
Abstract
Objective
To assess the frequency of comorbidities in subjects with COPD and their association with respiratory symptom severity and COPD exacerbations.
Materials and methods
This was an analysis of the BREATHE study, a cross-sectional survey of COPD conducted in the general population of eleven countries in the Middle East and North Africa, including Pakistan. The study population consisted of a sample of subjects with COPD for whom the presence of comorbidities was documented. Three questionnaires were used. The screening questionnaire identified subjects who fulfilled an epidemiological case definition of COPD and documented any potential comorbidities; the detailed COPD questionnaire collected data on respiratory symptoms, COPD exacerbations, and comorbidities associated with COPD; the COPD Assessment Test collected data on the impact of respiratory symptoms on well-being and daily life.
Results
A total of 2,187 subjects were positively screened for COPD, of whom 1,392 completed the detailed COPD questionnaire. COPD subjects were more likely to report comorbidities (55.2%) than subjects without COPD (39.1%, P<0.0001), most frequently cardiovascular diseases. In subjects who screened positively for COPD, the presence of comorbidities was significantly (P=0.03) associated with a COPD Assessment Test score ≥10 and with antecedents of COPD exacerbations in the previous 6 months (P=0.03).
Conclusion
Comorbidities are frequent in COPD and associated with more severe respiratory symptoms. This highlights the importance of identification and appropriate management of comorbidities in all subjects with a diagnosis of COPD.
Introduction
Comorbidities are frequent in subjects with COPD,Citation1 and the incidence of these has been assessed in many studies.Citation2–Citation4 In a large study of 30,000 COPD patients in the UK, it was estimated that COPD patients presented a fivefold-higher risk of cardiovascular diseases, a threefold-higher risk of stroke, and a twofold-higher risk of diabetes.Citation3 Given that the prevalence of both COPD and its principal comorbidities, such as cardiovascular diseases or diabetes, are rising around the world,Citation5,Citation6 the risk of coexistence of these chronic diseases is expected to increase. It is now recognized that the presence of comorbidities in COPD patients has a major impact on quality of life and on mortality.Citation7 The majority of data regarding the burden of comorbidities associated with COPD has come from industrialized countries, where it has been shown that COPD comorbidities have an important impact on burden of disease and represent an important driver of cost.Citation8,Citation9
In the Middle East and North Africa (MENA), the prevalence of COPD has been estimated at around 4% of adults aged over 40 years in the general population.Citation10 This prevalence is expected to grow rapidly, since smoking rates in the region are generally high and rising.Citation11,Citation12 In addition, the principal COPD comorbidities are also frequent in this region, the prevalence of diabetes in the MENA region being one of the highest in the world (11%).Citation13,Citation14 Furthermore, it was reported in 2000 that six of the ten countries with the highest prevalence of diabetes in the world are in this region. In the first decade of this century, the prevalence of diabetes in Saudi Arabia increased from 10% in 1999 to 30% in 2009,Citation15 whereas the overall worldwide prevalence was estimated to be only 2.8% in 2000.Citation16
Data on the prevalence and the impact of COPD-related comorbidities are limited in the MENA region. BREATHE was an international study conducted in ten countries of the MENA region and in Pakistan with the aim of estimating the prevalence of COPD symptoms in the general population, and of describing smoking habits, management, and burden of COPD and related health care utilization.Citation17 The analysis described here addresses the presence of comorbidities in subjects with COPD identified in the BREATHE database. The objective of this analysis was to assess the frequency of comorbidities in subjects with COPD and their association with respiratory symptom severity and COPD exacerbations.
Materials and methods
This analysis was performed on data from the BREATHE study, the methodology of which has been described in detail elsewhere.Citation17 Briefly, this study was a cross-sectional epidemiological survey of COPD conducted in a random sample of the general population of eleven countries (Algeria, Egypt, Jordan, Lebanon, Morocco, Pakistan, Saudi Arabia, Syria, Tunisia, Turkey, and the United Arab Emirates [UAE]) between June 2010 and December 2011. The present analysis concerned data related to comorbidities associated with COPD.
Study procedures and data collection
This study was based on the population analyzed in the BREATHE study,Citation17 a population-based sample aged at least 40 years contacted by telephone. The overall response rate, defined as the ratio between the number of subjects who completed the screening questionnaire and the number of potentially eligible subjects, was 74.2%.
Three questionnaires were used in the study. The screening questionnaire, completed by 62,086 subjects,Citation17 collected data on demographics, respiratory symptoms, smoking habits, and the presence of comorbidities. The objective of the screening questionnaire was to identify subjects who fulfilled an epidemiological case definition of COPD.Citation10 In this epidemiological definition, COPD cases were defined as eligible subjects fulfilling both of the following criteria:
either: 1) diagnosis criterion – already diagnosed with COPD, emphysema, or chronic bronchitis; or 2) symptom criterion – presenting either with symptoms that fulfill the definition of chronic bronchitis or with dyspnea.
smoking criterion: lifetime smoking exposure of ≥10 pack-years.
All subjects positively screened for COPD were included in the present analysis.
The second questionnaire consisted of a detailed COPD questionnaire that was administered only to subjects screened positively for COPD (n=2,187), and collected data on symptom severity, COPD exacerbations, and comorbidities. A total of 1,392 subjects with COPD completed this questionnaire.Citation18 The characteristics of this population were similar to those screened positively for COPD (n=2,187 subjects) in terms of demographics and COPD symptoms.Citation18
Data relating to comorbidities were documented from replies to the following two questions of the detailed questionnaire.
Aside from your respiratory condition, do you suffer from any other serious or chronic health conditions?
Yes
No
If yes, what other serious or chronic health conditions do you have?
Arthritis
Asthma
Cancer or tumor
Depression
Diabetes
Cardiovascular disease
High blood pressure/hypertension
Other (specify)
The third questionnaire, which consisted of the COPD Assessment Test (CAT),Citation18,Citation19 was administered to subjects with COPD who had completed the detailed questionnaire.Citation19 The CAT documents the impact of COPD on subjects’ well-being and daily life. A score <10 indicates a low impact, a score of 10–19 a medium impact, a score of 20–40 a high to very high impact. The scores were then crossed with the presence of comorbidities. The CAT questionnaire was completed by 1,015 of the 1,392 subjects completing the detailed COPD questionnaire (72.9%).
The presence of exacerbations was assessed over a period of 6 months. Since the number of exacerbations was not documented in the BREATHE study, the GOLD (Global initiative for chronic Obstructive Lung Disease) classification was adapted according to exacerbation history (yes or no). The definition of exacerbation used in the BREATHE study has been described elsewhere.Citation18 An exacerbation was considered to have occurred in the previous 6 months if the subject fulfilled any of the following criteria:
In the last 6 months, have you been told by your physician that you have had worsening of your “respiratory condition”? Yes
In the last 6 months, have you been told by your physician that you have had acute bronchitis? Yes
In the last 6 months, what aspects of your “respiratory condition” have worsened? (Cough during the daytime, cough during the night, phlegm, breathlessness or shortness of breath and fatigue, ability to perform regular activities): at least two symptoms cited.
The CAT score and exacerbation history were used to classify subjects with COPD into four groups depending on their symptoms and risk of exacerbations, according to the recommendations of the 2011 GOLD report.Citation1 Group A was low risk (no exacerbations) and fewer symptoms (CAT score <10), group B low risk and more symptoms (CAT ≥10), group C to high risk (one or more exacerbations) and fewer symptoms, and Group D high risk and more symptoms.
Data analysis
The data presented in this study are principally descriptive. The occurrence of comorbidities was compared between subjects completing the screening questionnaire who fulfilled the criteria for COPD (n=2,187) and those that did not fulfill these criteria (n=59,707). Adjusted odds ratios were calculated controlling for potential confounding by age and sex using logistic regression analysis. The association between comorbidities on the one hand and occurrence of exacerbations, severity of COPD symptoms, and GOLD severity groups on the other was evaluated in COPD subjects who had completed the detailed COPD questionnaire (n=1,392). Study variables were compared using the χ2 test and the Mantel–Haenszel test as appropriate. All statistical tests were two-tailed, with a probability threshold of 0.05 taken as the upper boundary for significance. Analyses were performed using SPSS version 17 (SPSS Inc, Chicago, IL, USA).
Ethics
The study was conducted according to the principles of Good Epidemiological Practices. Participating subjects did not receive any financial compensation for their participation in the study. Because the survey had no repercussions on medical practice, ethics committee authorization was not required. All data collected were kept confidential and anonymous. Written informed consent was not obtained from participants as this was a telephone survey in the general population.
Study responsibilities
This study was initiated and funded by GlaxoSmithKline (the study sponsor). The study sponsor enlisted an academic steering committee to advise on the design and implementation of the study and on the analysis and interpretation of the results, for which the committee members received consultancy fees from the study sponsor. The committee members had full access to the study data, and were actively involved in the preparation of the present article. Operational management of the study and data analyses was delegated by the study sponsor to MS Health (Rabat, Morocco), an independent contract-research organization. The study sponsor funded editorial support from a medical writing agency (Foxymed, Paris, France) for the preparation of the present article.
Results
The analysis was performed on data pooled from all eleven participating countries.
Study sample
A total of 2,187 subjects fulfilled the epidemiological case definition of COPD (COPD population), of whom 1,392 completed the detailed COPD questionnaire. The latter population (n=1,392) represents the principal study population for the present analysis. The demographic characteristics of subjects screened positively or negatively for COPD are presented in . Subjects with COPD were on average older and more likely to be male than subjects without COPD.
Table 1 Characteristics of the screening population
Distribution of comorbidities
The distribution of comorbidities among subjects screened positively or negatively for COPD is presented in . A total of 29,272 subjects in the screening population (47.1%) reported at least one comorbidity. The most frequently reported comorbidity was cardiovascular disease, followed by diabetes. The presence of all comorbidities was more frequent in women than in men, and notably for cardiovascular disorders, reported in 28.8% of all women and 18.3% of all men. In both men and women, the frequency of reported comorbidities increased with age.
Table 2 Occurrence of comorbidities as a function of age and sex
Comorbidities were significantly (P<0.0001) more frequently reported in subjects screened positively for COPD (66.2%) than in controls who did not (46.5%). This corresponds to an odds ratio, adjusted for age and sex, of 2.63 (95% confidence interval 2.40–2.89). All individual comorbidities documented were also more frequent in the subjects screened positively for COPD (). Comorbidities were reported by 66.8% of COPD subjects who completed the detailed COPD questionnaire (930/1,392 subjects).
Table 3 Occurrence of comorbidities and association with COPD screen
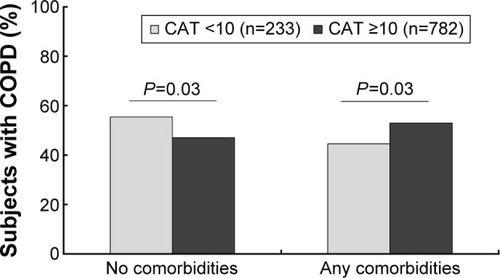
Presence of comorbidities according to CAT score
Of the COPD subjects who completed the detailed COPD questionnaire, 1,015 subjects provided CAT scores (72.9%). The majority of subjects (77.0%, n=782) reported a CAT score ≥10, indicating a high impact of respiratory symptoms on subject functioning. The distribution of comorbidities according to CAT score is presented in . The probability of reporting a comorbidity was significantly (P=0.03) higher in subjects with a CAT score ≥10 compared to those with a CAT score <10.
Figure 1 Presence of comorbidities according to CAT scores.
Presence of comorbidities according to the occurence of exacerbations
Of the 1,392 subjects with COPD who completed the detailed COPD questionnaire, a total of 661 (47.5%) subjects reported COPD exacerbations (). The association between the presence of comorbidities and the occurrence of exacerbations was assessed (). Overall, the proportion of subjects who reported exacerbations was significantly higher in the group of subjects with documented comorbidities than in those without (50.4% versus 44.6%, P=0.03 [χ2 test]). With respect to individual comorbidities, this association was no longer significant, except for asthma (P=0.003 [χ2 test]) and digestive diseases (P=0.02 [χ2 test]).
Table 4 Presence of comorbidities in COPD subjects with or without exacerbation
Presence of comorbidities according to severity of symptoms and exacerbation history
A total of 1,015 subjects were classified into GOLD severity groups according to their CAT score and exacerbation history. Overall, half of the assessed population (n=549, 54.1%) were classified into group D, consisting of subjects with severe symptoms (CAT score ≥10) and a high risk of exacerbation (one or more exacerbations within the last 6 months of the study). The distribution of subjects with comorbidities (n=518) according to severity group is presented in . The majority of subjects with comorbidities (57.8%, n=299) were classified into the group with severe symptoms and high risk of exacerbation (group D). However, the distribution of subjects between GOLD severity grades did not differ significantly between those with comorbidities and those without comorbidities (P=0.08 [χ2 test]).
Table 5 Classification of subjects with or without comorbidities according to CAT score and exacerbation history
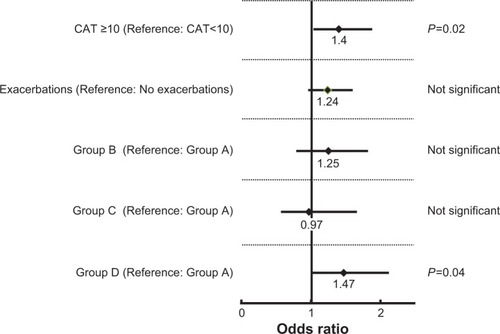
The relationship between the presence of comorbidities on the one hand and the severity of COPD or the occurrence of exacerbation on the other was evaluated in the population of subjects classified according to GOLD severity group (n=1,015). The results are presented in . The presence of comorbidities in COPD subjects was significantly associated with a high CAT score (≥10) (P=0.02) and GOLD group D (P=0.04).
Figure 2 Relationship between comorbidities, severity of COPD, and occurrence of COPD exacerbation.
Abbreviation: CAT, COPD Assessment Test.
Discussion
This analysis of the BREATHE study revealed that two-thirds of COPD subjects reported comorbidities, principally cardiovascular diseases and diabetes, a significantly higher proportion than in subjects without COPD. The presence of comorbidities was significantly associated with COPD exacerbations and a higher impact of respiratory symptoms on functioning. The majority of subjects (57.8%, n=299) with comorbidities were assigned to group D of the GOLD severity classification, the most severe grade.
The coexistence of COPD and cardiovascular diseases or diabetes found in our study has been reported in several previous studies.Citation2–Citation4,Citation20,Citation21 A recent review of 25 studies reporting cardiovascular comorbidity in COPD subjects revealed that the relative risk of occurrence of cardiovascular comorbidities among COPD subjects ranged from 2.1 to 5.0 compared to subjects without COPD.Citation4 This strong association between COPD and cardiovascular diseases may be explained by the fact that tobacco smoking is an important common risk factor for both COPD and cardiovascular diseases.Citation22 In our study, the highest rate of COPD subjects reporting cardiovascular disease and diabetes was found in the UAE (71.4% and 50.0%, respectively; data not shown). This reflects the high prevalence of these diseases in the general populations of countries in the Gulf area, as illustrated by recent national statistics from Abu Dhabi showing that in 2011, 17% of the general population had hypertension and 21% had diabetes.Citation23
This study revealed that the presence of comorbidities was significantly associated with a CAT score ≥10, which reflects a high impact of respiratory symptoms on functioning. This result is consistent with outcomes from other studies using different patient-reported outcome measures, which have highlighted the association between the presence of comorbidities and an impairment of quality of life or functioning in COPD subjects.Citation24–Citation26 The CAT threshold of ten was chosen, since this is the one recommended in the 2011 GOLD guidelines for the classification of patients with COPD,Citation1 but it cannot be excluded that the strength of the association with comorbidities may differ if another CAT threshold were to be used.
We found that the presence of comorbidities was associated with an increased risk of experiencing COPD exacerbations. There are few data available concerning the relationship between the presence of comorbidities and COPD exacerbations in COPD, although a US study has reported that patients with comorbidities presented a higher risk of exacerbations than those without.Citation27 Moreover, it is well documented that COPD exacerbations constitute a risk factor for subsequent development of cardiovascular disease.Citation4,Citation28 To our knowledge, our study is one of the first to use the GOLD severity-grade groups (A–D) in the classification of COPD subjects with comorbidities. We found that the majority of COPD subjects (57.8%) with comorbidities were classified in group D, corresponding to subjects who reported severe symptoms (CAT ≥10) and previous exacerbations. This is consistent with previous reports of more severe COPD symptoms in subjects with comorbidities.Citation29
This study had certain limitations. Since data collection was based on self-report without medical ascertainment, it is possible that this may have introduced some anamnestic bias or underreporting of information on comorbidities. Given that this was a general population survey in which spirometry could not be performed systematically, there is likely to be some imprecision in the estimation of the proportion of subjects fulfilling the epidemiological definition of COPD used in the study. Secondly, in certain countries, such as the UAE, the number of subjects who respond to the COPD detailed questionnaire and who report comorbidities is low. This precludes the analysis of the data at an individual country level, which may lead to loss of information when the prevalence of individual comorbidities, such as diabetes, varies markedly between participating countries.
Conclusion
This study showed that the prevalence of comorbidities among COPD subjects is high in the MENA region. The presence of comorbidities was associated with increased severity of COPD symptoms and exacerbations of the disease. This highlights the importance of seeking out and managing appropriately comorbidities in all individuals with a diagnosis of COPD.
Acknowledgments
The authors would like to thank all members of the BREATHE Study Steering Committee for their contributions to this study: A Alzaabi (Abu Dhabi, UAE), M Beji (Tunis, Tunisia), A Ben Kheder (Tunis, Tunisia), M Idrees (Riyadh, Saudi Arabia), G Iraqi (Rabat, Morocco), A Javed (Peshawar, Pakistan), JA Khan (Karachi, Pakistan), A Khattab (Cairo, Egypt), ML Koniski (Beirut, Lebanon), B Mahboub (Sharjah, UAE), S Nafti (Algiers, Algeria), NM Obeidat (Amman, Jordan), M Polatli (Aydin, Turkey), A Sayiner (Izmir, Turkey), N Shahrour (Damascus, Syria), MA Tageldin (Cairo, Egypt), S Taright (Algiers, Algeria), E Uzaslan (Bursa, Turkey), S Wali (Jeddah, Saudi Arabia). Foxymed also provided medical writing support in the form of writing assistance, collating authors’ comments, grammatical editing, and referencing that was paid for by GlaxoSmithKline.
Disclosure
BM, AA, and MNI have received honoraria from Glaxo-SmithKline Laboratories for their contribution to the BREATHE study. AL is an employee of MS Health, the clinical and epidemiological research company responsible for the implementation, collection of data, and statistical analysis of results of the BREATHE study. HS is an employee of Foxymed, a medical communication and consultancy company that participated in the exploration, interpretation of the results, and preparation of this manuscript on behalf of GlaxoSmithKline Laboratories. LT and AEH are employees of GlaxoSmithKline Laboratories, which funded the BREATHE study and markets a number of treatments for COPD, and own shares in the company.
References
- GOLD (Global initiative for chronic Obstructive Lung Disease)Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary DiseaseBethesda (MD)GOLD2011
- ManninoDMThornDSwensenAHolguinFPrevalence and outcomes of diabetes, hypertension and cardiovascular disease in COPDEur Respir J200832496296918579551
- FearyJRRodriguesLCSmithCJHubbardRBGibsonJEPrevalence of major comorbidities in subjects with COPD and incidence of myocardial infarction and stroke: a comprehensive analysis using data from primary careThorax2010651195696220871122
- MüllerovaHAgustiAErqouSMapelDWCardiovascular comorbidity in chronic obstructive pulmonary disease: systematic literature reviewChest201314441163117823722528
- World Health OrganizationThe Global Burden of Disease: 2004 UpdateGenevaWHO2008
- World Health OrganizationGlobal Surveillance, Prevention and Control of Chronic Respiratory Diseases: A Comprehensive ApproachGenevaWHO2007
- BarnesPJCelliBRSystemic manifestations and comorbidities of COPDEur Respir J20093351165118519407051
- BatyFPutoraPMIsenringBBlumTBrutscheMComorbidities and burden of COPD: a population based case-control studyPloS One201385e6328523691009
- de Miguel DiezJCarrasco GarridoPGarcía CarballoMDeter-minants and predictors of the cost of COPD in primary care: a Spanish perspectiveInt J Chron Obstruct Pulmon Dis20083470171219281084
- TageldinMANaftiSKhanJADistribution of COPD-related symptoms in the Middle East and North Africa region: results of the BREATHE studyRespir Med2012106Suppl 2S25S3223290701
- KhattabAJavedAIraquiGSmoking habits in the Middle East and North Africa region: results of the BREATHE studyRespir Med2012106Suppl 2S16S2423290700
- World Health OrganizationPrevalence of tobacco use among adults and adolescents2012 Available from: http://gamapserver.who.int/gho/interactive_charts/tobacco/use/atlas.htmlAccessed December 1, 2015
- International Diabetes FederationIDF Diabetes Atlas5th edBrusselsIDF2012
- SherifSSumpioBEEconomic development and diabetes prevalence in MENA countries: Egypt and Saudi Arabia comparisonWorld J Diabetes20156230431125789111
- AlqurashiKAAljabriKSBokhariSAPrevalence of diabetes mellitus in a Saudi communityAnn Saudi Med2011311192321245594
- WildSRoglicGGreenASicreeRKingHGlobal prevalence of diabetes: estimates for the year 2000 and projections for 2030Diabetes Care20042751047105315111519
- El HasnaouiARashidNLahlouASalhiHDobleANejjariCChronic obstructive pulmonary disease in the adult population within the Middle East and North Africa region: rationale and design of the BREATHE studyRespir Med2012106Suppl 2S3S1523290702
- IdreesMKoniskiMLTarightSManagement of chronic obstructive pulmonary disease in the Middle East and North Africa region: results of the BREATHE studyRespir Med2012106Suppl 2S33S4423290703
- JonesPWShahrourNNejjariCPsychometric evaluation of the COPD Assessment Test (CAT): data from the BREATHE study in the Middle East and North Africa regionRespir Med2012106Suppl 2S86S9923290707
- SinDDAnthonisenNRSorianoJBAgustiAGMortality in COPD: role of comorbiditiesEur Respir J20062861245125717138679
- SchnellKWeissCOLeeTThe prevalence of clinically-relevant comorbid conditions in patients with physician-diagnosed COPD: a cross-sectional study using data from NHANES 1999–2008BMC Pulm Med2012122622695054
- CavaillèsABrinchault-RabinGDixmierAComorbidities of COPDEur Respir Rev20132213045447524293462
- Health Authority Abu DhabiHealth Statistics 2011Abu DhabiHAAD2012
- AlmagroPCastroAHelping COPD patients change health behavior in order to improve their quality of lifeInt J Chron Obstruct Pulmon Dis2013833534523901267
- FortinMDuboisMFHudonCSoubhiHAlmirallJMultimorbidity and quality of life: a closer lookHealth Qual Life Outcomes200755217683600
- YeoJKarimovaGBansalSComorbidity in older patients with COPD – its impact on health service utilisation and quality of life, a community studyAge Ageing2006351333716364931
- Rascon-AguilarIEPamerMWludykaPRole of gastroesophageal reflux symptoms in exacerbations of COPDChest200613041096110117035443
- WalterREWilkJBLarsonMGSystemic inflammation and COPD: the Framingham Heart StudyChest20081331192517908709
- YawnBPKaplanAComorbidities in people with COPD: a result of multiple diseases, or multiple manifestations of smoking and reactive inflammation?Prim Care Respir J200817419920518338090