
Abstract
Background
The optimal antiplatelet regimen after in-coronary intervention among patients presenting with complex coronary artery lesions or acute coronary syndrome (ACS) has remained unclear. This study sought to evaluate the clinical outcomes of triple antiplatelet treatment (TAPT) (cilostazol added to aspirin plus clopidogrel) in these patients.
Methods
The PubMed, EMBASE, MEDLINE, and other Internet sources were searched for relevant articles. The primary end point was major adverse cardiac events (MACE), including all-cause mortality, myocardial infarction, and target vessel revascularization. The incidence of definite/probable stent thrombosis and bleeding were analyzed as the safety end points.
Results
Eleven clinical trials involving 9,553 patients were analyzed. The risk of MACE was significantly decreased following TAPT after stent implantation in the ACS subgroup (odds ratio [OR]: 0.72; 95% confidence interval [CI]: 0.61–0.85; P<0.001), which might mainly result from the lower risk of all-cause mortality in this subset (OR: 0.62; 95% CI: 0.48–0.80; P<0.001). The risk of bleeding was not increased with respect to TAPT.
Conclusion
TAPT after stent implantation was associated with feasible benefits on reducing the risk of MACE, especially on reducing the incidence of all-cause mortality among patients suffering from ACS, without higher incidence of bleeding. Larger and more powerful randomized trials are still warranted to prove the superiority of TAPT for such patients.
Introduction
Since the application of the rapidly developed interventional techniques widely in the clinic, improved clinical outcomes have been reported among patients with coronary artery disease (CAD), especially those suffering from acute coronary syndrome (ACS) or presenting with complex coronary artery lesions.Citation1 Though successful stenting is considered to strengthen these beneficial effects, the risk of stent thrombosis (ST) and restenosis among these patients is still high, which are considered frequent causes of death and recurrent myocardial infarction (MI) derived from the superimposition of a platelet-rich thrombus.Citation2 As a result, a routine dual antiplatelet treatment (DAPT) consisting of aspirin and a P2Y12 receptor antagonist has been chosen as an adjuvant therapy after percutaneous coronary intervention (PCI).Citation3 However, ~10% of patients undergoing stent implantation receiving DAPT developed thrombotic events leading to high morbidity and mortality,Citation4,Citation5 which were thought to be driven by high on-treatment platelet reactivity (HTPR).Citation6 Currently, overcoming HTPR and optimizing the antiplatelet regimen post-PCI for these patients still remain as important problems.
Cilostazol is a selective inhibitor of phosphodiesterase III, which inhibits platelet aggregation in response to ADP, epinephrine, collagen, and arachidonic acid.Citation7 It can also suppress the production of platelet-derived endothelial cell growth factor, which is considered to drive its extensive application in patients undergoing stent implantation.Citation7,Citation8
In recent years, several large observational clinical trials (Obs)Citation9,Citation10 and meta-analysesCitation11,Citation12 have demonstrated that adding cilostazol to aspirin plus clopidogrel decreased the risk of major adverse cardiac events (MACE) compared to the conventional dual regimen. A recent meta-analysis published by Bundhun et al,Citation13 as well as several other randomized trials,Citation14,Citation15 had stated the superiority of triple antiplatelet therapy (TAPT) for type 2 diabetes mellitus (T2DM) patients after intracoronary stenting procedure. The large randomized controlled trial (RCT) conducted by Lee et alCitation16 indicated lower risk of late luminal loss, percentage intimal hyperplasia volume, and angiographic restenosis related to the TAPT, resulting in decreased risk of target lesion revascularization (TLR) after 12-month follow-up. However, the COronary BIfurcation Stent (COBIS) II Registry,Citation17 focused on patients with bifurcation lesions, showed that TAPT post-PCI had no beneficial effects on reducing the risk of long-term clinical outcomes, and another clinical trialCitation18 showed similar negative results of TAPT among patients suffering from unprotected left main (LM) disease. Of note, patients suffering from ACS or with complex coronary artery lesions are highly likely to develop thrombotic events after stent implantation. These conflicting data have called the optimal antiplatelet regimen into question, and there is no related meta-analysis paying attention to this topic. Therefore, we performed this meta-analysis involving as many related clinical trials as possible to evaluate the efficacy and safety of TAPT compared to DAPT after stent implantation for patients suffering from ACS or with complex coronary artery lesions.
Methods
Literature search
The references comparing clinical outcomes of TAPT with DAPT post-PCI among patients presenting with complex coronary artery lesions (defined as long coronary artery lesions, chronic total occlusion lesions, unprotected LM lesions, bifurcation lesions, multivessel artery disease, or the composite of all these) and/or suffering from ACS were searched in the PubMed, EMBASE, MEDLINE, and the Cochrane Controlled Trials Registry from their dates of inception until June 2016, as well as several other Internet sources. Combinations of several relevant keywords were used to make sure all relevant studies were included, including “triple antiplatelet therapy”, “TAPT”, “dual anti-platelet therapy”, “DAPT”, “acute myocardial infarction or AMI”, “acute coronary syndrome or ACS”, “chronic total occlusion”, “left main”, “bifurcation”, “long lesions”, “stent implantation”, “percutaneous coronary intervention” or “PCI”. All potentially relevant citations and references from published reviews or meta-analyses were subsequently screened for eligibility.
Inclusion and exclusion criteria
The included studies were required to fulfill the following criteria: 1) adult patients with complex coronary artery lesions and/or suffering from ACS (age range: 18–90 years) undergoing stent implantation; 2) clinical trials comparing the TAPT and the DAPT groups; and 3) reported results of adverse clinical events. The exclusion criteria were as follows: 1) patients with cardiogenic shock; 2) nonhuman or ongoing studies; 3) non-English-language studies; 4) reviews or meta-analyses; and 5) duplicated studies, or different studies using the same sample.
Data extraction, synthesis, and quality assessment
All relevant articles were reviewed by two independent investigators (FZG and DGB) using standardized data abstraction forms to assess their eligibility. The third investigator (LXB) resolved disagreements. These following data were extracted from each included study: the name or the first author of the trial, publication year, baseline demographics, characteristics of lesions, details of antiplatelet regimens and PCI procedure, as well as clinical outcomes during follow-up. These included trials were divided into two subgroups, described as the “complex lesions” subgroup and the “ACS” subgroup. The quality of all retrieved studies was assessed according to the Newcastle–Ottawa Scale (NOS)Citation19 and the Jadad scoreCitation20 for the cohorts and randomized studies, respectively.
Study end points
The primary end point of this study was incidence of MACE, including all-cause mortality, MI (including both Q-wave MI and non-Q-wave MI) and target vessel revascularization (TVR) (TLR was used instead in one trial due to the absence of relevant dataCitation10). The secondary end point was the risk of stroke. The incidence of definite/probable ST, according to the definition of the Academic Research Consortium,Citation21 and bleeding, including major and minor bleeding, were chosen to be evaluated as the safety end points. There were slight differences among these included trials in terms of the definitions of clinical end points, and standardized definitions were followed.
Statistical analysis
This meta-analysis was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement.Citation22 STATA 12.0 (StataCorp LP, College Station, TX, USA) was used to perform the statistical analysis. All the end points were applied as dichotomous variables, expressed with odds ratios (ORs) and 95% confidence intervals (CIs). When a P-value was less than 0.05, it was considered statistically significant. The Cochran’s Q test and the I2 statistic were used to measure statistical heterogeneity. Significant heterogeneity was considered and a random-effects model would be selected if the P-value of the Q test was <0.10 and/or the I2 was ≥50%. In contrast, the fixed-effects model with the Mantel–Haenszel method was used instead. Publication bias was examined via the Egger’s test (P<0.1 for significant asymmetry).Citation23 The sensitivity analyses were also performed by excluding one study at a time to assess the stability of the overall treatment effects. All of the P-values were two tailed.
Results
Eligible studies and patient characteristics
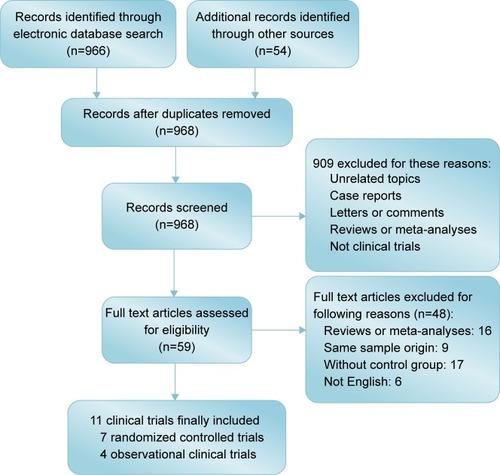
After screening 996 initial articles through the electronic databases and another 54 articles from several other Internet sources, 11 clinical trials were finally identified, including 7 RCTsCitation16,Citation24–Citation29 and 4 ObsCitation9,Citation10,Citation17,Citation18 (). Among these included clinical trials, there were 2 trials for long artery lesions,Citation16,Citation24 1 for unprotected LM disease,Citation18 1 for bifurcation lesion,Citation17 and 1 for mixed complex lesions.Citation29 Another 6 clinical trials focused on patients suffering from ACS.Citation9,Citation10,Citation25–Citation28 Only 1 observational trialCitation17 performed subanalysis following propensity score matching, and the data were analyzed from the matched subgroup instead. The baseline characteristics, antiplatelet regimens and procedural details of the included studies are summarized in –. The qualities of included studies are described in .
Table 1 Baseline characteristics of the included trials
Table 2 Characteristics of the patients’ past medical histories among the included trials
Table 3 Angiographic and procedural characteristics
Figure 1 Flow chart depicting the selection of the studies included in this meta-analysis.
Major adverse cardiac events
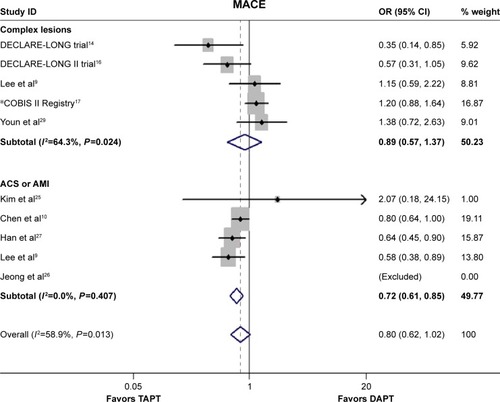
As shown in , the overall risk of MACE was not reduced significantly following TAPT (OR: 0.80; 95% CI: 0.62–1.02, P=0.077; I2=58.9%, P=0.013); a similar result was observed in the subgroup of complex lesions (OR: 0.89, 95% CI: 0.57–1.37, P=0.588; I2=64.3%, P=0.024), while the contrary result was shown in the ACS subgroup (OR: 0.72, 95% CI: 0.61–0.85, P<0.001; I2=0%, P=0.407). The results from the Egger’s test indicated no publication bias (P=0.918), and the stability of results was proved by the sensitivity analysis.
Figure 2 The ORs of MACE associated with TAPT compared with DAPT.
Abbreviations: ACS, acute coronary syndrome; AMI, acute myocardial infarction; CI, confidence interval; COBIS, COronary BIfurcation Stent; DAPT, dual antiplatelet treatment; DECLARE-LONG II, drug-eluting stenting followed by cilostazol treatment reduces late restenosis in patients with long coronary lesions; MACE, major adverse cardiac events; OR, odds ratio; TAPT, triple antiplatelet treatment.
All-cause mortality
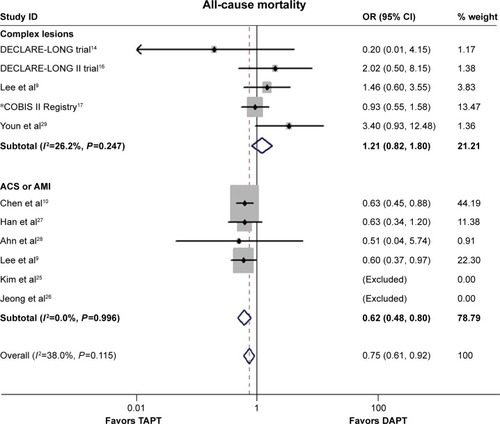
As depicted in , lower overall risk of all-cause mortality was observed related to TAPT (OR: 0.75, 95% CI: 0.61–0.92, P=0.006; I2=38%, P=0.115), which were mainly derived from the results of the ACS subgroup (OR: 0.62, 95% CI: 0.48–0.80, P<0.001; I2=0%, P=0.996). No publication bias was found by the Egger’s test (P=0.250). The sensitivity analysis demonstrated these superior effects of TAPT.
Figure 3 The ORs of all-cause mortality associated with TAPT compared with DAPT.
Abbreviations: ACS, acute coronary syndrome; AMI, acute myocardial infarction; CI, confidence interval; COBIS, COronary BIfurcation Stent; DAPT, dual antiplatelet treatment; DECLARE-LONG II, drug-eluting stenting followed by cilostazol treatment reduces late restenosis in patients with long coronary lesions; OR, odds ratio; TAPT, triple antiplatelet treatment.
Myocardial infarction
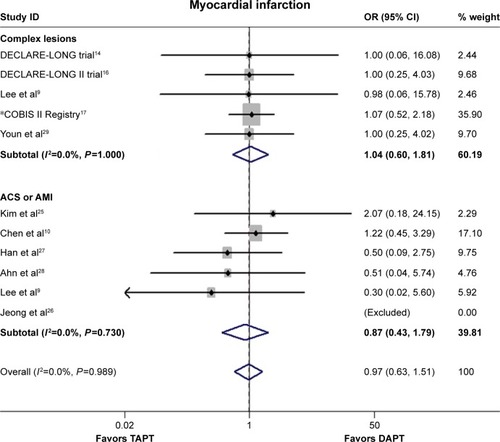
There was no difference between the TAPT group and the DAPT group with respect to the incidence of MI (OR: 0.97, 95% CI: 0.63–1.51, P=0.901; I2=0%, P=0.989, ), as well as the ACS (OR: 0.87, 95% CI: 0.43–1.79, P=0.710; I2=0%, P=0.730) and complex lesions subgroups (OR: 1.04, 95% CI: 0.60–1.81, P=0.894; I2=0%, P=1.000). No publication bias was encountered via the Egger’s test (P=0.219).
Figure 4 The ORs of myocardial infarction associated with TAPT compared with DAPT.
Abbreviations: ACS, acute coronary syndrome; AMI, acute myocardial infarction; CI, confidence interval; COBIS, COronary BIfurcation Stent; DAPT, dual antiplatelet treatment; DECLARE-LONG II, drug-eluting stenting followed by cilostazol treatment reduces late restenosis in patients with long coronary lesions; OR, odds ratio; TAPT, triple antiplatelet treatment.
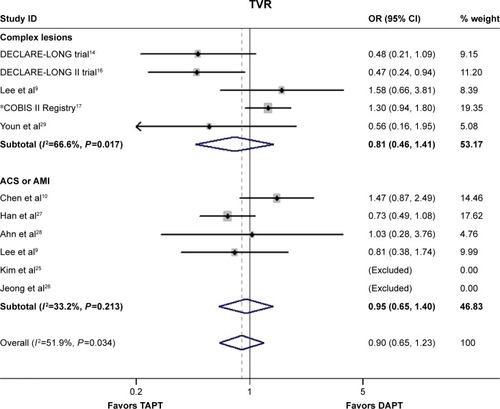
Target vessel revascularization
The incidence of TVR did not differ significantly between the two groups (OR: 0.90, 95% CI: 0.65–1.23, P=0.491; I2=51.9%, P=0.034, ), and similar results could also be obtained in both subgroups (complex lesions: OR: 0.81, 95% CI: 0.46–1.41, P=0.450; I2=66.6%, P=0.017; ACS: OR: 0.95, 95% CI: 0.65–1.40, P=0.802; I2=33.2%, P=0.213). Egger’s test indicated that there was no publication bias (P=0.348).
Figure 5 The ORs of TVR associated with TAPT compared with DAPT.
Abbreviations: ACS, acute coronary syndrome; AMI, acute myocardial infarction; CI, confidence interval; COBIS, COronary BIfurcation Stent; DAPT, dual antiplatelet treatment; DECLARE-LONG II, drug-eluting stenting followed by cilostazol treatment reduces late restenosis in patients with long coronary lesions; OR, odds ratio; TAPT, triple antiplatelet treatment; TVR, target vessel revascularization.
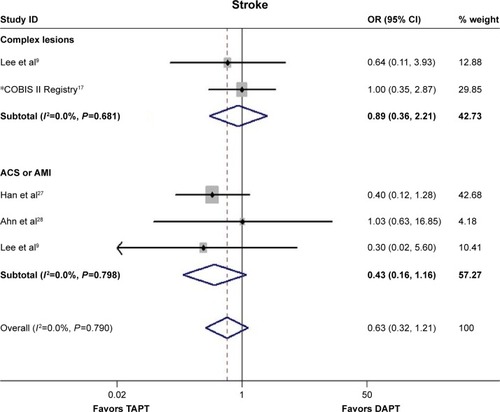
Stroke
TAPT was not associated with lower risk of stroke compared to DAPT (OR: 0.63, 95% CI: 0.32–1.21, P=0.163; I2=0%, P=0.790, ). In the ACS or the complex lesions subgroup, the incidence of stroke did not differ significantly between the triple treatment and the dual treatment groups (complex lesions: OR: 0.89, 95% CI: 0.36–2.21, P=0.807; I2=0%, P=0.681; ACS: OR: 0.43, 95% CI: 0.16–1.16, P=0.094; I2=0%, P=0.798). The results from the Egger’s test suggested no publication bias regarding the incidence of stroke (P=0.762).
Figure 6 The ORs of stroke associated with TAPT compared with DAPT.
Abbreviations: ACS, acute coronary syndrome; AMI, acute myocardial infarction; CI, confidence interval; COBIS, COronary BIfurcation Stent; DAPT, dual antiplatelet treatment; DECLARE-LONG II, drug-eluting stenting followed by cilostazol treatment reduces late restenosis in patients with long coronary lesions; OR, odds ratio; TAPT, triple antiplatelet treatment.
Safety end points
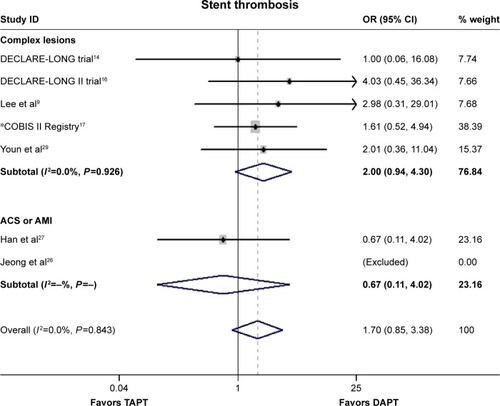
Definite/probable ST
The comparison between TAPT and DAPT showed no significant difference with respect to the risk of definite/probable ST (OR: 1.70, 95% CI: 0.85–3.38, P=0.133; I2=0%, P=0.843, ), while similar results were observed in the ACS subgroup (OR: 0.67, 95% CI: 0.11–4.02, P=0.661) and complex lesions subgroup (OR: 2.00, 95% CI: 0.94–4.30, P=0.074; I2=0%, P=0.926). No publication bias was observed based on the results of the Egger’s test (P=0.792).
Figure 7 The ORs of stent thrombosis associated with TAPT compared with DAPT.
Abbreviations: ACS, acute coronary syndrome; AMI, acute myocardial infarction; CI, confidence interval; COBIS, COronary BIfurcation Stent; DAPT, dual antiplatelet treatment; DECLARE-LONG II, drug-eluting stenting followed by cilostazol treatment reduces late restenosis in patients with long coronary lesions; OR, odds ratio; TAPT, triple antiplatelet treatment.
Bleeding
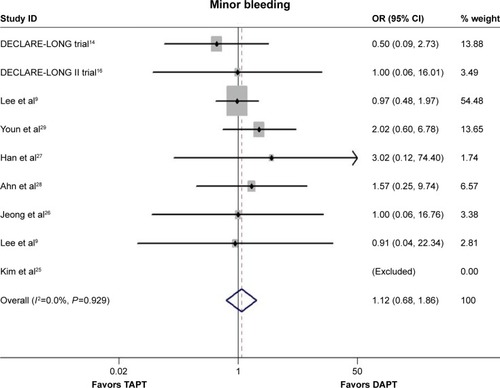
The incidence of major or minor bleeding was not increased with TAPT compared with DAPT (major bleeding: OR: 1.07, 95% CI: 0.60–1.90, P=0.809; I2=0%, P=0.637, ; minor bleeding: OR: 1.12, 95% CI: 0.68–1.86, P=0.649; I2=0%, P=0.929, ). No publication bias was observed (P=0.675 and P=0.727 for major and minor bleeding, respectively).
Figure 8 The ORs of major bleeding associated with TAPT compared with DAPT.
Abbreviations: CI, confidence interval; COBIS, COronary BIfurcation Stent; DAPT, dual antiplatelet treatment; DECLARE-LONG II, drug-eluting stenting followed by cilostazol treatment reduces late restenosis in patients with long coronary lesions; OR, odds ratio; TAPT, triple antiplatelet treatment.
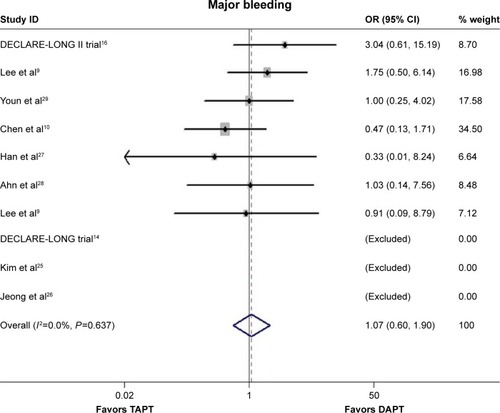
Figure 9 The ORs of minor bleeding associated with TAPT compared with DAPT.
Abbreviations: CI, confidence interval; COBIS, COronary BIfurcation Stent; DAPT, dual antiplatelet treatment; DECLARE-LONG II, drug-eluting stenting followed by cilostazol treatment reduces late restenosis in patients with long coronary lesions; OR, odds ratio; TAPT, triple antiplatelet treatment.
Discussion
In this meta-analysis, the major finding was that TAPT after stent implantation seemed to be associated with lower incidence of MACE, compared to DAPT, among ACS patients, which was thought mainly to result from the significant reduction in risk of all-cause mortality in this specific subset. The risk of bleeding, including major and minor bleeding, was not increased after TAPT, and the triple regimen did not reduce the incidence of MI, TVR, ST, and stroke.
The optimal antiplatelet regimen after intracoronary intervention among patients suffering from CAD has remained controversial. The routine dual regimen is used widely for these patients, particularly for patients with conditions complicated with diabetes mellitus (DM), complex coronary artery lesions, and ACS, in whom high risk of developing thrombotic events after stent implantation has been found. After treatment with the conventional dual antiplatelet regimen after stenting procedure, ~10% of patients still developed thrombotic events and subsequently faced higher incidence of adverse events.Citation4,Citation5 Instead, a triple regimen adding cilostazol to the routine DAPT for these patients was considered to obtain better outcomes. Recently, two large RCTs published by Lee et alCitation16 and Han et alCitation27 indicated ideal results of the triple regimen. In the Drug-Eluting Stenting Followed by Cilostazol Treatment Reduces Late Restenosis in Patients with Long Coronary Lesions (DECLARE-LONG II) trial,Citation16 499 patients undergoing long stent implantation (stent length: ≥30 mm) were enrolled, and decreased extent of late luminal loss, resulting in reduced risk of 12-month TLR, was observed. Moreover, Han et alCitation27 demonstrated that TAPT reduced long-term cardiac and cerebral events after PCI in patients suffering from ACS (TAPT vs DAPT: 10.3% vs 15.1%, P=0.011) by analyzing the data of 1,212 patients. Bundhun et alCitation13 recently performed a meta-analysis involving patients with complications of CAD and DM undergoing stent implantation; significant reduced risk of MACE was found in the triple group without any increase in risk of bleeding, the results being in line with the mentioned RCTs. However, several other clinical trials showed contrary results. The COBIS II RegistryCitation17 performed a subgroup analysis after propensity score matching, in which 1,302 patients with bifurcation lesions were divided into two groups at a 1:1 ratio and repeatedly analyzed. The final results showed that TAPT had no beneficial effect in terms of improving long-term clinical outcomes, similar to the results from another clinical trial.Citation18 In the retrospective cohort, a total of 245 patients (124 for TAPT, 121 for DAPT) presenting with unprotected LM disease were enrolled, and only limited or even no benefits of triple regimen were shown in terms of reducing risk of MACE, including death, MI, TVR, or stroke. The conflicting data from these clinical trials indicated that the superiority of TAPT compared to DAPT post-PCI still remains controversial and that there are only specific patient populations that might truly benefit from the regimen.
In this meta-analysis, lower incidence of MACE was observed in the subset of ACS, which might mainly be due to the significant reduced risk of all-cause mortality in this subgroup. To our knowledge, the acute phase of ACS was commonly complicated by the prothrombotic and inflammatory environment, which might aggravate myocardial injury and delay myocardial recovery, leading to worse clinical outcomes although early revascularization had been performed. Furthermore, these negative reactions might also be enhanced by the primary PCI if the procedure lasted a very long time or if multiple stents were implanted during the primary procedure. It should be noted that the routine dual regimen (aspirin plus a P2Y12 receptor antagonist) post-PCI could only have limited effects in terms of preventing these negative reactions if the patients had HTPR.Citation6 The new triple regimen of adding cilostazol to aspirin plus clopidogrel for antiplatelet therapy is considered to be helpful. Cilostazol is a selective inhibitor of phosphodiesterase III, which is known to hydrolyze cyclic adenosine monophosphate (cAMP), resulting in the accumulation of cAMP in vascular smooth muscle cells (VSMCs), which can suppress platelet aggregation, thus differing from aspirin or clopidogrel in the antiplatelet mechanism.Citation30 It might be more helpful in diminishing the prothrombotic and inflammatory response because cilostazol has additional effects in terms of suppressing platelet aggregation. The combination of the three agents might decrease HTPR and lead to intensified antiplatelet effect, which could reduce subsequent damage to myocardial cells and improve myocardial recovery, leading to better clinical outcomes.
Additionally, results from this meta-analysis showed that TAPT had no positive effects in terms of reducing the incidence of TVR, which are contrary to the results obtained by several other meta-analyses.Citation11,Citation12,Citation31 Lee et alCitation16 had reported that TAPT played a positive role in reducing the risk of TLR among 499 patients undergoing long stent implantation. In their opinion, the possible reasons might be that cilostazol-induced cAMP accumulation inhibits the activation of mitogen-activated protein kinase while upregulating the antioncogenes p53 and p21, leading to induced apoptosis in VSMCs and resulting in the antiproliferative effects on VSMCs.Citation32,Citation33 On the other hand, P-selectin-mediated platelet activation and subsequent Mac-1-mediated leukocyte activation are considered to be related with late lumen loss after coronary stenting, while cilostazol plays an important role in inhibiting their expression.Citation34 However, several other clinical trials showed that TAPT was not associated with lower risk of TVR and/or TLR compared to DAPT. Though Han et alCitation27 had indicated that TAPT reduced cardiac and cerebral events after 12-month follow-up for patients with ACS, the results of TVR between TAPT group and DAPT group did not show statistical significance (7.8% vs 10.4%, P=0.118). Three other clinical trialsCitation17,Citation18,Citation29 among patients presenting with bifurcation lesion, unprotected LM disease or mixed complex lesions, respectively, also provided similar results. It should be noted that underexpansion and malapposition of implanted stents is potentially considered to be related to the development of thrombotic events, which might mainly contribute to most of the adverse events. Among these CAD patients undergoing stent implantation, there are still several difficulties in achieving optimal stent deployment, particularly in those with complex coronary artery lesions or those suffering from ACS. Of note, long or multiple stents implanted during the procedure at one time among these high-risk patients might make it much more difficult to achieve optimal stent deployment. Moreover, the implanted stents with different structures and drug coatings could affect the process of endothelialization, which is thought to be highly responsible for restenosis in stents. Moreover, the PCI procedure with long or multiple stents for these high-risk patients might cause large stress, which could easily induce severe inflammatory response, just as described earlier, affecting the proliferation of VSMCs and leading these patients out of the effects of adding cilostazol to the routine dual regimen. In fact, the follow-up triple regimens, including duration and dosage of the cilostazol added to the routine dual regimen, might also play an important role in the final results. In addition, risk factors, such as more number of current smokers, high incidence of DM, or poor compliance with antiplatelet treatment, occurring in different subsets might also be the possible confounding sources affecting the final results. As a result, these reasons might explain why the triple regimen did not reduce the risk of MACE, including MI, all-cause mortality or stroke, in the subgroup “complex lesions”.
Several problems remain unsolved in this study. First, it was a dilemma to specify the optimal duration and dosage of cilostazol to be added to the routine dual regimen due to the lack of enough available data. Second, the selection of different types of implanted stents, which play an important role with respect to benefits of TAPT, remained uncertain. As a result, more powerful RCTs focusing on the related topics might be warranted to guide clinical decision making.
Limitations
This study had several limitations. First, this meta-analysis was performed with no individual patient data, and the small sample sizes of the several included RCTs also made the evaluation of efficacy for TAPT easily be influenced. Second, details related to the PCI procedure, such as the time of procedure, types of stents, techniques, and the choices of sheath with different sizes, might be the unavoidable potential confounding factors that influence the medicine’s effects on patients with complex coronary artery lesions. Third, the insufficient analyses of these data from quantitative coronary analysis among each included trial limited us from studying the specific benefits on angiographic results. Fourth, the absence of data with respect to new-generation ADP receptor antagonists, such as prasugrel and ticagrelor, did not allow us to evaluate their safety and efficacy for these included patients. Additionally, adverse reactions to drug reduced tolerance-inducing discontinuation of cilostazol, which might also influence the final results. Last but not the least, there were no strict durations and dosages of TAPT and DAPT for these included patients, and no limited follow-up period for these included trials might also sway the final results.
Conclusion
TAPT post-PCI was seemed to be related with lower risk of MACE, especially in reducing the incidence of all-cause mortality among patients suffering from ACS, without any increased risk of bleeding. However, more powerful randomized clinical trials comparing TAPT to DAPT after PCI procedure in such patients with more precise subgroups are still warranted to guide clinical application of this triple antiplatelet regimen.
Authors contributions
FZG and DGB were involved in the design, literature search, assessment of study quality and drafting of the manuscript. Disagreements were resolved by LXB. FZG and DGB performed statistical analysis and critically revised the manuscript. GXF and GYL constructed the maps. TNL critically revised the original study design and the manuscript. All authors contributed toward data analysis, drafting and critically revising the paper and agree to be accountable for all aspects of the work.
Acknowledgments
The study was supported by the Jiangsu Provincial Special Program of Medical Science (BL2013001).
Disclosure
The authors report no conflicts of interest in this work.
References
- O’GaraPTKushnerFGAscheimDD2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice GuidelinesCirculation20131274e362e42523247304
- GroveELWurtzMThomasMRKristensenSDAntiplatelet therapy in acute coronary syndromesExpert Opin Pharmacother201516142133214726293612
- CowleyMJKuritzkyLDevelopments in antiplatelet therapy for acute coronary syndromes and considerations for long-term managementCurr Med Res Opin20092561477149019419337
- IakovouISchmidtTBonizzoniEIncidence, predictors, and outcome of thrombosis after successful implantation of drug-eluting stentsJAMA2005293172126213015870416
- DaemenJWenaweserPTsuchidaKEarly and late coronary stent thrombosis of sirolimus-eluting and paclitaxel-eluting stents in routine clinical practice: data from a large two-institutional cohort studyLancet2007369956266767817321312
- ParodiGMarcucciRValentiRHigh residual platelet reactivity after clopidogrel loading and long-term cardiovascular events among patients with acute coronary syndromes undergoing PCIJAMA2011306111215122321934054
- ConeJWangSTandonNComparison of the effects of cilostazol and milrinone on intracellular cAMP levels and cellular function in platelets and cardiac cellsJ Cardiovasc Pharmacol199934449750410511123
- GotoSCilostazol: potential mechanism of action for antithrombotic effects accompanied by a low rate of bleedingAtheroscler Suppl200564311
- LeeKHAhnYKimSSKAMIR (Korea Acute Myocardial Infarction Registry) InvestigatorsComparison of triple anti-platelet therapy and dual anti-platelet therapy in patients with acute myocardial infarction who had no-reflow phenomenon during percutaneous coronary interventionCirc J201377122973298123986083
- ChenKYRhaSWLiYJKorea Acute Myocardial Infarction Registry InvestigatorsTriple versus dual antiplatelet therapy in patients with acute ST-segment elevation myocardial infarction undergoing primary percutaneous coronary interventionCirculation2009119253207321419528339
- ChenYZhangYTangYHuangXXieYLong-term clinical efficacy and safety of adding cilostazol to dual antiplatelet therapy for patients undergoing PCI: a meta-analysis of randomized trials with adjusted indirect comparisonsCurr Med Res Opin2014301374924083626
- SakuraiRKooBKKanedaHBonneauHNNagaiRCilostazol added to aspirin and clopidogrel reduces revascularization without increases in major adverse events in patients with drug-eluting stents: a meta-analysis of randomized controlled trialsInt J Cardiol201316752250225822727963
- BundhunPKQinTChenMHComparing the effectiveness and safety between triple antiplatelet therapy and dual antiplatelet therapy in type 2 diabetes mellitus patients after coronary stents implantation: a systematic review and meta-analysis of randomized controlled trialsBMC Cardiovasc Disord20151511826450578
- LeeSWParkSWKimYHDrug-eluting stenting followed by cilostazol treatment reduces late restenosis in patients with diabetes mellitus the DECLARE-DIABETES trial (a randomized comparison of triple antiplatelet therapy with dual antiplatelet therapy after drug-eluting stent implantation in diabetic patients)J Am Coll Cardiol200851121181118718355656
- HaSJKimSJHwangSJEffect of cilostazol addition or clopidogrel doubling on platelet function profiles in diabetic patients undergoing a percutaneous coronary interventionCoron Artery Dis201324869069724152567
- LeeSWParkSWKimYHDECLARE-LONG II Study InvestigatorsA randomized, double-blind, multicenter comparison study of triple antiplatelet therapy with dual antiplatelet therapy to reduce restenosis after drug-eluting stent implantation in long coronary lesions: results from the DECLARE-LONG II (drug-eluting stenting followed by cilostazol treatment reduces late restenosis in patients with long coronary lesions) trialJ Am Coll Cardiol201157111264127021392640
- SongPSSongYBYangJHTriple versus dual antiplatelet therapy after percutaneous coronary intervention for coronary bifurcation lesions: results from the COBIS (COronary BIfurcation Stent) II RegistryHeart Vessels201530445846824682436
- LeeHJYuCWHwangHKLong-term effectiveness and safety of triple versus dual antiplatelet therapy after percutaneous coronary intervention for unprotected left main coronary artery diseaseCoron Artery Dis201324754254823994880
- Biondi-ZoccaiGGAbbateAAgostoniPLong-term benefits of an early invasive management in acute coronary syndromes depend on intracoronary stenting and aggressive antiplatelet treatment: a metaregressionAm Heart J2005149350451115864240
- JadadARMooreRACarrollDAssessing the quality of reports of randomized clinical trials: is blinding necessary?Control Clin Trials19961711128721797
- LaskeyWKYancyCWMaiselWHThrombosis in coronary drug-eluting stents: report from the meeting of the Circulatory System Medical Devices Advisory Panel of the Food and Drug Administration Center for Devices and Radiologic Health, December 7–8, 2006Circulation2007115172352235717470710
- LiberatiAAltmanDGTetzlaffJThe PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaborationBMJ2009339b270019622552
- EggerMDavey SmithGSchneiderMMinderCBias in meta-analysis detected by a simple, graphical testBMJ199731571096296349310563
- LeeSWParkSWKimYHComparison of triple versus dual antiplatelet therapy after drug-eluting stent implantation (from the DECLARE-Long trial)Am J Cardiol200710071103110817884371
- KimJYLeeKShinMCilostazol could ameliorate platelet responsiveness to clopidogrel in patients undergoing primary percutaneous coronary interventionCirc J200771121867187218037738
- JeongYHHwangJYKimISAdding cilostazol to dual antiplatelet therapy achieves greater platelet inhibition than high maintenance dose clopidogrel in patients with acute myocardial infarction: results of the adjunctive cilostazol versus high maintenance dose clopidogrel in patients with AMI (ACCEL-AMI) studyCirc Cardiovasc Interv201031172620118150
- HanYLiYWangSCilostazol in addition to aspirin and clopidogrel improves long-term outcomes after percutaneous coronary intervention in patients with acute coronary syndromes: a randomized, controlled studyAm Heart J2009157473373919332203
- AhnCMHongSJParkJHKimJSLimDSCilostazol reduces the progression of carotid intima-media thickness without increasing the risk of bleeding in patients with acute coronary syndrome during a 2-year follow-upHeart Vessels201126550251021153029
- YounYJLeeJWAhnSGMulticenter randomized trial of 3-month cilostazol use in addition to dual antiplatelet therapy after biolimus-eluting stent implantation for long or multivessel coronary artery diseaseAm Heart J20141672241.e1248.e124439986
- SaviPZachayusJLDelesque-TouchardNThe active metabolite of Clopidogrel disrupts P2Y12 receptor oligomers and partitions them out of lipid raftsProc Natl Acad Sci U S A200610329110691107416835302
- ChenJMengHXuLEfficacy and safety of cilostazol based triple antiplatelet treatment versus dual antiplatelet treatment in patients undergoing coronary stent implantation: an updated meta-analysis of the randomized controlled trialsJ Thromb Thrombolysis2015391233424869717
- ItoCKusanoEFurukawaYModulation of the erythropoietin-induced proliferative pathway by cAMP in vascular smooth muscle cellsAm J Physiol Cell Physiol20022836C1715C172112419709
- HayashiSMorishitaRMatsushitaHCyclic AMP inhibited proliferation of human aortic vascular smooth muscle cells, accompanied by induction of p53 and p21Hypertension2000351 pt 223724310642304
- InoueTUchidaTSakumaMCilostazol inhibits leukocyte integrin Mac-1, leading to a potential reduction in restenosis after coronary stent implantationJ Am Coll Cardiol20044471408141415464320