
Abstract
Introduction
Chronic obstructive pulmonary disease (COPD) is recognized as a multisystemic inflammatory disease associated with extrapulmonary comorbidities, including respiratory muscle weakness and cardiovascular and cardiac autonomic regulation disorders. We investigated whether alterations in respiratory muscle strength (RMS) would affect cardiac autonomic modulation in COPD patients.
Methods
This study was a cross-sectional study done in ten COPD patients affected by moderate to very severe disease. The heart rate variability (HRV) signal was recorded using a Polar cardiofrequencimeter at rest in the sitting position (10 minutes) and during a respiratory sinus arrhythmia maneuver (RSA-M; 4 minutes). Linear analysis in the time and frequency domains and nonlinear analysis were performed on the recorded signals. RMS was assessed using a digital manometer, which provided the maximum inspiratory pressure (PImax) and the maximum expiratory pressure (PEmax).
Results
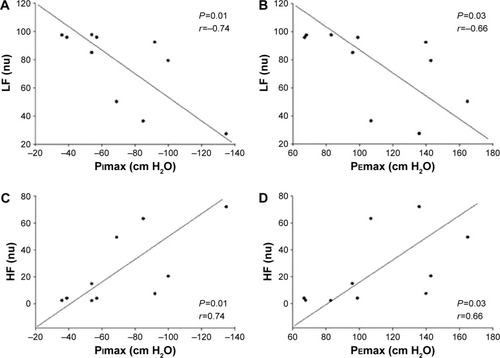
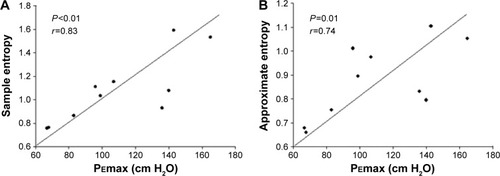
During the RSA-M, patients presented an HRV power increase in the low-frequency band (LFnu) (46.9±23.7 vs 75.8±27.2; P=0.01) and a decrease in the high-frequency band (HFnu) (52.8±23.5 vs 24.0±27.0; P=0.01) when compared to the resting condition. Significant associations were found between RMS and HRV spectral indices: PImax and LFnu (r=−0.74; P=0.01); PImax and HFnu (r=0.74; P=0.01); PEmax and LFnu (r=−0.66; P=0.01); PEmax and HFnu (r=0.66; P=0.03); between PEmax and sample entropy (r=0.83; P<0.01) and between PEmax and approximate entropy (r=0.74; P=0.01). Using a linear regression model, we found that PImax explained 44% of LFnu behavior during the RSA-M.
Conclusion
COPD patients with impaired RMS presented altered cardiac autonomic control, characterized by marked sympathetic modulation and a reduced parasympathetic response; reduced HRV complexity was observed during the RSA-M.
Introduction
Chronic obstructive pulmonary disease (COPD) is characterized by persistent and progressive airflow limitation resulting from abnormal inflammatory response of the airways and lungs to noxious particles inhalation.Citation1 Apart from inducing lung damage, COPD is recognized as a multisystemic inflammatory disease associated with extrapulmonary comorbidities that can substantially affect the disease prognosis.Citation1,Citation2 The prevalence of comorbidities in COPD patients ranges between 65% and 81%,Citation2 and they represent the primary causes of death in more than 60% of COPD patients.Citation3 Specifically, the prevalence of cardiovascular disorders in COPD patients is ~40%;Citation2 such disorders are directly associated with cardiac autonomic regulation.Citation4,Citation5
The integration of the cardiovascular, respiratory, and muscular systems constitutes a complex and sophisticated mechanism of energy generationCitation6 in which the cardiovascular system activity, aiming at organic homeostasis preservation, is controlled by the autonomous nervous system (ANS).Citation7 However, cardiorespiratory disorders, such as COPD, can induce changes in the sympathovagal balance, which can result in detrimental alterations in the ANS functioning of these patients.Citation5 The heart rate variability (HRV) analysis is an important tool for the assessment of the ANS behavior,Citation8 used to determine pathological conditions and investigate physiological modifications, which can be associated with physical exercise performance.Citation6,Citation8
Reduced HRV is associated with increased morbidity and mortality in COPD patients,Citation4,Citation5 and this has led various researchers to investigate the ANS behavior during respiratory maneuvers, position changes, and pharmacological blockade.Citation9 It is widely known that in COPD patients the HRV is reduced, and postural adjustments, which induce a predominantly sympathetic stimulation, are also impaired. However, the number of studies that evaluated the parasympathetic component is scarce.Citation10
The heart rate (HR) follows an oscillatory pattern synchronized with the respiratory cycle; this phenomenon is known as respiratory sinus arrhythmia (RSA). During inspiration, HR increases mainly due to the vagal withdrawal effect on the sinus node, while, during expiration, parasympathetic activity is regulated and HR decreases. RSA significantly decreases the sympathovagal balance, markedly increasing vagal modulation on the sinus node.Citation11
Recent studies investigated the relationship between respiratory muscle strength (RMS) and HRV in COPD patients and showed that respiratory muscle weakness can modify the HRV. However, this alteration still needs to be quantified; this could lead to an improvement of therapeutic treatment in pulmonary rehabilitation programs.Citation12,Citation13 Starting from this evidence, we investigated if alterations in RMS may affect cardiac autonomic modulation in COPD patients. We hypothesized that respiratory muscle weakness negatively affects HRV at rest and during an RSA maneuver (RSA-M) in COPD patients.
Methods
Study design
We performed a cross-sectional case study on a convenience nonprobability sample; the study was conducted within Santa Cruz Hospital’s Pulmonary Rehabilitation Program (Santa Cruz do Sul, RS, Brazil). The study was approved by the Research Ethics Committee of the University of Santa Cruz do Sul, protocol number 1.100.926, and all volunteers signed an informed consent statement prior to participation.
Subjects
Ten patients with a clinical diagnosis of COPD, confirmed by pulmonary function test, participating in a pulmonary rehabilitation program and without disease exacerbation for at least 30 days were included in the study. Patients with complex cardiac arrhythmias, unstable angina, uncontrolled systemic arterial hypertension, or myocardial ischemia were excluded from the study.
Measurements
Patients were evaluated in a laboratory at a temperature of 22°C and relative humidity between 50% and 60%. They were instructed to avoid stimulants and alcoholic drinks and not to perform exhausting physical exercise the day before the test; they were also instructed not to smoke or use bronchodilators for 6 hours before the test. Baseline variables, including systolic arterial pressure, diastolic arterial pressure, HR, respiratory frequency, and peripheral oxygen saturation, were measured. Clinical data including sex, age, body mass index, ethnicity, COPD stage,Citation3 and smoking status were also collected.
Pulmonary function
Pulmonary function was assessed using a digital spirometer (Microloop®, MK8, Care Fusion, Hoechberg, Germany), which provided measures of the slow vital capacity, the forced vital capacity (FVC), the forced expiratory volume in 1 second (FEV1), and the FEV1/FVC ratio. Spirometry was performed according to the recommendations of the American Thoracic Society,Citation14 and the results were analyzed according to the values predicted by Pereira et al.Citation15 The classification of severity of airflow limitation in COPD was performed according to the Global Initiative for Chronic Obstructive Lung Disease (GOLD) recommendationsCitation1 and patients were classified as moderate (GOLD II), severe (GOLD III), or very severe (GOLD IV).
Respiratory muscle strength
RMS was assessed using a digital manometer (MDI®, MVD300, Porto Alegre, Brazil), which provided measures of the maximum inspiratory pressure (PImax) and the maximum expiratory pressure (PEmax). The assessment was performed according to the recommendations for the Brazilian population. The PImax followed by PEmax was obtained from residual volume and total lung capacity; during the maneuver, the subjects remained seated, wearing nose clips and with a rigid, plastic flanged mouthpiece in place.Citation16 The values were then compared with those described in literature and expressed as percentage of predicted values.Citation16
Heart rate variability
HR and RR intervals were recorded using a telemetric cardiac monitor (Polar® S810i, Kempele, Finland) at rest (10 minutes) and during an RSA-M (4 minutes). Recorded signals contained at least 256 points.Citation17 An elastic band (Polar T31 transmissor) was placed around the patient’s thorax at the level of the lower third of the sternum while the patient was in sitting position, and signals were continuously transmitted to the receiving unit by an electromagnetic field. Recorded data were then transferred to the Kubios HRV® analysis software (version 2.2, Matlab Kuopio, Finland) for subsequent analysis.
For HRV recording during the RSA-M, subjects were instructed to perform a series of deep and slow inspirations and expirations, with a pulmonary volume that varied from the total lung capacity (maximal inspiration) to the residual volume (maximal expiration); each respiratory cycle was performed in 10 seconds, with a 5-second inspiration and a 5-second expiration, resulting in five to six respiratory cycles per minute.Citation18
Frequency domain, time domain, and nonlinear analysis were performed on signals recorded at rest and during the RSA-M. Time domain analysis provided mean RR, standard deviation (SD) RR, mean HR, SD HR, the square root of the mean-squared differences of successive HR and RR intervals, and the RR tri-index. Spectral analysis provided the HRV signal power in the low-frequency (LF) and in the high-frequency (HF) bands, expressed in normalized units (nu), and the LF/HF ratio. Nonlinear analysis provided the approximate entropy (ApEn) and the sample entropy (SampEn) indices.
Statistical analysis
Data were analyzed using the Sigmaplot® statistical package (version 11.0, Systat Software Inc., San Jose, CA, USA). The results were analyzed for normality through the Shapiro–Wilk test and presented descriptively as mean and standard deviation (parametric) or as median and minimum and maximum interval (nonparametric). To reject the null hypothesis, the Student’s t-test was used for parametric data and the Mann–Whitney test was used for nonparametric data. Spearman’s correlation analysis was performed to investigate the correlations between variables. A linear regression model was used to determine the RMS effect on the HRV. Residuals were evaluated under the assumptions of normality, constant variance, and independence. P≤0.05 was considered significant.
Results
A total of 12 COPD patients were recruited; two patients who presented arrhythmias were excluded during the screening phase. Clinical characteristics of patients included in the study are listed in . Data are in line with others found in literature, with the exception of the number of COPD patients with obesity.
Table 1 COPD patients’ clinical characteristics
Spectral and complexity HRV indices were significantly different between the resting condition and the RSA-M (). Our results showed that the RSA-M did not modify the time domain of HRV parameters (P>0.05). However, in the frequency domain, interestingly, the LF power and the LF/HF ratio increased (P=0.01), while the HF power decreased (P=0.01). This behavior suggests a sympathovagal modulation contrary to what is expected during the RSA-M. Moreover, ApEn and SampEn significantly decreased, indicating an HRV complexity decrease during the RSA-M.
Table 2 HRV indices at rest and during the RSA maneuver
shows the correlations between RMS and HRV. Moderate-to-strong correlations were found between PImax and spectral HRV index and between PEmax and spectral HRV index during the RSA-M (P<0.05).
Figure 1 Moderate-to-strong correlations were found between PImax and PEmax, and spectral HRV indices during the RSA-M.
Abbreviations: HRV, heart rate variability; RSA-M, respiratory sinus arrhythmia maneuver; HF, power in the high-frequency band; LF, power in the low-frequency band; PImax, maximum inspiratory pressure; PEmax, maximum expiratory pressure; nu, normalized units; cm H2O, centimeters of water.
Strong correlations were also observed between HRV complexity indices (ApEn and SampEn) and PEmax during the RSA-M, as shown in . A simple linear regression model was applied and the results are listed in . We found that, during the RSA-M, isolated PImax explained 44% of LFnu behavior.
Table 3 Linear regression analysis to predict LF from PImax, during the RSA-M
Figure 2 Strong correlations were also observed between HRV complexity indices (ApEn and SampEn) and PEmax during the RSA-M.
Abbreviations: HRV, heart rate variability; RSA-M, respiratory sinus arrhythmia maneuver; PEmax, maximum expiratory pressure; SampEn, sample entropy; ApEn, approximate entropy; cm H2O, centimeters of water.
Discussion
The primary finding of this study was that patients affected with COPD presented increased parasympathetic activity at rest in the sitting position when compared to the RSA-M. However, during the RSA-M, COPD patients presented enhanced sympathetic response and reduced parasympathetic tone, with an HRV complexity reduction. Finally, moderate-to-strong correlations were observed between RMS and spectral HRV index and between RMS and nonlinear HRV index. Our findings are relevant to understand COPD effects on HR autonomic modulation and their relationship with impaired RMS.
In this study, we observed marked parasympathetic modulation in COPD patients at rest. This is in line with literature findings and has been previously explained by the FEV1 reduction and the bronchoconstriction increase, which are characteristic in these patients.Citation19 However, the RSA-M induces a stimulation of the ANS,Citation15 as it is a maneuver able to elicit a parasympathetic response. We observed that patients presented a response contrary to what was expected during the parasympathetic accentuation maneuver. Our results are in line with those by Reis et al,Citation18 who observed increased sympathetic activation and reduced parasympathetic response. Controlled breathing could possibly accentuate pulmonary hyperinflation, which is already present in these patients as a result of chronic airways obstruction.Citation10,Citation18
Novel results were obtained in this study regarding the ANS complexity, assessed through HRV nonlinear indices SampEn and ApEn; complexity was found to be reduced during the RSA-M when compared to resting conditions. Literature results show that COPD patients present reduced ANS complexity when compared with healthy subjects.Citation20 In this line of evidence, Mazzuco et alCitation9 observed that the RSA-M, when compared with other autonomic tests that predominantly stimulate the sympathetic drive, was able to better evidence the impairments caused by the disease. This can be explained by the fact that parasympathetic modulation is more impaired in these patients due to air trapping and gas-exchange disturbances.Citation9
Moderate-to-strong correlations were observed in this study between RMS (PImax and PEmax) and spectral and nonlinear HRV indices; moreover, isolated PImax was found to be able to explain 44% of LF power behavior. Respiratory muscle weakness influences the phrenic dynamics and the expired air volume, with a functional residual capacity increase. Thus, it could be responsible for the alteration of the cardiac autonomic control response.Citation12 Therefore, we can assume that impaired RMS can substantially influence the RSA-M effect and the HRV behavior and that inspiratory muscle weakness can determine greater vagal attenuation in COPD patients. It is known that respiratory muscle weakness leads to fast and shallow breathing and that diaphragmatic incursion is limited by pulmonary hyperinflation. Thus, the ergoreceptor may be activated early and may be responsible for the fast central response in cardiac autonomic control.Citation12 A similar result was obtained between respiratory muscle weakness and reduced HRV in chronic heart failure patients.Citation11 Based on the result of this study, we propose an equation for LF prediction during the RSA-M: LF during the RSA-M =120.71–(0.623× PImax).
This study does possess limitations that deserve to be mentioned. Because of rigid exclusion criteria and the selection of patients with more than 95% of sinus beats, our sample is not fully representative of the entire COPD population, which is known to include patients with arrhythmias that compromise data recording and analysis. Moreover, only patients with GOLD stage II or higher COPD stage were included in the study; however, patients in the early stages of the disease could have a lower impact of the disease on cardiac autonomic control. In this study, we evaluated a relatively small cohort of COPD patients. Interestingly, most of the previous studies enrolled similar numbers of patients,Citation5,Citation9–Citation12 whereas few studies analyzed larger cohorts of patients.Citation18–Citation20 Another limitation of this work consists of the fact that underlying inflammation was not evaluated and that sarcopenia was not quantified. Such analyses could contribute to a better understanding of the mechanisms involved in mechanoneurological control, such as flow and blood oxygenation reduction, both in the brain and in the peripheral muscles.Citation21 Therefore, studies with greater, heterogeneous samples, including more comprehensive investigations, are needed.
This study bears great significance and importance for the clinical management of COPD patients. The novel results hereby presented about RMS in COPD patients might lead to an effective improvement in pulmonary rehabilitation in a clinical setting. Respiratory muscle training, potential clinical routine use of controlled breathing pattern in COPD patients during pulmonary rehabilitation, and any adverse effects on cardiopulmonary dynamics need further investigation in future studies.
Conclusion
In conclusion, patients affected by COPD presented in creased parasympathetic activity and ANS complexity at rest in the sitting position when compared to the RSA-M. This suggests an autonomic modulation alteration in basal conditions. During the RSA-M, a marked sympathetic modulation and a reduced parasympathetic response, with an HRV complexity reduction, were induced. Finally, RMS was found to be strongly associated with the sympathovagal response in COPD patients. These findings are relevant to understanding of COPD effects on HR autonomic modulation, and this is important to elucidate pathobiological mechanisms linking COPD to its comorbidities.
Author contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Acknowledgments
This study was funded by the University of Santa Cruz do Sul – UNISC, Santa Cruz Hospital and DECIT/SCTIE-MS/FAPERGS/CNPq 1264-2551/13-1. FAPESP (n 2013/23013-0).
Disclosure
The authors report no conflicts of interest in this work.
References
- Global Initiative for Chronic Obstructive Lung DiseasePocket Guide to COPD Diagnosis, Management and PreventionGlobal Initiative for Chronic Obstructive Lung Disease2015 Available from: http://www.goldcopd.it/materiale/2015/GOLD_Pocket_2015.pdfAccessed October 27, 2015
- Dal NegroRWBonadimanLTurcoPPrevalence of different comorbidities in COPD patients by gender and GOLD stageMultidiscip Respir Med20151012426246895
- DivoMCoteCTorresJPComorbidities and risk of mortality in patients with chronic obstructive pulmonary diseaseAm J Respir Crit Care Med2012186215516122561964
- RoqueALValentiVEMassettiTChronic obstructive pulmonary disease and heart rate variability: a literature updateInt Arch of Med201474325945125
- NicolinoJRamosDLeiteMRAnalysis of autonomic modulation after an acute session of resistance exercise at different intensities in chronic obstructive pulmonary disease patientsInt J Chron Obstruct Pulmon Dis20151022322925673982
- CarusoFCRReisMSSiqueiraACBGardimMCataiAMBorghi-SilvaADetermining anaerobic threshold through heart rate variability in patients with COPD during cycloergometer exerciseFisioter Mov2012254717725
- PaschoalMAPetrelluzziKFSGonçalvesNVOStudy of heart rate varability in patients with chronic obstructive pulmonary diseaseRev Ciênc Méd20021112737
- AbreuLCHeart rate variability as a functional marker of developmentJ Hum Growth Dev2012223279282
- MazzucoAMedeirosWMSperlingMPRRelationship between linear and nonlinear dynamics of heart rate and impairment of lung function in COPD patientsInt J Chron Obstruct Pulmon Dis2015101651166126316739
- PantoniCBFReisMSMartinsLEBCataiAMCostaDBorghi-SilvaAStudy on autonomic heart rate modulation at rest among elderly patients with chronic obstructive pulmonary diseaseRev Bras Fisioter20071113541
- ReisMSArenaRArchizaBToledoCFCataiAMBorghi-SilvaADeep breathing heart rate variability is associated with inspiratory muscle weakness in chronic heart failurePhysiother Res Int2014191162424039021
- ReisMSArenaRDeusAPSimõesRPCataiAMBorghi-SilvaADeep breathing heart rate variability is associated with respiratory muscle weakness in patients with chronic obstructive pulmonary diseaseClinics201065436937520454493
- ReisMSSampaioLMLacerdaDAcute effects of different levels of continuous positive airway pressure on cardiac autonomic modulation in chronic heart failure and chronic obstructive pulmonar diseaseArch Med Sci20106571972722419931
- GibsonGJWhitelawWSiafakasNTests of overall respiratory function. ATS/ERS statement on respiratory muscle testingAm J Respir Crit Care Med20021664521526
- PereiraCACSatoTRodriguesSCNew reference values for forced spirometry in white adults in BrazilJ Bras Pneumol200733439740617982531
- NederJAAndreoniSCastelo-FilhoANeryLEReference values for lung function tests. I. Static volumesBraz J Med Biol Res19993270371710412549
- Heart rate variability: standards of measurement, physiological interpretation, and clinical useTask Force of European Society of Cardiology and the North American Society of Pacing ElectrophysiologyEur Heart J1996173543818737210
- ReisMSAnaPRodrigoPAnicetoIAVCataiAMBorghi-silvaAAutonomic control of heart rate in patients with chronic cardiorespiratory disease and in healthy participants at rest and during a respiratory sinus arrhythmia maneuverRev Bras Fisioter201014210611320464168
- CarvalhoTDPastreCMAbreuLC DeMarquesLCFractal correlation property of heart rate variability in chronic obstructive pulmonary diseaseInt J Chron Obstruct Pulmon Dis20116232821311690
- ChengSTWuYKYangMCPulmonary rehabilitation improves heart rate variability at peak exercise, exercise capacity and health-related quality of life in chronic obstructive pulmonary diseaseHeart Lung201443324925524685394
- OliveiraMFZeltJTJonesJHDoes impaired O2 delivery during exercise accentuate central and peripheral fatigue in patients with coexistent COPD-CHF?Front Physiol2015551425610401