
Abstract
Background
Inhaled corticosteroid use is associated with increased rates of pneumonia in COPD patients. The underlying mechanism is unknown, although recent data suggest that pneumonia is more frequent in patients treated with fluticasone propionate (FP) than budesonide. Macrophages and neutrophils from COPD patients are deficient in clearing bacteria, and this might explain increased bacterial colonization in COPD. Inhaled corticosteroid may further suppress this response; therefore, we examined the effect of FP and budesonide on phagocytosis of common respiratory pathogens by monocyte-derived macrophages (MDMs) and neutrophils.
Methods
MDMs from COPD patients (n=20–24) were preincubated with FP or budesonide for 1 or 18 hours, after which phagocytosis of fluorescently labeled inert beads or heat-killed Haemophilus influenzae/Streptococcus pneumoniae were measured fluorimetrically after 1 or 4 hours. Additionally, CXCL8, IL6, and TNFα concentrations in supernatants by ELISA, MDM-scavenger-receptor expression by flow cytometry, and MDM ability to kill bacteria were measured. Neutrophils from COPD patients (n=8) were preincubated with corticosteroids for 1 hour and bacteria phagocytosis measured by flow cytometry.
Results
After 1 hour’s preincubation, neither corticosteroid altered MDM phagocytosis of beads or H. influenzae; however, budesonide (10−7 M) increased S. pneumoniae phagocytosis by 23% (P<0.05). After 18 hours’ preincubation, neither corticosteroid altered MDM phagocytosis of any prey, although H. influenzae phagocytosis by budesonide was significantly greater compared to FP at 10−6 and 10−5 M (P<0.05). The 1-hour preincubation with either corticosteroid inhibited bacteria-induced CXCL8 release (at 10−7 and 10−5 M, P<0.05); however, this effect was lost at 18-hour preincubation. There was no change in receptor expression, bacterial killing, or neutrophil phagocytosis by either corticosteroid.
Conclusion
These data suggest that dissolved FP and budesonide do not have an overall effect on MDM or neutrophil phagocytosis of bacteria.
Introduction
Inhaled corticosteroids (ICSs) are now prescribed to >70% of patients with COPD.Citation1 ICSs used in COPD patients (mostly in combination inhalers with long-acting β2-adrenergic agonists [LABAs]) have been shown to improve patients’ symptoms and health status, reduce decline in FEV1, and decrease exacerbation rates.Citation2 These patients are predominantly prescribed ICSs such as fluticasone propionate (FP) or budesonide; however, randomized controlled trials have suggested that inhaled FP alone or in combination with the LABA salmeterol is associated with an increased rate of pneumonia.Citation3–Citation7 On the other hand, most double-blind, randomized controlled studies with budesonide treatment alone or in combination with the LABA formoterol reported no increased risk of pneumonia when compared with formoterol alone or placebo.Citation8 Furthermore, large observational, population-based studies in real-world, clinical practice with COPD patients have suggested a higher risk of pneumonia for therapy with FP than with budesonide.Citation9–Citation12 Similarly, a recent evaluation of meta-analyses that considered the risk of pneumonia related to treatment of COPD patients with FP or budesonide showed an association with FP causing a statistically significant increased risk of pneumonia, whereas budesonide showed no association.Citation13 This finding is of increased importance, as patients with COPD who are hospitalized with pneumonia have been shown to have increased mortality compared to those without COPD.Citation14,Citation15
It remains unclear why different ICSs have differential effects on the increased risk of pneumonia. One reason may be a greater suppression of macrophage and/or neutrophil functions mediated by FP, such as phagocytosis and/or bacterial killing. The immunosuppressant potency of FP can be up to tenfold greater than that of budesonide, as reported for in vitro inhibition of innate immunoresponse to bacterial triggers in human alveolar macrophages.Citation16 Furthermore, suppression of local immunity by FP in the airways/lung may be prolonged because inhaled FP resides for several hours in the airway lining fluid and mucus, most likely in the form of undissolved particles, which only dissolve slowly.Citation17,Citation18 This contrasts with budesonide, which is completely dissolved and absorbed into the airway tissue within a few minutes and thus quickly cleared from the airway lumen.Citation13,Citation17,Citation18 Additionally, the clearance of particulate FP by phagocytic mechanisms may lead to extremely high concentrations of the drug residing within the phagolysosomes, which may further impair phagocytosis/killing of bacteria, resulting in impaired/delayed bacterial clearance.
Alveolar macrophages play a major role in removal of potentially pathogenic microorganisms via phagocytosis and are essential for maintenance of the pulmonary environment.Citation19 One reason for the increased incidence of bacterial infections in the respiratory tract of COPD patients might be failure of macrophages to clear pathogens because of reduced phagocytosis, due to chronic activation.Citation20 We have shown that this defect can also be observed in macrophages obtained from blood-derived monocytes.Citation21 These monocyte-derived macrophages (MDMs) from patients with COPD exhibit reduced phagocytosis of both Gram-negative and Gram-positive bacteria, but not inert beads, thereby mimicking the effect observed in alveolar macrophages. A recent study in COPD patients has shown that long-term therapy with FP increased sputum bacterial load and relative abundance of Haemophilus influenzae and Streptococcus pneumoniae, the key bacteria involved in development of pneumonia, indicating a potential link between macrophage function and the effects of FP in COPD.Citation22
We hypothesized that the higher rates of pneumonia associated with FP compared to budesonide are caused by greater inhibition of macrophage or neutrophil function and defective clearance of bacteria. Therefore, the aim of the study was to investigate the phagocytic ability and immunoresponse of MDMs and neutrophils from COPD patients treated in vitro with FP or budesonide compared to drug-vehicle-treated control cells.
Methods
Subject selection
COPD subjects were recruited from the National Heart and Lung Institute, Royal Brompton Hospital, London (UK). All subjects gave written, informed consent as approved by the London–Chelsea NRES committee. Demographic data are presented in . All COPD subjects were clinically stable and had not experienced any exacerbations for at least 4 weeks prior to inclusion in the study. All were treated with ICSs.
Table 1 Demographics of COPD subjects
Cell culture
Monocytes were isolated from peripheral blood mononuclear cells using a Percoll gradient and adherence technique, followed by culture in 2 ng/mL granulocyte-macrophage colony-stimulating factor (R&D Systems, Minneapolis, MN, USA) for 12 days to generate MDMs as described previously.Citation21 Neutrophils were isolated from whole blood following sedimentation using 6% (w:v) dextran followed by Percoll density-gradient separation as reported previously.Citation23
Cell treatment
MDMs and neutrophils were left untreated or exposed to FP, budesonide, or 0.1% (v:v) dimethyl sulfoxide (DMSO; vehicle) for 1 hour or 18 hours prior to the addition of phagocytic prey and remained in the media throughout the experiment.
Bacterial culture and labeling for phagocytosis assays
Nontypeable H. influenzae strain 1479 and S. pneumoniae serotype 9 V strain 10,692 were cultured and heat-killed at 70°C for 2 hours. Bacteria were fluorescently labeled using Alexa Fluor 488 NHS ester (2 mg/mL in DMSO) in the dark at room temperature overnight. Labeled bacteria were washed repeatedly in PBS to remove unbound labeling, resuspended in PBS, and stored at −20°C.
Phagocytosis assays
Fluorescently labeled polystyrene beads or bacteria were added to cells and incubated for the times indicated. Cells were washed with PBS and extracellular particle fluorescence quenched by adding Trypan blue (2% w:v) for 1 minute. Excess fluid was removed and fluorescence determined using an excitation at 480 nm and emission 520 nm. The relative amount of bacteria phagocytosed is reported as relative fluorescent units (RFUs). Cell viability was measured using MTT assay. None of the treatments at any time of analysis had any effect on cell viability (Figure S1).
Cytokine analysis
ELISAs were performed to measure concentrations of TNFα, CXCL8, IL6, and IL10 in cell supernatants according to the manufacturer’s instructions (R&D Systems). The lower limit of detection for all cytokines was 31 pg/mL.
Scavenger-receptor analysis
After phagocytosis, cells were transferred to fluorescence- activated cell-sorting (FACS) tubes, washed, and resuspended in 4% (v:v) paraformaldehyde. Cells were blocked with 1% human serum, then washed and resuspended in FACS buffer (PBS +0.5% [w:v] BSA +0.05% [w:v] sodium azide). Cells were incubated for antibodies against TLR2 Alexa Fluor 647, TLR4-PE, CD36-APC, CD206-PE, and CD163-PeCy7, or for MARCO staining, anti-MARCO primary antibody, followed by IgG3 Alexa Fluor 488 secondary antibody, for 30 minutes on ice, washed, and resuspended in PBS. Receptor expression was analyzed on a FACS Canto II (BD, Franklin Lakes, NJ, USA). Cells were gated using fluorescence minus-one gating. The amount of given types of receptor being expressed was analyzed by median fluorescence intensity and the percentage of cells expressing individual receptors also reported. Gating strategy is shown in Figure S2.
Bacteria-killing assay
Live bacteria were washed twice in PBS and sonicated. Bacteria were added to cells and incubated on ice for 1 hour to allow adherence, followed by incubation at 37°C for 4 hours. Cells were washed in PBS to remove excess bacteria, and incubated in benzylpenicillin (40 µg/mL) and gentamicin (20 µg/mL) for 30 minutes to kill extracellular bacteria that had not been phagocytosed. Cells were washed three times in PBS to remove antibiotics, and then incubated in 2% (v:v) saponin for 12 minutes to lyse cells. Samples were diluted and spread onto agar plates (Columbia agar with chocolate horse blood for H. influenzae, blood agar base two with horse blood for S. pneumoniae) and cultured overnight at 37°C. The next day, colonies were counted.
Neutrophil-phagocytosis assay
Fluorescently labeled bacteria were added to neutrophils and incubated for the times indicated. Phagocytosis was stopped by adding 4% (w:v) paraformaldehyde and centrifugation of cells. Cells were resuspended in PBS and fluorescence assessed by flow cytometry. Data was analyzed using FlowJo software. Cell viability was measured using a Live/Dead cell-viability assay (Thermo Fisher Scientific, Waltham, MA, USA). The percentage of neutrophils that phagocytosed bacteria is expressed as percentage phagocytosis and the amount of phagocytosed bacteria expressed as median fluorescence intensity.
Statistical analysis
Data are shown as arithmetic mean ± SEM of independent donors. Statistical differences were determined using two-way repeated-measure ANOVA with post hoc testing. Values of P<0.05 were considered significant.
Results
Effect of corticosteroids on phagocytosis by macrophages
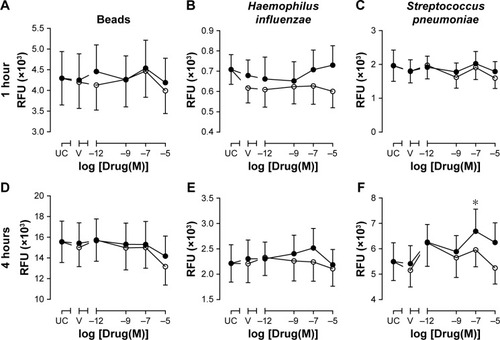
In order to determine whether Corticosteroids (CSs) altered MDM phagocytosis, a series of experiments were devised using both inert beads and two common respiratory pathogenic bacteria species associated with COPD: H. influenzae and S. pneumoniae. Firstly, MDMs were pretreated with FP or budesonide (or DMSO vehicle) for 1 hour to determine the acute effects of CSs on phagocytic response after 1 and 4 hours’ incubation with phagocytic prey. There were no significant effects of FP or budesonide (or drug vehicle) on phagocytosis of inert beads or bacteria after 1 hour’s incubation with phagocytic prey (). This was also the case after 4 hours’ incubation (), with the exception of 10−7 M budesonide, which significantly increased S. pneumoniae phagocytosis by 23% compared to vehicle control (P<0.05, ). This effect was not observed for the other concentrations of budesonide, and FP had no effect on S. pneumoniae phagocytosis. When the effects of the two CSs were compared, there was no statistically significant difference in phagocytosis at any drug concentration or for any prey (). None of the treatments used significantly altered the viability of MDMs (Figure S1).
Figure 1 Effects of 1 hour’s pretreatment with fluticasone propionate or budesonide on phagocytosis of beads or bacteria at 1 hour and 4 hours.
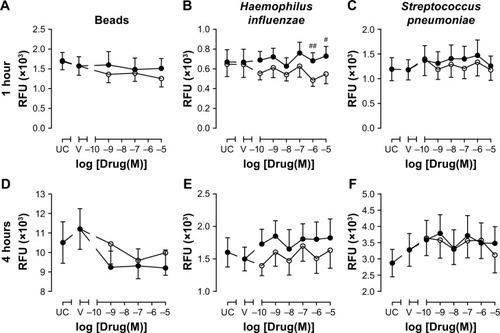
To determine the effects of chronic exposure to CSs, MDMs were pretreated with CSs for 18 hours. The phagocytic response of MDMs to inert beads or bacteria after 1 or 4 hours’ incubation was not significantly affected by pretreatment with budesonide or FP (), although a trend for approximately 20% increase of 4 hours phagocytosis of both H. influenzae and S. pneumoniae was observed for budesonide at the concentration range studied (). When the effects of CSs were compared with one another, there was a significant difference in 1-hour phagocytosis of H. influenzae between budesonide and FP at 10−6 M (40% difference, P<0.01) and 10−5 M (33% difference, P<0.05), showing a greater degree of H. influenzae phagocytosis after 18 hours’ pretreatment with budesonide than with FP at these two high concentrations (). None of the treatments used significantly altered the viability of MDMs (Figure S1).
Figure 2 Effects of 18 hours’ pretreatment with fluticasone propionate or budesonide on phagocytosis of beads or bacteria at 1 hour and 4 hours.
Effect of corticosteroids on bacteria-induced cytokine release
It is well known that CSs inhibit proinflammatory cytokine release by macrophages. In order to confirm that the concentrations of CSs used in these experiments were effective, CXCL8, IL6, TNFα, and IL10 were measured in cell supernatants after 1 or 4 hours’ phagocytosis of inert beads or bacteria. Cytokine concentrations in cell supernatants were not significantly affected after 1 hour’s incubation of macrophages with inert beads or bacteria (data not shown). After 4 hours, incubation of MDMs with H. influenzae or S. pneumoniae significantly induced CXCL8, IL6, and TNFα release from macrophages (). Incubation with inert beads had no significant effect on cytokine release. Levels of IL10 were consistently below the limit of detection for any treatment (data not shown). Pretreatment with CS vehicle (DMSO) had no effect on cytokine release (). Compared to vehicle control, pretreatment with FP or budesonide for 1 hour caused a nonsignificant trend for concentration-dependent inhibition of inert bead-induced CXCL8 () and IL6 release (), but not TNFα release (). Pretreatment with FP for 18 hours resulted in a similar trend for inert bead-induced CXCL8 release (), but not for IL6 () or TNFα release ().
Figure 3 Effects of 1 hour’s pretreatment with fluticasone propionate or budesonide on release of CXCL8, IL6, and TNFα induced by phagocytosis of beads or bacteria at 4 hours.
Notes: (A–C) Monocyte-derived macrophages from COPD patients (n=12) were left not treated (NT), or pretreated for 1 hour with drug vehicle (V) prior to incubation with fluorescently labeled beads, Haemophilus influenzae (HI), or Streptococcus pneumoniae (SP) bacteria for 4 hours. Supernatants were analyzed by ELISA for CXCL8 (A), IL6 (B), and TNFα (C) release. Data are mean ± SEM; **P<0.01, ***P<0.001 between no treated (NT) and treatment. (D–L) Monocyte-derived macrophages from COPD patients (n=12) were pretreated for 1 hour with fluticasone propionate (○) or budesonide (●) at indicated concentrations or drug vehicle (V) prior to incubation with fluorescently labeled beads or bacteria for 4 hours. Supernatants were analyzed by ELISA for CXCL8, IL6, and TNFα release. Data are percentage responses compared to vehicle control, expressed as mean ± SEM; *P<0.05, **P<0.01 between drugs and vehicle (V).
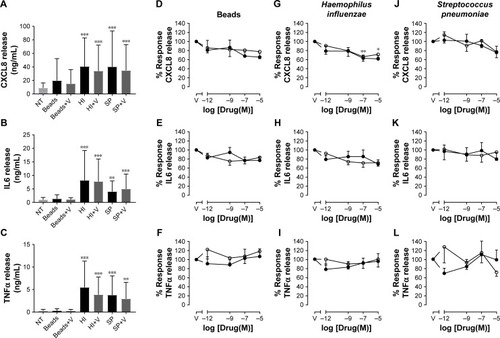
Figure 4 Effects of 18 hour's pretreatment with fluticasone propionate or budesonide on release of CXCL8, IL6, and TNFα induced by phagocytosis of beads or bacteria at 4 hours.
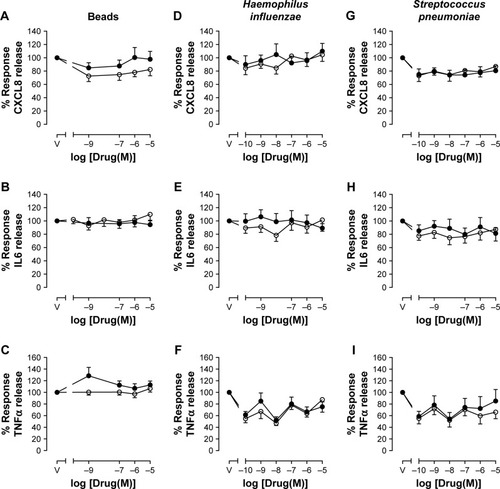
Compared to vehicle control, pretreatment with FP or budesonide for 1 hour caused a statistically significant concentration-dependent inhibition of CXCL8 release induced by H. influenzae, with maximal 34% inhibition by FP and 38% inhibition by budesonide (). A similar trend for approximately 30% maximal inhibition was seen for IL6 release (), but not for TNFα release (). These effects of 1 hour’s pretreatment with CSs on CXCL8 and IL6 release were lost after 18 hours’ pretreatment (). However, approximately 20%–40% inhibition of TNFα release induced by H. influenzae was observed after 18 hours’ pretreatment with FP or budesonide over the whole concentration range studied, although these effects were not statistically significant (). Compared to vehicle control, pretreatment with FP or budesonide for 1 or 18 hours had no significant effect on S. pneumoniae-induced CXCL8 ( and ), IL6 ( and ), or TNFα release ( and ), although a trend for approximately 20% inhibition was seen for all cytokines.
Effect of corticosteroids on macrophage-scavenger-receptor expression
In order to determine whether the effects of CSs on cytokine release were due to alterations in scavenger-receptor expression, CD36, CD206, CD163, TLR2, TLR4, and MARCO expression levels were analyzed on MDM surfaces after 4 hours’ exposure to phagocytic prey. Following phagocytosis of H. influenzae, the percentage of cells expressing TLR2 and TLR4 significantly increased five- to sixfold and seven- to tenfold, respectively, compared to untreated cells ( and S1), whereas there were no significant effects on the other receptors studied. There was no effect of S. pneumoniae phagocytosis on the percentage of cells expressing any of the receptors analyzed. MDM pretreatment for 1 or 18 hours with 10−5 M CSs did not significantly alter the percentage of cells expressing any of the receptors analyzed ( and S1). The number of receptors being expressed by each cell was not altered by bacteria or pretreatment with CSs when analyzed by median fluorescence intensity ( and S1).
Table 2 Effects of 1 hour’s pretreatment with fluticasone propionate or budesonide on scavenger-receptor expression
Effect of corticosteroids on bacterial killing by MDMs
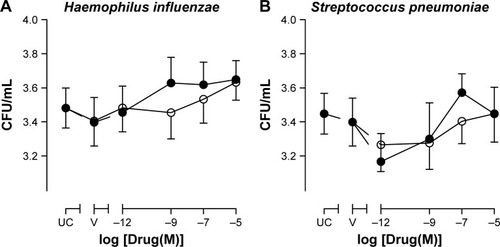
Phagocytosis of bacteria may not be sufficient to clear invading organisms from the site of infection, as macrophages must also kill the internalized bacteria. In order to determine whether the bactericidal role of MDMs was also affected by CSs, the ability of MDMs to kill bacteria was measured. Neither FP, budesonide, nor drug vehicle (DMSO) had any significant effect on the killing of H. influenzae or S. pneumoniae at 4 hours postinfection ().
Figure 5 Effects of fluticasone propionate or budesonide on intracellular killing of Haemophilus influenzae or Streptococcus pneumoniae by MDMs from COPD patients.
Abbreviation: MDMs, monocyte-derived macrophages.
Effect of corticosteroids on phagocytosis by neutrophils
In order to determine whether the effect of CSs was limited to macrophages or whether other phagocytic cells could also be affected, phagocytosis by neutrophils (isolated from peripheral blood of COPD subjects) pretreated with CSs was also studied. Pretreatment of neutrophils with FP, budesonide, or drug vehicle (DMSO) for 1 hour had no significant effect on the ability of neutrophils to phagocytose H. influenzae or S. pneumoniae (Figure S3) or the amount of bacteria phagocytosed (Figure S4) at any time point studied between 5 minutes’ and 60 minutes’ exposure to bacteria.
Discussion
Inhaled corticosteroids such as FP or budesonide are currently prescribed to COPD patients, mostly as combination inhalers with LABAs, to reduce exacerbation frequency; however, inhaled FP has been associated with increased rates of pneumonia.Citation9–Citation12 This may be due to highly potent and prolonged suppression of macrophages and neutrophilic functions responsible for bacteria phagocytosis and killing after inhalation of FP.
Using an in vitro model, we showed that neither FP nor budesonide had effects on phagocytosis of inert beads, H. influenzae, or S. pneumoniae by MDMs derived from blood monocytes isolated from COPD patients, although 1 hour’s pretreatment with budesonide at 10−7 M increased 4-hour phagocytosis of S. pneumoniae significantly by approximately 20%, and a trend for a similar increase for phagocytosis of both H. influenzae and S. pneumoniae was observed after 18 hours’ pretreatment with budesonide in the whole concentration range studied (10−10–10−5 M). Although there were some differences in effects on phagocytosis between FP and budesonide, this was not reflected in the overall phagocytic ability of MDMs. However, additional effects may have been observed if cells had been cultured for longer than 18 hours in CSs prior to assessment of phagocytosis. These in vitro data obtained with dissolved CSs suggest that the increase in incidence of pneumonia in COPD patients treated with FP is not due to changes in macrophage-phagocytosis function.
It is well known that CSs inhibit the release of proinflammatory cytokines from macrophages, and that this contributes to their therapeutic function. We showed that exposure to H. influenzae or S. pneumoniae for 4 hours induced the release of CXCL8, IL6, and TNFα from MDMs, and that already after 1 hour’s pretreatment, both FP and budesonide reduced the release of these cytokines in a concentration-dependent manner. Nevertheless, there were no statistically significant differences between the effects of FP and budesonide on cytokine release at any time point after exposure to bacteria.
Once a bacterium has been phagocytosed by a macrophage, it undergoes a process known as “bacterial killing”, which includes the generation and release of intracellular reactive oxygen species and/or proteases to break down the bacteria.Citation24 Decreased ability to kill bacteria may result in macrophages being overwhelmed by bacteria and lead to bacterial colonization and establishment of infection. As such, we studied the effects of the two CSs on bacterial killing by MDMs. However, neither FP nor budesonide altered bacterial killing at 4 hours postinfection, suggesting that this innate immunofunction is not compromised by these CSs.
There are few data in the literature regarding the effects of CSs on phagocytosis. The data presented in this study contrast with earlier work, whereby MDMs exposed to dexamethasone showed an increase in phagocytosis and killing of Staphylococcus aureus via a glucocorticoid-receptor-dependent mechanism.Citation25 Administration of FP to a murine model of Klebsiella pneumoniae infection demonstrated increased bacterial load in these animals that was not attributed to alterations in bacterial phagocytosis or killing, but to a suppression in production of nitric oxide and TNFα.Citation26 Previously, we have shown that budesonide improved phagocytosis of both H. influenzae and S. pneumoniae in MDMs (five- and threefold, respectively, at 10−6 M);Citation21 however, budesonide has also been shown to reduce phagocytosis of Escherichia coli in alveolar macrophages.Citation27 The reason for these differences for budesonide is not clear; however, they may be related to the different incubation times that cells were exposed to phagocytic prey in these studies. Zetterlund et alCitation27 incubated macrophages with bacteria for only 10 minutes, as opposed to the 1- and 4-hour incubation periods used in this study and the 1-hour period in the study by Taylor et al.Citation21 The difference in the effect of budesonide between the present study and our previous study could be due to the increased statistical power in this study. As both MDMs and alveolar macrophages display a similar phagocytic defect,Citation21 we would predict that alveolar macrophages would behave similarly in response to CSs. However, this would need confirmation and was outside the scope of the current study.
In order to determine potential mechanisms of CS action on macrophage function, scavenger-receptor expression was analyzed. A variety of receptors were analyzed in this study to reflect the diverse array of receptors involved in phagocytosis. These included the scavenger receptors CD36 and CD163, the mannose receptor CD206, the bacteria-recognition receptors TLR2 (lipoteichoic acid receptor; Gram-positive bacteria) and TLR4 (LPS receptor; Gram-negative bacteria), and MARCO, which binds both Gram-positive and -negative bacteria. However, none of the receptors analyzed was affected by FP or budesonide in the present study. Dexamethasone has been shown to increase phagocytosis of latex beads and E. coli by MDMs, with an associated increase in expression of scavenger receptors (MARCO, mannose receptors, and CD163).Citation28 Similarly, in monocytes and MDMs, increased efferocytosis in the presence of dexamethasone has been associated with increased expression of CD16 and CD163.Citation29 Furthermore, dexamethasone-treated cells show a reduction in paxillin present in podosomes, associated with reduced tyrosine phosphorylation, and a marked increase in levels of Rac.Citation29 Rac proteins are critical regulators of phagocytic function involved in actin assembly, pseudopod extension, and generation of reactive oxygen species for pathogen elimination, and in addition are very important in neutrophil migration.Citation30 However, as no change in phagocytosis was seen in this study, this may link to the lack of effect on scavenger receptors.
Neutrophils are important phagocytic cells and vital in the resolution of lung inflammation. Both FP and budesonide have been shown to prolong neutrophil survival by inhibiting neutrophil apoptosis.Citation31,Citation32 FP also suppresses neutrophil chemotaxis and fibrinogen degradation,Citation33 whereas budesonide has no effect on neutrophil chemotaxis.Citation34 This suggests that neutrophils are sensitive to CSs, but that FP may be more inhibitory than budesonide and contribute to the increased risk of pneumonia. We extended our study to include examination of neutrophil function; however, similarly to MDMs, neutrophil phagocytosis was not affected by exposure to FP or budesonide. This would suggest that neutrophil phagocytosis does not influence the increased rates of pneumonia in FP-treated COPD patients. There is little information regarding the effects of CSs on neutrophil phagocytosis of bacterial pathogens. In vivo studies of dexamethasone administration in a rat model of acute lung injury suggested that dexamethasone had no effect on neutrophil phagocytosis, albeit showed a slight suppression of oxidative burst.Citation35 In human blood neutrophils, an early study showed delayed phagocytosis of Pseudomonas aeruginosa by hydrocortisone and methylprednisolone, but dexamethasone had no effect, whereas all three CSs showed bactericidal effects.Citation36 In a recent study in blood neutrophils from patients with ulcerative colitis who had been on high prednisolone dosages (>10,000 mg), neutrophil phagocytosis of E. coli was not impaired compared with neutrophils from patients on lower-dose or no prednisolone treatment,Citation37 which is consistent with the lack of effects presented herein.
A limitation of our study in terms of applicability to the clinical situation is that we exposed MDMs and neutrophils to dissolved CSs, whereas undissolved, particulate FP may remain in epithelial lining fluid for many hours after inhalation.Citation13 The phagocytosis of particulate FP may lead to FP accumulation at extremely high intracellular concentrations within phagolysosomes, which may impair phagocytosis of bacteria to a greater extent than shown in the present in vitro study using dissolved FP. At these very high intracellular concentrations, the killing of bacteria by MDMs and phagocytosis by neutrophils might also be impaired, although no such effects were observed in this study up to 10−5 M FP concentration. However, it was not possible to compare particulate FP in this system.
Conclusion
Our results suggest that dissolved FP and budesonide do not have an overall effect on MDM or neutrophil phagocytosis of bacteria. However, we cannot exclude such effects of particulate FP, which is present in epithelial lining fluid for many hours after inhalation. Therefore, further study of the effects of particulate FP on functions of airway macrophages and neutrophils is warranted, as impaired function of these cells may explain or contribute to higher rates of pneumonia associated with FP treatment compared to budesonide and non-ICS treatments of COPD patients.
Acknowledgments
This study was supported by the National Institute for Health Research Respiratory Disease Biomedical Research Unit at the Royal Brompton and Harefield NHS Foundation Trust, Imperial College London, and AstraZeneca. The authors would like to thank Anna Miller-Larsson for assistance with this study and the preparation of this manuscript.
Supplementary materials
Figure S1 Effects of fluticasone propionate or budesonide on viability of MDMs after phagocytosis.
Notes: MDMs from COPD patients (n=20–24) were untreated (UC [untreated control]), or pretreated for 1 hour (A–F) or 18 hours (G–L) with fluticasone propionate (○), budesonide (●), or drug vehicle (V) prior to incubation with fluorescently labeled beads or bacteria for 1 hour or 4 hours. Cell viability was measured by MTT assay. Data presented as percentage viability compared to UC and shown as mean ± SEM; *P<0.05 between UC and drug.
Abbreviation: MDMs, monocyte-derived macrophages.
![Figure S1 Effects of fluticasone propionate or budesonide on viability of MDMs after phagocytosis.Notes: MDMs from COPD patients (n=20–24) were untreated (UC [untreated control]), or pretreated for 1 hour (A–F) or 18 hours (G–L) with fluticasone propionate (○), budesonide (●), or drug vehicle (V) prior to incubation with fluorescently labeled beads or bacteria for 1 hour or 4 hours. Cell viability was measured by MTT assay. Data presented as percentage viability compared to UC and shown as mean ± SEM; *P<0.05 between UC and drug.Abbreviation: MDMs, monocyte-derived macrophages.](/cms/asset/0cd7e3ed-26b0-45ba-92ba-cad83e9d6b64/dcop_a_169337_sf0001_b.jpg)
Figure S2 Flow cytometry gating strategy.
Notes: (A–H) Monocyte-derived macrophages were gated by the forward-scatter (FSc) vs side-scatter (SSc) population. Negative expression was gated on untreated population (red) or secondary antibody (MARCO), and a shift to the right indicates positive expression of receptors. Graphs show untreated cells (blue), H. influenzae-positive cells (light green), and cells treated with fluticasone propionate (orange), budesonide (dark green), and vehicle control (pink).
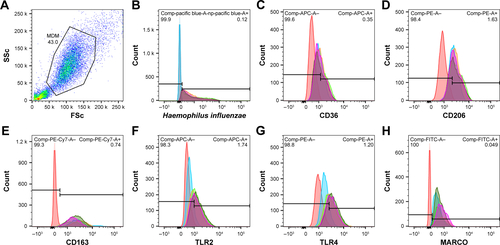
Figure S3 Effects of fluticasone propionate or budesonide on percent phagocytosis of Haemophilus influenzae and Streptococcus pneumoniae by COPD neutrophils.
Notes: Neutrophils from COPD patients were pretreated with fluticasone propionate (○) or budesonide (●) at indicated concentrations or drug vehicle (V) for 1 hour and subsequently incubated with H. influenzae (A–D) or S. pneumoniae (E–H) for 5, 10, 15, or 60 minutes, cells washed, fixed in 4% paraformaldehyde, and fluorescence measured by flow cytometry. Graphs show percentage of neutrophils that phagocytosed bacteria. Data shown as mean ± SEM with no statistical differences observed; n=7.
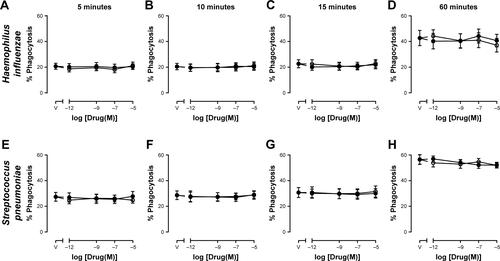
Figure S4 Effects of fluticasone propionate or budesonide on amount of Haemophilus influenzae and Streptococcus pneumoniae phagocytosed by COPD neutrophils.
Notes: Neutrophils from COPD patients were pretreated with fluticasone propionate (○) or budesonide (●) at indicated concentrations or drug vehicle (V) for 1 hour and subsequently incubated with H. influenzae (A–D) or S. pneumoniae (E–H) for 5, 10, 15, or 60 minutes, cells washed, fixed in 4% paraformaldehyde, and fluorescence measured by flow cytometry. Graphs show the amount of phagocytosed bacteria expressed as median fluorescence intensity (MFI). Data shown as mean ± SEM with no statistical differences observed; n=7.
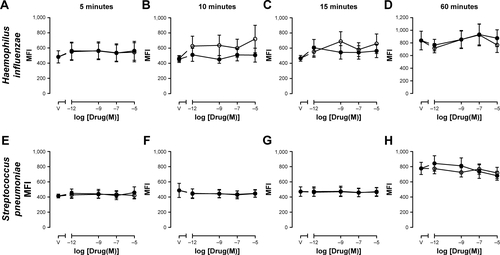
Table S1 Effects of 18 hours’ pretreatment with fluticasone propionate (FP) or budesonide (Bud) on scavenger-receptor expression
Disclosure
The authors report no conflicts of interest in this work.
References
- SuissaSBarnesPJInhaled corticosteroids in COPD: the case againstEur Respir J2009341131619567599
- PostmaDSCalverleyPInhaled corticosteroids in COPD: a case in favourEur Respir J2009341101219567598
- CrimCCalverleyPMAndersonJAPneumonia risk in COPD patients receiving inhaled corticosteroids alone or in combination: TORCH study resultsEur Respir J200934364164719443528
- WedzichaJACalverleyPMSeemungalTAThe prevention of chronic obstructive pulmonary disease exacerbations by salmeterol/fluticasone propionate or tiotropium bromideAm J Respir Crit Care Med20081771192617916806
- AnzuetoAFergusonGTFeldmanGEffect of fluticasone propionate/salmeterol (250/50) on COPD exacerbations and impact on patient outcomesCOPD20096532032919863361
- FergusonGTAnzuetoAFeiREmmettAKnobilKKalbergCEffect of fluticasone propionate/salmeterol (250/50 µg) or salmeterol (50 µg) on COPD exacerbationsRespir Med200810281099110818614347
- JenkinsCRJonesPWCalverleyPMEfficacy of salmeterol/fluticasone propionate by GOLD stage of chronic obstructive pulmonary disease: analysis from the randomised, placebo-controlled TORCH studyRespir Res2009105919566934
- HollisSJorupCLythgoeDMartenssonGRegnellPEckerwallGRisk of pneumonia with budesonide-containing treatments in COPD: an individual patient-level pooled analysis of interventional studiesInt J Chron Obstruct Pulmon Dis2017121071108428435240
- JansonCLarssonKLisspersKHPneumonia and pneumonia related mortality in patients with COPD treated with fixed combinations of inhaled corticosteroid and long acting β2 agonist: observational matched cohort study (PATHOS)BMJ2013346f330623719639
- YangHHLaiCCWangYHSevere exacerbation and pneumonia in COPD patients treated with fixed combinations of inhaled corticosteroid and long-acting β2 agonistInt J Chron Obstruct Pulmon Dis2017122477248528860742
- WangCYLaiCCYangWCThe association between inhaled corticosteroid and pneumonia in COPD patients: the improvement of patients’ life quality with COPD in Taiwan (IMPACT) studyInt J Chron Obstruct Pulmon Dis2016112775278327877031
- SuissaSPatenaudeVLapiFErnstPInhaled corticosteroids in COPD and the risk of serious pneumoniaThorax201368111029103624130228
- JansonCStratelisGMiller-LarssonAHarrisonTWLarssonKScientific rationale for the possible inhaled corticosteroid intraclass difference in the risk of pneumonia in COPDInt J Chron Obstruct Pulmon Dis2017123055306429089754
- RestrepoMIMortensenEMPughJAAnzuetoACOPD is associated with increased mortality in patients with community-acquired pneumoniaEur Respir J200628234635116611653
- HolguinFFolchEReddSCManninoDMComorbidity and mortality in COPD-related hospitalizations in the United States, 1979 to 2001Chest200512842005201116236848
- EkALarssonKSiljerudSPalmbergLFluticasone and budesonide inhibit cytokine release in human lung epithelial cells and alveolar macrophagesAllergy199954769169910442524
- DalbyCPolanowskiTLarssonTBorgströmLEdsbäckerSHarrisonTWThe bioavailability and airway clearance of the steroid component of budesonide/formoterol and salmeterol/fluticasone after inhaled administration in patients with COPD and healthy subjects: a randomized controlled trialRespir Res20091010419878590
- EdsbäckerSWollmerPSelroosOBorgströmLOlssonBIngelfJDo airway clearance mechanisms influence the local and systemic effects of inhaled corticosteroids?Pulm Pharmacol Ther200821224725817950641
- BarnesPJAlveolar macrophages as orchestrators of COPDCOPD200411597016997739
- BerensonCSGarlippMAGroveLJMaloneyJSethiSImpaired phagocytosis of nontypeable Haemophilus influenzae by human alveolar macrophages in chronic obstructive pulmonary diseaseJ Infect Dis2006194101375138417054066
- TaylorAEFinney-HaywardTKQuintJKDefective macrophage phagocytosis of bacteria in COPDEur Respir J20103551039104719897561
- ContoliMPaulettiARossiMRLong-term effects of inhaled corticosteroids on sputum bacterial and viral loads in COPDEur Respir J2017504170045128982774
- AllportJRDonnellyLEKefalasPA possible role for mono (ADP-ribosyl) transferase in the signalling pathway mediating neutrophil chemotaxisBr J Clin Pharmacol1996421991068807150
- AberdeinJDColeJBewleyMAMarriottHMDockrellDHAlveolar macrophages in pulmonary host defence: the unrecognized role of apoptosis as a mechanism of intracellular bacterial killingClin Exp Immunol2013174219320223841514
- van der GoesAHoekstraKvan den BergTKDijkstraCDDexamethasone promotes phagocytosis and bacterial killing by human monocytes/macrophages in vitroJ Leukoc Biol200067680180710857852
- PattersonCMMorrisonRLd’SouzaATengXSHappelKIInhaled fluticasone propionate impairs pulmonary clearance of Klebsiella pneumoniae in miceRespir Res2012134022651370
- ZetterlundALarssonPHMüller-SuurCPalmbergLLarssonKBudesonide but not terbutaline decreases phagocytosis in alveolar macrophagesRespir Med19989221621669616506
- GratchevAKzhyshkowskaJUtikalJGoerdtSInterleukin-4 and dexamethasone counterregulate extracellular matrix remodelling and phagocytosis in type-2 macrophagesScand J Immunol2005611101715644118
- GilesKMRossKRossiAGHotchinNAHaslettCDransfieldIGlucocorticoid augmentation of macrophage capacity for phagocytosis of apoptotic cells is associated with reduced p130Cas expression, loss of paxillin/pyk2 phosphorylation, and high levels of active RacJ Immunol2001167297698611441106
- CostaCGermenaGHirschEDissection of the interplay between class I PI3Ks and Rac signaling in phagocytic functionsScientific-World Journal2010101826183920852826
- ZhangXMoilanenEKankaanrantaHBeclomethasone, budesonide and fluticasone propionate inhibit human neutrophil apoptosisEur J Pharmacol2001431336537111730731
- GizyckiMJHattotuwaKLBarnesNJefferyPKEffects of fluticasone propionate on inflammatory cells in COPD: an ultrastructural examination of endobronchial biopsy tissueThorax200257979980312200525
- Llewellyn-JonesCGHillSLStockleyRAEffect of fluticasone propionate on neutrophil chemotaxis, superoxide generation, and extracellular proteolytic activity in vitroThorax19944932072128202875
- StrandbergKBlidbergKSahlanderKPalmbergLLarssonKEffect of formoterol and budesonide on chemokine release, chemokine receptor expression and chemotaxis in human neutrophilsPulm Pharmacol Ther201023431632320307681
- O’LearyECEvansGFZuckermanSHIn vivo dexamethasone effects on neutrophil effector functions in a rat model of acute lung injuryInflammation19972165976089429907
- BaltchALHammerMCSmithRPComparison of the effect of three adrenal corticosteroids on human granulocyte function against Pseudomonas aeruginosaJ Trauma19862665255333088287
- OkitaYMikiCYoshiyamaSNeutrophil dysfunction in steroid-overdosed patients with ulcerative colitis: potential relevance of macrophage migration inhibitory factor to increased postoperative morbiditySurg Today201141111504151121969153