
Abstract
Background and aims
Chronic obstructive pulmonary disease (COPD) is a heterogeneous disease characterized by different phenotypes with either bronchial airways alterations or emphysema prevailing. As blood biomarkers could be clinically useful for COPD stratification, we aimed at investigating the levels of blood biomarkers in COPD patients differentiated by phenotype: prevalent chronic airway disease versus emphysema.
Methods
In 23 COPD patients with prevalent airway disease (COPD-B), 22 COPD patients with prevalent emphysema (COPD-E), 9 control smokers (CSs), and 18 control nonsmokers (CNSs), we analyzed the expression levels of interleukin (IL)-1α, IL-1β, IL-2, IL-4, IL-6, IL-8, IL-10, tumor necrosis factor (TNF)-α, interferon (IFN)-γ, epidermal growth factor (EGF), monocyte chemotactic protein (MCP)-1, and vascular endothelial growth factor by enzyme-linked immunosorbent assay in plasma/serum; glutathione peroxidase and superoxide dismutase (SOD)-1 by immunochemical kits in plasma; and free F2-isoprostanes (F2-IsoPs) by gas chromatography in plasma.
Results
F2-IsoPs level was increased in COPD-B and COPD-E compared with CSs and CNSs; in addition, CS showed higher levels than CNSs; SOD1 level was lower in COPD-B and COPD-E than that in CNSs. Interestingly, MCP-1 level was higher only in COPD-E versus CSs and CNSs; EGF and IL-8 levels were higher in COPD-B and COPD-E versus CNSs; IL-6 level was increased in all three smoking groups (COPD-B, COPD-E, and CSs) versus CNS; IFN-γ and IL-1α levels were higher in CSs than in CNSs; and IL-1α level was also higher in CSs versus COPD-B and COPD-E. In all subjects, F2-IsoPs level correlated positively and significantly with MCP-1, IL-2, IL-1β, IFN-γ, and TNF-α and negatively with SOD1. When correlations were restricted to COPD-E and COPD-B groups, F2-IsoPs maintained the positive associations with IFN-γ, TNF-α, and IL-2.
Conclusion
We did not find any specific blood biomarkers that could differentiate COPD patients with prevalent airway disease from those with prevalent emphysema. The MCP-1 increase in COPD-E, associated with the imbalance of oxidant/antioxidant markers, may play a role in inducing emphysema.
Introduction
Chronic obstructive pulmonary disease (COPD) is characterized by poor reversible airflow limitation caused by varying combinations of bronchial airway disease and lung parenchymal emphysema.Citation1 The identification of blood biomarkers, particularly for emphysema, which could assess this heterogeneity may help to manage and treat patients with COPD.Citation1 The analysis of peripheral blood samples is considered a valid method for monitoring inflammatory biomarkers,Citation2 in addition to being easily available.
Smoking induces a significant increase of monocyte chemotactic protein (MCP)-1 levels in the bronchoalveolar lavage (BAL) fluid of both healthy smokersCitation3 and patients with chronic bronchitis,Citation4 and COPD patients show higher plasma MCP-1 levels compared with healthy controls.Citation5 However, MCP-1 plasma levels have not been analyzed according to the different COPD phenotypes. Both interleukin (IL)-1α and IL-1β are proinflammatory cytokines produced mainly by monocytes, macrophages, and fibroblasts.Citation6,Citation7 There are increased levels of IL-1β in serum, sputum, and BAL in patients with stable COPD.Citation8,Citation9 There is evidence that inflammation in COPD is characterized by an increase in the levels of IL-6, IL-8, and tumor necrosis factor (TNF)-α in the peripheral blood.Citation10 IL-8 is a chemotactic factor for neutrophils. Levels increase in induced sputum of COPD patients as the number of exacerbations increases.Citation11 The proinflammatory cytokine IL-6 may play an important role in the progression of COPD severity,Citation12 and increased serum levels of IL-6 during COPD exacerbations have been described.Citation13 However, comorbidities may influence the IL-6 plasma level increase.Citation14 TNF-α is an important chemotactic protein for neutrophils, and its increase in the blood of COPD patients may induce an increased expression of adhesion molecules. Increased circulating TNF-α might also be the cause of skeletal muscle cell apoptosis (muscle cachexia) in COPD patients.Citation15,Citation16 IL-2 is necessary for the differentiation and expansion of T lymphocytes. Its serum levels were higher in patients with stable disease compared with patients with progressive COPD.Citation17 IL-4, a pleiotropic cytokine, produced by activated T cells, can facilitate the differentiation of both mucus-secreting tissueCitation18,Citation19 and B lymphocytes.Citation20 Interferon (IFN)-γ is produced by Th1 lymphocytes and is an essential component of the host immune responses to pathogens.Citation21 All COPD exacerbations are characterized by increased plasma levels of vascular endothelial growth factor (VEGF), which is a signal protein that stimulates vasculogenesis and angiogenesis. Increased plasma levels of IL-10, an anti-inflammatory cytokine, are found when COPD exacerbations are induced by virus.Citation22 Epidermal growth factor (EGF) stimulates human airway smooth muscle proliferation.Citation23 An increased EGF expression is reported in the epithelium and submucosal cells of patients with chronic bronchitis.Citation24
Among the oxidant and antioxidant markers, the super-oxide dismutase (SOD)-1 family contains enzymes that catalyze the dismutation (or partitioning) of the superoxide (O2−) radical into either ordinary molecular oxygen (O2) or hydrogen peroxide (H2O2). Glutathione peroxidase (GPx) reduces lipid hydroperoxides to their corresponding alcohols and reduces free H2O2 to water. An increase in GPx and SOD activities has been found during exacerbations of COPD compared with stable disease.Citation25 In addition, there are F2-isoprostanes (F2-IsoPs), which are prostaglandin-like compounds formed by the free radical-mediated oxidation of arachidonic acid.Citation26 They are a fundamental marker for measuring oxidative stress in the body. F2-IsoPs also have potent biological effects associated with inflammation and therefore may mediate chronic disease initiation and progression. In particular, 8-iso prostaglandin F2 (PGF2),Citation27 an isomer of the PGF2 family (F2-IsoPs) also known as iPF2α-III, is a stimulating factor for pulmonary vascular and bronchial smooth muscle contraction.Citation28,Citation29 This suggests that this isoprostane may be a local marker of airway inflammation caused by oxidant injury. Again, a comparison of these oxidant and antioxidant markers between different phenotypes of COPD has not yet been performed.
The aim of this study was, therefore, to analyze some relevant inflammatory, oxidant, and antioxidant molecules present in different phenotypes of COPD patients showing prevalent airway disease versus prevalent emphysema.
Patients and methods
Subjects
All COPD and healthy control subjects included in this study were recruited from the Respiratory Medicine Unit of Istituti Clinici Scientifici Maugeri (Pavia, Italy). In COPD patients, the severity of the airflow obstruction was staged using the current Global Initiative for Chronic Obstructive Lung Disease criteria.Citation1 All former smokers had stopped smoking for at least 1 year prior to the study. The phenotypic attribution of each patient (prevalent airway disease versus prevalent emphysema) was based on clinical and instrumental data.Citation30,Citation31 According to this model, a score >0.56 corresponded to the emphysema phenotype and <0.56 corresponded to the prevalent airway disease phenotype. The group of patients with prevalent airway disease also suffered from chronic bronchitis. Chronic bronchitis was defined by the presence of cough and sputum production for at least 3 months in each of the 2 years prior to enrollment.Citation1 By definition, chronic bronchitis was not present in the group of COPD patients with prevalent emphysema. Control smokers (CSs) and control nonsmokers (CNSs) were recruited as volunteers. None of the patients were treated with theophylline, roflumilast, antibiotics, antioxidants, mucolytics, and/or glucocorticoids in the month prior to the collection of blood samples. All the patients were in a stable phase of the disease and had been free from any episode of exacerbation for at least 3 months. They were all on regular treatment with bronchodilators according to the prescription of the referring physician. summarizes the clinical details and functional data of the subjects.
Table 1 Clinical characteristics of COPD patients by phenotype and control subjects who provided blood samples
Ethical approval
Written informed consent was obtained from each participant prior to the study. The study was carried out in conformity with the 1975 Declaration of Helsinki, according to the local ethics committee guidelines, and it was approved by the Ethics Committee of the Istituti Clinici Scientifici Maugeri of Pavia (formerly, Fondazione Salvatore Maugeri, Istituto di Ricovero e Cura a Carattere Scientifico [IRCCS]; ethical committee number: 966).
Lung function tests and volumes
Pulmonary function tests were performed as previously describedCitation32 according to the guideline recommendations.Citation33 Pulmonary function tests included measurements of forced expiratory volume in 1 second (FEV1; L), FEV1%, FEV1/forced vital capacity (FVC; %), residual volume (RV), RV%, diffusing capacity of the lungs for carbon monoxide (DLCO), DLCO%, and the number of exacerbations/year under baseline conditions in all the subjects examined (V6200 Autobox Pulmonary Function Laboratory; SensorMedics, Yorba Linda, CA, USA; ).
Blood/serum collection and analysis
Blood samples were collected in Vacutainer® tubes (Becton Dickinson, Plymouth, UK) within 1 week after the diagnosis and spirometry evaluations. For serum preparation, venous blood was immediately centrifuged at 3,000 g for 15 minutes at 4°C. Serum was separated and stored in aliquots at −20°C until analysis.
Measurement of blood biomarkers
Serum cytokines and growth factors
The following cytokines and growth factors were determined: IL-1α, IL-1β, IL-2, IL-4, IL-6, IL-8, IL-10, TNF-α, INF-γ, EGF, MCP-1, and VEGF. All these analyses were included in a single panel analyzed and quantified with Evidence Investigator, a high-throughput automated biochip immunoassay system (Randox Laboratories, Crumlin, UK). The biochip used consisted of a 9×9 mm substrate on which discrete test regions have been constructed. The binding ligands (antibodies) were attached to predefined sites on the chemically modified surface of the biochip. After the enzyme-linked immunosorbent assay procedure, each spot is imaged to capture the chemiluminescent signals generated at them on the array. The light signal is captured by a charge-coupled device camera as part of an imaging station and converted by image-processing software to provide results compared with calibration curves for each location on the biochip. The use of this protein array technologyCitation34 has advantages over conventional assay methods that include simultaneous detection of multiple analyses from a minute plasma sample within a single assay.
Blood antioxidant enzymes – GPx1 and SOD1
The quantitative determination of GPx1 in whole blood was performed using a commercial immunochemical kit (RANSEL; Randox Laboratories). Briefly, the heparinized whole blood was diluted with 1 mL of diluting agent and incubated for 5 minutes. After incubation, 1 mL of hemoglobin reagent (cyanide) was added in order to avoid falsely elevated results due to the presence of endogenous peroxidases. Finally, the samples were assayed within 20 minutes using an automated analyzer (BT2000; Biotecnica Instruments, Limena, Italy). The quantitative determination of SOD1 in whole blood was performed using a commercial immunochemical kit (RANSOD; Randox Laboratories). Briefly, 0.5 mL of heparinized whole blood samples was centrifuged for 10 minutes at 3,000 rpm in order to carefully wash the erythrocytes. Then, the erythrocytes were washed four times with 0.9% NaCl solution and centrifuged for 10 minutes at 3,000 rpm after each wash. Subsequently, the erythrocytes were made up to 2.0 mL with cold redistilled water, mixed, and left to stand at +4°C for 15 minutes. Finally, the lysate was diluted with sample diluent and assayed immediately using an automated analyzer (BT2000; Biotecnica Instruments) according to the manufacturer’s instructions.
Plasma oxidative stress markers – free F2-IsoPs
Blood was collected in heparinized tubes, and then blood samples were centrifuged at 2,400 g for 15 minutes at 4°C; the platelet-poor plasma was saved, and the buffy coat was removed by aspiration. Plasma samples were stored at −20°C until analyzed. Free F2-IsoPs were determined by gas chromatography/negative-ion chemical ionization tandem mass spectrometry (GC/NICI-MS/MS) in samples, as described by Signorini et al.Citation35,Citation36 In previous studies,Citation35–Citation39 GC/NICI-MS/MS has proved to be a reliable procedure (in terms of specificity, repeatability, and accuracy) to assess F2-IsoPs as an indicator of free radical-induced lipid peroxidation. For plasma-free F2-IsoPs determination, butylated hydroxytoluene (90 μM) was added to the plasma as an antioxidant. An aliquot of plasma (1 mL) was spiked with tetradeuterated PGF2α (PGF2α-d4. 500 pg in 50 μL of ethanol; Cayman, Ann Arbor, MI, USA), as an internal standard. After acidification, by the addition of 2 mL of acidified water (pH =3), the extraction and purification procedure was carried out. It consisted of two solid-phase separation steps: an octadecylsilane (C18) cartridge followed by an aminopropyl (NH2) cartridge (Waters, Milford, MA, USA).Citation35 A derivatization step followed the solid-phase extraction. The carboxylic group was derived as the pentafluorobenzyl ester, whereas the hydroxyl groups were converted to trimethylsilyl ethers. In the GC/NICI-MS/MS analysis, the measured ions were the product ions at m/z of 299 and 303 derived from the [M−181]-precursor ions (m/z =569 and m/z =573) produced from 15-F2t-IsoPs, the most represented F2-IsoP isomer, and the tetradeuterated derivative of the PGF2α-d4, respectively.Citation35 Plasma-free F2-IsoPs were expressed as picograms per milliliter. The calibration curve correlations were adequate (rCitation2=0.994); accuracy was 97.8%, and the variability coefficient was 2.5. The minimum detection limit was 5 pg/mL.
Statistical analysis
Continuous data were expressed as mean ± standard deviation (SD). Biomarkers were expressed as median (range). Analysis of variance (ANOVA) and unpaired t-tests were applied for functional data. The Kruskal–Wallis test followed by Mann–Whitney U tests was applied for nonparametric parameters to compare all groups; p-values <0.05 were considered as significant. All calculations were performed using the StatView® (1992–1998 Version 5.0.1; SAS Institute Inc., Cary, NC, USA).
Results
Clinical characteristics of subjects
We studied blood serum biomarkers from 72 subjects: 45 with stable COPD, 9 CSs with normal lung function, and 18 nonsmokers with normal lung function (). COPD patients were divided into two groups by phenotype: COPD patients with prevalent airway disease (COPD-B group; n=23) and COPD patients with prevalent emphysema (COPD-E group; n=22) as stated in the “Methods” section, following cutoff values previously defined.Citation30 The smoking history did not differ significantly between the three smoking groups. COPD-B and COPD-E groups had similar age (mean ± SD: 73.78±5.87 and 71.77±5.56, respectively), and both differed from CSs (54.85±8.29, p<0.01) and CNSs (49.28±7.56, p<0.01). Values of FEV1, RVs (L and %), and FEV1/FVC (%) in each COPD group differed significantly from both control groups (healthy smokers and healthy nonsmokers). No significant differences were observed for functional parameters (FEV1, FEV1/FVC (%), RV, and DLCO), 6-minute walking test (6MWD), or numbers of exacerbations/year between the two COPD groups (B and E; ).
Cytokines, growth factors, antioxidant enzymes, and oxidative stress markers in the blood
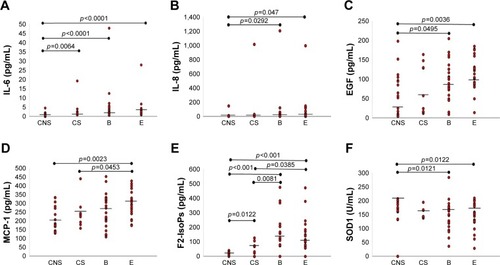
Serum levels of IL-1β, IL-2, IL-4, IL-10, TNF-α, VEGF, and GPx1 did not differ significantly in the four groups (). IL-1α was significantly lower in COPD-B (p=0.0119), COPD-E (p=0.0408), and CNSs (p=0.0064) compared with CSs ( and ). IL-6 levels were significantly higher in COPD-B (p<0.0001), COPD-E (p<0.0001), and CSs (p=0.0064) compared with CNSs ( and ; ). IL-8 was significantly higher in COPD-B (p=0.0292) and COPD-E (p=0.0047) compared with CNSs ( and ; ). IFN-γ levels were significantly higher in CSs (p=0.0206) compared with CNSs ( and ). EGF levels were significantly higher in COPD-B (p=0.0459) and COPD-E (p=0.0036) than in CNSs ( and ; ). Interestingly, MCP-1 levels were significantly increased only in COPD-E compared with CSs and CNSs (p=0.0453 and 0.0023, respectively; and ; ). SOD1 levels were significantly lower in COPD-B (p=0.0121) and COPD-E (p=0.0122) compared with CNSs ( and ; ). F2-IsoPs levels were significantly increased in COPD-B (p=0.0081 and <0.0001, respectively) and COPD-E (p=0.0385 and <0.0001, respectively) compared with both CSs and CNSs; CSs (p=0.0122) also showed increased F2-IsoPs levels compared with CNSs ( and ; ).
Table 2 Quantification of molecules related to oxidative stress and cytokines in the blood
Table 3 Statistical analysis between groups regarding the oxidative stress molecules and cytokines reported in
Figure 1 IL-6 is significantly increased in the blood of COPD patients with prevalent emphysema (E group), prevalent airway disease (B group), and CSs compared with CNSs (A); IL-8 is significantly increased in COPD-E and COPD-B compared with CNSs (B); EGF is significantly increased in COPD patients from COPD-E and COPD-B groups compared with CNSs (C); MCP-1 is significantly increased in COPD-E compared with CSs and CNSs (D); SOD-1 is significantly decreased in COPD-E and COPD-B compared with CNSs (E); F2-IsoPs is significantly increased in both COPD-B and COPD-E groups compared with CSs and CNSs, and CSs also showed higher levels compared with CNSs (F). Bar lines represent median values.
Abbreviations: CNS, control nonsmoker; COPD, chronic obstructive pulmonary disease; CS, control smoker; EGF, epidermal growth factor; F2-IsoPs, F2-isoprostanes; IL, interleukin; MCP, macrophage chemotactic protein; SOD, superoxide dismutase.
Correlations between oxidative stress markers and markers of inflammation or functional parameters
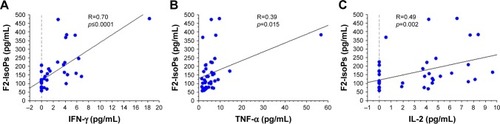
In the overall study population (patients and control subjects), the levels of F2-IsoPs oxidant marker correlated signifi-cantly and positively with the levels of circulating MCP-1 (R=0.30, p=0.014), IL-2 (R=0.33, p=0.008), IL-1β (R=0.34, p=0.005), IFN-γ (R=0.48, p=0.0001), and TNF-α (R=0.44, p=0.0004; , respectively). Interestingly, F2-IsoPs levels also correlated inversely with SOD1 levels in the blood (R=−0.41, p=0.0001; ). Considering the COPD patients alone (B+E), F2-IsoPs levels in the blood correlated significantly and positively with IFN-γ levels (R=0.70, p<0.0001), TNF-α (R=0.39, p=0.015), and IL-2 (R=0.49, p=0.002; , respectively). All the R and p-values were maintained after exclusion of the outlier case: , R=0.459, p=0.0003; , R=0.413, p=0.0010; , R=−0.394, p=0.0019; , R=0.679, p<0.0001; , R=0.344, p=0.0338. No other significant correlations were observed between blood–blood biomarkers or blood versus functional data.
Figure 2 Regression analysis performed in all COPD patients (COPD-E and COPD-B groups) and CS and CNS groups showing correlations between F2-IsoPs and MCP-1 (A), IL-2 (B), IL-1β (C), IFN-γ (D), TNF-α (E), and SOD1 (F). All inflammatory molecules correlated positively and significantly with the oxidative stress marker F2-IsoPs. SOD1 correlated inversely and significantly with the oxidative stress marker F2-IsoPs.
Note: COPD-B, COPD patients with prevalent airway disease; COPD-E, COPD patients with prevalent emphysema.
Abbreviations: CNS, control nonsmoker; COPD, chronic obstructive pulmonary disease; CS, control smoker; F2-IsoPs, F2-isoprostanes; IFN, interferon; IL, interleukin; MCP, macrophage chemotactic protein; SOD, superoxide dismutase; TNF-α, tumor necrosis factor-α.
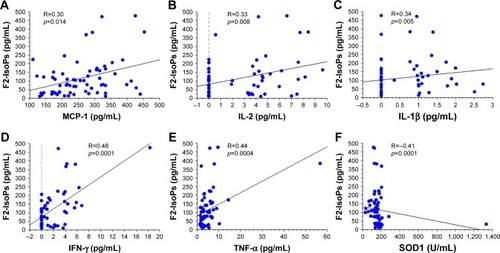
Figure 3 Regression analysis performed in all COPD patients (COPD-E and COPD-B groups) showing correlations between F2-IsoPs and IFN-γ (A), TNF-α (B), and IL-2 (C). All inflammatory molecules correlated positively and significantly with the oxidative stress marker F2-IsoPs.
Abbreviations: COPD, chronic obstructive pulmonary disease; F2-IsoPs, F2-isoprostanes; IFN, interferon; IL, interleukin; TNF, tumor necrosis factor.
Discussion
We have shown in this study that there is an increase in the oxidative stress marker F2-IsoPs and that there is a decrease in the antioxidant SOD1 in the blood of COPD patients, including those with prevalent airway disease and those with prevalent emphysema, compared with CNSs. A parallel increase in the inflammatory IL-6 and IL-8 and an increase in the remodeling marker EGF were also observed in these patients. MCP-1 selectively increased in the subgroup of patients with prevalent emphysema when compared to CNSs. In COPD patients, F2-IsoPs correlated positively with selected inflammatory markers.
Previous studies have shown higher plasma MCP-1 levels in COPD patients compared with healthy controlsCitation4 and greater concentrations of inflammatory cells together with higher levels of IL-1β, IL-6, IL-8, and MCP-1 in smokers compared with nonsmokers.Citation2 However, these studies are only partially comparable with ours since we studied MCP-1 blood levels and inflammatory cytokines in two different phenotypes of COPD and compared them with both CSs and CNSs. Furthermore, 69% of our COPD patients were ex-smokers (quit smoking since at least 1 year). Interestingly, as an extension of a previous study,Citation4 we observed that the MCP-1 level in the blood was significantly increased in the subgroup of COPD patients with prevalent emphysema, suggesting a potential role for this molecule underlying the lung alterations related to this phenotype of COPD. In line with this notion, increased inflammation was reported in the lung parenchyma and alveolar spaces of patients with severe emphysema compared with patients with milder forms of disease.Citation40 However, we could not evaluate the role played by smoking habit in relation to blood biomarkers expression in our patients because of the lack of recent smoking exposure of the majority of our COPD patients (69% of patients equally distributed between B and E groups were ex-smokers since 1 year).
In blood samples, SOD1 levels have been found to be higher in lung cancer (LC)–COPD patients compared with LC patients alone or control subjects;Citation41 conversely, no significant changes in SOD1 genotype frequencies were found between COPD patients and CSs.Citation42 Exhaled 8-isoprostane concentrations were increased in COPD patients compared with healthy smokers and healthy nonsmokers,Citation43 and F2-IsoPs were considered central in the pathogenesis of COPD.Citation44 We observed a clear imbalance between blood F2-IsoPs and SOD1 in both groups of COPD patients (B and E), showing an increase in the oxidant marker, F2-IsoPs, and a decrease in SOD1 compared with CNSs. This finding seems to apply to all COPD patients irrespective of the degree of prevalent airway disease or lung emphysema. Interestingly, the oxidant molecule, F2-IsoPs, was positively correlated with the inflammatory markers of systemic inflammation (MCP-1, IL-2, IL-1β, IFN-γ, and TNF-α) and inversely correlated with SOD1 blood levels in all subjects, reinforcing the notion of a potential relationship between oxidant burden increase and related inflammation, on the one side, and decreased lung protection, on the other.
The blood glutathione peroxidase activity has been reported to be decreased in COPD patients compared with CNSs,Citation45 and this decrease was particularly significant in severe COPD compared with mild disease.Citation46 An increase in antioxidant defenses during exacerbations of COPD has also been reported.Citation25 We did not observe any significant variation in GPx1 levels in our COPD patients with prevalent airway disease or prevalent emphysema compared with CSs or CNSs. This apparent discrepancy may be due in part to the mild/moderate disease state of our patients and also to the different patient stratification (B and E groups) used in the present study.
In a study of COPD patients with increasing disease severity, the level of heparin-binding EGF was increased compared with control subjects.Citation47 In another study, comparing subjects with and without computed tomography-detected emphysema and the absence of bronchial obstruction, a significant reduction in EGF blood levels was observed in the emphysema group.Citation48 These studies are poorly comparable with each other and with our present work on account of significant differences in the COPD patients grouping; however, our observation of increased EGF blood levels in both COPD (B and E) subgroups in comparison with CNSs confirms in part Cockayne et al’s study resultsCitation47 and supports the notion of an involvement of remodeling biomarkers in COPD, particularly in the presence of bronchial obstruction.
In line with previous studies,Citation49 we confirmed increased levels of IL-6 and IL-8 in the blood of COPD patients compared with CNSs, markers that have also been associated with progressive airflow obstruction (IL-6) and progressive emphysema (IL-6 and IL-8).Citation50
IL-2 has been reported to be increased in COPD patients compared with controls,Citation50 but was lower in rapid decliners compared with stable COPD patients.Citation51 IL-10 in the blood of COPD patients was reported as increased in one study,Citation50 but in another study, it did not differ in COPD patients compared with controls.Citation52 IL-2 and IL-10 as well as IFN-γ and TNF-α were not reported to be associated with the progression of emphysema.Citation50 In our present study, the levels of IL-2 and IL-10 as well as IFN-γ and TNF-α in the two COPD (B and E) groups were not different with respect to CSs and CNSs, suggesting a relatively modest role for these blood biomarkers in the endotyping of our COPD groups.
In a recent study, biomass smoking COPD patients showed higher levels of Th2 cells and serum IL-4 compared with tobacco-smoking COPD patients.Citation20 In agreement, we did not find any significant difference in the blood IL-4 measurements when comparing smokers and ex-smokers from the COPD groups (B and E) to control subjects, suggesting again a minor role for this circulating cytokine in the endotyping of COPD patients.
VEGF serum levels have been variously reported as proportionally increased in COPD patients with increasing disease severityCitation53 compared with control subjects, or not changed in either stable or exacerbated COPD when the association with clinically significant outcomes was studied.Citation54 We did not find any significant changes in VEGF levels when comparing the COPD-B and COPD-E groups with CSs and CNSs, suggesting again that this remodeling biomarker does not seem to play a significant role in COPD endotyping.
In mice, cigarette smoke-induced neutrophilia is dependent on IL-1α,Citation55 and mice smoke exposure leads to increased recruitment and activation of dendritic cells.Citation56 Airway epithelial cells-derived IL-1α increased upon epithelial exposure to cigarette smoke extract.Citation57 In our study, we found the highest IL-1α blood values in smokers compared both with CNSs and with the two COPD groups (B and E), suggesting that it is the smoking habit, more than the disease state, that most influences the blood level of this cytokine.
Plasma levels of IL-1β have been reported as increased in smokers with COPD compared with CSsCitation49 or CNSs,Citation58 and sputum gene expression of IL-1β at baseline was higher in frequent exacerbators with COPD.Citation59 In bronchial and lung tissue, IL-1β immunoexpression was found to be very low, and it was similar in COPD patients and control subjects.Citation60 In our present study, we did not find significant differences in IL-1β blood levels when COPD-B and COPD-E groups were compared with CSs or CNSs. This may be due to the stable state of the disease of our patients and, in part, to the different stratification method used for grouping of our COPD patients. As a limitation of this study, we did not establish cutoff values for each one of the biomarkers studied for COPD-B and COPD-E groups, related to CNSs. This was due to the relatively low number of patients studied.
Conclusion
We did not find any specific blood biomarkers that could differentiate COPD patients with prevalent airway disease from those with prevalent emphysema. Studies sampling directly the target organ by bronchial biopsy, BAL, or sputum investigations are warranted to further characterize these COPD phenotypes.
Acknowledgments
This study was supported by Istituti Clinici Scientifici Maugeri, IRCCS, Ricerca Corrente.
Disclosure
The authors report no conflicts of interest in this work.
References
- VestboJHurdSSAgustiAGGlobal strategy for the diagnosis, management and prevention of chronic obstructive pulmonary disease: GOLD executive summaryAm J Respir Crit Care Med2013187434736522878278
- ReubenDBChehAIHarrisTBPeripheral blood markers of inflammation predict mortality and functional decline in high-functioning community-dwelling older personsJ Am Geriatr Soc200250463864411982663
- KuschnerWGD’AlessandroAWongHBlancPDDose-dependent cigarette smoking-related inflammatory responses in healthy adultsEur Respir J1996910198919948902455
- CapelliADi StefanoAGnemmiIIncreased MCP-1 and MIP-1beta in bronchoalveolar lavage fluid of chronic bronchitisEur Respir J199914116016510489845
- LiuSFWangCCFangWFChenYCLinMCMCP1-2518 polymorphism and chronic obstructive pulmonary disease in Taiwanese menExp Lung Res201036527728320497022
- LordPCWilmothLMMizelSBMcCallCEExpression of interleukin-1 alpha and beta genes by human blood polymorphonuclear leukocytesJ Clin Invest1991874131213212010544
- RosenwasserLJBiologic activities of IL-1 and its role in human diseaseJ Allergy Clin Immunol199810233443509768571
- FerhaniNLetuveSKozhichAExpression of high-mobility group box 1 and of receptor for advanced glycation end products in chronic obstructive pulmonary diseaseAm J Respir Crit Care Med2010181991792720133931
- SinghBAroraSKhannaVAssociation of severity of COPD with IgE and interleukin-1 betaMonaldi Arch Chest Dis2010732868720949775
- TanniSEPelegrinoNRAngeleliAYCorreaCGodoyISmoking status and tumor necrosis factor-alpha mediated systemic inflammation in COPD patientsJ Inflamm (Lond)201072920534161
- WedzichaJASeemungalTAMacCallumPKAcute exacerbations of chronic obstructive pulmonary disease are accompanied by elevations of plasma fibrinogen and serum IL-6 levelsThromb Haemost200084221021510959691
- CosioMGSaettaMAgustiAImmunologic aspects of chronic obstructive pulmonary diseaseN Engl J Med2009360232445245419494220
- SeemungalTHarper-OwenRBhowmikARespiratory viruses, symptoms, and inflammatory markers in acute exacerbations and stable chronic obstructive pulmonary diseaseAm J Respir Crit Care Med200116491618162311719299
- VanfleterenLESpruitMAGroenenMClusters of comorbidities based on validated objective measurements and systemic inflammation in patients with chronic obstructive pulmonary diseaseAm J Respir Crit Care Med2013187772873523392440
- BarnesPJCytokine-directed therapies for the treatment of chronic airway diseasesCytokine Growth Factor Rev200314651152214563353
- LewisMIApoptosis as a potential mechanism of muscle cachexia in chronic obstructive pulmonary diseaseAm J Respir Crit Care Med2002166443443612186814
- PaoneGLeoneVContiVBlood and sputum biomarkers in COPD and asthma: a reviewEur Rev Med Pharmacol Sci201620469870826957273
- TemannUAPrasadBGallupMWA novel role for murine IL-4 in vivo: induction of MUC5AC gene expression and mucin hypersecretionAm J Respir Cell Mol Biol19971644714789115759
- DabbaghKTakeyamaKLeeHMUekiIFLausierJANadelJAIL-4 induces mucin gene expression and goblet cell metaplasia in vitro and in vivoJ Immunol1999162106233623710229869
- Solleiro-VillavicencioHQuintana-CarrilloRFalfán-ValenciaRVargas-RojasMIChronic obstructive pulmonary disease induced by exposure to biomass smoke is associated with a Th2 cytokine production profileClin Immunol2015161215015526220216
- SchoenbornJRWilsonCBRegulation of interferon-gamma during innate and adaptive immune responsesAdv Immunol2007964110117981204
- AlmansaRSanchez-GarciaMHerreroAHost response cytokine signatures in viral and nonviral acute exacerbations of chronic obstructive pulmonary diseaseJ Interferon Cytokine Res201131540941321235417
- HirstSJBarnesPJTwortCHQuantifying proliferation of cultured human and rabbit airway smooth muscle cells in response to serum and platelet derived growth factorAm J Respir Cell Mol Biol1992765745811449805
- VignolaAMChanezPChiapparaGTransforming growth factor-b expression in mucosal biopsies in asthma and chronic bronchitisAm J Respir Crit Care Med19971562 Pt 15915999279245
- SadowskaAMLuytenCVintsAMVerbraeckenJVan RanstDDe BackerWASystemic antioxidant defences during acute exacerbation of chronic obstructive pulmonary diseaseRespirology200611674174717052302
- MusiekESMorrowJDF2-isoprostanes as markers of oxidant stress: an overviewCurr Protoc Toxicol2005 Chapter 17:Unit 17.5
- RokachJKhanapureSPHwangSWAdiyamanMLawsonJAFitzGeraldGANomenclature of isoprostanes: a proposalProstaglandins19975468538739533181
- BanerjeeMKangKHMorrowJDRobertsLJNewmanJHEffects of a novel prostaglandin, 8-epi PGF2 alpha, in rabbit lung in situAm J Physiol19922633 Pt 2H660H6631415588
- KawikovaIBarnesPJTakasakiTTadjkarimiSYacoubMHBelvisMG8-epi prostaglandin F2a, a novel noncyclooxygenase derived prostaglandin, constricts airways in vitroAm J Respir Crit Care Med19961535905968564103
- PistolesiMCamiciottoliGPaolettiMIdentification of a predominant COPD phenotype in clinical practiceRespir Med2008102336737618248806
- CamiciottoliGBigazziFPaolettiMCestelliLLavoriniFPistolesiMPulmonary function and sputum characteristics predict computed tomography phenotype and severity of COPDEur Respir J201342362663523258785
- Di StefanoACaramoriGGnemmiIAssociation of increased CCL5 and CXCL7 chemokine expression with neutrophil activation in severe stable COPDThorax2009641196897519703829
- QuanjerPHTammelingGJCotesJEPedersenOFPeslinRYernaultJCLung volumes and forced ventilatory flows. Report Working Party Standardization of Lung Function Tests, European Community for Steel and Coal. Official Statement of the European Respiratory SocietyEur Respir J Suppl1993165408499054
- FitzGeraldSPLamontJVMcConnellRIBenchikh elODevelopment of a high-throughput automated analyzer using biochip array technologyClin Chem20055171165117615890889
- SignoriniCComportiMGiorgiGIon trap tandem mass spectrometric determination of F2-isoprostanesJ Mass Spectrom200338101067107414595856
- SignoriniCCiccoliLLeonciniSFree iron, total F-isoprostanes and total F-neuroprostanes in a model of neonatal hypoxic-ischemic encephalopathy: neuroprotective effect of melatoninJ Pineal Res200946214815419141088
- De FeliceCCiccoliLLeonciniSSystemic oxidative stress in classic Rett syndromeFree Radic Biol Med200947444044819464363
- SignoriniCPerroneSSgherriCPlasma esterified F2-isoprostanes and oxidative stress in newborns: role of nonprotein-bound ironPediatr Res200863328729118287967
- SofflerCCampbellVLHasselDMMeasurement of urinary F2-isoprostanes as markers of in vivo lipid peroxidation: a comparison of enzyme immunoassays with gas chromatography-mass spectrometry in domestic animal speciesJ Vet Diagn Invest201022220020920224077
- RetamalesIElliottWMMeshiBAmplification of inflammation in emphysema and its association with latent adenoviral infectionAm J Respir Crit Care Med2001164346947311500352
- Mateu-JiménezMSánchez-FontARodríguez-FusterARedox imbalance in lung cancer of patients with underlying chronic respiratory conditionsMol Med Epub201617
- YoungRPHopkinsRBlackPNFunctional variants of antioxidant genes in smokers with COPD and in those with normal lung functionThorax200661539439916467073
- MontuschiPCollinsJVCiabattoniGExhaled 8-isoprostane as an in vivo biomarker of lung oxidative stress in patients with COPD and healthy smokersAm J Respir Crit Care Med20001623 Pt 11175117710988150
- RolinSMasereelBDognéJMProstanoids as pharmacological targets in COPD and asthmaEur J Pharmacol20065331–38910016458293
- SantosMCOliveiraALViegas-CrespoAMSystemic markers of the redox balance in chronic obstructive pulmonary diseaseBiomarkers20049646146915849066
- KluchováZPetrásováDJoppaPDorkováZTkácováRThe association between oxidative stress and obstructive lung impairment in patients with COPDPhysiol Res2007561515616497100
- CockayneDAChengDTWaschkiBSystemic biomarkers of neutrophilic inflammation, tissue injury and repair in COPD patients with differing levels of disease severityPLoS One201276e3862922701684
- de-TorresJPBlancoDAlcaideABSmokers with CT detected emphysema and no airway obstruction have decreased plasma levels of EGF, IL-15, IL-8 and IL-1raPLoS One201384e6026023577098
- AgustiASinDDBiomarkers in COPDClin Chest Med201435113114124507841
- BradfordEJacobsonSVarastehJThe value of blood cytokines and chemokines in assessing COPDRespir Res201718118029065892
- D’ArmientoJMScharfSMRothMDEosinophil and T cell markers predict functional decline in COPD patientsRespir Res20091011319925666
- ZhangLChengZLiuWWuKExpression of interleukin (IL)-10, IL-17A and IL-22 in serum and sputum of stable chronic obstructive pulmonary disease patientsCOPD201310445946523537276
- Farid HosseiniRJabbari AzadFYousefzadehHSerum levels of vascular endothelial growth factor in chronic obstructive pulmonary diseaseMed J Islam Repub Iran20142885 eCollection 201425664286
- BoeckLMandalJCostaLRothMTammMStolzDLongitudinal measurement of serum vascular endothelial growth factor in patients with chronic obstructive pulmonary diseaseRespiration20159029710426066063
- NikotaJKShenPMorissetteMCCigarette smoke primes the pulmonary environment to IL-1α/CXCR-2-dependent nontypeable Haemophilus influenzae-exacerbated neutrophilia in miceJ Immunol201419363134314525092891
- BotelhoFMNikotaJKBauerCMCigarette smoke-induced accumulation of lung dendritic cells is interleukin-1α-dependent in miceRespir Res2012138122992200
- OseiETNoordhoekJAHackettTLInterleukin-1α drives the dysfunctional cross-talk of the airway epithelium and lung fibroblasts in COPDEur Respir J201648235936927418555
- SinghBAroraSKhannaVAssociation of severity of COPD with IgE and interleukin-1 betaMonaldi Arch Chest Dis2010732868720949775
- FuJJMcDonaldVMBainesKJGibsonPGAirway IL-1β and systemic inflammation as predictors of future exacerbation risk in asthma and COPDChest2015148361862925950204
- Di StefanoACaramoriGBarczykAInnate immunity but not NLRP3 inflammasome activation correlates with severity of stable COPDThorax201469651652424430176