
Abstract
Background
The aim of this population-based study was to investigate the risk of developing noninfectious rhinitis (NIR) in subjects with chronic obstructive pulmonary disease (COPD).
Materials and methods
This is a longitudinal population-based study comprising 3,612 randomly selected subjects from Gothenburg, Sweden, aged 25–75 years. Lung function was measured at baseline with spirometry and the included subjects answered a questionnaire on respiratory symptoms. At follow-up, the subjects answered a questionnaire with a response rate of 87%. NIR was defined as symptoms of nasal obstruction, nasal secretion, and/or sneezing attacks without having a cold, during the last 5 years. COPD was defined as a spirometry ratio of forced expiratory volume in 1 second divided by forced vital capacity (FEV1/FVC) <0.7. Subjects who reported asthma and NIR at baseline were excluded from the study. The odds ratios for developing NIR (ie, new-onset NIR) in relation to age, gender, body mass index, COPD, smoking, and atopy were calculated.
Results
In subjects with COPD, the 5-year incidence of NIR was significantly increased (10.8% vs 7.4%, P=0.005) and was higher among subjects aged >40 years. Smoking, atopy, and occupational exposure to gas, fumes, or dust were also associated with new-onset NIR. COPD, smoking, and atopy remained individual risk factors for new-onset NIR in the logistic regression analysis.
Conclusions
This longitudinal population-based study of a large cohort showed that COPD is a risk factor for developing NIR. Smoking and atopy are also risk factors for NIR. The results indicate that there is a link present between upper and lower respiratory inflammation in NIR and COPD.
Video abstract
Point your SmartPhone at the code above. If you have a QR code reader the video abstract will appear. Or use:
Introduction
Noninfectious rhinitis (NIR) affects 40% of the adult population, has a significant impact on health-related quality of life, and results in substantial health–economic costs to the society.Citation1–Citation3 NIR is characterized by symptoms of upper airway inflammation, such as nasal obstruction, secretion, itching and sneezing, and represents several pathological entities, including allergic rhinitis, vasomotor rhinitis, and chronic rhinosinusitis.Citation4 The disease has previously been linked to asthma, smoking, occupational exposure to gas, fumes, or dust, and also to gastroesophageal reflux disease, but for many patients with NIR, the pathophysiology remains unknown.Citation1,Citation3,Citation5,Citation6 NIR has been reported in individuals with chronic obstructive pulmonary disease (COPD), but epidemiological evidence is lacking.Citation7 COPD is an inflammatory, progressive airway disease with persistent airflow limitation. The airflow limitation in COPD is caused by a combination of small airway disease (obstructive bronchiolitis) and the destruction of lung parenchyma (emphysema). Exposure to noxious particles and gases, particularly tobacco smoking, but also occupational exposure to gas, fumes, or dust, is related to the development of COPD.Citation8,Citation9 Interestingly, the same risk factors have also been associated with NIR.Citation1,Citation6 COPD occurs predominantly in patients aged >40 years as a direct result of the slow initial development of the disease.Citation10–Citation12 Furthermore, new research has shown paranasal sinus opacification to be associated with COPD and self-reported respiratory symptoms.Citation13
The estimated prevalence of COPD in the Nordic countries, defined according to the Global Initiative for Chronic Obstructive Lung Disease stage I and higher, varies from 9.4% to 18.8%.Citation14–Citation18 To date, only a few studies have evaluated a possible link between NIR and COPD. This is surprising, as both NIR and COPD are common inflammatory conditions in the respiratory tract and could potentially be linked through a generalized airway inflammation in accordance with “the united airways” concept introduced to explain the link between upper and lower inflammatory airway disease in asthma and NIR, even though other inflammatory mechanisms are likely to be involved.Citation7
The diagnosis and classification of COPD is based on a clinical assessment and spirometry is mandatory.Citation8 To the authors’ knowledge, there are no large population-based studies of the relationship between rhinitis and COPD based on spirometry data. In the present study, data on spirometry and respiratory symptoms were combined from a large longitudinal population-based cohort, followed for 5 years. The main hypothesis of the study was that COPD is related to the development of NIR.
Material and methods
The adult onset asthma and nitric oxide cohort
This study is a part of the longitudinal population-based study called ADONIX (adult onset asthma and nitric oxide). ADONIX was approved by The Regional Ethical Review Board of Gothenburg (Dnr Ö 092-01) and has previously been described in detail.Citation5 The ADONIX study was designed to evaluate risk factors for airway disease such as NIR, COPD, and asthma. A total of 6,665 subjects, randomly selected, aged 25–75 years, from the municipal register of Gothenburg, Sweden, were included at baseline between 2001 and 2003. Written informed consent was obtained from all participants. The subjects performed spirometry and answered a questionnaire with questions on upper and lower respiratory symptoms and diseases. The subjects also underwent a measurement of fractional exhaled nitric oxide (FeNO) and a laboratory analysis of specific immunoglobulin E antibodies for atopy status. After 5 years, the included subjects were asked to answer a follow-up questionnaire. The response rate at follow-up was 87%.
Study design
This study evaluates the risk of developing new-onset NIR in relation to having COPD during a 5-year observation period. The questions used for new-onset NIR and associated risk factors, such as smoking, educational status, and occupational exposure to gas, fumes, or dust, are shown in . The questions on occupational exposure to gas, fumes, or dust, and educational status were added in 2005 and were therefore not answered by all the participants at baseline. For this reason, occupational exposure and educational status were analyzed separately in a sub-analysis.
Table 1 Questionnaire items on new-onset NIR, gas, fumes, and dust, smoking, and educational status
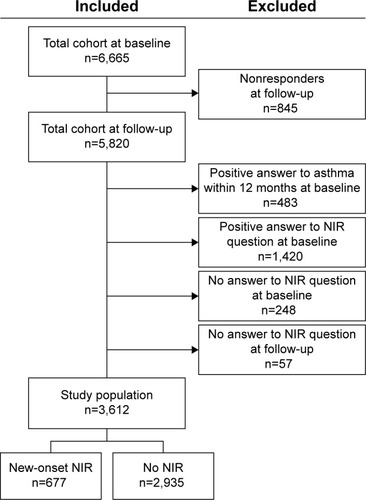
The study population is shown in . Subjects who reported NIR at baseline were excluded from the study population, along with subjects who did not answer the NIR question at follow-up. To avoid misclassification between asthma and COPD, all the subjects who reported asthma during the past 12 months at baseline were also excluded. As a result, 3,612 subjects were included in the analyses.
Figure 1 Flow chart of the study population and the subjects excluded.
Spirometry was performed with a dry wedge spirometer (Vitalograph, Buckingham, UK). According to the guidelines available at the time of the study,Citation19 the best of a minimum of three similar maneuvers was used. The ratio of the forced expiratory volume in 1 second (FEV1) divided by forced vital capacity (FVC) was calculated and a cut-off value for the FEV1/FVC ratio of <0.7 defined COPD in accordance with the Global Initiative for Chronic Obstructive Lung Disease guidelines,Citation8 apart from the fact that no reversibility test was performed. Spirometry data were available for 93% of the subjects at baseline (n=3,348). FeNO was measured before spirometry using a chemiluminescence analyzer and has been extensively described elsewhere.Citation20 A cut-off value of 50 ppb or more in the exhaled NO concentration was used to indicate a high likelihood of asthma in patients with COPD.Citation21 Atopy was defined as a positive Phadiatop® test (Pharmacia, Uppsala, Sweden). Class 0 was regarded as negative and Class 1 as positive (atopic).Citation22 Data on age, gender, and body mass index (BMI) were also collected ().
Table 2 New-onset of NIR in relation to age, gender, BMI, atopy, COPD, and smoking
Statistics
Analyses were performed with the SAS statistical software version 9.4 (SAS Institute Inc., Cary, NC, USA). Univariate analyses included using t-tests and chi-square tests for continuous and categorical variables respectively. A multivariate logistic regression model was used to calculate odds ratios and 95% confidence intervals. P-values <0.05 were considered statistically significant.
Results
The comparison between subjects with new-onset NIR and no NIR at follow-up is presented in . As shown, there was no significant difference in mean age, gender, or BMI. The prevalence of COPD was 8% in the total study population and 9.2% for subjects aged over 40 years. New-onset NIR was significantly associated with COPD (10.8 vs 7.4 P=0.005). New-onset NIR was also related to smoking (P=0.004) and atopy (P<0.001) in the univariate analyses.
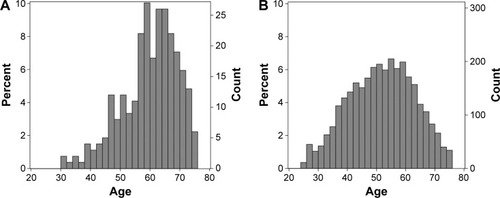
In the logistic regression analysis adjusted for age, gender, BMI, COPD, smoking, and atopy, COPD, smoking, and atopy remained independently associated with new-onset NIR (). The interaction between COPD and smoking in relation to new-onset NIR was calculated and was found to be nonsignificant (data not shown). There was no association between atopy and COPD, indicating a low risk of asthma misclassification (19.1% vs 19.2%, P=1). As shown in , the vast majority of the subjects with COPD were aged >40 years, as expected. Only 4.3% (11 of 257 subjects with COPD) displayed a FeNO value >50 ppb, ie, values that indicate the presence of atopy and asthma.
Figure 2 Odds ratios for new-onset NIR in relation to age, gender, BMI, COPD, smoking, and atopy.
Note: Never smoker was used as reference category among the smoking categories.
Abbreviations: BMI, body mass index; CI, confidence interval; COPD, chronic obstructive pulmonary disease; NIR, noninfectious rhinitis.
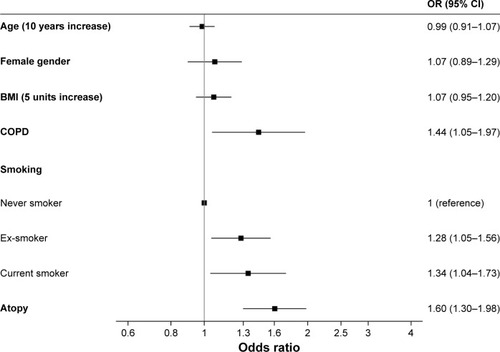
Figure 3 Age distribution when comparing the COPD group (A) and the general population (B).
The sub-analysis of occupational exposure to gas, fumes, or dust (n=2,257), and educational status (n=2,256) introduced in 2005 revealed a significant association with new-onset NIR for gas, fumes, or dust (P=0.006) but not for educational status (P=0.75) (data not shown).
Discussion
In this longitudinal population-based study of a large cohort, the risk of developing NIR, over a 5-year period increased in individuals with COPD. Smoking and atopy were also risk factors for NIR. The results indicate that there is a link present between upper and lower respiratory inflammation in NIR and COPD, and it is therefore important to assess NIR in patients with COPD.
NIR is identified by the presence of nasal symptoms, but identifying individuals with COPD requires spirometry. The authors are not aware of any previous studies of NIR in COPD, including spirometry data from a large general population sample. In this study, spirometry was performed without bronchodilation according to the standard used at the time. This could have resulted in misclassification between COPD and asthma. In an attempt to minimize the risk of misclassification to eosinophilic inflammation and asthma, all subjects reporting asthma within 12 months at baseline were excluded from the analyses. Also, atopy in subjects with COPD was analyzed and no significant association with COPD was identified. Furthermore, only 4.3% of the subjects in the COPD group had FeNO >50 ppb, which indicates a low prevalence of eosinophilic inflammation in this group. Therefore, the subjects in this study with an FEV1/FVC of <0.7 are believed to be a representative of COPD.
The prevalence of COPD in this general population sample was 8.8%, which is consistent with previous estimates ranging between 9.4% and 18.8%.Citation14–Citation18 The prevalence was also higher in subjects aged ≥40 and above, which is in accordance with other studies of COPD.Citation11
The main finding in this study was that the 5-year cumulative incidence of NIR was higher in the subjects with COPD, both in the univariate analyses and the logistic regression analyses. Smoking and atopy also remained independent risk factors for new-onset NIR in the logistic regression analyses. Although a previous study based on questionnaire data alone has indicated a relationship between rhinitis and COPD in a large population sample, this study adds vital information on lung function that is needed for a COPD diagnosis and confirms that there is a relationship between the two diseases.Citation7
Although the study shows a link between upper and lower respiratory inflammation in COPD and NIR, it is important to note that the findings do not imply a causal relationship between COPD and NIR. In spite of this, both diseases share common features that could be of importance for disease development in the airway at different levels. A similar inflammatory response can be elicited in both the upper and lower airways following exposure to inhaled irritants and sensitizers in the common airstream. Gas, fumes, or dust are regarded as risk factors for COPD,Citation9 as well as for NIR.Citation6 Individual vulnerability in the airway mucosa to irritants or deficits in systemic inflammatory responses could also explain why COPD and NIR can more commonly be found in the same subjects. The humoral spread of inflammatory mediators via the blood stream to both the upper and lower airways as seen in rhinitis and asthma is another possibility.Citation23
Tobacco smoke is an airborne irritant that is significantly associated not only with the development of COPD but also with NIR.Citation1,Citation11,Citation12,Citation24 In terms of the temporal relationship between the onset of COPD and NIR, it is important to recognize that the airway inflammation in COPD and NIR is likely to develop over time. In the absence of histological specimens from the airway, it is not possible to determine when and where inflammation starts and symptoms may begin later than signs of airway inflammation. Differences in the concentrations to which the upper and lower airways are exposed may also explain different patterns of symptom debut. Tobacco smoke is mainly inhaled through the mouth directly to the lungs and the tobacco load on the nasal mucosa is likely to be lower. To be able to establish plausible common pathophysiological mechanisms, there is therefore a need for clinical studies.
Two possible risk factors for new-onset NIR were analyzed separately, due to their late introduction in the questionnaire that missed a part of the study population, ie, educational status and occupational exposure to gas, fumes, or dust. Educational status was not associated with new-onset NIR, despite having previously been considered to be a risk factor for COPD.Citation25 Occupational exposure to gas, fumes, or dust was not included in the logistic regression due to missing data, but in the sub-analyses it showed an association with new-onset NIR. In developing countries, this is a major risk factor for COPD due to cooking over open fires and it may also be important for NIR, but the exposure in developed countries, such as Sweden, is expected to be low.
The main strength of the present study is its longitudinal population-based design with a large general population, including the availability of spirometry data for 93% of the subjects. It is, however, also important to consider the limitations of this study. NIR includes several phenotypes of rhinitis, both allergic and nonallergic, as well as chronic rhinosinusitis. As a result, the NIR question does not enable us to link COPD to a specific phenotype of rhinitis. The interval of 5 years in the follow-up questionnaire may have introduced recall bias when answering the NIR question. Furthermore, this epidemiological study did not include a clinical assessment of COPD by a doctor and therefore have no information on the severity of the disease. The COPD definition that was used may also have introduced misclassification to other lower airway diseases showing a similar spirometry pattern, but, as previously discussed, the risk of including asthmatics in this study was minimized.
There is an established inflammatory link between asthma and rhinitis, which many regard as the concept of generalized airway inflammation – “the united airways”, helping to define and understand the disease.Citation3 This study provides new evidence linking NIR to COPD, supported by the fact that both diseases involve inflammation of the airway mucosa and that they share common risk factors, such as exposure to tobacco smoke and cooking fumes. In contrast to the link between allergic rhinitis and asthma, the authors are aware of no common inflammatory pathway in COPD and NIR, such as the allergic inflammation that could explain the coexistence of the two diseases. To be able to confirm a pathophysiological relationship, further studies are needed, but the present study shows that COPD should be regarded as a co-factor in the development of NIR.
The link between NIR and COPD also suggest that the diagnosis and treatment of the two diseases in the same patient could be of importance for patient outcome in terms of early diagnosis, disease control, and patient satisfaction, which has to be addressed further.
Conclusion
This longitudinal population-based study of a large cohort shows that COPD is a risk factor for developing NIR. Smoking and atopy are also risk factors for NIR. The results indicate that there is a link present between upper and lower respiratory inflammation in NIR and COPD.
Author contributions
All authors contributed toward data analysis, drafting and critically revising the paper and agree to be accountable for all aspects of the work.
Acknowledgments
The authors would like to thank the Department of Occupational and Environmental Medicine, Sahlgrenska University Hospital, for its contribution in retrieving and filing data. The authors wish to thank the Gothenburg Medical Society, the Acta Otolaryngologica Foundation, the Eriksson Brothers fund and the Swedish Research Council for Health, Working Life and Welfare for their contribution.
Disclosure
The authors report no conflicts of interest in this work.
References
- HellgrenJLillienbergLJarlstedtJKarlssonGTorenKPopulation-based study of non-infectious rhinitis in relation to occupational exposure, age, sex, and smokingAm J Ind Med2002421232812111687
- CardellLOOlssonPAnderssonMTOTALL: high cost of allergic rhinitis-a national Swedish population-based questionnaire studyNPJ Prim Care Respir Med2016261508226845513
- BousquetJKhaltaevNCruzAAAllergic Rhinitis and its Impact on Asthma (ARIA) 2008 update (in collaboration with the World Health Organization, GA(2)LEN and AllerGen)Allergy200863Suppl 86816018331513
- FokkensWJLundVJMullolJEuropean Position Paper on Rhinosinusitis and Nasal Polyps 2012. A summary for otorhinolaryngologistsRhinology201250111222469599
- HellgrenJOlinACTorenKIncreased risk of rhinitis symptoms in subjects with gastroesophageal refluxActa Otolaryngol2014134661561924665868
- ThilsingTRasmussenJLangeBKjeldsenADAl-KalemjiABaelumJChronic rhinosinusitis and occupational risk factors among 20- to 75-year-old Danes-A GA(2) LEN-based studyAm J Ind Med201255111037104322648974
- NihlenUMontnemeryPAnderssonMSpecific nasal symptoms and symptom-provoking factors may predict increased risk of developing COPDClin Physiol Funct Imaging200828424025018331572
- Global Strategy for the Diagnosis, Management and Prevention of COPD, Global Initiative for Chronic Obstructive Lung Disease (GOLD)2016 Available from: http://www.goldcopd.org/Accessed January 7, 2016
- HagstadSBackmanHBjergAPrevalence and risk factors of COPD among never-smokers in two areas of Sweden – occupational exposure to gas, dust or fumes is an important risk factorRespir Med2015109111439144526440676
- LindbergABjergARonmarkELarssonLGLundbackBPrevalence and underdiagnosis of COPD by disease severity and the attributable fraction of smoking Report from the Obstructive Lung Disease in Northern Sweden StudiesRespir Med2006100226427215975774
- HalbertRJNatoliJLGanoABadamgaravEBuistASManninoDMGlobal burden of COPD: systematic review and meta-analysisEur Respir J200628352353216611654
- LundbackBLindbergALindstromMObstructive Lung Disease in Northern Sweden StudiesNot 15 but 50% of smokers develop COPD? – report from the obstructive lung disease in Northern Sweden studiesRespir Med200397211512212587960
- HansenAGHelvikASThorstensenWMParanasal sinus opacification at MRI in lower airway disease (the HUNT study-MRI)Eur Arch Otorhinolaryngol201627371761176826499376
- DanielssonPOlafsdottirISBenediktsdottirBGislasonTJansonCThe prevalence of chronic obstructive pulmonary disease in Uppsala, Sweden – the Burden of Obstructive Lung Disease (BOLD) study: cross-sectional population-based studyClin Respir J20126212012721651748
- NielsenRJohannessenABenediktsdottirBPresent and future costs of COPD in Iceland and Norway: results from the BOLD studyEuro Respir J2009344850857
- BuistASMcBurnieMAVollmerWMBOLD collaborative research groupInternational variation in the prevalence of COPD (the BOLD Study): a population-based prevalence studyLancet2007370958974175017765523
- HansenJGPedersenLOvervadKOmlandOJensenHKSorensenHTPrævalensen af kronisk obstruktiv lungesygdom – sekundærpublication [Prevalence of chronic obstructive pulmonary disease–secondary publication]Ugeskr Laeger20091714129862988 Swedish19824224
- Jyrki-TapaniKSovijarviALundbackBChronic obstructive pulmonary disease in Finland: prevalence and risk factorsCOPD20052333133917146998
- Standardization of Spirometry, 1994 Update. American Thoracic SocietyAm J Respir Crit Care Med19951523110711367663792
- OlinACRosengrenAThelleDSLissnerLBakeBTorenKHeight, age, and atopy are associated with fraction of exhaled nitric oxide in a large adult general population sampleChest200613051319132517099006
- DweikRABoggsPBErzurumSCIrvinCGLeighMWLundbergJOAn official ATS clinical practice guideline: interpretation of exhaled nitric oxide levels (FENO) for clinical applicationsAm J Respir Crit Care Med2011184560261521885636
- MatricardiPMNisiniRPizzoloJGD’AmelioRThe use of Phadiatop in mass-screening programmes of inhalant allergies: advantages and limitationsClin Exp Allergy19902021511552357615
- DenburgJAvan EedenSFBone marrow progenitors in inflammation and repair: new vistas in respiratory biology and pathophysiologyEur Respir J200627344144516507840
- BuistASVollmerWMMcBurnieMAWorldwide burden of COPD in high- and low-income countries. Part I. The burden of obstructive lung disease (BOLD) initiativeInt J Tuberc Lung Dis200812770370818544191
- PrescottELangePVestboJSocioeconomic status, lung function and admission to hospital for COPD: results from the Copenhagen City Heart StudyEur Respir J19991351109111410414412