
Abstract
Background
Delayed encephalopathy after acute carbon monoxide (CO) poisoning (DEACMP) commonly occurs after recovering from acute CO poisoning. This study was performed to assess the efficacy of the combined application of dexamethasone and hyperbaric oxygen (HBO) therapy in patients with DEACMP.
Patients and methods
A total of 120 patients with DEACMP were recruited and randomly assigned into the experimental group (receiving dexamethasone 5 mg/day or 10 mg/day plus HBO therapy) and control group (HBO therapy as monotherapy). Meanwhile, the conventional treatments were provided for all the patients. We used the Mini-Mental State Examination (MMSE) scale to assess the cognitive function, the National Institutes of Health Stroke Scale (NIHSS) to assess the neurological function and the remission rate (RR) to assess the clinical efficacy. Myelin basic protein (MBP) in the cerebrospinal fluid (CSF) was also measured.
Results
After 4 weeks of treatment, compared to the control group, the experimental group had a significantly higher remission rate (P=0.032), a significantly higher average MMSE score (P=0.037) and a significantly lower average NIHSS score (P=0.002). Meanwhile, there was a trend toward better improvement with dexamethasone 10 mg/day, and the level of MBP in the CSF of patients was significantly lower in the experimental group than in the control group (P<0.0001). The addition of dexamethasone did not significantly increase the incidence of adverse events.
Conclusion
These results indicate that the combined application of dexamethasone and HBO therapy could yield better efficacy for patients with DEACMP and should be viewed as a potential new therapy.
Introduction
As a colorless, odorless and tasteless gas, carbon monoxide (CO) is very difficult to detect when escaping. A CO concentration of more than 35 ppm will be harmful to human health.Citation1 In modern society, CO poisoning is highly common and results in substantial mortality and morbidity.Citation2 Moreover, ~13%–50% of severely CO-poisoned patients who experience coma would suffer from memory impairment, cognitive dysfunction, and behavioral disorders after 2–60 days of incubation. This complication in clinical practice is viewed as delayed encephalopathy after acute CO poisoning (DEACMP).Citation3,Citation4 DEACMP is a disease with poor prognosis and could cause huge economic burden for individuals, families and society.Citation5
Currently, the pathogenesis of DEACMP is still unclear.Citation6 Some researchers believed that it was caused by oxygen deficit.Citation7 Other previous studies indicated that DEACMP was associated with the inflammatory reaction in blood vessels, and immune damage.Citation8,Citation9 Chen et alCitation10 reported that the excitatory amino acid might play an important role in the occurrence of DEACMP. Partly due to the unclear pathogenesis, there is still no “gold” standard for the treatment of this disease. Annane et alCitation11 found that hyperbaric oxygen (HBO) therapy was effective in the treatment of patients with acute CO poisoning. HBO therapy could increase the blood oxygen in brain tissues, promote the decomposition of carboxyhemoglobin and remove CO in blood, which could be beneficial for the damaged brain cells to recover. Meanwhile, many researchers also reported that the combined application of HBO therapy and other medications could have a good efficacy for DEACMP treatment, especially in the acute phase.Citation12,Citation13 Our previous study found that N-butylphthalide and HBO therapy could significantly improve the cognitive dysfunction of patients with DEACMP.Citation1
Meanwhile, in an animal experiment, our group also found that dexamethasone could decrease the incidence of DEACMP.Citation14 This might be related to the antioxidation and cell protection function of dexamethasone.Citation15 However, to date, there are few studies investigating the efficacy of dexamethasone in treating patients with DEACMP. Therefore, we conducted this study to assess whether the addition of dexamethasone to HBO therapy could significantly improve the efficacy of HBO therapy as monotherapy. Additionally, a previous study reported that the level of myelin basic protein (MBP) in the cerebrospinal fluid (CSF) of patients with DEACMP was elevated, and moreover it could be a predictive marker of DEACMP.Citation16 Our previous study also found an elevated level of MBP in the CO-poisoned rats.Citation17 Therefore, we also studied the level of MBP in the CSF of patients with DEACMP.
Patients and methods
Recruited patients
The Institutional Review Board of Baotou Central Hospital reviewed and approved the purpose and design of our work. This clinical trial was performed between July 2014 and August 2016. Patients meeting the following criteria were included: 1) patients who met the criteria of DEACMP; 2) patients with Mini-Mental State Examination (MMSE) score of not more than 24;Citation18 and 3) patients who provided written informed consent. Meanwhile, the following exclusion criteria were used: 1) patients who were allergic to dexamethasone; 2) patients with intellectual impairment; and 3) patients who were pregnant. In total, 120 patients with DEACMP were included.
Experimental methods
The included patients were randomly assigned into two groups in a 1:1 ratio: the experimental and control groups. We used the random number table to conduct randomization, and the raters and patients were blinded to allocation. The conventional treatments, including using antibiotics, sputum suction, reducing or avoiding respiratory tract infection, maintaining unobstructed airway, maintaining stable blood pressure and blood glucose, regulating water electrolytes, and preventing urinary tract infection, were followed in all patients. At the same time, patients in the two groups were placed in the oxygen chamber with 0.25 MPa absolute pressure for 80 min/day.Citation1 The patients in the experimental group were further randomly assigned into two groups in a 1:1 ratio. Half of the patients received dexamethasone 10 mg/day and the other half received dexamethasone 5 mg/day. The doses of dexamethasone mainly referred to the previous study that used dexamethasone to treat CO-poisoned patients.Citation19 The treatment was provided 5 days/week for 4 weeks.
Outcome assessment
Then, the MMSE score was used to assess the cognitive function and the National Institutes of Health Stroke Scale (NIHSS) was used to assess the neurological function. According to the MMSE score, complete recovery (CR), partial recovery (PR) and no relief (NR) were defined.Citation1 The remission rate (RR) was defined by the percentage of CR. Meanwhile, we collected the CSF of patients before and after the treatment to study the effect of dexamethasone on the level of MBP. The CSF was collected by lumbar puncture, and the MBP level was measured by enzyme-linked immunosorbent assay (ELISA) technique. The potential adverse events were also recorded and analyzed to assess the acceptability of the combined application of dexamethasone and HBO therapy.
Statistical analysis
We used mean ± standard deviation (SD) to show the continuous data in this study. Student’s t-test and chi-squared test were conducted to assess whether the baseline characteristics were matched. We performed the analysis of covariance (ANCOVA) to assess the effect of the treatment modalities on the posttreatment MMSE and NIHSS scores.Citation1 Also, this method was applied to assess the effect of dexamethasone on the level of MBP. In this study, the intention-to-treat (ITT) analysis was conducted, and a P-value of <0.05 was set to be significant.
Results
Baseline data
The included 120 patients with DEACMP were randomly assigned into two groups. Each group had 60 patients. In the experimental group, 30 patients received dexamethasone 10 mg/day and the remaining 30 patients received dexamethasone 5 mg/day. The average CO exposure time in the experimental and control groups was 5.41 hours and 5.22 hours, respectively. In addition, no significant differences in other baseline data, such as age, body mass index (BMI) and carboxyhemoglobin level, were found between the experimental and control groups. The detailed information of the two groups is given in . Meanwhile, there was no significant difference in the baseline characteristics between patients receiving 5 mg/day and patients receiving 10 mg/day.
Table 1 Demographic characteristics of the included patients
MMSE score
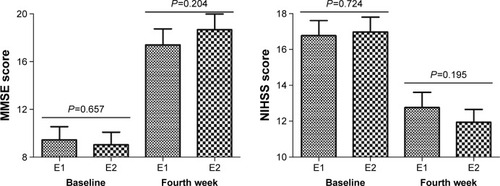
The MMSE scale was assessed at two time points (). Before the treatment, the average MMSE scores between the two groups were similar (P=0.878). After the treatment, the average MMSE scores were significantly increased in the experimental (P<0.0001) and control groups (P<0.0001). However, the results of ANCOVA test showed that the two treatment modalities had a significantly different effect on MMSE scores. At the end of the trial, the experimental group had a significantly higher average MMSE score than that of the control group (P=0.037). Furthermore, compared to patients receiving dexamethasone 5 mg/day, patients receiving dexamethasone 10 mg/day had a nonsignificantly higher average MMSE score (P=0.204; ).
Figure 1 MMSE and NIHSS scores in the experimental and control groups.
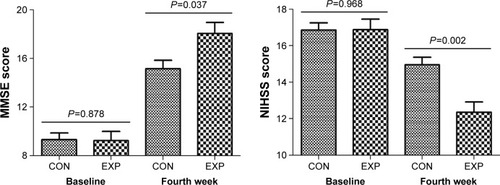
Figure 2 MMSE and NIHSS scores in the dexamethasone 5 mg/day and 10 mg/day groups.
Abbreviations: MMSE, Mini-Mental State Examination; NIHSS, National Institutes of Health Stroke Scale.
Remission rate
As shown in , the MMSE scores of patients in the two groups were not more than 24 before the treatment. But after the treatment, the MMSE scores of 14 patients and 25 patients in the control and experimental groups, respectively, were more than 24. These patients met the CR criteria. Compared to the control group, the experimental group had a significantly higher RR (23.3% vs 41.6%, P=0.032). Furthermore, compared to patients receiving dexamethasone 5 mg/day, patients receiving dexamethasone 10 mg/day had a nonsignificantly higher RR (P=0.432, 36.6% vs 46.6%).
Table 2 RR in the two groups at baseline and end of the fourth week based on MMSE scores
NIHSS score
The NIHSS was assessed at two time points (). Before the treatment, the average NIHSS scores between the two groups were similar (P=0.968). After the treatment, the average NIHSS scores were significantly decreased in the experimental (P<0.0001) and control groups (P=0.014). However, the results of ANCOVA test showed that the two treatment modalities had a significantly different effect on NIHSS scores. At the end of the trial, the experimental group had a significantly lower average NIHSS score than the control group (P=0.002). Furthermore, compared to patients receiving dexamethasone 5 mg/day, patients receiving dexamethasone 10 mg/day had a nonsignificantly lower average NIHSS score (P=0.195; ).
MBP level
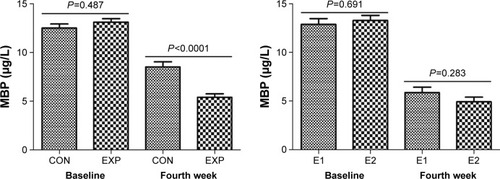
The level of MBP in the CSF was measured at two time points (). Before the treatment, the level of MBP was not significantly different between the two groups (P=0.487). After the treatment, the levels of MBP in the control group (P=0.006) and experimental group (P<0.0001) were significantly decreased. But the results of ANCOVA test showed that compared to the control group, the experimental group had significantly lower level of MBP (P<0.0001). Furthermore, compared to patients receiving dexamethasone 5 mg/day, patients receiving dexamethasone 10 mg/day had a nonsignificantly lower level of MBP (P=0.283; ).
Figure 3 The level of MBP in CSF of patients with DEACMP.
Abbreviations: CO, carbon monoxide; CON, control; CSF, cerebrospinal fluid; DEACMP, delayed encephalopathy after acute CO poisoning; EXP, experimental; MBP, myelin basic protein.
Adverse events
During the whole treatment, no serious adverse events were observed in the two groups, partly because of the short time of taking dexamethasone. No significantly changed blood glucose and blood lipid levels were observed. In the experimental group, two patients had mild nausea, one patient experienced mild vomiting, two patients had loss of appetite, three patients reported mild headache and one patient had mild dizziness. In the control group, one patient had mild nausea, four patients reported mild headache and two patients had loss of appetite. Patients with these adverse events could recover by themselves and did not require special treatment.
Discussion
In this study, we found that the HBO therapy as monotherapy could significantly increase the MMSE scores and decrease the NIHSS scores of patients with DEACMP after the acute-phase treatment, which was consistent with the results in our previous study.Citation1 Meanwhile, we found that the addition of dexamethasone could significantly improve the efficacy of HBO therapy. In this study, compared to the control group, the experimental group had significantly higher MMSE scores, higher RR and lower NIHSS scores. Additionally, the addition of dexamethasone did not significantly increase the incidence of adverse events. Therefore, these results demonstrate that the combined application of dexamethasone and HBO therapy could be a potential effective treatment method for patients with DEACMP in the acute-phase treatment. Moreover, we found that there was a trend toward better improvement with dexamethasone 10 mg/day. Because of the limited number of included patients, future studies are needed to verify and support these results.
One point should be noted that the statistical significance is not always equivalent to the clinical significance. Osoba et alCitation20 reported that it was very important to determine the clinically meaningful differences, because, in some conditions, the small numerical differences in average scores might result in statistically significant results when the large subjects were used. In this study, we used Cohen’s d to assess whether these differences in MMSE scores, NIHSS scores and the level of MBP in the CSF were really clinically meaningful.Citation21 The value of Cohen’s d more than 0.5 indicated that the effect size was moderate and significant.Citation21 In this study, the Cohen’s d value was 0.59 on MMSE scores, 0.57 on NIHSS scores and 0.87 on the level of MBP. These results indicated that the combined application of dexamethasone and HBO therapy could yield better clinical efficacy and should be viewed as a potential new therapy for patients with DEACMP.
Atalay et alCitation22 reported that dexamethasone might have effects on brain tissue lipid peroxidation during the treatment of CO-poisoned rats. Another animal study indicated that the early dexamethasone treatment might have a positive effect on preventing DEACMP after 18 days of treatment.Citation23 Our previous study found that dexamethasone 30 mg/kg per day could significantly reduce the mortality of CO-poisoned rats.Citation24 Currently, the pharmacological mechanism of dexamethasone is not known. Our previous study found that dexamethasone could attenuate inflammation by protecting myelin sheath from the damage of inflammation response.Citation14 As for HBO therapy, it could be beneficial for the damaged brain cells to recover via increasing the blood oxygen in brain tissues. These results indicated that the combined application of HBO therapy and dexamethasone could be effective in treating patients with DEACMP.
Kim et alCitation25 reported that the main pathological lesion of DEACMP was the diffuse white matter demyelination. Another study found that the chemically modified MBP was related to the delayed CO-mediated neuropathology.Citation26 Tzakos et alCitation27 reported that MBP played an important role in maintaining the stability of structure and function of myelin sheath in the central nervous system. In this study, we found that the level of MBP was significantly decreased in both groups, but the level was significantly lower in patients receiving dexamethasone. In addition, the high dose of dexamethasone produced more reduction in MBP level. These results might indicate that the HBO therapy and dexamethasone directly or indirectly acted on MBP within the brain to cause the efficacy. Meanwhile, our results indicated that MBP could be a potential predictive marker for DEACMP and an index to estimate whether the treatment modalities were effective for DEACMP. However, future studies are needed to find out whether MBP could be targeted as a pharmacological strategy to prevent delayed encephalopathy.
There were some limitations in our study: 1) the number of patients with DEACMP in each group was relatively small, and we did not conduct the sample size calculation; 2) in this study, we only assessed the efficacy of dexamethasone and HBO therapy in the acute-phase treatment of DEACMP; hence, future studies are needed to assess its long-term efficacy; 3) it would have been better to randomize the recruited patients into three groups (control, E1 and E2) from the start rather than randomize into two groups (control and experimental) and then splitting off the experimental; 4) all the patients in our study were from the same city, which might limit the applicability of our findings.Citation28 Finally, a significant difference in efficacy between the high- and low-dose dexamethasone was not found in this study; future studies are needed to determine the optimal dose.
Conclusion
Our study found that the combined application of dexamethasone and HBO therapy could yield better efficacy for patients with DEACMP than HBO therapy as monotherapy. Compared to dexamethasone 5 mg/day, the efficacy of dexamethasone 10 mg/day had a tendency to be better. Meanwhile, the level of MBP in the CSF was significantly decreased in both groups after the treatment. Because this study was limited by the small sample size, future studies are needed to verify and support our findings.
Acknowledgments
Sincere gratitude is extended to the nurses in our department and participants for their efforts and cooperation.
Disclosure
The authors report no conflicts of interest in this work.
References
- WangBXiangWXueHEfficacy of N-Butylphthalide and hyperbaric oxygen therapy on cognitive dysfunction in patients with delayed encephalopathy after acute carbon monoxide poisoningMed Sci Monit Epub2016
- HampsonNBPiantadosiCAThomSRWeaverLKPractice recommendations in the diagnosis, management, and prevention of carbon monoxide poisoningAm J Respir Crit Care Med201218611 1095 110123087025
- GoldsteinMCarbon monoxide poisoningJ Emerg Nurs2008346 538 54219022078
- HsiaoCLKuoHCHuangCCDelayed encephalopathy after carbon monoxide intoxication-long-term prognosis and correlation of clinical manifestations and neuroimagesActa Neurol Taiwan200413 64 7015478677
- HuHPanXWanYZhangQLiangWFactors affecting the prognosis of patients with delayed encephalopathy after acute carbon monoxide poisoningAm J Emerg Med2011293 261 26420825794
- HaraSMukaiTKurosakiKMizukamiHKuriiwaFEndoTRole of nitric oxide system in hydroxyl radical generation in rat striatum due to carbon monoxide poisoning, as determined by microdialysisToxicology20072391 136 14317703866
- GormanDLinHYWilliamsCEarly evidence of a regulated response to hypoxaemia in sheep that preserves the brain cortexNeurosci Lett20063943 174 17816300896
- WangWLiJChangYEffects of immune reaction in rats after acute carbon monoxide poisoningUndersea Hyperb Med2011384 23921877552
- ThomSRBhopaleVMHanSTClarkJMHardyKRIntravascular neutrophil activation due to carbon monoxide poisoningAm J Respir Crit Care Med200617411 1239 124816931637
- ChenMLuTJChenXJDifferential roles of NMDA receptor subtypes in ischemic neuronal cell death and ischemic toleranceStroke20083911 3042 304818688011
- AnnaneDChaddaKGajdosPJars-GuincestreMCChevretSRaphaelJCHyperbaric oxygen therapy for acute domestic carbon monoxide poisoning: two randomized controlled trialsIntensive Care Med2011377 486 49221125215
- LoCPChenSYChouMCDiffusion – tensor MR imaging for evaluation of the efficacy of hyperbaric oxygen therapy in patients with delayed neuropsychiatric syndrome caused by carbon monoxide inhalationEur J Neurol2007147 777 78217594334
- ProckopLDChichkovaRICarbon monoxide intoxication: an updated reviewJ Neurol Sci20072621 122 13017720201
- XiangWPXueHWangBJDelayed encephalopathy of acute carbon monoxide intoxication in rats: potential mechanism and intervention of dexamethasonePak J Pharm Sci2014276 suppl 2025 202825410067
- RocksénDLilliehöökBLarssonRJohanssonTBuchtADifferential anti-inflammatory and anti-oxidative effects of dexamethasone and N-acetylcysteine in endotoxin-induced lung inflammationClin Exp Immunol20001222 249 25611091282
- IdeTKamijoYMyelin basic protein in cerebrospinal fluid: a predictive marker of delayed encephalopathy from carbon monoxide poisoningAm J Emerg Med2008268 908 91218926351
- XiangWPZhangFXueHMechanism of delayed encephalopathy in acute carbon monoxide poisoning rats and mouse nerve growth factor in early interventionChin Pharm J20134824 2123 2127
- ShuAHWangQChenXBEffect of different depths of anesthesia on postoperative cognitive function in laparoscopic patients: a randomized clinical trialCurr Med Res Opin201531 1883 188726202165
- MaXYClinical study of large dose of dexamethasone combined with hyperbaric oxygen in treatment of acute carbon monoxide poisoningMed Innov China20131023 045 047
- OsobaDRodriguesGMylesJZeeBPaterJInterpreting the significance of changes in health-related quality-of-life scoresJ Clin Oncol1998161 139 1449440735
- SawilowskySNew effect size rules of thumbJ Mod Appl Stat Methods200982 467 474
- AtalayHAybekHKoseogluMThe effects of amifostine and dexamethasone on brain tissue lipid peroxidation during oxygen treatment of carbon monoxide-poisoned ratsAdv Ther2006232 332 34116751165
- LiQSongJJZhangHYFuKLanHBDengYDexamethasone therapy for preventing delayed encephalopathy after carbon monoxide poisoningBiotech Histochem2015908 561 56726052629
- XiangWPLiQYXueHThe predictive value of myelin basic protein in rats with the final outcome of carbon monoxide poisoning and the dexamethasone intervention functionJ Brain Nerv Dis2014225 344 346
- KimJHChangKHSongICDelayed encephalopathy of acute carbon monoxide intoxication: diffusivity of cerebral white matter lesionsAJNR Am J Neuroradiol2003248 1592 159713679276
- ThomSRBhopaleVMFisherDZhangJGimottyPDelayed neuropathology after carbon monoxide poisoning is immune-mediatedProc Natl Acad Sci U S A200410137 13660 1366515342916
- TzakosAGTroganisATheodorouVStructure and function of the myelin proteins: current status and perspectives in relation to multiple sclerosisCurr Med Chem20051213 1569 158715974988
- ChenJZhouCLiuZDivergent urinary metabolic phenotypes between major depressive disorder and bipolar disorder identified by a combined GC–MS and NMR spectroscopic metabonomic approachJ Proteome Res2015148 3382 338926168936