCT group followed PCT algorithm on first day of admission. Algorithm nonadherence was even more important the following days. For 14 patients (22.6%), antibiotic therapy was initiated in discordance with the algorithm criteria, based on the judgment of the treating clinician, nine of them showing an infiltrate on the chest X-ray. Two patients were treated with antibiotics for other reasons than AECOPD, namely urinary tract infection and oral candidiasis. Four patients withdrew consent after enrollment, and one patient did not meet inclusion criteria in terms of AECOPD. One patient did not follow algorithm due to transfer to another department, and two patients failed the algorithm due to other technical issues. In the control group, 46 patients (79%) were treated according to local guidelines.
Discussion
According to recent international treatment strategies, antibiotics play an important role in treating patients with COPD who experience a severe exacerbation.Citation20 Given that a majority of these exacerbations are apparently not due to bacterial infection and given that antibiotic resistance and side effects have become an ever-increasing problem in the past few decades, tools to reduce the antibiotic exposure are urgently needed.Citation3–Citation7 Several previously conducted randomized controlled trials showed reduction of antibiotic exposure in LRTIs when using a PCT-guided treatment algorithm.Citation17,Citation18,Citation21,Citation22 These studies were mainly conducted by a single Swiss research group, thus suggesting external validation.
Moreover, most of these studies used expensive, advanced PCT assays that require both expertise and experience and can therefore not easily be introduced in every day clinical practice.
Consequently, we wanted to investigate whether simple POC measurements of PCT combined with such an algorithm can guide respiratory physicians in treating AECOPD and hereby reduce the use of antibiotics. Our findings demonstrate that the PCT-guided strategy can reduce redundant antibiotic therapy in hospitalized patients, the fraction of patients receiving antibiotics for ≥5 days being reduced from 67% to 42% in the ITT population (ie, a reduction of 37%) and from 74% to 21% in the PPP (ie, a reduction of 72%). Hereby, the findings in our trial strengthen the evidence provided by the previous studies and demonstrate the effectiveness of PCT-guided antibiotic management in AECOPD. As initial PCT measurement was carried out within 24 hours after admission, PCT values were in many cases entailing either cessation or continuation of already initiated antibiotic treatment, thus explaining that antibiotic prescription rate at day 1 in the ITT population was not significantly smaller in the PCT-arm (74% vs 58%, P=0.08).
Furthermore, POC PCT measurements seem to be at least as efficient as standard assays and can be introduced in every day practice, also in departments where the local biochemistry laboratory cannot offer the test.
The main limitation of the study is the population size. A relatively small number of 120 patients was included. Nevertheless, the size was large enough to detect the difference in usage of antibiotics. As mentioned earlier, we were not able to detect differences in adverse outcomes with our sample size, but this was not the aim of our study, since the safety of PCT-guided antibiotic strategies in LRTIs has previously been demonstrated.Citation17,Citation18,Citation21,Citation22
Second, we observed algorithm nonadherence to a variable extent, and for 14 out of 62 patients in the PCT group, the algorithm was overruled the first day of admission, and antibiotic therapy was initiated anyway. Algorithm nonadherence was more important the following days, and even lower antibiotic prescription rates could be expected with higher algorithm adherence. However, in order to avoid possible undertreatment, decisions on prescription and discontinuation of antibiotics always have to take clinical observations into consideration,Citation23 as conducted in this protocolled pragmatic trial. This accounts for some algorithm nonadherence, together with the fact, that new algorithms can be challenging to implement in a busy department.
Since our study was designed and conducted as a pragmatic trial, comparable results can be expected in a real-life setting. Furthermore, POC measurement of PCT, although easy to master, showed to be challenging at times in a busy daily routine. On the other hand, POC PCT measurement and PCT-guided algorithm increased awareness and tended to force the clinician to take a stand on antibiotic prescription and discontinuation, thereby alone leading to lower antibiotic prescription rates in comparison to the control arm. It can be speculated, whether higher PCT algorithm adherence could be obtained in the future, when the confidence in PCT as a valid biomarker for bacterial infection in AECOPD is more prevalent among clinicians. Thus, conducting a similar study with a CRP-guided treatment algorithm, having the power to detect potential safety issues, would add valuable knowledge to this topic, since CRP is widely used as inflammatory marker.Citation24 Nevertheless, there are no controlled trials supporting CRP as a guide for antimicrobial therapy.Citation25
Conclusion
Our study shows that an antibiotic strategy algorithm based on POC measurement of PCT in patients admitted with AECOPD can reduce the overall use of antibiotics substantially, thus possibly containing the selection of resistant bacterial strains. Finally, cost-effectiveness of PCT-guided antibiotic therapy has been proven in another clinical setting.Citation26 It can be anticipated that the reduction of antibiotic exposure in patients admitted with AECOPD has the potential to reduce overall costs, although such calculations are difficult to conduct, since the economic implications of possibly reduced antibiotic resistance and side effects are hard to quantify. Given our results, we strongly suggest easier access to PCT measurements and the implementation of PCT-guided treatment algorithms in patients experiencing AECOPD. Moreover, POC PCT measurement may be a suitable option in environments where the physician’s attention and interest toward antibiotic reduction strategies is suboptimal, since the direct availability of the test seemed to increase awareness of this issue among treating physicians.
Acknowledgments
The ProToCOLD study group is most grateful to all the clinicians who recruited patients for the study. Especially, we want to thank nurse Pia Andersen, who coordinated PCT measurement and patient flow at the Department of Respiratory Medicine at Copenhagen University Hospital Bispebjerg. This work was supported by bioMérieux Denmark ApS, which provided both the automated immunoassay system (mini VIDAS®) and the assays used for POC PCT measurement during the study period. Thermo Fisher Scientific, MA, USA supported the running costs of the study with €2,000. BioMérieux and Thermo Fisher were neither involved in the study design, in the collection, analysis, and interpretation of data, and in the writing of the report nor in the decision to submit the article for publication.
Disclosure
Caspar Corti received an unrestricted grant of €2,000 by Thermo Fisher Scientific, MA, USA, and bioMérieux Denmark Aps supported the study non-financially. The authors report no other conflicts of interest in this work.
References
- RamFSFRodriguez-RoisinRGranados-NavarreteAGarcia-AymerichJBarnesNCAntibiotics for exacerbations of chronic obstructive pulmonary diseaseCochrane Database Syst Rev200622CD00440316625602
- QuonBSGanWQSinDDContemporary management of acute exacerbations of COPD: a systematic review and metaanalysisChest2008133375676618321904
- SeemungalTHarper-OwenRBhowmikARespiratory viruses, symptoms, and inflammatory markers in acute exacerbations and stable chronic obstructive pulmonary diseaseAm J Respir Crit Care Med200116491618162311719299
- RohdeGWiethegeABorgIRespiratory viruses in exacerbations of chronic obstructive pulmonary disease requiring hospitalisation: a case-control studyThorax2003581374212511718
- PapiABellettatoCMBraccioniFInfections and airway inflammation in chronic obstructive pulmonary disease severe exacerbationsAm J Respir Crit Care Med2006173101114112116484677
- SethiSEvansNGrantBJBMurphyTFNew strains of bacteria and exacerbations of chronic obstructive pulmonary diseaseN Engl J Med2002347746547112181400
- DrekonjaDMAmundsonWHDecarolisDDKuskowskiMALederleFAJohnsonJRAntimicrobial use and risk for recurrent Clostridium difficile infectionAm J Med2011124111081.e1e721944159
- SethiSMurphyTFBacterial infection in chronic obstructive pulmonary disease in 2000: a state-of-the-art reviewClin Microbiol Rev200114233636311292642
- StolzDTammMDiscriminate use of antibiotics for exacerbation of COPDCurr Opin Pulm Med200915212613219532027
- SethiSWronaCGrantBJBMurphyTFStrain-specific immune response to Haemophilus influenzae in chronic obstructive pulmonary diseaseAm J Respir Crit Care Med2004169444845314597486
- SchuetzPAminDNGreenwaldJLRole of procalcitonin in managing adult patients with respiratory tract infectionsChest201214141063107322474148
- AssicotMGendrelDCarsinHRaymondJGuilbaudJBohuonCHigh serum procalcitonin concentrations in patients with sepsis and infectionLancet199334188445155188094770
- ChirouzeCSchuhmacherHRabaudCLow serum procalcitonin level accurately predicts the absence of bacteremia in adult patients with acute feverClin Infect Dis200235215616112087521
- DandonaPNixDWilsonMFProcalcitonin increase after endotoxin injection in normal subjectsJ Clin Endocrinol Metab1994796160516087989463
- SimonLGauvinFAmreDKSaint-LouisPLacroixJSerum procalcitonin and C-reactive protein levels as markers of bacterial infection: a systematic review and meta-analysisClin Infect Dis200439220621715307030
- UzzanBCohenRNicolasPCucheratMPerretG-YProcalcitonin as a diagnostic test for sepsis in critically ill adults and after surgery or trauma: a systematic review and meta-analysisCrit Care Med20063471996200316715031
- SchuetzPChrist-CrainMThomannRProHOSP Study GroupEffect of procalcitonin-based guidelines vs standard guidelines on antibiotic use in lower respiratory tract infections: the ProHOSP randomized controlled trialJAMA2009302101059106619738090
- Christ-CrainMJaccard-StolzDBingisserREffect of procalcitonin-guided treatment on antibiotic use and outcome in lower respiratory tract infections: cluster-randomised, single-blinded intervention trialLancet2004363940960060714987884
- Christ-CrainMStolzDBingisserRProcalcitonin guidance of antibiotic therapy in community-acquired pneumoniaAm J Respir Crit Care Med20061741849316603606
- Global Initiative for Chronic Obstructive Lung Disease (GOLD) [homepage on the Internet]Global Strategy for the Diagnosis, Management and Prevention of COPD, 20152015 Available from: http://www.goldcopd.org/Accessed January 3, 2016
- SchuetzPMüllerBChrist-CrainMProcalcitonin to initiate or discontinue antibiotics in acute respiratory tract infectionsEvid Based Child Health2013841297137123877944
- StolzDChrist-CrainMBingisserRAntibiotic treatment of exacerbations of COPD: a randomized, controlled trial comparing procalcitonin-guidance with standard therapyChest2007131191917218551
- MüllerBHarbarthSStolzDDiagnostic and prognostic accuracy of clinical and laboratory parameters in community-acquired pneumoniaBMC Infect Dis2007711017335562
- PruchaMBellinganGZazulaRSepsis biomarkersClin Chim Acta20154409710325447700
- SchuetzPAlbrichWChrist-CrainMChastreJMuellerBProcalcitonin for guidance of antibiotic therapyExpert Rev Anti Infect Ther20108557558720455686
- DeliberatoROMarraARSanchesPRClinical and economic impact of procalcitonin to shorten antimicrobial therapy in septic patients with proven bacterial infection in an intensive care settingDiagn Microbiol Infect Dis201376326627123711530