
Abstract
Purpose
Previous studies have reported that anemia increased mortality in patients with COPD. However, it is unclear whether anemia is associated with increased COPD mortality in the general population. The purpose of our study is to identify whether anemia is related to long-term mortality in COPD using a large population-based database.
Patients and methods
Using the National Health Insurance Service-Health Screening Cohort, we identified COPD patients with available hemoglobin level. We analyzed mortality among patients with COPD from 2003 to 2013 according to hemoglobin level.
Results
A total of 7,114 patients with COPD were identified. Mean age was 65.0±9.3 years, and 62.9% were male. Anemia was present in 469 patients (6.6%). The overall mortality rate was 46.5% in anemia and 32.1% in non-anemia groups (p<0.001). The hazard ratio of anemia for mortality was 1.31 (95% CI, 1.11–1.54). Among patients with anemia, the hemoglobin level correlated well with mortality.
Conclusion
Anemia was associated with increased long-term mortality of COPD, and even mild anemia was related to a significantly increased risk.
Keywords:
Introduction
COPD was the third leading cause of death worldwide in 2010.Citation1 Mortality in patients with COPD is related to various measures, including forced expiratory volume in 1 second, ratio of inspiratory to total lung capacities, exercise capacity, dyspnea scores, body mass index (BMI), and exacerbation frequency.Citation2
Anemia is a well-known comorbidity of COPD. The prevalence of anemia in COPD ranges from 7.5% to 32.7%.Citation3 Anemia reflects chronic illness and burden of disease, and COPD patients with anemia have an increased risk for poor outcomes. Previous studies have reported that anemia increased mortality in COPD;Citation4–Citation9 however, these studies only included patients who were receiving long-term oxygen therapy or required hospitalization or analyzed a small number of patients or short-term survival. To the best of our knowledge, no large-scale and population-based studies have evaluated the effect of anemia on the long-term survival of COPD.
The purpose of our study was to identify whether anemia is related to long-term mortality in COPD using a large population-based database. We also aimed to evaluate whether the degree of anemia affects the survival of patients with COPD.
Materials and methods
Source of data
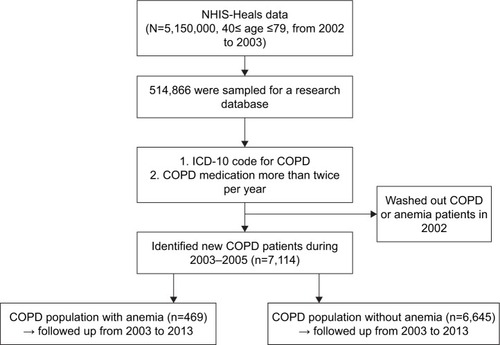
Since 2000, the National Health Insurance Service (NHIS) in Korea has provided a health insurance service to nearly all people living in Korea. Consequently, a large amount of health-related data has accumulated in the NHIS system. Using this database, the Korean NHIS has established a research database. Because all Koreans have been recommended to undergo a national health screening every 2 years, the NHIS was able to generate a health screening cohort that was the NHIS-Health Screening (NHIS-Heals) database. From 2002 to 2003, a total of 5,150,000 people between the ages of 40 and 79 years received national health screening. Among them, 514,866 people were sampled and followed up from 2002 to 2013 for a research database, which was used for our study (). NHIS-Heals database comprised a random selection of 10% (n=514,866) of all health screening participants (n=5,150,000) in 2002 and 2003. This research database included data on socioeconomic status (household income), medical treatments, medical care institutions, and general health examinations. NHIS data is de-identified by government. This study was approved by the Institutional Review Board of NHIS Ilsan Hospital.
Figure 1 Flow chart of the study population.
Study population
Because the NHIS database did not include spirometry data essential for the diagnosis of COPD and did not also include an individual’s medical history or symptoms, we identified COPD patients using the International Classification of Disease-Tenth Revision (ICD-10) and prescription details in the health screening cohort. We used the diagnostic criteria that an individual should visit the medical facility at least twice per year with both a COPD diagnostic code and a prescription for 1 or more COPD medications. Similar to previous studies,Citation10–Citation13 COPD patients were identified by the presence of all of the following criteria: >40 years of age; ICD-10 codes for COPD (J43-J44, except J430); and COPD medication use at least twice per year. COPD medications include long-acting muscarinic antagonist, long-acting beta-2 agonist (LABA), inhaled corticosteroid (ICS), ICS plus LABA, short-active muscarinic antagonist (SAMA), short-acting beta-2 agonist (SABA), SAMA plus SABA, methylxanthines, systemic corticosteroids, and systemic beta agonists. The national health screening cohort included laboratory data, from which we obtained the hemoglobin levels. Hemoglobin status was categorized as anemia or non-anemia according to the World Health Organization guidelines (anemia defined as hemoglobin <12 g/dL in females, <13 g/dL in males).Citation14 The population with COPD or anemia in 2002 was excluded, and only patients with newly diagnosed COPD from 2003 to 2005 were enrolled. We followed these COPD patients from 2003 to 2013 to analyze the effect of anemia on COPD survival (). All Koreans have been recommended to undergo a national health screening every 2 years; therefore, all individuals had 1 or 2 hemoglobin measurements from 2003 to 2005. If an individual had 2 measurements, we used the first hemoglobin result.
Determinants of disease and demographic factors
The demographic factors of COPD patients were analyzed at the time of COPD diagnosis and first health screening visits. Socioeconomic status was divided into 5 categories according to household income. Charlson comorbidity index (CCI) was calculated according to a previous study.Citation15 BMI was calculated based on height and body weight. The patients were categorized as underweight (BMI<18.5), normal (18.5–22.9), overweight (23–24.9), obese I (25.0–29.9), or obese II (≥30).Citation16 Smoking status was divided into 3 groups according to a health questionnaire completed at the first health screening visit. Never-smokers were defined as those who answered that they had never smoked. Ex-smokers were defined as those who answered that they had smoked before, but did not smoke at the time of the health screening visit. Current smokers were defined as those who answered that they smoked at the time of the health screening visit.
Study outcomes
Patients were enrolled at the time of COPD diagnosis and followed up until the end of the study period or death. The monthly mortality was compared between anemic and non-anemic groups from 2003 to 2013. We also analyzed the effect of different hemoglobin levels on mortality.
Statistical analysis
Differences between groups were assessed using the Chi-square test for categorical variables and Student’s t-test for continuous variables. A Cox proportional hazards model was used to identify independent variables for mortality of COPD. Results were presented as hazard ratio (HR) and 95% CI. Violation of proportional hazards assumption was tested by exploring log (-log [survival]) curves. A p-value <0.05 was considered statistically significant. All statistical analyses were performed with the SAS program, version 9.4 (SAS Institute, Cary, NC, USA).
Results
Study population
A total of 7,114 patients with COPD were included during the period 2003 to 2005 (). Mean age was 65.0±9.3 years, and 62.9% were male. Anemia was present in 469 (6.6%) patients. Gender distribution was similar between anemia and non-anemia groups, but elderly patients were more frequent in the anemic group. Mean hemoglobin level was 11.5±1.1 g/dL in the anemia group and 14.2±1.2 g/dL in the non-anemia group. Anemic patients had higher CCI and lower BMI. Overall, patients in the anemia group were older and more likely to have chronic illness than those in the non-anemia group.
Table 1 Demographic and clinical characteristics of COPD patients with or without anemia
Mortality
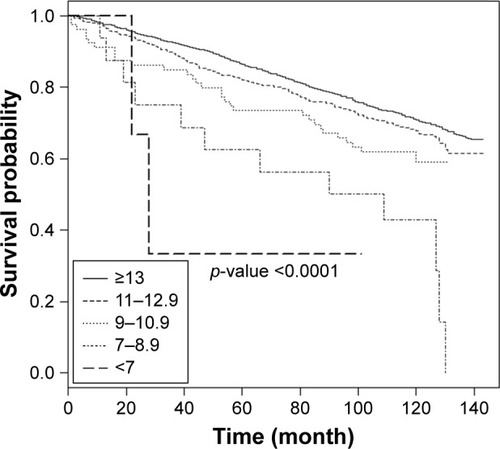
The overall mortality rate during the study period was 46.5% in the anemia group and 32.1% in the non-anemia group. The mean follow-up duration was 100.0±36.5 months (87.7±39.9 in anemia vs 100.8±36.1 in non-anemia). showed a Cox proportional hazards model for factors associated with mortality in COPD patients. In multivariate analysis, overall mortality was associated with old age, low socioeconomic status, high CCI, low BMI, and anemia. The HR of anemia for mortality was 1.31 (95% CI, 1.11–1.54). Lower hemoglobin levels were also associated with increased mortality regardless of anemia severity. The HR for death in patients with a hemoglobin value between 11.0 and 13.0 g/dL compared with a hemoglobin value over 13.0 g/dL was 1.23 (95% CI, 1.04–1.45). Patients with hemoglobin <7 g/dL had an approximately 5-fold higher risk of death than non-anemic patients. shows the Kaplan–Meier survival curves for anemia and non-anemia. The survival rate of anemia group was lower than that of the non-anemia group. The 5-year survival rate was 0.72 in the anemia group and 0.84 in the non-anemia group. shows the data for different hemoglobin levels. These show a clear difference in survival rate according to hemoglobin. Even in anemia patients, the decrease in hemoglobin level was closely related to the decrease in survival rate. When we analyzed the HR for mortality using continuous hemoglobin values (g/dL), the HR of hemoglobin for mortality was 0.92 (95% CI, 0.86–0.96).
Table 2 Cox proportional hazards model for factors associated with mortality in COPD patients
Figure 2 Kaplan–Meier survival curves for anemia and non-anemia.
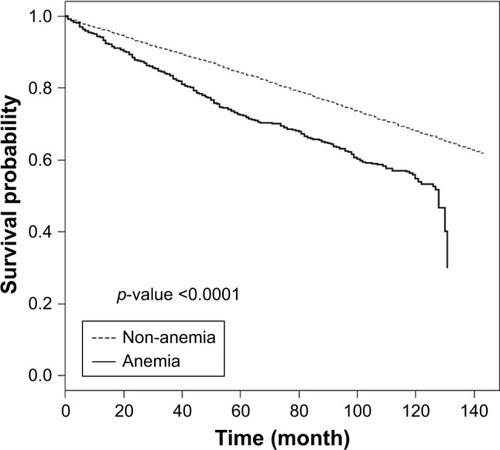
Figure 3 Kaplan–Meier survival curves by different hemoglobin levels.
Discussion
To the best of our knowledge, this is the first study that evaluated the long-term effect of anemia on COPD survival in the general population. Our data showed that the prevalence of anemia in COPD was 6.6% and that anemia was associated with increased long-term mortality. Hemoglobin level was well correlated with mortality. Even a mild decrease in hemoglobin increased the risk of death, and the risk of mortality increased in proportion to the decrease in hemoglobin.
Although anemia is a well-known comorbidity of COPD, studies on the impact of hemoglobin on COPD mortality are lacking, and the characteristics of populations in previous studies were highly variable. Overall, studies have shown a trend for increased mortality in COPD patients with anemia. However, most studies had retrospective designs, included patients who were receiving long-term oxygen therapy or required hospitalization, or analyzed a small number of patients or short-term survival. Overall, previous studies might be categorized into 3 broad groups: COPD patients with long-term oxygen therapy or non-invasive ventilation; stable COPD outpatients; and hospitalized COPD patients with acute exacerbation.
The pivotal study analyzing the long-term effect of anemia on COPD mortality was conducted by Chambellan et al.Citation4 They used the ANTADIR (Association Nationale pour le Traitement a Domicile de l’Insuffisance Respiratoire) database, which was generated from the French national home-care system for patients requiring oxygen support or mechanical ventilation. Among COPD patients receiving long-term oxygen therapy, the prevalence of anemia was 12.6% in men and 8.2% in women. The hematocrit was an independent predictor of survival, hospital admission rate, and cumulative duration of hospitalization in this population. The long-term survival rate decreased with lower hematocrit levels. Kollert et al analyzed similar patients who had severe COPD and chronic respiratory failure with non-invasive ventilation.Citation17 They reported that high hemoglobin level prior to the initiation of non-invasive ventilation was associated with better long-term survival. The optimal cutoff value for prediction of death was 14.3 g/dL for females and 15.1 g/dL for males.
The effect of anemia on mortality for stable COPD outpatients has also been reported. Cote et al reported hemoglobin level and its clinical impact for stable COPD outpatients in a USA Veterans Administration pulmonary clinic.Citation18 The number of total COPD patients was 683, and anemia was present in 116 (17%). Anemia was independently associated with increased dyspnea and reduced the 6-minute walking distance; however, it was not a significant independent predictor of mortality. Boutou et al also conducted a retrospective study to evaluate the association between anemia and survival in stable COPD outpatients.Citation7 Of a total 294 COPD patients, 46 (15.6%) had anemia. Anemia was an independent predictor of mortality (HR 1.87, 95% CI, 1.06–3.29) and was associated with shorter median survival.
The association between anemia and mortality in hospitalized COPD patients has been recently evaluated. Martinez-Rivera et al reported that anemia and previous exacerbations were independent predictors of 1-year mortality in hospitalized COPD patients.Citation6 Patients with anemia had a relative risk of death of 5.9 (95% CI, 1.9–18.9). Toft-Petersen et al similarly reported that a lower hemoglobin level at admission was related to higher risk of long-term mortality after discharge.Citation9 Some studies have evaluated short-term mortality in anemic COPD patients with hospitalization. Rasmussen et al evaluated the 90-day mortality among COPD patients who needed invasive mechanical ventilation.Citation5 In these patients, anemia was associated with increased mortality, and the adjusted 90-day mortality risk ratio was 2.6 (95% CI, 1.5–4.5). Ergan and Ergün also reported that anemia was a risk factor of in-hospital death in COPD patients requiring mechanical ventilation.Citation8 In multivariate analysis, the odds ratio of anemia for hospital mortality was 3.99 (95% CI, 1.4–11.4).
Previous studies have reported the prevalence of anemia in COPD ranging from 7.5% to 32.7%.Citation3 The prevalence in our study was 6.6%. Anemia reflects chronic illness and burden of disease, and our cohort included a relatively healthy population who regularly underwent the national health screening examination. The patients included in this study were newly diagnosed patients with COPD and probably milder than other cohorts previously reported. Therefore, the prevalence in our study might be lower than in other studies. Interestingly, other studies on stable outpatients with COPD have reported a prevalence of anemia ranging from 15.6% to 17.1%.Citation7,Citation18
Although several studies have shown that anemia in COPD is related to increased mortality, to our knowledge, there are no studies that evaluated the association between anemia and long-term mortality of COPD in the general population. Our study also included a larger number of COPD patients with long-term follow-up compared with previous studies. Our results are significant in that anemia increases mortality even in the general COPD population who do not require oxygen therapy, hospitalization, or frequent healthcare use. We also showed that even a mild decrease in hemoglobin increased the risk of death. Toft-Petersen et al reported similar results.Citation9 They showed that a decrease in hemoglobin by only 1 g/dL compared with the normal value had an HR for death of 1.37 (95% CI, 1.15–1.64) in males and 1.28 (95% CI, 1.06–1.53) in females.
Our study has some limitations. First, we could not use spirometry data, but used only ICD-10 codes and medications for COPD diagnosis. However, this working definition has been utilized and validated in many previous studies.Citation10–Citation13 We could not also use an individual’s medical history or symptoms that might be helpful for COPD diagnosis. Second, confounding factors could have affected the mortality. COPD mortality is associated with various factors. We attempted to control for possible confounders, such as socioeconomic status, CCI, BMI, and smoking; however, other factors were not examined. Especially, we did not include the important comorbidities of COPD that may have influenced mortality. Moreover, anemia has numerous causes that may be confounders, and we could not exclude patients with comorbidity associated with anemia. Third, this is a retrospective observational study and so could involve missing data or follow-up loss. However, in the NHIS database, every detail of healthcare utilization was recorded without any missing data. Moreover, since national insurance is mandatory by law, almost the entire population in Korea can be followed in the NHIS database without loss. This advantage of the NHIS database can increase the value of the results obtained in this study.
Conclusion
Our large population-based study showed that anemia was associated with increased long-term mortality of COPD. Even mild anemia was related to a significantly increased risk of death. Hemoglobin level was well correlated with risk of death. More studies are needed to prospectively evaluate the effects of anemia on COPD mortality.
Acknowledgments
This study used NHIS-HealS data (NHIS-2017-2-406) made by NHIS.
Disclosure
The authors report no conflicts of interest with NIHS and with this work.
References
- LozanoRNaghaviMForemanKGlobal and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010Lancet20123802095212823245604
- BerryCEWiseRAMortality in COPD: causes, risk factors, and preventionCOPD2010737538220854053
- YohannesAMErshlerWBAnemia in COPD: a systematic review of the prevalence, quality of life, and mortalityRespir Care20115664465221276321
- ChambellanAChailleuxESimilowskiTPrognostic value of the hematocrit in patients with severe COPD receiving long-term oxygen therapyChest20051281201120816162707
- RasmussenLChristensenSLenler-PetersenPJohnsenSPAnemia and 90-day mortality in COPD patients requiring invasive mechanical ventilationClin Epidemiol201031521326654
- Martinez-RiveraCPortilloKMuñoz-FerrerAAnemia is a mortality predictor in hospitalized patients for COPD exacerbationCOPD2012924325022360381
- BoutouAKKarrarSHopkinsonNSPolkeyMIAnemia and survival in chronic obstructive pulmonary disease: a dichotomous rather than a continuous predictorRespiration20138512613122759351
- ErganBErgünRImpact of anemia on short-term survival in severe COPD exacerbations: a cohort studyInt J Chron Obstruct Pulmon Dis2016111775178327536089
- Toft-PetersenAPTorp-PedersenCWeinreichUMRasmussenBSAssociation between hemoglobin and prognosis in patients admitted to hospital for COPDInt J Chron Obstruct Pulmon Dis2016112813282027877035
- KimJLeeJHKimYAssociation between chronic obstructive pulmonary disease and gastroesophageal reflux disease: a national cross-sectional cohort studyBMC Pulm Med2013135123927016
- KimJRheeCKYooKHThe health care burden of high grade chronic obstructive pulmonary disease in Korea: analysis of the Korean Health Insurance Review and Assessment Service dataInt J Chron Obstruct Pulmon Dis2013856156824277985
- KimJKimKKimYThe association between inhaled long-acting bronchodilators and less in-hospital care in newly-diagnosed COPD patientsRespir Med201410815316123993445
- RheeCKYoonHKYooKHMedical utilization and cost in patients with overlap syndrome of chronic obstructive pulmonary disease and asthmaCOPD20141116317024111662
- World Health OrganizationHaemoglobin Concentrations for the Diagnosis of Anaemia and Assessment of Severity. Vitamin and Mineral Nutrition Information SystemGenevaWorld Health Organization2011 Available from: http://www.who.int/vmnis/indicators/haemoglobin.pdfAccessed August 17, 2017
- CharlsonMEPompeiPAlesKLMacKenzieCRA new method of classifying prognostic comorbidity in longitudinal studies: development and validationJ Chronic Dis1987403733833558716
- AnuuradEShiwakuKNogiAThe new BMI criteria for Asians by the regional office for the western pacific region of WHO are suitable for screening of overweight to prevent metabolic syndrome in elder Japanese workersJ Occup Health20034533534314676412
- KollertFTippeltAMüllerCHemoglobin levels above anemia thresholds are maximally predictive for long-term survival in COPD with chronic respiratory failureRespir Care2013581204121223232736
- CoteCZilberbergMDModySHDordellyLJCelliBHaemoglobin level and its clinical impact in a cohort of patients with COPDEur Respir J20072992392917251227