
Abstract
Background
Data are scarce on patient physical activity (PA) level during exacerbations of chronic obstructive pulmonary disease (eCOPD). The objective of the study was to evaluate the level and determinants of change in PA during an eCOPD.
Materials and methods
We conducted a prospective cohort study with recruitment from emergency departments (EDs) of 16 participating hospitals from June 2008 to September 2010. Data were recorded on socioeconomic characteristics, dyspnea, forced expiratory volume in 1 second (FEV1%), comorbidities, health-related quality of life, factors related to exacerbation, and PA in a stable clinical condition and during the eCOPD episode.
Results
We evaluated 2,487 patients. Common factors related to the change in PA during hospital admission or 7 days after discharge to home from the ED were lower PA at baseline and during the first 24 hours after the index evaluation. Age, quality of life, living alone, length of hospital stay, and use of anticholinergic or systemic corticosteroids in treating the exacerbation were associated with the change in PA among hospitalized patients. Predictors of change among patients not admitted to hospital were baseline FEV1% and dyspnea at rest on ED arrival.
Conclusion
Among the patients evaluated in an ED for an eCOPD, the level and change in PA was markedly variable. Factors associated with exacerbation (PA 24 hours after admission, medication during admission, and length of hospital stay) and variables reflecting patients’ stable clinical condition (low level of PA, age, quality of life, FEV1%) are predictors of the change in PA during a moderate-to-severe eCOPD.
Introduction
Among older individuals, there is a complex association between functional decline, defined as loss of capacity to carry out activities of daily life,Citation1,Citation2 and hospitalization. It is well known that hospitalization can lead to functional decline.Citation1,Citation2 Sometimes, however, functional decline precedes hospitalization.Citation3 The etiology of functional decline goes beyond the disease process that triggered the admission and it is likely that several mechanisms are involved. One possible contributor is decreased mobility – a reduction in an individual’s usual level of physical activity (PA). During hospitalization, geriatric patients spend 83% of their time in bed and just 4% standing or walking.Citation4 Low mobility in hospitalized patients has been shown to be a predictor of adverse outcomes.Citation5
After adjusting for demographic and clinical characteristics, older patients who increased their walking distance by 600 steps (equivalent to walking for 12 minutes) from the first day of admission to the second day were discharged 2.13 days before those who did not achieve this level of PA.Citation6
Relatively little is known about the association between change in PA level and exacerbation-related outcomes in patients with COPD. However, the evidence base has begun to grow and it has been seen that PA may have an influence on very important outcomes, such as mortality and readmissions.Citation7,Citation8 During exacerbations, COPD patients report even less daily outdoor PA,Citation9 and their level of PA falls even further during hospitalization for an exacerbation of COPD (eCOPD).Citation10 In fact, patients often do not recover their PA level within the first month after an eCOPD.Citation10
The aim of this study was to evaluate changes in PA during episodes of moderate-to-severe eCOPD requiring assessment in an emergency department (ED) and identify determinants of these changes.
Methods/design
This prospective cohort study recruited patients from 16 hospitals in the Spanish National Health Service. Patients with an eCOPD attending the ED were informed about the study objectives and invited to participate, and if they agreed, written informed consent was obtained. All data collected were kept confidential and the Institutional Review Boards of the participating hospitals approved this study. Recruitment started in June 2008 and ended in September 2010. A description of the study protocol has been published.Citation11
Patients were eligible for the study if they arrived at the ED with symptoms consistent with an eCOPD. COPD was confirmed by spirometry if the patient had a forced expiratory volume in 1 second/forced vital capacity (FEV1/FVC) ratio <70%. The severity of airflow limitation was classified in accordance with the Global Initiative for Chronic Obstructive Lung Disease (GOLD).Citation12
Exacerbation was defined as an event characterized by a change in the patient’s baseline dyspnea, cough, and/or sputum that was beyond normal day-to-day variations and may have warranted a change in medication.Citation12 Patients newly diagnosed with COPD in the ED were included in the study, provided that the diagnosis was confirmed by spirometry within 60 days after the index episode at a time when they were stable. Patients were excluded from the study if they did not wish to participate or if, at the time they were being evaluated in the ED, their eCOPD was complicated by a comorbidity such as pneumonia, pneumothorax, pulmonary embolism, lung cancer, or left cardiac failure.
Data collection
Data collected upon arrival at the ED included socioeconomic data, information about the patient’s respiratory state (arterial blood gases, respiratory rate, dyspnea), level of consciousness measured by the Glasgow Coma Scale,Citation13 and presence of other conditions included in the Charlson Comorbidity Index.Citation14
For patients admitted to the hospital from the ED, we collected additional data from the patient’s medical record as well as from interviews on the first day after admission and on the day of discharge. They were asked questions about their PA, their general health, and their level of dyspnea before the index eCOPD, 24 hours after being admitted to hospital, and at hospital discharge. Patients discharged from the ED to home were also asked questions related to these variables (their PA, their general health, and their level of dyspnea), in their case, referring to before the index eCOPD, 24 hours after being discharged from the hospital ED, and 1 week after the index ED visit.
For PA level, we focused on walking. Participants were given six response options about their daily activity (walking) before the exacerbation: I just walk from bed to a chair; I am housebound but walk inside the house; I walk a few hundred meters outside; I walk for errands; I regularly walk – walking a walk at least 3 days a week; and I take part in some kind of sport. This PA scale was based on the health, activity, dyspnea, obstruction (HADO) score,Citation15 already validated, and has been used in previous studies. This scale showed good correlation with the St George’s Respiratory Questionnaire activity subscale. It also shows, in this sample, good correlation with the European Quality of Life-5 Dimensions (EQ-5D; Pearson’s r correlation coefficient: 0.42 in admitted patients and 0.49 in those discharged; P for both <0.0001) and the fatigue scale (r correlation coefficient: 0.39 and 0.30, respectively; P for both <0.0001).
At 24 hours after the index ED evaluation, patients were asked about the level of PA they were able to perform at that time, as well as their general health status and dyspnea. Similar response options were given at the time of discharge for patients who had been admitted to the hospital from the ED assessment and after 7 days for those discharged to home from the ED assessment. These were: I am bedridden; I sit down; I walk to the bathroom; I walk in the room; I walk outside the room with limitations; and I can walk outside the room without limitations. Baseline general health status was measured using the EQ-5D questionnaire.Citation16,Citation17
To measure the level of dyspnea at baseline we used the Medical Research Council breathlessness scale, which uses a five-category scale that ranges from “I only get breathless with strenuous exercise” to “I am too breathless to leave the house”.Citation18 The level of dyspnea during the follow-up, that is, 24 hours after the index ED visit and at hospital discharge was measured with a specific question “How do you rate your level of dyspnea today” with a seven-point response scale from very severe to none, similar to the previously validated Borg Dyspnea Scale.Citation19,Citation20
For all patients, additional variables collected from medical records included pulmonary function as measured by FEV1; hospital admissions for COPD during the previous 12 months; baseline respiratory therapy; and the presence of comorbidities needed to determine the Charlson Comorbidity Index.Citation14
Further, for all patients, we reviewed medical records and conducted telephone interviews 2 months after the index ED evaluation to ascertain their vital status and whether they had been readmitted to hospital.
Definitions of outcome measures
The main outcome variable was change in PA. For patients admitted to the hospital, this was defined as the difference between PA reported at hospital discharge and that reported 24 hours after being admitted to the hospital. For patients discharged to home from the ED, it was defined as the difference between PA reported 1 week after being discharged from the ED and that reported 24 hours after being discharged from the ED to home.
Additional outcome parameters were mortality during the 2 months after the ED index visit; readmission for an eCOPD during these 2 months; and, for patients admitted to the hospital from the index ED visit, length of stay, measured as the day the patient was discharged from hospital minus the day he or she was admitted.
Statistical analysis
The unit of the analysis was the patient. For patients who had more than one ED visit during the recruitment period, only the first one was considered for the analysis.
Descriptive statistics included frequencies and percentages for categorical variables and means and standard deviation (SD) for continuous variables. Main sociodemographic and clinical characteristics, as well as patient-reported measures at baseline, were compared between patients admitted to hospital from the index ED evaluation and those discharged to home.
Generalized linear models were used in the univariate analysis to determine which variables were related to PA level at discharge among patients admitted to the hospital or 1 week after discharge to home from the ED. Patients who died during this period were excluded from the analysis.
In the multivariate analysis, separate generalized linear models were used for patients admitted to the hospital and those discharged to home from the ED. All variables with a P-value lower than 0.20 were included in the multivariate analysis. Variables with P<0.05 were included in the final models. The effect of the participating hospital in the final models was also taken into account by means of multilevel models.
All effects were considered to be significant at P<0.05. All statistical analyses were performed using SAS for Windows, version 9.2 (SAS Institute Inc., Cary, NC, USA).
Results
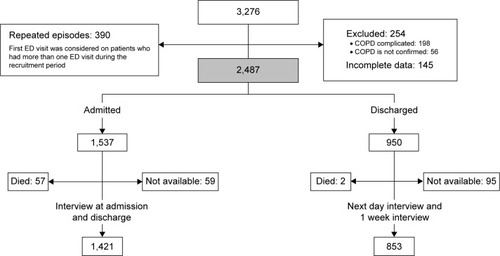
A total of 3,276 eCOPD episodes were identified for the study. The final population included 2,487 patients. The recruitment process is outlined in .
Figure 1 Flowchart of exclusions and missing cases.
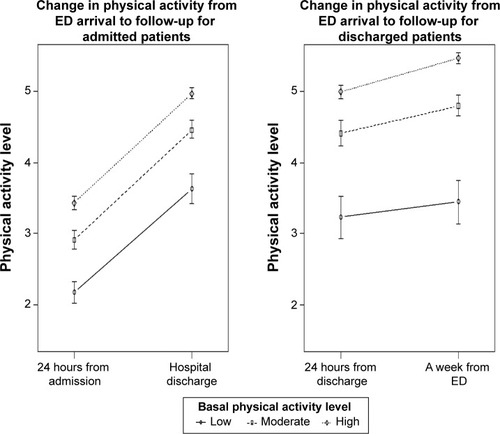
Both groups of eCOPD patients showed increases in PA during follow-up, that is, at hospital discharge or 1 week after discharge to home from the ED (). However, 16% of the admitted patients did not perform any PA during their hospitalization and 17% walked only in their hospital room during that time, while among those discharged from the ED the corresponding percentages were 10% and 9%, respectively ().
Table 1 Descriptive characteristics of the sample by admission status
Figure 2 Changes in physical activity from ED arrival to follow-up by basal physical activity level and admission status.
Abbreviation: ED, emergency department.
Variables associated with change in PA during hospital admission were: age; baseline FEV1%; the need for home oxygen therapy; noninvasive mechanical ventilation or continuous positive airway pressure ventilation; number of admissions for an eCOPD during the previous 12 months; Charlson Comorbidity Index score; level of consciousness as measured by the Glasgow Coma Scale score; presence of dyspnea at rest upon ED arrival; length of stay; PA at baseline; and PA in the first 24 hours after admission. Taking the best score in each variable as a reference, all had significant inverse association with change in PA during the hospitalization or the 7 days after being discharged to home from the ED ().
Table 2 Univariate analysis of predictors of change of physical activity at hospital discharge or 7 days after visiting the ED
In multivariate analyses, we evaluated factors associated with the change in PA during hospital admission or an equivalent time (1 week) in patients discharged to home from the ED. Among patients admitted to the hospital, changes in PA from admission to discharge () were influenced by their previous level of PA: level of PA 24 hours after admission (limited to those patients with the lowest level of PA): age: health-related quality of life (HRQoL) as measured by the EQ-5D: and length of hospital stay: as well as use of inhaled anticholinergic medications (associated with an increase in PA) or corticosteroids (associated with a decrease in PA). Among patients discharged to home from the ED, changes in PA after 1 week () were influenced by previous level of PA: level of PA 24 hours after the index ED visit: FEV1%: and the presence of dyspnea at rest upon ED arrival.
Table 3 Change in PA level in admitted patients: multivariate analysis
Table 4 Change in PA level in ED discharged patients: multivariate analysis
For both groups, patients admitted to the hospital and those discharged to home from the ED, shows outcomes including mortality, length of stay, and readmission by PA levels. Among patients admitted to the hospital, the length of hospital stay was associated with the level of PA both at baseline and at 24 hours after admission (falling from 8.9 to 5.3 days with increasing baseline PA and 9.2 to 6.8 with increasing PA at 24 hours, respectively) as was mortality during admission (varying from 15% to 1% and 10.5% to 0%, respectively). Further, readmission rates within 2 months were related to the level of PA at discharge from the hospital, or 1 week after the index visit in patients discharged (varying from 40% to 15% and 41% to 11%, respectively, with increasing levels of PA).
Table 5 Outcomes by physical activity levels in patients admitted and discharged from ED
Discussion
The results of this study indicate that the level of PA is quite variable during an eCOPD that requires an ED visit, as are the variables associated with the change in PA during the exacerbation, and these differ between patients admitted to hospital and those discharged to home. PA levels at baseline, 24 hours after hospital admission, and at the time of hospital discharge or 7 days after the index ED assessment are associated with length of stay, readmission, and mortality during admission.
Hospitalization has previously been associated with decreases in PA. Fisher et al found that older people hospitalized for an acute medical illness performed little PA, spending only 4.1% of their time walking.Citation21 In 17 hospitalized patients with severe COPD who were fitted with accelerometers, Pitta et al found that PA was significantly lower than the PA level of patients with stable COPD.Citation7 In contrast, our study showed that COPD patients have a wide range of PA during a hospital admission for an eCOPD. In fact, in the first 24 hours after admission, 17.5% of patients in our study walked, at least, in their hospital rooms. Apart from the use of different measurement tools, these differences could be explained by the larger size of our cohort and the range of COPD severity among the participants.
Little information is available about PA among patients experiencing an eCOPD who are not admitted to hospital. As might be expected, in our cohort these patients had a higher level of PA in the first 24 hours after the index ED visit than those who were admitted to the hospital. Only 17% of patients discharged to home from the ED reported minimal PA at 24 hours (categories 1–3) compared to 65% of admitted patients.
Donaldson et al showed that COPD patients spent only 1.5 days indoors immediately after an exacerbation – not necessarily a severe one – which implies a quick return to normality.Citation9 In contrast, Pitta et al found that several patients failed to achieve the PA level of stable COPD patients 1 month after their hospital discharge.Citation10 Our data for non-admitted eCOPD patients were generally in agreement with a relatively fast recovery.
Some factors associated with the change in PA during hospital admission are related to the general clinical condition of the patient, such as older age, poorer HRQoL, living alone, and reporting the lowest level of PA at baseline (confined to bed or a chair). Other associated variables were PA during the first 24 hours after admission, length of stay, and use of anticholinergic or systemic corticosteroids to treat the eCOPD.
Interestingly, among patients admitted to the hospital, factors related to the severity of COPD, such as FEV1%, level of dyspnea when the patient was stable, comorbidities, and hospitalizations for eCOPD in the previous year played no role in the change of PA during the admission. Further, even variables related to the ED visit (reflecting the severity of the exacerbation), such as level of respiratory failure, also had no relationship with the change in PA. These findings are in accordance with the results of Fisher et al who found no association between the number of steps taken by patients during admission and the severity of the illness.Citation21
Among patients admitted to the hospital, the lower the PA level during the first 24 hours after admission, the smaller the change in PA at hospital discharge. This finding suggests that early activity might improve later PA and perhaps other outcomes among patients hospitalized for an eCOPD.
In our study, HRQoL was related to the change in PA during hospitalization. Among stable COPD patients, HRQoL has previously been identified as a predictor of PA.Citation22 An association between changes in PA and changes in HRQoL has been also observed,Citation23 although such an association has not been demonstrated during an eCOPD.
Among patients discharged to home from the ED, the only variables of the eCOPD episode that were associated with changes in PA were baseline level of PA, FEV1%, and dyspnea at rest upon arrival at the ED.
Surprisingly, the use of anticholinergic medication during admission was associated with a positive change in PA. This could reflect appropriate treatment of a severe eCOPD that improves hyperinflation and makes PA easier.Citation24 In contrast, the use of systemic corticosteroids was associated with a decline in PA, which could be related to deterioration of muscle function.Citation10
Summarizing, in both groups of our sample, we identified important factors beyond to the two common predictive variables, namely, PA at baseline and 24 hours. Among those discharged from the ED, these predictors were just baseline COPD obstructive severity level and dyspnea status at ED arrival; while for those admitted several parameters related to general health status of the patient (age, EQ-5D, and living arrangements) and, importantly, to the index admission (length of stay and medication used) make a difference to the prediction of changes. These findings indicate that variables besides COPD status, including some treatments, play an important role.
Several studies have suggested that PA may be therapeutic during hospitalization. Among patients hospitalized for an acute medical condition, those who had shorter lengths of stay took more steps on the first complete day in hospital.Citation21 In another study by Fisher et al patients hospitalized for an acute medical illness who increased their walking by at least 600 steps from the first to the second 24-hour day were discharged 1.7 days earlier than those who did not.Citation6 Shadmi and Zisberg observed a 1.5-day shorter length of stay in patients who were mobile outside their hospital rooms compared with those who were only mobile inside their rooms.Citation25
Low-grade systemic inflammation is part of the COPD disease process. Skeletal muscle wasting has been related to the use of systemic corticosteroids and immobilization, and has been associated with functional deterioration during hospitalization in eCOPD patients.Citation10 PA would increase the circulating level of anti-inflammatory cytokines such as interleukin (IL)-6, IL-1ra, IL-10, and soluble tumor necrosis factor receptors,Citation26 which could help restore equilibrium in this inflammatory stateCitation27 (although it is not known which agents mediate this effect). A rehabilitation program undertaken during admission for eCOPD has been shown to prevent muscle deterioration.Citation28 We speculate that early mobilization would work as a kind of rehabilitation, with similar benefits to a structured program.
The multicenter design and the large number of patients included in the two arms of the study – those admitted and those directly discharged from the ED – are the main strength of this study.
Limitations of our study should also be noted. We did not objectively measure PA with accelerometers, as has been done in smaller studies. Using these devices in a large, multicenter study such as ours would have been extremely complicated. Prospective studies are likely to have missing data, this being inherent to the design. Our study is no exception, although we were able to include a high proportion of patients at follow-up and collect complete information for the variables considered in the analysis.
In summary, we found that among patients evaluated in an ED for an eCOPD the level of PA is quite variable. Immediately following the eCOPD, variables related to the exacerbation and those reflecting the general clinical condition of the patient influence changes in the level of PA, especially among those admitted to hospital from the ED. Future studies should confirm these results using objective PA measurements. Maximizing bronchodilator treatment and beginning PA at a very early stage following an eCOPD could improve outcomes in these patients.
Acknowledgments
We are grateful for the support of the 16 participating hospitals (Hospital Costa del Sol, Hospital Valme, Hospital de Motril, Corporació Sanitaria Parc Taulí, Hospital del Mar, Hospital Universitario de La Princesa, Hospital Universitario Gregorio Marañón, Hospital Universitario La Paz, Hospital de Móstoles, Hospital Marqués de Valdecilla, Hospital Santa Marina, Hospital San Eloy, Hospital Galdakao-Usansolo, Hospital Txagorritxu, Complejo Hospitalario Donostia, and Hospital Cruces), as well as the ED physicians, other clinicians, and staff members of the various services, research units, quality units, and medical records sections of these hospitals. We also gratefully acknowledge the patients who participated in the study.
This work was supported in part by grants from the Fondo de Investigación Sanitaria (PI 06\1010, PI06\1017, PI06\714, PI06\0326, PI06\0664); Department of Health of the Basque Country, Department of Education, Universities and Research of the Basque Government (UE09/62); the Research Committee of the Hospital Galdakao; and the thematic networks – Red IRYSS (Investigacion en Resultados y Servicios Sanitarios (G03/220) – of the Instituto de Salud Carlos III.
The authors also acknowledge the editorial assistance provided by Patrick Skerrett.
The IRYSS-COPD group included the following coinvestigators: Dr Jesús Martínez-Tapias (Hospital Virgen de las Nieves, Granada); Alba Ruiz (Hospital de Motril, Granada); Dr Eduardo Briones (Unidad de Epidemiología. Distrito Sanitario Sevilla); Dra Silvia Vidal (Unidad de Investigación, Hospital Costa del Sol, Marbella); Dr Emilio Perea-Milla, Francisco Rivas (Servicio de Epidemiología, Hospital Costa del Sol, Málaga – REDISSEC); Dr Maximino Redondo (Servicio de Laboratorio, Hospital Costa del Sol, Málaga-REDISSEC); Javier Rodríguez Ruiz (Responsable de Enfermería del Área de Urgencias, Hospital Costa del Sol, Málaga); Dra Marisa Baré (Epidemiología y Evaluación, Corporació Sanitaria Parc Taulí-CSPT, Sabadell REDIS-SEC), Dr Manel Lujan, Dra Concepción Montón (Servicio de Neumología, CSPT/REDISSEC); Dra Amalia Moreno, Dra Josune Ormaza, Dr Javier Pomares (Servicio de Neumología, CSPT); Dr Juli Font (Medicina, Servicio de Urgencias; CSPT), Dra Cristina Estirado, Dr Joaquín Gea (Servicio de Neumología, Hospital del Mar/CIBERES, Barcelona); Dra Elena Andradas (subdirectora de Promoción de la Salud y Epidemiología del Ministerio de Sanidad, Servicios Sociales e Igualdad), Dr Juan Antonio Blasco (Unidad de Evaluación de Tecnologías Sanitarias, Agencia Laín Entralgo, Madrid), Dra Nerea Fernández de Larrea (Subdirección General de Tec-nología e Innovación Sanitarias. Consejería de Sanidad de la Comunidad de Madrid/REDISSEC); Rosa Girón (Hospital de La Princesa, Madrid), María del Puerto Cano Aguirre (Hospital de Torrejón, Madrid); Dr Jose Luis Lobo (Servicio de Neumología, Hospital Txagorritxu, Araba); Dra Esther Pulido (Servicio de Urgencias, Hospital Galdakao-Usansolo, Bizkaia); Dr Mikel Sánchez (Servicio de Urgencias, Hospital Galdakao-Usansolo); Dr Luis Alberto Ruiz (Servicio de Respiratorio, Hospital de Cruces, Bizkaia); Dra Ane Miren Gastaminza (Hospital San Eloy, Bizkaia); Dra Eva Tabernero (Servicio de Neumología, Hospital de Santa Marina), Carmen Haro (Servicio de Urgencias, Hospital de Santa Marina, Bizkaia); Dr Ramon Agüero (Servicio de Neumología, Hospital Marqués de Valdecilla, Santander); Dr Gabriel Gutiérrez (Servicio de Urgencias, Hospital Cruces, Bizkaia); Dra Belén Elizalde (Dirección Territorial de Gipuzkoa); Dr Felipe Aizpuru (Unidad de Investigación, Hospital Txagorritxu, Álava/REDISSEC); Dra Inmaculada Arostegui, Irantzu Barrio (Departamento de Matemática Aplicada, Estadística e Investigación Operativa, UPV/EHU- REDISSEC); Amaia Bilbao (Hospital Universitario Basurto/REDISSEC); Dr Cristóbal Esteban (Servicio de Neumología, Hospital Galdakao-Usansolo, Bizkaia/REDISSEC); Dra Nerea González, Susana Garcia, Iratxe Lafuente, Urko Aguirre; Miren Orive, Ane Anton, and Dr Jose M Quintana (Unidad de Investigación, Hospital Galdakao-Usansolo, Bizkaia/REDISSEC).
Disclosure
The authors report no conflicts of interest in this work.
References
- BuurmanBMvan MunsterBCKorevaarJCde HaanRJde RooijSEVariability in measuring (instrumental) activities of daily living functioning and functional decline in hospitalized older medical patients: a systematic reviewJ Clin Epidemiol20116461962721074969
- McCuskerJKakumaRAbrahamowiczMPredictors of functional decline in hospitalized elderly patients: a systematic reviewJ Gerontol A Biol Sci Med Sci200257M569M57712196493
- CovinskyKEPalmerRMCounsellSRPineZMWalterLCChrenMMFunctional status before hospitalization in acutely ill older adults: validity and clinical importance of retrospective reportsJ Am Geriatr Soc20004816416910682945
- BrownCJReddenDTFloodKLAllmanRMThe underrecognized epidemic of low mobility during hospitalization of older adultsJ Am Geriatr Soc2009571660166519682121
- BrownCJFriedkinRJInouyeSKPrevalence and outcomes of low mobility in hospitalized older patientsJ Am Geriatr Soc2004521263127015271112
- FisherSRKuoYFGrahamJEOttenbacherKJOstirGVEarly ambulation and length of stay in older adults hospitalized for acute illnessArch Intern Med20101701942194321098357
- PittaFTroostersTSpruitMAProbstVSDecramerMGosselinkRCharacteristics of physical activities in daily life in chronic obstructive pulmonary diseaseAm J Respir Crit Care Med200517197297715665324
- EstebanCArosteguiIAburtoMInfluence of changes in physical activity on frequency of hospitalization in chronic obstructive pulmonary diseaseRespirology20141933033824483954
- DonaldsonGCWilkinsonTMHurstJRPereraWRWedzichaJAExacerbations and time spent outdoors in chronic obstructive pulmonary diseaseAm J Respir Crit Care Med200517144645215579723
- PittaFTroostersTProbstVSSpruitMADecramerMGosselinkRPhysical activity and hospitalization for exacerbation of COPDChest200612953654416537849
- QuintanaJMEstebanCBarrioIThe IRYSS-COPD appropriateness study: objectives, methodology, and description of the prospective cohortBMC Health Serv Res20111132222115318
- The Global Strategy for the Diagnosis, Management and Prevention of Chronic Obstructive Pulmonary DiseaseGlobal Initiative for Chronic Obstructive Lung Disease (GOLD)2011 Available from: http://www.goldcopd.org/Accessed Jan 21, 2011
- TeasdaleGJennettBAssessment of coma and impaired consciousness. A practical scaleLancet1974281844136544
- CharlsonMEPompeiPAlesKLMacKenzieCRA new method of classifying prognostic comorbidity in longitudinal studies: development and validationJ Chronic Dis1987403733833558716
- EstebanCQuintanaJMAburtoMMorazaJCapelasteguiAA simple score for assessing stable chronic obstructive pulmonary diseaseQJM20069975175917030529
- BrooksREuroQol: the current state of playHealth Policy199637537210158943
- BadiaXRosetMMontserratSHerdmanMSeguraAThe Spanish version of EuroQol: a description and its applications. European Quality of Life scaleMed Clin (Barc)1999112Suppl 1798510618804
- FletcherCMElmesPCFairbairnASWoodCHThe significance of respiratory symptoms and the diagnosis of chronic bronchitis in a working populationBr Med J1959225726613823475
- HareendranALeidyNKMonzBUWinnetteRBeckerKMahlerDAProposing a standardized method for evaluating patient report of the intensity of dyspnea during exercise testing in COPDInt J Chron Obstruct Pulmon Dis2012734535522745534
- MarinJMCarrizoSJGasconMSanchezAGallegoBCelliBRInspiratory capacity, dynamic hyperinflation, breathlessness, and exercise performance during the 6-minute-walk test in chronic obstructive pulmonary diseaseAm J Respir Crit Care Med20011631395139911371407
- FisherSRGoodwinJSProtasEJAmbulatory activity of older adults hospitalized with acute medical illnessJ Am Geriatr Soc201159919521158744
- García-AymerichJFélezMAEscarrabillJPhysical activity and its determinants in severe chronic obstructive pulmonary diseaseMed Sci Sports Exerc2004361667167315595285
- EstebanCQuintanaJMAburtoMImpact of changes in physical activity on health-related quality of life among patients with COPDEur Respir J20103629230020075059
- O’DonnellDELavenezianaPThe clinical importance of dynamic lung hyperinflation in COPDCOPD2006321923217361503
- ShadmiEZisbergAIn-hospital mobility and length of stayArch Intern Med2011171129821788551
- SteensbergAFischerCPKellerCMøllerKPedersenBKIL-6 enhances plasma IL-1ra, IL-10, and cortisol in humansAm J Physiol Endocrinol Metab2003285E433E43712857678
- BrandtCPedersenBKThe role of exercise-induced myokines in muscle homeostasis and the defense against chronic diseasesJ Biomed Biotechnol2010201052025810.1155/2010/52025820224659
- TroostersTProbstVSCrulTResistance training prevents deterioration in quadriceps muscle function during acute exacerbations of chronic obstructive pulmonary diseaseAm J Respir Crit Care Med20101811072107720133927