
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
TRPM8 plays a key role in COPD. The development of pulmonary hypertension (PH) in COPD adversely affects survival and exercise capacity. Thus, the aim of this study was to evaluate the possible association between single nucleotide polymorphisms (SNPs) in TRPM8 and COPD or PH in COPD among the Chinese Han population. A total of 513 COPD patients and 506 controls were enrolled in the study. Six tag SNPs (tSNPs) were genotyped. The relationship between COPD or PH in COPD and the six tSNPs was evaluated using the χ2 test and genetic model analysis. In the rs9789398 polymorphism, the T/C genotype was associated with an increased risk for COPD (P=0.005). Under the assumption of models of inheritance, there was an association between the rs9789398 polymorphism and COPD. In the rs9789675 polymorphism, the G/A genotype was associated with an increased risk for COPD (P=0.021). Furthermore, by the χ2 test, we found that the minor allele “A” of rs9789675 (odds ratio [OR] =0.63, 95% confidence interval [CI], 0.42–0.97, P=0.034) and the minor allele “C” of rs9789398 (OR =1.59, 95% CI, 1.03–2.44, P=0.034) were associated with a decreased risk of PH in COPD in allele models. In genetic models, the genotypes “GA” and “AA” of rs9789675 were associated with a decreased risk of PH in COPD. The genotypes “TC” and “CC” of rs9789398 were associated with a decreased risk of PH in COPD. Moreover, “CG” of rs1004478 was significantly associated with a decreased risk of PH in COPD. There was a significant association between the five SNPs (rs2362290, rs9789675, rs9789398, rs1003540, and rs104478) in the TRPM8 gene and the risk of PH in COPD. Our findings indicated that rs9789398 in the TRPM8 gene was significantly associated with the risk of COPD in the Chinese Han population. Moreover, rs9789675, rs9789398, and rs1004478 were significantly associated with the risk of PH in COPD. This study provides a novel insight into COPD and PH in the development of COPD.
Introduction
COPD is one of the leading causes of morbidity and mortality worldwide and is characterized by a partially reversible airflow limitation. Usually, when exposed to noxious particles or gases, COPD is progressive and associated with abnormal inflammatory responses of the lungs.Citation1–Citation4 Based on data from the World Health Organization, COPD may become the fourth leading cause of death by 2020,Citation5–Citation8 and in China, ∼9%–10% of adult patients and 8.2% of patients in the age group of 40 years would develop COPD.Citation9,Citation10
Recently, cigarette smoking is recognized as the major risk factor for COPD. However, only 10%–15% of smokers develop clinically significant COPD.Citation11–Citation14 The role of genetic factors in the development of COPD has been investigated by many studies such as family studies and hypothesis-free genome-wide association (GWA) studies,Citation15,Citation16 although the underlying COPD pathogenesis based on the molecular genetics is not well understood. Currently, many studies put forward that COPD is associated with both genetic and environmental factors. Based on the WHO classification, pulmonary hypertension (PH) is associated with lung diseases and/or hypoxemia.Citation17 It has been reported that 5%–40% of COPD patients who underwent right heart catheterization (RHC) might develop an elevation of pulmonary arterial pressure.Citation18 In addition, pulmonary arterial pressure is demonstrated as an important prognostic indicator for COPD.Citation19
Transient receptor potential cation channel subfamily M member 8 (TRPM8) is activated by a temperature range of 8°C–22°C, which could evoke a sensation of coolness.Citation20 Thus, respiratory autonomic responses might be introduced by breathing cold air, including airway constriction, cough, and mucosal secretion, which trigger an asthma attack or indeed exacerbate preexisting disease,Citation21 such as COPD. Therefore, the aim of the current study was to investigate the potential relationship between single nucleotide polymorphisms (SNPs) in the TRPM8 gene and COPD or PH in COPD among the Chinese Han population.
Subjects and methods
Study participants
A total of 513 subjects diagnosed with COPD from the southern part of China were recruited (81 females, 432 males; median age, 68.02 years). COPD was diagnosed based on the criteria of the National Heart, Lung and Blood Institute (NHLBI)/WHO Global initiative for chronic Obstructive Lung Disease (GOLD).Citation22 Patients with post-bronchodilator (BD) forced expiratory volume in 1 second (FEV1, 80% predicted) and FEV1/forced vital capacity (FVC, 0.7) were enrolled in the study. Patients were excluded from the study if they had other significant respiratory diseases, such as lung cancer, pulmonary tuberculosis, cystic fibrosis, and bronchial asthma.
PH was diagnosed by transthoracic Doppler echocardiography (TTE). The entry criteria for PH in COPD cases were tricuspid regurgitant (TR) velocity ≥2.8–2.9 m/sec and pulmonary artery systolic pressure (PASP) ≥40 mmHg. In our study, the patients diagnosed with COPD were divided into two groups according to the TTE: group 1, COPD with PH (24 females, 126 males; median age, 70.03 years), and group 2, COPD without PH (57 females, 363 males; median age, 67.19 years).
In addition, 506 healthy individuals were enrolled (92 females, 414 males; median age, 56.49 years) as a control group. All participants were from Han population of the southern part of China.
Spirometry and calculated method
COPD was defined as a post-BD FEV1/FVC ratio of 0.7 in patients aged ≥40 years, according to the GOLD guideline. Percentages of the predicted values were used to show the spirometry results. In addition, the results were calculated based on Morris’s predictive equations as follows (height in inches):
TTE and the calculated method
PH was defined by RHC showing precapillary PH with a mean pulmonary artery pressure of >25 mmHg and a normal pulmonary artery wedge pressure of <15 mmHg.Citation23,Citation24 RHC was recognized as a standard criteria for the diagnosis of PH, which could provide more accurate pulmonary vascular resistance and pulmonary arterial hypertension. When the pulmonary outflow was obstructed, TTE could provide an estimate of the right ventricular systolic pressure (RVSP), as the value was equivalent to the systolic pulmonary arterial pressure. Based on the velocity of TR jet, the RVSP and pulmonary arterial pressure can be calculated. The velocity of the TR jet can be used to calculate the RVSP using the simplified Bernoulli equation:
Demographic and clinical data
A standardized epidemiological questionnaire was designed to collect the demographic and personal data, and the information such as personal details (age, sex, ethnicity, and residential region), diet habit, smoking history, and family history of COPD was included.
Written informed consent was provided by all participants in the study. The study was approved by the ethics committee of the First Affiliated Hospital of Guangzhou Medical University. Approximately 5 mL of peripheral blood was taken from each subject.
Selection and genotyping of tag SNPs (tSNPs)
SNPs were selected from the regulatory region of TRPM8 gene which were from the coding regions within 3,000 bp. SNPs with minor allele frequency (MAF) >5% in the HapMap Chinese Han Beijing population were selected. tSNPs were selected based on the linkage disequilibrium (LD) analysis of 45 samples from controls. The methods for sequencing and SNP annotation were as follows: genomic DNA was extracted from whole blood using the QIAamp DNA Blood Mini Kit (QIAGEN Co. Ltd., Düsseldorf, Germany). DNA concentration was measured using a NanoDrop 2000 (Thermo Scientific, Fitchburg, WI, USA). tSNPs were genotyped with the SNPseq assay, an efficient multiple gene region enrichment/next-generation sequencing-based assay for SNP genotyping by Genesky Biotechnologies, Inc. (Shanghai, China). Briefly, segments of DNA containing tSNPs were amplified using the EasyTarget™ Amplification Kit (Genesky Biotechnologies, Inc.), which was developed using cycled primer extension and ligation-dependent amplification (CPELA). The CPELA method has been described as a fast and simple method for multiple gene region enrichment for massively parallel sequencing.Citation27 Next-generation sequencing of the amplification products was carried out by HiSeq 2000 Sequencer (Illumina, Inc., San Diego, CA, USA) following the manufacturer’s standard sequencing protocols. Output sequence data were trimmed and then compared with fragment reference sequences (hg19) using the Blat program.Citation28 Burrows- Wheeler Aligner (BWA, v0.7.5a) was used to map the reads,Citation29 followed by Sequence Alignment/Map (SAM)-to-BAM conversion, sorting, and removal of duplicates using SAM tools (v0.1.19).Citation30,Citation31 Combined SNP calling was performed on the resulting BAM files using Genome Analysis Toolkit (GATK) and Varscan programs.Citation32 The Annovar program was used for SNP annotation.Citation33
Statistical analysis
Quantitative data were shown as median ± standard deviation. Student’s t-test was used to compare the differences of quantitative data, and χ2 test was applied for qualitative data comparison. Deviation from Hardy–Weinberg equilibrium (HWE) of genotypic distribution of each SNP in controls was analyzed using Fisher’s exact test. When P>0.05, we defined that the population were in genetic balance. The population would not be suitable for enrolling in the study as control if P<0.05. In addition, the Pearson’s χ2 and Fisher’s exact tests were used to calculate the allele frequencies of cases and controls, and MAF in controls was defined as baseline. After adjusting for age, sex, and smoking status, odds ratios (ORs) and 95% confidence interval (95% CI) were calculated using unconditional logistic regression analysis.Citation34 The relationship between the selected SNPs and the risk of COPD was calculated using genotypic model analysis (codominant, dominant, recessive, overdominant, and log additive) by the website software program SNPStats.Citation35 The analyses, including LD, haplotype construction, and genetic association at polymorphism loci, were performed using the Haploview software package (version 4.2) and SHEsis software platform22. In the LD analysis, pairwise distance among SNPs >500 kb was ignored. D′ value was used to evaluate the LD for each pair of SNPs, and variants with the red square indicated that the two related sites were in complete LD (D′=1). D′ value equaling to 0.8 indicated that the related tSNPs formed one block.Citation36,Citation37 Haplotypes were constructed using SNPs in the same LD block, and haplotype frequency of >0.05 was selected. Finally, one SNP in TRPM8 from each LD block was selected for the research.
Statistical analyses were performed using Microsoft Excel (Microsoft Corporation, Redmond, WA, USA) and SPSS 19.0 statistical package (IBM Corporation, Armonk, NY, USA). In the study, all the P-values were two-sided, and P<0.05 was defined as statistically significant.
Results
The characteristics of the enrolled patients are given in . A total of 531 COPD patients from the southern part of China were enrolled in the study, including 150 individuals with PH, and 506 healthy sex-matched volunteers were enrolled in the control group. No significant differences were found between the COPD and control groups in terms of sex (P=0.3128) or body mass index (BMI; P=0.575). However, COPD patients were significantly older than healthy controls (68.02±11.21 years vs 56.49±9.43 years, P<0.001). Patients with COPD had longer average smoking exposure (43.08 vs 39.45 pack-years, P<0.001) and significantly worse lung functions as compared with control subjects in terms of the predicted FEV1% (36.77% vs 95.77%, P<0.001) and FEV1/FVC ratio (0.43 vs 0.81, P<0.001).
Table 1 Characteristics and grouping of the study population
Patients with COPD were divided into two groups based on the PASP value: COPD with PH and COPD without PH. For the group with PH in COPD, there were no significant differences in age, sex, BMI, and smoking status (P=0.190, 1.000, 0.051, and 0.467, respectively). Moreover, the two groups exhibited significantly different PASP values (49.64 vs 25.37, P<0.001) and FEV1/FVC (P=0.004).
Association of TRPM8 SNPs with risk of COPD
summarizes the basic characteristics of the SNPs in the study population and shows that all the five SNPs from controls were in HWE (P>0.05). The differences in frequency distributions of alleles between cases and controls compared by Pearson’s χ2 test showed that the minor allele “C” of rs9789398 from TRPM8 was significantly associated with the risk of COPD in the study population (P=0.040, OR =1.33, 95% CI =1.01–1.74).
Table 2 Basic characteristics of SNPs in the enrolled population
Comparing the possession of minor allele, it has been hypothesized that harboring the minor allele of each SNP was a risk factor. shows the relationship between SNPs and the risk of COPD under various genetic models. Our analyses showed that crude analysis of rs9789398 was associated with an increased risk of COPD under the dominant model (P=0.024, OR =1.41, 95% CI =1.05–1.90), the overdominant model (P=0.021, OR =1.43, 95% CI =1.05–1.94), and log-additive model (P=0.037, OR =1.34, 95% CI =1.02–1.77). However, after adjusting for age, sex, and smoking status, no significant relationship was observed between rs9789398 and the risk of COPD under any different genotypic models.
Table 3 Association between rs9789398 genotypes and the risk of COPD
Association between COPD and smoking status was well documented. A smoking status stratification analysis was performed to eliminate potential confounding effects caused by differences in smoking history. As shown in , there was no significant association between SNPs and the risk of COPD in nonsmokers (n=247) or former smokers (n=454). However, SNP analysis among samples from current smokers (n=318) showed that the rs9789675 and rs9789398 polymorphisms were significantly associated with the risk of COPD after adjusting for age, sex, and pack-years. In the rs9789675 polymorphism, the GA genotype was associated with an increased risk of COPD (P=0.021). Under the assumption of models of inheritance, the rs9789675 polymorphism was significantly related to the risk of COPD (the dominant model: GA + AA vs GG: OR =2.00, 95% CI =1.08–3.72, P=0.026; the overdominant model: GA vs GG–AA: OR =1.94, 95% CI =1.02–3.67, P=0.04). Moreover, it was shown that the rs9789398 polymorphism was associated with the risk of COPD (the codominant model: TT vs TC vs CC: OR =2.48, 95% CI =1.25–4.93, P=0.022; the dominant model: TC–CC vs TT: OR =2.48, 95% CI =1.28–4.77, P=0.0057; the overdominant model: TC vs TT–CC: OR =2.43, 95% CI =1.23–4.80, P=0.0092). The TC genotype was associated with an increased risk of COPD (P=0.005).
Table 4 Association between TRPM8 and COPD by smoking status: stratified analysis
Based on haplotype analyses, rs2362290, rs9789675, rs9789398, rs1003540, and rs1004478 were in complete LD. However, no significant association between the selected haplotype and the risk of COPD was found.
Association of the TRPM8 SNPs with the risk of PH in COPD
also shows the MAF of all SNPs genotyped in the COPD with PH group. HWE test revealed that the genotypic distribution of all SNPs conformed to HWE in the control group (P>0.05). Using the χ2 test, two SNPs (rs9789675 and rs9789398) were significantly associated with the risk of PH among COPD patients (OR =0.63, 95% CI, 0.42–0.97, P=0.034 and OR =1.59, 95% CI, 1.03–2.44, P=0.034, respectively).
As shown in , crude analysis revealed that the genotypes “GA” and “AA” of rs9789675 were associated with a decreased risk of PH in COPD under the dominant model (P=0.036, OR =0.62, 95% CI =0.39–0.98), the dominant model (P=0.013, OR =0.40, 95% CI =0.19–0.88), and the log-additive model (P=0.027, OR =0.62, 95% CI =0.23–0.97). “TC” and “CC” of rs9789398 were associated with a decreased risk of PH in COPD under the dominant model (P=0.027, OR =0.60, 95% CI =0.37–0.95), the overdominant model (P=0.04, OR =0.47, 95% CI =0.05–4.05), and log-additive model (P=0.026, OR =0.61, 95% CI =0.39–0.95). In addition, “CG” of rs1004478 was also significantly associated with a decreased risk of PH in COPD under the codominant model (P=0.048, OR =0.60, 95% CI =0.40–0.91), the dominant model (P=0.036, OR =0.66, 95% CI =0.45–0.97), and overdominant model (P=0.015, OR =0.61, 95% CI =0.41–0.91). After adjusting for sex, age, and smoking status, these three SNPs also showed a significant association with the risk of PH in COPD.
Table 5 Association between genotypes (rs9789675, rs9789398, and rs1004478) and the risk of PH in COPD
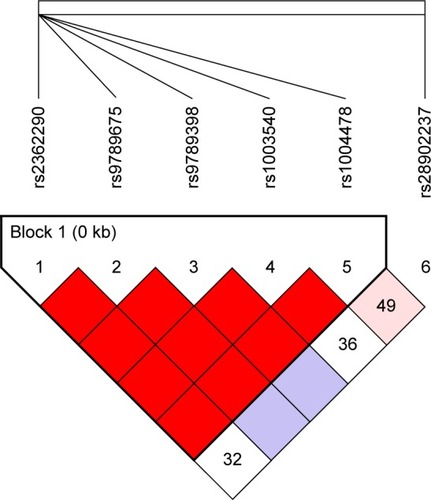
As shown in , one haplotype block including five SNPs (rs2362290, rs9789675, rs9789398, rs1003540, and rs1004478) with D′=1 was detected in TRPM8 SNPs by haplotype analyses. Haplotypes with frequencies equaling to 1% were selected for the analysis. The five SNPs constructed four haplotypes (“AGTGG”, “GGTAC”, “AGTGC”, and “AACGC”). As shown in , there was a trend toward an increased risk of COPD and the haplotype “AGTGC” in the TRPM8 gene after adjusting for sex, age, and smoking status (OR =1.44, 95% CI =0.98–2.12, P=0.043).
Table 6 Haplotype association with response (n=508, adjusted for smoking status + sex + age)
Figure 1 LD plots containing four SNPs from the TRPM8.
Abbreviations: LD, linkage disequilibrium; LOD, likelihood of odds; SNP, single nucleotide polymorphism; TRPM8, transient receptor potential cation channel subfamily M member 8.
Discussion
Based on the data from 513 COPD patients and 506 controls from the Chinese Han population, the study demonstrated that rs9789398 in the TRPM8 gene was significantly associated with the risk of COPD in the Chinese Han population. Moreover, rs9789675, rs9789398, and rs1004478 in TRPM8 were significantly associated with the risk of PH in COPD.
Previous data demonstrated that TRP superfamily of existence of cation channels in a broad range of cell types played key roles in respiratory diseases such as COPD and asthma.Citation38 Among this subfamily, TRPM2, TRPM4, and TRPM8 are emerging as possible targets in the treatment of respiratory diseases.Citation39 In 2006, TRPM8 antagonists was used as potential therapeutic agents for the treatment of asthma, COPD, and allergic rhinitis.Citation40 Subsequently, TRPM8 antagonists have been designed to treat several conditions such as COPD and PH. The possible treatment of respiratory disorders with TRPM8-specific ligands is currently being examined at an early exploratory stage. A Russian ethnic group showed that subjects with heterozygous genotype GC in SNP rs11562975 were characterized by increasing sensation of cold, hypometabolic response to local skin cooling, and non-temperature activation of TRPM8 ion channel by menthol, ie, decrease in total metabolism, pulmonary ventilation, and coefficient of oxygen extraction.Citation40 Although no SNPs located in TRPM8 were reported, abundant genetic variation contributing to COPD susceptibility has been put forward. Using quantitative meta-analysis, Castaldi et alCitation16 showed that four variants in GSTM1, TGFB1, TNF, and SOD3 would influence the development of COPD. The associations of HHIP on 4q31, FAM13A on 4q22, BICD1 on 12p11., and CHRNA3/5 on 15q25 with the risk of COPD were reported in the GWA study.Citation15
COPD is widely recognized as a complex disease with genetic–environmental interactions, which has become one of the primary causes of morbidity.Citation41–Citation43 Traditionally, it is considered that cigarette smoking is an underlying risk factor for the development of COPD. However, data showed that only 10%–15% of chronic, heavy cigarette smokers would develop symptomatic airflow obstruction. In the current study, there was no significant association between studied SNPs and the risk of COPD among nonsmokers or former smokers. Notably, the analysis of the SNPs of the rs9789675 and the rs9789398 polymorphisms demonstrated that the two SNPs were significantly associated with the risk of COPD among current smokers, which might contribute to elucidate the pathogenesis of COPD and the high incidence of COPD among smokers.
Mild-to-moderate PH is a common complication of COPD. Previous evidence demonstrated that pulmonary vascular remodeling in COPD was the main reason for increased pulmonary artery pressure. Moreover, the remodeling was recognized as the result from the combined effects of hypoxia, inflammation, and loss of capillaries in severe emphysema.Citation44 Notably, previous evidence demonstrated that TRPM8 might mediate secretion of bronchial epithelial cells introduced by cold temperature, including IL-1α, IL-1β, IL-4, IL-6, etc.Citation45,Citation46 Our data showed that three SNPs, including rs9789675, rs9789398, and rs1004478 located in TRPM8, were significantly associated with the risk of PH in COPD. Although no experimental evidence supports the association, further study will be taken into consideration focusing on the role of the SNPs in the risk of PH.
There are some limitations to be noted. First, genetic associations with COPD or PH in COPD were not able to elucidate causal mechanisms, and a larger sample size and a greater number of loci would be needed for additional evidence regarding the role of these genes in COPD and PH in COPD. Second, the effects of secondhand smoke or other smoke in the “non-smoking” individuals were not taken into account. Hence, our future research would incorporate the analysis of the relationship between COPD and the detailed smoking status, including smoking intensity, secondhand smoking, and air smog. Moreover, in the current study, the investigation was not performed in heterozygous patients due to the limited sample size. Further study enrolling larger sample size is needed to verify the strength of the study.
To the best of our knowledge, we are the first to identify one candidate locus (rs9789398) associated with an increased risk of COPD in the Chinese Han population. In addition, we are the first to report that three candidate loci rs9789398, rs9789675, and rs1004478 were associated with the risk of PH development in COPD. These findings might provide a novel insight for exploring the pathogenesis of COPD and new treatment strategies. In a further study, the functional changes introduced by mutated TRPM8 need to be explored, including the underlying mechanisms.
Acknowledgments
This study was funded by the Natural Science Foundation of Guangdong Province (no 1035101200300000). We are grateful to the COPD patients and control subjects for their participation in this study. We also thank the clinicians and hospital staff who contributed to the sample and data collection.
Disclosure
The authors report no conflicts of interest in this work.
References
- HoggJCTimensWThe pathology of chronic obstructive pulmonary diseaseAnnu Rev Pathol2009443545918954287
- LopezADShibuyaKRaoCChronic obstructive pulmonary disease: current burden and future projectionsEur Respir J200627239741216452599
- TrajkovDMirkovska-StojkovikjJPetlichkovskiAAssociation of cytokine gene polymorphisms with chronic obstructive pulmonary disease in MacedoniansIran J Allergy Asthma Immunol200981314219279357
- PauwelsRARabeKFBurden and clinical features of chronic obstructive pulmonary disease (COPD)Lancet2004364943461362015313363
- PauwelsRABuistASCalverleyPMJenkinsCRHurdSSGOLD Scientific CommitteeGlobal strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. NHLBI/WHO global initiative for chronic obstructive lung disease (GOLD) workshop summaryAm J Respir Crit Care Med200116351256127611316667
- ManninoDMCOPD: epidemiology, prevalence, morbidity and mortality, and disease heterogeneityChest20021215 Suppl121S126S12010839
- LøkkeALangePVestboJFabriciusPGDeveloping COPD – 25 years follow-up study of the general populationUgeskr Laeger2006168504422442417217870
- VestboJHurdSSAgustíAGGlobal strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summaryAm J Respir Crit Care Med2013187434736522878278
- HalbertRJNatoliJLGanoABadamgaravEBuistASManninoDMGlobal burden of COPD: systematic review and meta-analysisEur Respir J200628352353216611654
- WangXLiLXiaoJAssociation of ADAM33 gene polymorphisms with COPD in a northeastern Chinese populationBMC Med Genet20091013220003279
- RennardSITreatment of stable chronic obstructive pulmonary diseaseLancet2004364943679180215337408
- FletcherCPetoRThe natural history of chronic airflow obstructionBr Med J19771607716451648871704
- SethiJMRochesterCLSmoking and chronic obstructive pulmonary diseaseClin Chest Med20002116786viii10763090
- ManninoDMHomaDMAkinbamiLJFordESReddSCChronic obstructive pulmonary disease surveillance – United States, 1971–2000Respir Care200247101184119912354338
- NakamuraHGenetics of COPDAllergol Int201160325325821778810
- CastaldiPJChoMHCohnMThe COPD genetic association compendium: a comprehensive online database of COPD genetic associationsHum Mol Genet201019352653419933216
- SimonneauGRobbinsIMBeghettiMUpdated clinical classification of pulmonary hypertensionJ Am Coll Cardiol2009541 supplS43S5419555858
- ChaouatABugnetASKadaouiNSevere pulmonary hypertension and chronic obstructive pulmonary diseaseAm J Respir Crit Care Med2005172218919415831842
- KesslerRFallerMFourgautGMennecierBWeitzenblumEPredictive factors of hospitalization for acute exacerbation in a series of 64 patients with chronic obstructive pulmonary diseaseAm J Respir Crit Care Med199915911581649872834
- PeierAMMoqrichAHergardenACA TRP channel that senses cold stimuli and mentholCell2002108570571511893340
- YoshiharaSGeppettiPHaraMCold air-induced bronchoconstriction is mediated by tachykinin and kinin release in guinea pigsEur J Pharmacol199629632912968904081
- RabeKFHurdSAnzuetoAGlobal Initiative for Chronic Obstructive Lung DiseaseGlobal strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summaryAm J Respir Crit Care Med2007176653255517507545
- RubinLJPrimary pulmonary hypertensionN Engl J Med199733621111178988890
- SimonneauGGatzoulisMAAdatiaIUpdated clinical classification of pulmonary hypertensionTurk Kardiyol Dern Ars201442Suppl 1455425697033
- RudskiLGLaiWWAfilaloJGuidelines for the echocardiographic assessment of the right heart in adults: a report from the American Society of Echocardiography endorsed by the European Association of Echocardiography, a registered branch of the European Society of Cardiology, and the Canadian Society of EchocardiographyJ Am Soc Echocardiogr2010237685713 quiz 786–78820620859
- KarasMGKizerJREchocardiographic assessment of the right ventricle and associated hemodynamicsProg Cardiovasc Dis201255214416023009911
- ZhangZLiCWuFGenomic variations of the mevalonate pathway in porokeratosisElife20154e0632226202976
- KentWJBLAT – the BLAST-like alignment toolGenome Res200212465666411932250
- LiHDurbinRFast and accurate long-read alignment with Burrows-Wheeler transformBioinformatics201026558959520080505
- LiHHandsakerBWysokerA1000 Genome Project Data Processing SubgroupThe sequence alignment/map format and SAMtoolsBioinformatics200925162078207919505943
- McKennaAHannaMBanksEThe genome analysis toolkit: a MapReduce framework for analyzing next-generation DNA sequencing dataGenome Res20102091297130320644199
- KoboldtDCZhangQLarsonDEVarScan 2: somatic mutation and copy number alteration discovery in cancer by exome sequencingGenome Res201222356857622300766
- WangKLiMHakonarsonHANNOVAR: functional annotation of genetic variants from high-throughput sequencing dataNucleic Acids Res20103816e16420601685
- BlandJMAltmanDGStatistics notes. The odds ratioBMJ20003207247146810827061
- SoléXGuinóEVallsJIniestaRMorenoVSNPStats: a web tool for the analysis of association studiesBioinformatics200622151928192916720584
- BarrettJCFryBMallerJDalyMJHaploview: analysis and visualization of LD and haplotype mapsBioinformatics200521226326515297300
- TeramotoSIshiiTYamamotoHYamaguchiYMatsuseTXenobiotic enzymes and genetics of COPDChest20051271408409 Author reply 40915654009
- BannerKHIgneyFPollCTRP channels: emerging targets for respiratory diseasePharmacol Ther2011130337138421420429
- GavvaNRDavisCLehtoSGRaoSWangWZhuDXTransient receptor potential melastatin 8 (TRPM8) channels are involved in body temperature regulationMol Pain201283622571355
- KozyrevaTVTkachenkoEIAPotapovaTAVoevodaMIRespiratory system response to cooling in subjects with single nucleotide polymorphism rs11562975 in gene of thermosensitive TRPM8 ion channelFiziol Cheloveka2014402949825272712
- BurchfielCMMarcusEBCurbJDEffects of smoking and smoking cessation on longitudinal decline in pulmonary functionAm J Respir Crit Care Med19951516177817857767520
- ItoKBarnesPJCOPD as a disease of accelerated lung agingChest2009135117318019136405
- AntóJMVermeirePVestboJSunyerJEpidemiology of chronic obstructive pulmonary diseaseEur Respir J200117598299411488336
- ChaouatANaeijeRWeitzenblumEPulmonary hypertension in COPDEur Respir J20083251371138518978137
- SabnisASReillyCAVeranthJMYostGSIncreased transcription of cytokine genes in human lung epithelial cells through activation of a TRPM8 variant by cold temperaturesAm J Physiol Lung Cell Mol Physiol20082951L194L20018441098
- SabnisASShadidMYostGSReillyCAHuman lung epithelial cells express a functional cold-sensing TRPM8 variantAm J Respir Cell Mol Biol200839446647418458237