
Abstract
Aim
The aim of this study was to investigate the effects of high-intensity aerobic training (AT) and high-intensity aerobic training combined with resistance training (ie, combined training [CT]) on cognitive function in patients with COPD.
Methods
Twenty-eight Caucasian male patients (68.35±9.64 years; mean ± SD) with COPD were recruited and randomized into two groups, AT and CT. Both groups performed physical reconditioning for 4 weeks, with a frequency of five training sessions per week. The CT group completed two daily sessions of 30 minutes: one aerobic session and one strength session, respectively; The AT group performed two 30-minute aerobic endurance exercise sessions on treadmill. Physical and cognitive function tests were performed before and after the training intervention performances.
Results
Exercise training improved the following cognitive functions: long-term memory, verbal fluency, attentional capacity, apraxia, and reasoning skills (P<0.01). Moreover, the improvements in the CT group were significantly greater than those in the AT group in long-term memory, apraxia, and reasoning skills (P<0.05).
Conclusion
CT may be a possible strategy to prevent cognitive decline and associated comorbidities in male patients with COPD.
Introduction
COPD is a complex multicomponent disorder with significant physical, psychological, and cognitive sequels that reduce the quality of life. COPD is associated with many extrapulmonary disorders that contribute to increased morbidity and mortality.Citation1 Cognitive decline is an associated pathologyCitation2 that affects 77% of patients with COPD.Citation3 This disturbance is probably a consequence of the neuronal damage produced by hypoxemia. Patients with COPD have an altered cerebral perfusion due to arterial oxygen desaturationCitation4 that may result in cognitive impairments.Citation5,Citation6
Cognitive impairment associated with COPD differs from Alzheimer disease.Citation7,Citation8 The neuropsychological impairment associated with COPD has a specific pattern characterized by moderate-to-severe deficits in isolated domains, such as attention, memory, executive functions, language skill, psychomotor speed, and complex visual-motor processes.Citation9 Exercise training is associated with maintenance and improvement of physical and cognitive functioning and psychological well-being.Citation10,Citation11
A meta-analysis of randomized controlled trials showed that a 14% improvement in aerobic activity coincided with an improvement in cognitive capacity.Citation12 However, despite the well-established link between exercise training and improved cognitive function, no specific training protocols exist.Citation13 Furthermore, it is unclear if the positive effects of physical activity on cognition in patients with COPD confer long-term benefits. The majority of exercise training interventions on cognitive function have primarily focused on aerobic endurance training, called aerobic training (AT). Consequently, the aim of this study was to compare the effects of high-intensity resistance training combined with AT (ie, combined training [CT]) vs aerobic endurance exercise intervention alone on cognitive function in patients with COPD.
Materials and methods
This study is a randomized controlled study, with two measurement periods (baseline and trial completed). The assessors of the cognitive and physical tests were formally blinded, whereas the participants and the trainers were not blinded.
Twenty-eight Caucasian male patients with mild- to-moderate COPD (I and II levels following the Gold Classification)Citation14 were recruited for this study (mean age 68.35±9.64 years). The inclusion criteria for the enrollment were as follows: age >50 years; former smokers, Tiffenau index (forced expiratory volume in the first second [FEV1]/forced vital capacity [FVC]) <70% and FEV1 postbronchodilator <80% of predicted value, reversibility of FEV1 <12% of basic value and <200 mL of absolute value (30 minutes after 400 mg salbutamol inhalation), and stable COPD diagnosis. The exclusion criteria were as follows: contraindication for physical activity practice; usage of oxygen therapy; evidence of dementia, evaluated by Mini-Mental State Evaluation;Citation15 history of brain injury; history of stroke; history of alcoholism; presence of anxiety and depressive symptoms, evaluated, respectively, by Hamilton Rating Scale for AnxietyCitation16,Citation17 and Beck Depression Inventory;Citation18,Citation19 usage of medication influencing cognition; and presence of comorbidity incompatible with the experimental protocol practice. A written consent was obtained from the participants after their being thoroughly informed of the purpose and potential risks of the study. The experimental procedures were designed and conducted following the ethical principles laid out in the 2008 revision of the Declaration of Helsinki, and they were approved by the Ethical Committee of the University of Molise.
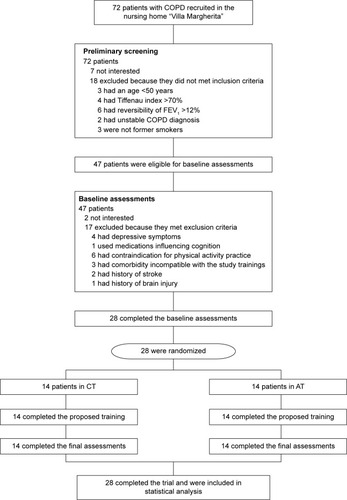
The recruitment process was conducted as follows: 72 patients with COPD at the nursing home “Villa Margherita” were enrolled during the 2 months prior to the beginning of the interventional protocols (July and August, 2014) and were considered as eligible. All these patients had not yet been included in any standard rehabilitation program. Successively, the patients were filtered on the basis of the inclusion and exclusion criteria and motivation to participate in the study. Twenty-eight participants met all these criteria. These participants carried out the physical interventions from September 1 to September 26, 2014, and they performed both the pre- and post-assessments. During the interventions, no dropouts occurred. More details about the recruitment and intervention timeline are reported in .
Figure 1 Flow-chart of the study.
Abbreviations: AT, aerobic training; CT, combined training; FEV1, forced expiratory volume in the first second.
The patients were randomized into two groups of equal numerosity (characteristics are shown in ): the first group, called CT (n=14), performed a training protocol composed by high-intensity aerobic and resistance exercises, associated with respiratory, balance, and mobility exercises; and the second group, called AT (n=14), performed a training protocol composed by high-intensity aerobic exercises, associated with respiratory, balance, and mobility exercises.
Table 1 Sample characteristics
Both groups performed two training sessions per day, the first one in the morning and the second one in the afternoon, for 5 days/wk, for a total of ten training sessions per week, for 4 weeks. The duration of each session was 30 minutes. Before and after the 30 minutes, the patients performed 5 minutes of warm-up (walking on the treadmill at 35% VO2max) and cooldown (stretching exercises), respectively. The description of the exercises and their progression of two protocols are reported in .
Table 2 Description of two protocols of training
The patients in both groups were tested, before and after the intervention period, on their cognitive performance with a battery of neurocognitive tests. These tests were chosen for their high reliability and reproducibility and because they have been already used in COPD population.Citation20
The tests are described as follows, starting from those whose results were considered as primary outcomes:
Rey 15-item memory test (or Rey test) is used to assess verbal memory.Citation21 In this test, the examiner reads 15 words, and the patients are told to remember all the 15 presented words, independently from their order. The 15 words are read again, and the patients are required to say all the words that they remember for the second time. This sequence of listening and repeating is performed five times, and one point is assigned for each remembered word during each sequence, for a maximum score of 75 points (Rey-immediate recall). After the last sequence, the patients are distracted for 15 minutes, and then they are required to say all the words that they remember in order to evaluate the long-term memory performance. One point is assigned for each remembered word for a maximum of 15 points (Rey-delayed recall [DR]).
Drawing copy test is used to evaluate praxis abilities.Citation22 In the first part of the test (drawing test I), the patient must copy three geometric drawings. The score is calculated on the basis of the adherence to the original model. The range of the assigned score is from 0 (the worst – no adherence at all) to 4 (the best – perfect adherence) for each drawing (total test score ranges from 0, the worst, to 12 – the best). In the second part of the test (drawing test II), the patient must complete a series of 12 uncompleted geometric drawings to obtain one of the three geometric models used in the first part of the test. The score is calculated assigning one point for each correct line drawn (maximum score of 70), so the total score is from 0 (worst) to 70 (best). In this case also, the time to complete the entire test was considered as scores.
The secondary outcomes of the study were instead the results of the following tests:
Attentive matrices test (attentive test) is a valid instrument to measure the selective and sustained attention.Citation23 It consists of three numeric matrices (ten columns of 13 numbers from 0 to 9). The participants are required to check specific target numbers in 45 seconds for each matrix. There is one target in the first matrix, two in the second one, and three in the third one. The score is calculated by assigning one point for each target correctly found in the three matrices (maximum of 60 for all the three matrices). The time to complete the three matrices is considered as score.
Raven’s progressive matrices tests (or Raven test) are multiple choice intelligence tests of abstract reasoning.Citation24 The test is composed of three series of 12 figures for a total of 36 figures. In each figure, the patient is asked to analyze a geometric pattern and to identify the correct missing piece among the four or six proposed pieces. One point is assigned for each missing piece that the patient correctly pointed out, so that the total score ranges from 0 (worst) to 36 (best).
Verbal fluency test is a test for the verbal fluency assessment.Citation25 In this test, the patient is required to list, in 2 minutes, all the words he knows concerning the four categories: colors, animals, fruits and names of cities (eg, in the category colors, the patient has to list white, black, red, etc.). The scores are calculated assigning one point for each correct word cited, divided into four. The range of scores is from 0 (very poor) to infinite (higher score = higher performance). Furthermore, the patients were tested relative to their physical levels. In order to verify the effectiveness of the proposed physical training, the patients were tested with the 6 minutes walking test, for the indirect evaluation of aerobic capacity (VO2max), whereas the one-repetition maximum was used to evaluate the muscle strength of quadriceps and arms (respectively, measured by leg extension and arm curl isotonic machines), and the data are reported in . The one-repetition maximum was estimated by BrzyckiCitation26 using the submaximum method in order to assure the safety of the participants. The intensity of the aerobic sessions, expressed as percentage of heart rate maximum, was monitored in both groups through heart rate monitors. The heart rate maximum was calculated using the Tanaka formula. The Borg Scale was also used to evaluate the rate of perceived exertion.
Table 3 Physical assessment results
Statistics
Participants’ randomization into the two groups was performed using a random number list, generated using the online software (https://www.random.org/sequences/, Dublin, Ireland). The procedure described was as follows: a progressive number was assigned to each of the participants in alphabetical order according to their surname; a random number list was subsequently generated; and, in accordance with this random number list order, the participants were allocated in blocks of two participants per group in the order CT and AT. After randomization, analysis of variance (ANOVA) and chi-squared analysis were performed to verify that the four groups were homogeneous at baseline in terms of participants’ age, instruction levels, functional status, Medical Research Council Scale scores, severity of the COPD, comorbidities, medications, and cognitive scores.
A multivariate ANOVA with repeated measures was performed to evaluate significant differences between the scores obtained in cognitive test: the two groups were used as between factor for analysis (CT vs AT), whereas the score obtained after and before the training period was used as within factor (pre vs post) and the scores obtained in the cognitive test were used as dependent variables. ANOVA with repeated measures was instead performed to evaluate significant differences on FEV1 and FEV1/FVC between the two groups and between pre- and post-evaluation.
Furthermore, Pearson correlation analysis was performed between the variations in cognitive scores and the variations in physical scores (variations calculated as Δ that was postscores minus prescores), in order to verify if a correlation existed between physical performance and cognitive modifications.
The alpha level for the analyses was set at 0.05. The analysis was performed using the Statistical Package for the Social Sciences (v.20.0; IBM Corporation, Armonk, NY, USA).
Results
After the randomization, the two groups were homogeneous in terms of age, instruction levels, functional status, Medical Research Council Scale scores, severity of the COPD, comorbidities, medications, and cognitive scores.
The multivariate ANOVA with repeated measures showed significant differences both between the pre- vs post-exercise training scores (F7,20=80.884; P<0.001) and between the two intervention groups (F7,20=3.216; P=0.019) and in the interaction time × groups (F7,20=4.534; P=0.004). The univariate analysis showed significant differences in between pre- vs postscores in Rey-DR, verbal fluency, attentive matrices, copy drawing II, and Raven test (with F1,26 between 27.994 and 75.214; P<0.001 for all the five tests). The CT group significantly improved in Rey-DR, copy drawing II, and Raven matrices (F1,26 between 4.872 and 5.314; P<0.05 for all the three tests) to a greater extent than the AT group. The univariate analysis also showed significant differences in the interaction time × groups in Rey-DR (F1,26=5.652; P=0.025), Raven test (F1,26=5.792; P=0.023), and copy drawing I (F1,26=10.156; P=0.004). These results are shown in . No significant differences were found in FEV1 and FEV1/FVC both between pre- and postevaluation and between the two groups. Furthermore, low or no significant correlations between functional and cognitive improvements were found.
Table 4 Results obtained by the two groups in the cognitive tests
Discussion
The main finding of this study concerns the improvement in cognitive function observed after 4 weeks of exercise training at high intensity. This result supports the idea that physical training has the potential to improve cognitive ability in patients with COPD.Citation10,Citation27
The second significant finding refers to the comparison between two types of training intervention at high intensity. The CT group displayed a significantly greater improvement in the Rey-DR, Raven test, and copy drawing I assessments compared to AT group. These results suggest that the strength training combined with AT can maximize the effects of physical training on cognition in patients with COPD. There is a dearth of data investigating the effects of resistance or combined resistance and aerobic exercise training interventions on cognitive function in patients with COPD.
The majority of previous training intervention studies in cognitive functions have utilized aerobic endurance exercise in isolationCitation13,Citation28 performed with moderate intensity.Citation29 The effects of physical exercise on cognitive performance appear to be attributable to various factors.Citation30
It is well known that the physical activity influences endocrine homeostasis, such as cortisol, testosterone, growth hormone, and hypothalamic hormones,Citation31 and the hormonal adaptation may be a possible mechanism mediating the positive effects of training. Furthermore, several hormones, influenced by physical activity, produce effects on psychological well-being through the reduction of cortisol, which causes an antidepressive effect.Citation32 The mood state improvement may indirectly facilitate the cognitive functions.Citation33 Consequently, it was hypothesized that the effects of exercise on cognition may be attributable to an emotional response that introduces noradrenalin into the central nervous system (CNS) directly.Citation34 In particularly serotonin and β-endorphin,Citation35 give positive effects on mood and they may act as a physiological modulators for memory.Citation36
The execution of free weight resistance exercises promotes a better development of coordinative ability, due to the higher levels of mental effort required for the executions of this type of exercises.Citation37 Little is known about the neuronal mechanisms involved in the increased neuronal drive in the early stages of strength training, although it has been suggested that this training increased cortical drive to the spinal motoneurons.Citation38 Strength increments arise as a consequence of numerous factors, but it would make sense to consider strength training as a kind of motor-learning process.Citation39 Moreover, as shown in a recent study, resistance training can improve the respiratory muscle performance with potential positive effects on blood oxygenation, and consequently, the cognition performance of patients with COPD.Citation40 Despite there being no direct evidences of the effectiveness of resistance training in improving the quality of life of patients with COPD, a recent meta-analysisCitation41 showed that resistance training should be incorporated in COPD rehabilitation programs, for positive effects of muscle strength, especially in leg muscles. This aspect may play an important role in delaying the disease progression and also in improving patients’ (including COPD) self-efficacy perception. Further studies will confirm this hypothesis. The aerobic component of the training, conducted intensively, may increase the ability of the heart to delivery oxygenCitation42 and it is possible to assume that it could be the physiological mediator of several mental health benefits related to a better oxygenation and a greater blood flow in cerebral areas. These physiological adaptations probably compensate the hypoxemic damage that characterizes the patients with COPD.Citation28,Citation30,Citation43 On the basis of previous studies, it was hypothesized that aerobic exercises may produce an increase in hippocampus volume and the stimulation of brain-derived neurotrophic factor, which positively influences the memory performances.Citation28,Citation44
In the human brain, aerobic exercise can increase the oxidative capability, developing a trophic effect in cerebral centers involved in sensory-motor function and in the central executive function related to the frontal lobe. The hippocampus volume might also be improved by high level of fitness training in humans.Citation45
The possible beneficial effects of exercise on blood circulation in patients with COPD are also suggested by the results of a recent study of Zambom-Ferraresi et al,Citation46 reporting a heart rate and blood lactate reduction, especially during aerobic combined with resistance training, in which strength improvements due to resistance training maximize the AT benefits. In addition, acute physical exercise, based on the combination of AT and resistance training, may improve cognitive performance by changing the levels of neurotransmitters in CNS, such as acetylcholine, dopamine, norepinephrine, epinephrine, adrenocorticotropic hormone, and vasopressin.Citation47,Citation48 These molecules are important neurotransmitters of the CNS and are able to promote cognitive function.Citation36
In conclusion, this study has demonstrated from a clinical point of view that the use of combined protocol could be more useful than AT alone in order to improve cognition. These results have been recently highlighted by a meta-analysis of Kelly et al.Citation49
A recent study concerning the exercise effects on cognition showed different benefits induced by different kinds of physical activity.Citation50 Variety in the exercise proposals may be recommended to promote cognition improvements in patients with COPD.
Conclusion
Strategies to improve neurocognitive functioning have important health implications to contrast neural degeneration in COPD. Subclinical neurocognitive deficits are associated with an increased risk of neurocognitive impairment, dementia, and mortality.Citation51
One strategy to improve neurocognitive functioning, which has gained increased attention, is the use of a combined exercise training intervention, in contrast to aerobic endurance training per se. For this reason, the CT protocol could be a possible means for the cognitive rehabilitation of patients with COPD. The moderate number of patients recruited may be a limitation for this study. It was due to the difficulty in recruiting patients with COPD who could be included in the experimentation. Moreover, this study did not analyze specifically the mechanism by which physical activity may improve the status of patients with COPD, and for this reason, the authors can only speculate on these mechanisms to explain the obtained findings.Citation30
Acknowledgments
The authors wish to thank Dr Stefano Moffa for his help.
Disclosure
The authors report no conflicts of interest in this work.
References
- WoutersEFCreutzbergECScholsAMSystemic effects in COPDChest2002121127130
- MeekPMLareauSCAndersonDMemory for symptoms in COPD patients: how accurate are their reports?Eur Respir J200118347448111589344
- GrantIHeatonRKMcSweenyAJAdamsKMTimmsRMNeuropsychologic findings in hypoxemic chronic obstructive pulmonary diseaseArch Intern Med1982142147014767103628
- OrtapamukHNaldokenSBrain perfusion abnormalities in chronic obstructive pulmonary disease: comparison with cognitive impairmentAnn Nucl Med20062029910616615418
- DustmanREEmmersonRShearerDPhysical activity, age, and cognitive neuropsychological functionJ Aging Phys Act19942143181
- MarchalGRiouxPPetit-TaboueMCRegional cerebral oxygen consumption, blood flow, and blood volume in healthy human agingArch Neurol199249101310201417508
- StussDTPeterkinIGuzmanDAGuzmanCTroyerAKChronic obstructive pulmonary disease: effects of hypoxia on neurological and neuropsychological measuresJ Clin Exp Neuropsychol19971945155249342687
- IsoahoRPuolijokiHHuhtiELaippalaPKivellaSLChronic obstructive pulmonary disease and cognitive impairment in the elderlyInt Psychogeriatr1996811131258805092
- LieskerJJPostmaDSBeukemaRJCognitive performance in patients with COPDRespir Med200498435135615072176
- DoddJWGetovSVJonesPWCognitive function in COPDEur Respir J201035491392220356988
- KozoraETranZVMakeBNeurobehavioral improvement after brief rehabilitation in patients with chronic obstructive pulmonary diseaseJ Cardiopulm Rehabil20022242643012464831
- AngevarenMAufdemkampeGVerhaarHJAlemanAVanheesLPhysical activity and enhanced fitness to improve cognitive function in older people without known cognitive impairmentCochrane Database Syst Rev2008162CD005381
- EtnierJLBerryMFluid intelligence in an older COPD sample after short-or long-term exerciseMed Sci Sports Exerc200133101620162811581543
- PauwelsRABuistASCalverleyPMJenkinsCRHurdSSGlobal strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary diseaseAm J Respir Crit Care Med201416351256127611316667
- PeruzzaSSergiGVianelloAChronic obstructive pulmonary disease (COPD) in elderly subjects: impact on functional status and quality of lifeRespir Med200397661261712814144
- BeckATEpsteinNBrownGSteerRAAn inventory for measuring clinical anxiety: psychometric propertiesJ Consult Clin Psychol19885668938973204199
- HillKGeistRGoldsteinRSLacasseYAnxiety and depression in end-stage COPDEur Respir J200831366767718310400
- BeckATSteerRACarbinMGPsychometric properties of the Beck depression inventory: twenty-five years of evaluationClin Psychol Rev19888177100
- LightRWMerrillEDesparsJAGordonGHMutalipassiLRPrevalence of depression and anxiety in patients with COPD. Relationship to functional capacityChest198587135383965263
- IncalziRAMarraCGiordanoACognitive impairment in chronic obstructive pulmonary diseaseJ Neurol2003250332533212638024
- ReyAMemorisationd’uneserie de 15 mots en 5 repetitions [storing a series of 15 words in 5 series]ReyAL’examen clinique en psycologie. [Clinical examination in psychology]Paris, FrancePresses Universitaires des France1958139193 French
- CaltagironeCGainottiGMasulloCMiceliGValidity of some neuropsychological tests in the assessment of mental deteriorationActa Psychiatr Scand19796015056474177
- SpinnlerHTognoniGItalian Group on the Neuropsychological Study of Ageing: Italian standardization and classification of neuropsychological testsItal J Neurol Sci19876811203654168
- RavenJThe Raven’s progressive matrices: change and stability over culture and timeCogn Psychol200041114810945921
- KaszniakAWGarronDCFoxJHBergenDHuckmanMCerebral atrophy, EEG slowing, age, education, and cognitive functioning in suspected dementiaNeurology197929912731279573407
- BrzyckiMStrength testing-predicting a one-rep max from reps-to-fatigueJ Phys Educ Recreat Dance19936418890
- EmeryCFShermerRLHauckERHsiaoETMacIntyreNRCognitive and psychological outcomes of exercise in a 1-year follow-up study of patients with chronic obstructive pulmonary diseaseHealth Psychol200322659860414640857
- EtnierJJohnstonRDagenbachDPollardRJRejeskiWJBerryMThe relationships among pulmonary function, aerobic fitness, and cognitive functioning in older COPD patientsChest1999116495396010531159
- SmithPJBlumenthalJAHoffmanBMAerobic exercise and neurocognitive performance: a meta-analytic review of randomized controlled trialsPsychosom Med201072323920223924
- KashiharaKMaruyamaTMurotaMNakaharaYPositive effects of acute and moderate physical exercise on cognitive functionJ Physiol Anthropol200928415516419652447
- KraemerWJRatamessNAHormonal responses and adaptations to resistance exercise and trainingSports Med200535433936115831061
- MeadGEMorleyWCampbellPGreigCAMcMurdoMLawlorDAExercise for depressionCochrane Database Syst Rev20093CD00436619588354
- FoxKRThe influence of physical activity on mental well-beingPublic Health Nutr200923a41141810610081
- McMorrisTTallonMWilliamsCIncremental exercise, plasma concentrations of catecholamines, reaction time, and motor time during performance of a noncompatible choice response time taskPercept Mot Skills200397259060414620248
- WeickerHStrüderHKInfluence of exercise on serotonergic neuromodulation in the brainAmino Acids2001201354711310929
- GoldPEZornetzerSFThe mnemon and its juices: neuromodulation of memory processesBehav Neural Biol19833821511896139106
- HeynPCJohnsonsKEKramerAFEndurance and strength training outcomes on cognitively impaired and cognitively intact older adults: a meta-analysisJ Nutr Health Aging200812640140918548179
- AagaardPSimonsenEBAndersenJLMagnussonPDyhre-PoulsenPNeural adaptation to resistance training: changes in evoked V-wave and H-reflex responsesJ Appl Physiol2002922309231812015341
- JensenJLMarstrandPCNielsenJBMotor skill training and strength training are associated with different plastic changes in the central nervous systemJ Appl Physiol20059941558156815890749
- NevesLChiappaADa SilvaVComparative effects of inspiratory muscle training and resistance training on respiratory and skeletal muscle strength in COPD: responses of the a pulmonary rehabilitation programEur Respir J201444suppl 58598
- IepsenUWJørgensenKJRingbækTHansenHSkrubbeltrangCLangePA combination of resistance and endurance training increases leg muscle strength in COPD: an evidence-based recommendation based on systematic review with meta-analysesChron Respir Dis201512213214525767138
- NelsonMERejeskiWJBlairSNPhysical activity and public health in older adults: recommendation from the American College of Sports Medicine and the American Heart AssociationMed Sci Sports Exerc20073981435144517762378
- BakerLDFrankLLFoster-SchubertKEffects of aerobic exercise on mild cognitive impairment: a controlled trialArch Neurol2010671717920065132
- EricksonKIPrakashRSVossMWAerobic fitness is associated with hippocampal volume in elderly humansHippocampus200919101030103919123237
- ChurchillJDGalvezRColcombeSSwainRAKramerAFGreenoughWTExercise, experience and the aging brainNeurobiol Aging200223594195512392797
- Zambom-FerraresiFCebolleroPGorostiagaEMEffects of combined resistance and endurance training versus resistance training alone on strength, exercise capacity, and quality of life in patients with COPDJ Cardiopulm Rehabil Prev2015351825068394
- RikliREEdwardsDJEffects of a three-year exercise program on motor function and cognitive processing speed in older womenRes Q Exerc Sport199162161672028094
- PoehlmanETGardnerAWGoranMIInfluence of endurance training on energy intake, norepinephrine kinetics, and metabolic rate in older individualsMetabolism19924199419481518423
- KellyMELoughreyDLawlorBARobertsonIHWalshCBrennanSThe impact of exercise on the cognitive functioning of healthy older adults: a systematic review and meta-analysisAgeing Res Rev201416123124862109
- IulianoEDi CagnoAAquinoGEffects of different types of physical activity on the cognitive functions and attention in older people: a randomised controlled studyExp Gerontol20157010511026183691
- MartinezCHRichardsonCRHanMKCigolleCTChronic obstructive pulmonary disease, cognitive impairment, and development of disability: the health and retirement studyAnn Am Thorac Soc20141191362137025285360