
Abstract
Rheumatoid arthritis (RA) is a chronic autoimmune disease that can lead to severe joint damage, disability and mortality. Quercetin (QUE) is a natural flavonoid that is ubiquitous in fruits and vegetables. This article reviews the effect of QUE on articular and extra-articular manifestations of RA in vitro and in vivo. In general, for articular manifestations, QUE inhibited synovial membrane inflammation by reducing inflammatory cytokines and mediators, decreasing oxidative stress, inhibiting proliferation, migration and invasion, and promoting apoptosis of fibroblast-like synoviocytes (FLS), regulated autoimmune response through modulating Th17/Treg imbalance and Th17 cells differentiation, reducing autoantibodies levels and regulating ectonucleoside triphosphate diphosphohydrolase (E-NTPDase)/ectoadenosine deaminase (E-ADA) activities, reduced bony damage via lowering matrix metalloproteinase (MMP)-1, MMP-3, receptor activator of nuclear factor kappa B ligand (RANKL) expression and osteoclasts formation. For extra-articular manifestations, QUE could reverse the neurodegenerative processes of the enteric nervous system (ENS) and exhibited cytoprotective, genoprotective and hepatoprotective effects. In addition, we also summarize some contradictory experimental results and explore the possibility for these differences to form a sound basis for the clinical application of QUE for RA.
Introduction
Rheumatoid arthritis (RA), a systemic inflammatory autoimmune disease, is more common in women than men with a worldwide prevalence of 0.5%–1.0%.Citation1 RA is featured with progressive cartilage and bone destruction by invasive hyperplastic synovial membrane, leading to an increased risk of disability and mortality.Citation2 Though current therapeutic options have, to some extent, improved the prognosis of RA, the pharmacological treatment seems to be continuously inadequate in preventing the progression of RA; therefore, new anti-arthritic therapies are essential.Citation3,Citation4 Currently, there is growing interest in the pharmacological potential of natural products.
Quercetin (QUE) is a type of flavonoid, which is ubiquitous in fruits and vegetables, such as onion, apples, beans and various berries.Citation5 A growing body of evidence has shown the anti-hypertensive,Citation6 anti-inflammatory,Citation7 anti-angiogenic,Citation8 anticancer,Citation9–Citation11 hepatoprotective,Citation12 anti-diabetic,Citation13 anti-aging,Citation14 and neuroprotectiveCitation15 potential of QUE. In addition, QUE is also proved to be effective in management of RA in pre-clinical or clinical studies. In this review, we discuss the effect of QUE on articular and extra-articular manifestations in RA.
Pharmacological Mechanism of QUE in Pre-Clinical Studies ()
The zymosan-induced arthritis, collagen-induced arthritis (CIA) and adjuvant-induced arthritis (AA) models are commonly used animal models of RA, which is helpful for understanding the complex pathogenic mechanisms involving inflammation, autoimmunity, and cartilage and bone destruction in RA.Citation16,Citation17
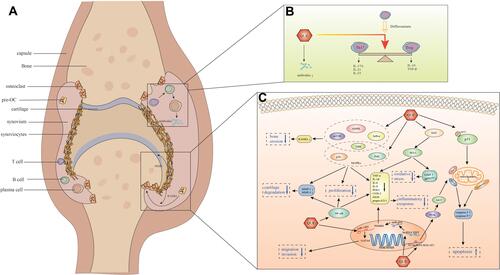
Figure 1 The anti-articular effect of QUE on RA in pre-clinical studies. (A): Rheumatoid arthritis joint. (B): The immune-regulatory effect of QUE on RA: QUE regulated Th17/Treg cell balance, decreased Th17 cells-related cytokines (IL-17A, IL-21 and IL-23), increased Treg cells-related cytokines (IL-10 and TGF-β), and reduced the autoantibodies levels. (C): The anti-inflammatory and bone protective mechanisms of QUE on RA: Anti-inflammatory effect: QUE decreased pro-inflammatory cytokines (TNF-α, IL-1β, IL-6, IL-8, PGE2, COX-2, iNOS, and prepro-ET-1) by regulating MAPKs (ERK, p38, JNK), NF-κB and Nrf2/HO-1 signaling pathway as well as lncRNA XIST/miR-485/PSMB8 axis; QUE decreased gp91phox expression, increased GSH levels through regulating Nrf2/HO-1 signaling pathway, indicating the participation of HO-1 in the anti-inflammatory effect of QUE; QUE inhibited FLS proliferation via inhibiting the activation of intracellular MAPKs (ERK, p38, JNK) and NF-κB signaling pathways; QUE inhibited the migration and invasion of FLS, which might be related to the up-regulatory effect on miR-146a and the down-regulatory effect on the downstream target GATA6; Besides, QUE upregulated lncRNA MALAT1, inducing the inhibitory effect on the activation of PI3K/AKT signaling pathway, leading to caspase-3, caspase-9, and Bax elevated, Bcl-2 diminished, the Bcl-2/Bax ratio decreased, ultimately to promote RAFLS apoptosis; QUE could also enhance p53 phosphorylation at ser15, leading to caspase-3 and caspase-9 activated, Bcl-2 expression diminished, Bax expression elevated, the Bcl-2/Bax ratio decreased, caused a loss in mitochondrial membrane potential, and enhanced the subsequent release of cytochrome c from mitochondria in FLS, ultimately to promote RAFLS apoptosis. Bone-protective effect: QUE suppressed RANKL expression of FLS by regulating mTOR, ERK, IκB-α and AMPK signaling pathway. QUE inhibited MMP-1 and MMP-3 expression of FLS via suppressing the activation of MAPKs (ERK, p38, JNK) and NF-κB signaling pathway.
Anti-Inflammatory Effect
Effect of QUE on Clinical Parameters and Inflammatory Parameters
Synovial inflammation is a hallmark of RA, and joint swelling reflects synovial membrane inflammation, characterized by leukocyte infiltration into the normal synovial compartment. Besides, the inflammatory milieu of the synovial compartment is correlated with the complex cytokine and chemokine network.Citation1,Citation18 Previous studies have proved that QUE could decrease paw edema in arthritis model.Citation19,Citation20
In zymosan-induced arthritis mice, QUE significantly reduced mechanical hyperalgesia and joint edema, inhibited the recruitment of total leukocytes, neutrophil and mononuclear cells, decreased the tumor necrosis factor (TNF)-α and interleukin (IL)-1β production, and inhibited zymosan-induced prepro-endothelin-1 (prepro-ET-1) and cyclooxygenase-2 (COX-2) mRNA expression in the knee joint of mice. These effects of QUE might be related to the inhibitory effect on nuclear factor (NF)-κB activation.Citation21
Similarly, QUE remarkably mitigated the paw edema and arthritis index scores, down-regulated the total pathological score (including inflammatory cells infiltration, synovium congestion and hyperplasia, and cartilage and bone erosion), decreased TNF-α, IL-1β, IL-6 and prostaglandin E2 (PGE2), inhibited nucleotide-binding oligomerization domain-like receptor family pyrin domain containing-3 (NLRP3) inflammasome (NLRP3, Caspase-1 and IL-1β) activation with no remarkable effect to pro-IL-1β and pro-Caspase-1 in CIA models.Citation22–Citation25 Further mechanistical studies suggested that QUE could improve impaired mitochondrial biogenesis and function via regulating silent information regulator 1 (SIRT1)/peroxisome proliferator-activated receptor γ coactivator-1α (PGC-1α)/nuclear respiratory factor 1 (NRF1)/mitochondrial transcription factor A (TFAM) signaling pathway, and QUE could inhibit inflammation by regulating high-mobility group box 1 (HMGB1)/Toll-like receptor 4 (TLR4)/p38/extracellular signal-regulated kinases (ERK)-1/2/NF-κB p65 signaling pathway.Citation24 But, interestingly, combined administration of QUE and methotrexate (MTX) exhibited no greater protection than administration of QUE alone for CIA mice.Citation26
As well, in AA model, oral or intra-cutaneous QUE significantly decreased arthritis index scoreCitation27,Citation28 and paw thickness, increased paw thermal latency, reduced infiltration of inflammatory cells and decreased p-P65 level in histological analysis of joint tissue.Citation28–Citation32 What’s more, intra-cutaneous QUE simultaneously with adjuvant induced and prior to the appearance of clinical signs also resulted in reduction of clinical scores, suggesting the preventive property of QUE on RA.Citation27 However, another study indicated that, in AA rats treated with QUE group, the changes in arthritis score observed were not obvious compared to the AA group, which were, partly, in contradiction with the related experimental results observed in zymosan-induced arthritis, CIA and AA model.Citation33 This might be partially associated with the difference in experimental models and administration dosage and ways. ELISIA analysis of the levels of inflammatory cytokines in AA model serum indicated that QUE decreased proinflammatory cytokines, including interferon (IFN)-γ, TNF and IL-6, increased anti-proinflammatory cytokines, including IL-4 and IL-1030. QUE also ameliorated nitric oxide (NO), decreased macrophage-derived inflammatory cytokines, including TNF-α, IL-1β, IL-6, monocyte chemotactic protein-1 (MCP-1),Citation27,Citation28,Citation32,Citation33 and myeloperoxidase (MPO) activity.Citation29 Adenosine deaminase (ADA), another inflammatory biomarker for RA.Citation34 QUE could inhibit ADA enzyme activity and gene expression in sera and joints.Citation28 Furthermore, the regulatory effect on miRNA-26b, miRNA-20a and glycogen synthase kinase-3β (GSK-3β)/NF-κB/NLRP3 signaling pathway, possibly, made contributions to the anti-inflammatory effect of the atorvastatin and QUE combination therapy on AA model.Citation32 In addition, suppression of lipoxygenase (LOX) production ameliorates inflammation of RA.Citation35 Meanwhile, QUE decreased the activity of 12/15-LOX in liver and lung of AA model, which might be correlated to the inhibitory effect of QUE on the activation of NF-κB in joint, lung and liver, and the activation of extracellular signal-regulated kinases (ERK) in joint and lung.Citation33
In vitro, an early study showed that QUE inhibited TNF-α-induced stimulation of IL-8 and MCP-1, partly, by inhibiting the activation of NF-κB in human RA fibroblast-like synoviocytes (RAFLS).Citation36 Furthermore, a recent study found that QUE could suppress TNF-α-induced production of IL-1β, IL-6 and IL-8 by targeting long non-coding RNA (lncRNA) (si)-X-inactive specific transcript (XIST), sponging microRNA (miR)-485, which, subsequently, targeting proteasome subunit β type-8 (PSMB8).Citation37 Besides, IL-1β stimulated the expression of COX-2 and PGE2, but for COX-1 in RAFLS. QUE inhibited the effects of IL-1β on COX-2 and PGE2, which were due partly to the inhibitory effect on activation of intracellular mitogen-activated protein kinase (MAPK) signaling pathways, including ERK, p38, c-Jun N-terminal kinase (JNK), and NF-κB signaling pathways.Citation38
In short, QUE attenuated clinical parameters, decreased pro-inflammatory cytokines and increased anti-inflammatory cytokines, which might be related to the regulatory effect of QUE on numerous signaling pathways, including GSK-3β, NF-κB, MAPKs (ERK, p-38, JNK), SIRT1/PGC-1α/NRF1/TFAM, and HMGB1/TLR4/p38/ERK1/2/NF-κB p65 signaling pathways, as well as lncRNA XIST/miR-485/PSMB8 axis.
Inhibition of Oxidative Stress
In rheumatoid joint, neutrophil can release various potentially harmful peptides and enzymes, and toxic oxygen metabolites to drive inflammation.Citation39 Reactive oxygen species (ROS) can activate signaling pathways involved in the inflammation of RA,Citation40 which is related to the levels of reduced glutathione (GSH), glutathione S-transferase (GST), glutathione reductase (GSR) and glutathione peroxidase (GSH-Px).Citation41
A recent study indicated that QUE could inhibit neutrophil infiltration and activation in joint of RA model and in LPS-mediated air pouch model. QUE could attenuate neutrophil invasion and increase apoptosis of activated neutrophil. In addition, QUE inhibited the formation of neutrophil extracellular traps (NETs) by suppressing autophagy.Citation30
QUE could counteract the oxidative stress associated with AA-induced in the joint tissues and plasma of rats.Citation28,Citation33 Also, QUE reduced ROS level and increased catalase activity in serum in complete Freund’s adjuvant (CFA)-induced arthritis.Citation42 As well, in zymosan-induced arthritis mice, QUE decreased gp91phox (a subunit of NADPH oxidase) mRNA expression, increased GSH levels, nuclear factor erythroid 2 related factor 2 (Nrf2) and heme oxygenase (HO-1) mRNA expression, indicating these antioxidant molecular effects of QUE might be associated with Nrf2/HO-1 signaling pathway.Citation21 As coincided with in zymosan-induced arthritis mice, QUE increased HO-1 at protein level in synovium and FLS (concentration- and time-dependent) of CIA rats.Citation22 Furthermore, in HO-1 siRNA transfected CIA-FLS, QUE or cobalt protoporphyrin IX (CoPP, the inducer of HO-1) failed to downregulate inflammatory cytokines and mediators (TNF-α, IL-1β, IL-6, PGE2, iNOS and COX-2), providing sound evidences indicating the participation of HO-1 in the anti-inflammation effects of QUE.Citation22 Interestingly, in AA rats, HO-1 protein level increased in joint, while decreased in lung, QUE treated further increased HO-1 expression in joint, and restored HO-1 to control level in lung compared to AA rats.Citation33
Briefly, QUE regulated neutrophil activities and exhibited antioxidant molecular effects to inhibit oxidative stress through Nrf2/HO-1 signaling pathway, to attenuate synovial inflammation.
Regulation of Behavior of FLS
The process that hyperplastic synovial membrane, acting as cytokine-producing tissue, facilitates structural damage is based on sustainable activation and aggressive behavior of FLS, including proliferation, migration, invasiveness and resistance to apoptosis.Citation18,Citation43
QUE inhibited IL-1β-induced proliferation of RAFLS by inhibiting the activation of intracellular MAPKs (ERK, p38, JNK) and NF-κB signaling pathways.Citation38 QUE also induced RAFLS apoptosis.Citation38 Moreover, QUE promoted RAFLS apoptosis by upregulating the lncRNA metastasis associated with lung adenocarcinoma transcript 1 (MALAT1), and MALAT1 induced RAFLS apoptosis via inhibiting the activation of the phosphoinositide 3-kinase/protein kinase B (PI3K/AKT) signaling pathway. Besides, in the RAFLS transfected with si-MALAT1, the expression of caspase-3, caspase-9 and Bax decreased, while the expression of Bcl-2 increased at protein level.Citation44 Similarly, another study indicated that QUE induced RAFLS apoptosis, activated caspase-3 and caspase-9, diminished Bcl-2 expression, elevated Bax expression, decreased the Bcl-2/Bax ratio, caused a loss in mitochondrial membrane potential, and enhanced the subsequent release of cytochrome c from mitochondria in concentration-dependent manner in RAFLS, which indicated that quercetin-induced RAFLS apoptosis through mitochondrial pathway.Citation45 It has been suggested that protein 53 (p53), a tumor suppressor, plays a vital role in regulating cellular behaviors in rheumatoid synovium.Citation46,Citation47 And, the phosphorylation of p53 at ser15 reflects its functional response to the cellular stress and leads to cell apoptosis.Citation48 QUE treatment could enhance p53 phosphorylation at ser15 in a concentration-dependent manner with no effect on the expression of total p53. Besides, further experimental results indicated that RAFLS treated with pifithrin-α (PFT-α, an inhibitor of p53) or siRNA targeting to p53 significantly abrogated quercetin-induced apoptosis, indicating that p53 activation was contributed to quercetin-induced apoptosis in RAFLS.Citation45
QUE could inhibit the migration and invasion of RAFLS in vitro, which was proved to be related to the up-regulatory effect on miR-146a and the down-regulatory effect on the downstream target GATA transcription factor 6 (GATA6) of QUE. miR-146a inhibitor transfection could enhance the migration and invasion of RAFLS. Moreover, miR-146a inhibitor transfection could inverse the inhibitory effect of QUE on RAFLS migration and invasion, abolish the suppression of QUE on GATA6 and F-actin, indicating that QUE inhibited the migration and invasion of RAFLS might be related to the regulatory effect on miR-146a/GATA6 axis.Citation49
In brief, QUE attenuated hyperplastic synovial membrane by regulating FLS behavior, including inducing apoptosis, inhibiting proliferation, migration and invasion.
Immune-Regulatory Effect
RA is an autoimmune disease. It has been identified that T cells and B cells play a crucial role in pathogenesis and pathology of RA.Citation50,Citation51 Moreover, it has proved that the presence of autoantibodies is related to more severe clinical symptoms and joint damage in RA patients.Citation1
In CIA model, the relative weight of spleen increased when compared with healthy controlled group, QUE could decrease spleen index.Citation24 Besides, QUE decreased the proportion of CD4+IL-17A+T cells, increased the percentage of CD4+CD25+Foxp3+ T cells.Citation22,Citation25 Besides, the further studies proved that QUE could significantly increase Foxp3 and decrease RORγt of Th17 cells (IL-17-producing CD4+ T cells) and Treg cells (Foxp3+ regulatory T cells) could inhibit CD4+ T cells polarized into Th17 cells and could decrease the proportion of CXCR3+IL-17A+ T cells and IFN-γ+IL-17A+CD4+ T cells, indicating the anti-arthritic effects of QUE might be partially due to the modulation of Th17/Treg cells balance and Th17 cells differentiation.Citation22,Citation25 Moreover, QUE activated peroxisome proliferator activator receptor γ (PPARγ) to promote the suppressor of cytokine signaling 3 (SOCS3) gene transcription then to inhibit signal transducer and activator of transcription 3 (STAT3) activation, QUE also redistributed the corepressor retinoid and thyroid-hormone receptors (SMRT) from PPARγ to STAT3 to inhibit the STAT3 transcriptional activity, namely, QUE target PPARγ to inhibit STAT3 by dual mechanisms, ultimately inhibiting Th17 differentiation.Citation25 But that, a little paradoxically, some experimental results were different from these. In Peripheral blood mononuclear cells (PBMCs) cultured with Th17-differentiation conditions, QUE reduced IL-17 cytokine production in culture medium, suppressed the percentage of IL-17-expressing CD4+ T cells, but exhibited no effect to the percentage of CD25Foxp3-expressing CD4+ regulatory T cells.Citation52 Different cell sources might contribute to these contradictory experimental results. QUE could also regulate the serum levels of Th17/Treg-related cytokines, namely, decreased Th17 cells-related cytokines (IL-17A, IL-21 and IL-23), increased Treg cells-related cytokines (IL-10 and TGF-β).Citation22,Citation25 In addition, QUE decreased the elevated levels of IFN-γ, IL-4 and CXCR3.Citation25,Citation29 Besides, QUE could reduce the serum autoantibodies levels, including anti-CII IgG, anti-CII IgG1 and anti-CII IgG2a in CIA models.Citation22,Citation24 A recent study indicated that QUE could diminish the sera levels of anti-cyclic citrullinated peptide antibody (anti-CCP) and rheumatoid factor (RF) in AA rats model.Citation28
Ectonucleoside triphosphate diphosphohydrolase (E-NTPDase) and ectoadenosine deaminase (E-ADA) in lymphocytes are involved in the pathogenesis of RA.Citation53,Citation54 QUE could reverse the increase of E-NTPDase activity and the decrease of E-ADA activity in lymphocytes. Besides, though there were no significant changes in the serum levels of ATP, ADP and AMP in QUE group compared with AA group, QUE lowered the increased serum adenosine levels of AA rats.Citation29
Collectively, QUE exhibited the immune-regulatory effect by restoring T cell homeostasis, regulating Th17 cells differentiation, regulating the levels of Th17/Treg-related cytokines, reducing autoantibodies production, and regulating E-NTPDase/E-ADA activities.
Bone-Protective Effect
In RA, proinflammatory cytokines, receptor activator of nuclear factor kappa B ligand (RANKL) and antibodies directed against citrullinated proteins secreted by synovitis mediate articular bone erosion, including stimulating the differentiation of bone-resorbing osteoclasts.Citation55 And, matrix metalloproteinases (MMPs) made contributions to the cartilage destruction.Citation56
QUE could inhibit IL-1β induced the expression of MMP-1, MMP-3 at mRNA and protein level in RAFLS, except for tissue inhibitor of metalloproteinase (TIMP)-1, which might be related to inhibiting the activation of intracellular MAPKs (ERK, p38, JNK) and NF-κB pathways.Citation38
QUE also suppressed IL-17 induced RANKL expression of RAFLS at mRNA and protein level, inhibited RANKL- and IL-17- produced TRAP positive osteoclasts formation, and decreased the expression of the osteoclast markers, including TRAP, cathepsin K, NF-ATc1, DC-STAMP, ATP6vOd2, and OC-STAMP. In addition, QUE exhibited similar inhibitory effect on osteoclastogenesis (TRAP positive osteoclasts formation and increased expression of the osteoclast markers) in culture system of monocytes with IL-17-prestimulated RAFLS, and in osteoclast precursors (pre-OC) cultured with Th17 cells and M-CSF. Moreover, QUE suppressed the phosphorylation of mTOR, ERK and IκB-α, while enhanced the phosphorylation of AMPK in IL-17 stimulated RAFLS, implying that these molecular effects of quercetin for RA might be mediated by aforementioned signaling pathways.Citation52
In brief, QUE exerted the bone-protective effect by decreasing MMPs, RANKL production, and osteoclasts formation by regulating MAPKs (ERK, p38, JNK), NF-κB, mTOR, ERK, IκB-α and AMPK.
Anti-Extra-Arthritic Effect
RA is a multi-systemic disease and some patients may develop extra-articular manifestations at the onset or in the progression of RA.Citation57
In CFA-induced arthritis model, QUE reduced the increased aspartate aminotransferase (AST), except for alanine aminotransferase (ALT) and alkaline phosphatase (ALP) in serum, decreased production of thiobarbituric acid-reactive substances (TBARS), and DNA damage, suggesting the hepatoprotective, genoprotective and cytoprotective effect of QUE in arthritic model.Citation42 Another study indicated that the levels of ALT and AST of methotrexate (MTX) treatment group were higher than control group, while QUE co-administered with MTX could reverse the hepatotoxicity.Citation31
Besides, in CFA-induced arthritis rats, the density of the enteric neurons and the enteric glial cells (EGC) in the myenteric and submucosal plexuses with neurodegeneration in the jejunum were remarkably decreased, glial fibrillary acidic protein (GFAP) and glial cell derived neurotrophic factor (GDNF) expression reduced, the mucosa and intestinal wall atrophied, and intestinal inflammation presented, and QUE substantially reversed most of these effects except the intestinal atrophy of the jejunum.Citation58
The antioxidant, anti-inflammatory and/or neuroprotective mechanisms might make contributions to the hepatoprotective, genoprotective and cytoprotective effect, and to the improvement of RA-induced arthritic neuropathy of QUE.
Potential Effect of QUE in Clinical Studies
Based on the effectiveness of QUE on RA in preclinical studies, some clinical studies have been performed to illuminate the protective effect on RA though related studies are few.
In a randomized double-blind clinical trial, 51 women with RA aged 19–70 years were assigned into quercetin (500 mg/day) or placebo groups for 8 weeks, finally, there were no significant differences in markers of oxidative stress including total antioxidant capacity (TAC), oxidized low-density lipoprotein (ox-LDL), malondialdehyde (MDA), and high sensitivity C-reactive protein (hs-CRP), and blood pressure between quercetin and placebo groups.Citation59
Meanwhile, subsequently, in another double-blind, placebo-controlled, randomized clinical trial, 50 women with RA were allocated to two groups: a quercetin group and a placebo group, receiving quercetin (500 mg/day) or a placebo, respectively, for 8 weeks. QUE groups presented a reduced early morning stiffness (EMS), morning pain, and after-activity pain, and a decreased plasma high-sensitivity TNF-α (hs-TNF-α) level, Disease Activity Score 28 (DAS-28) and health assessment questionnaire (HAQ) scores.Citation60
The grouping, dosage and administration method of QUE, gender of subject in the two clinical trials above were same. A study suggested that QUE exhibited no effect on oxidative or inflammatory status in RA patients, but another study indicated that QUE could significantly improve clinical symptoms and decrease inflammatory factors of RA patients. Subjects with different levels of disease activity and different evaluation indexes were the possible reasons for these differences in the two studies.
Conclusion and Future Directions
RA is a chronic inflammatory joint disease, the main pathological process includes synovial membrane inflammation, autoimmune response, cartilage and bone damage, and oxidative stress. RA patients with insufficient treatment can have various extra-articular manifestations.Citation1,Citation2,Citation61
In this review, the anti-RA effect of QUE is summarized on anti-articular and anti-extra-articular () in pre-clinical studies. Firstly, QUE decreased synovial inflammation through reducing joint clinical parameters and inflammatory cytokines, inhibiting oxidative stress, and regulating behavior of FLS. Secondly, QUE exhibited immune-regulatory effect by regulating Th17/Treg balance and Th17 cells differentiation, reducing autoantibodies levels, and regulating E-NTPDase/E-ADA activities. Thirdly, QUE exerted bone-protective effect by suppressing MMPs, RANKL expression, and inhibiting TRAP positive osteoclasts formation. Fourthly, for extra-articular manifestations, QUE exhibited cytoprotective, genoprotective and hepatoprotective effect in arthritic model, and QUE could reverse the neurodegenerative processes of enteric nervous system (ENS) in arthritic rats. Furthermore, some experimental results are paradoxical which might be due to the different experimental models, administration methods or dosages, and most of the pre-clinical evidences are derived from anti-inflammatory effect. Therefore, more pre-clinical studies, especially research on immune-regulatory, bone-protective and anti-extra-articular effect, are urgently needed in future.
Table 1 Potential Mechanism of QUE in Pre-Clinical Studies
For clinical studies, the conclusion of the current two clinical studies seemed to be confusing and the existing evidence did not show the corresponding excellent therapeutic potential in pre-clinical studies. The major gap about the efficacy of QUE on RA between pre-clinical and clinical might be attributed to the limited clinical evidence. Furthermore, clinical trials of RA patients with different disease activity, larger sample size, gender difference, exploration of administration methods or dosages, pharmacokinetics, etc. will also be needed. Only sufficient evidence of pre-clinical and clinical could form a sound basis for the clinical application of QUE for RA.
Ethics
There are no ethical issues involved in the article.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
Additional information
Funding
References
- Smolen JS, Aletaha D, McInnes IB. Rheumatoid arthritis. Lancet. 2016;388(10055):2023–2038. doi:10.1016/S0140-6736(16)30173-8
- Aletaha D, Smolen JS. Diagnosis and management of rheumatoid arthritis: a review. JAMA. 2018;320(13):1360–1372. doi:10.1001/jama.2018.13103
- Burmester GR, Pope JE. Novel treatment strategies in rheumatoid arthritis. Lancet. 2017;389(10086):2338–2348. doi:10.1016/S0140-6736(17)31491-5
- Nash P. 2019 update: EULAR RA management recommendations, efficacy and safety systematic literature reviews. Ann Rheum Dis. 2020;79:679–680. doi:10.1136/annrheumdis-2019-216821
- Andres S, Pevny S, Ziegenhagen R, et al. Safety aspects of the use of quercetin as a dietary supplement. Mol Nutr Food Res. 2018;62(1):1700447. doi:10.1002/mnfr.201700447
- Marunaka Y, Marunaka R, Sun H, et al. Actions of quercetin, a polyphenol, on blood pressure. Molecules. 2017;22(2):209. doi:10.3390/molecules22020209
- Li Y, Yao J, Han C, et al. Quercetin, Inflammation and Immunity. Nutrients. 2016;8(3):167. doi:10.3390/nu8030167
- Lupo G, Cambria MT, Olivieri M, et al. Anti-angiogenic effect of quercetin and its 8-methyl pentamethyl ether derivative in human microvascular endothelial cells. J Cell Mol Med. 2019;23(10):6565–6577. doi:10.1111/jcmm.14455
- Fernandez-Palanca P, Fondevila F, Mendez-Blanco C, Tunon MJ, Gonzalez-Gallego J, Mauriz JL. antitumor effects of quercetin in hepatocarcinoma in vitro and in vivo models: a systematic review. Nutrients. 2019;11:12. doi:10.3390/nu11122875
- Kim SH, Yoo ES, Woo JS, et al. Antitumor and apoptotic effects of quercetin on human melanoma cells involving JNK/P38 MAPK signaling activation. Eur J Pharmacol. 2019;860:172568. doi:10.1016/j.ejphar.2019.172568
- Tavana E, Mollazadeh H, Mohtashami E, et al. Quercetin: a promising phytochemical for the treatment of glioblastoma multiforme. Biofactors. 2019;46:356–366. doi:10.1002/biof.1605
- Afifi NA, Ibrahim MA, Galal MK. Hepatoprotective influence of quercetin and ellagic acid on thioacetamide-induced hepatotoxicity in rats. Can J Physiol Pharmacol. 2018;96(6):624–629. doi:10.1139/cjpp-2017-0651
- Eid HM, Haddad PS. The antidiabetic potential of quercetin: underlying mechanisms. Curr Med Chem. 2017;24(4):355–364. doi:10.2174/0929867323666160909153707
- Vaiserman A, Koliada A, Zayachkivska A, Lushchak O. Nanodelivery of natural antioxidants: an anti-aging perspective. Front Bioeng Biotechnol. 2019;7:447. doi:10.3389/fbioe.2019.00447
- Zhang XW, Chen JY, Ouyang D, Lu JH. Quercetin in animal models of alzheimer’s disease: a systematic review of preclinical studies. Int J Mol Sci. 2020;21(2). doi:10.3390/ijms21020493
- Gegout P, Gillet P, Chevrier D, Guingamp C, Terlain B, Netter P. Characterization of zymosan-induced arthritis in the rat: effects on joint inflammation and cartilage metabolism. Life Sci. 1994;55(17):PL321–326. doi:10.1016/0024-3205(94)00771-3
- Choudhary N, Bhatt LK, Prabhavalkar KS. Experimental animal models for rheumatoid arthritis. Immunopharmacol Immunotoxicol. 2018;40(3):193–200. doi:10.1080/08923973.2018.1434793
- McInnes IB, Schett G. Pathogenetic insights from the treatment of rheumatoid arthritis. Lancet. 2017;389(10086):2328–2337. doi:10.1016/S0140-6736(17)31472-1
- Guardia T, Rotelli AE, Juarez AO, Pelzer LE. Anti-inflammatory properties of plant flavonoids. Effects of rutin, quercetin and hesperidin on adjuvant arthritis in rat. Farmaco. 2001;56(9):683–687. doi:10.1016/S0014-827X(01)01111-9
- Rotelli AE, Guardia T, Juarez AO, de la Rocha NE, Pelzer LE. Comparative study of flavonoids in experimental models of inflammation. Pharmacol Res. 2003;48(6):601–606. doi:10.1016/S1043-6618(03)00225-1
- Guazelli CFS, Staurengo-Ferrari L, Zarpelon AC, et al. Quercetin attenuates zymosan-induced arthritis in mice. Biomed Pharmacother. 2018;102:175–184. doi:10.1016/j.biopha.2018.03.057
- Yang Y, Zhang X, Xu M, Wu X, Zhao F, Zhao C. Quercetin attenuates collagen-induced arthritis by restoration of Th17/Treg balance and activation of heme oxygenase 1-mediated anti-inflammatory effect. Int Immunopharmacol. 2018;54:153–162. doi:10.1016/j.intimp.2017.11.013
- Kawaguchi K, Kaneko M, Miyake R, Takimoto H, Kumazawa Y. Potent inhibitory effects of quercetin on inflammatory responses of collagen-induced arthritis in mice. Endocr Metab Immune Disord Drug Targets. 2019;19(3):308–315. doi:10.2174/1871530319666190206225034
- Shen P, Lin W, Ba X, et al. Quercetin-mediated SIRT1 activation attenuates collagen-induced mice arthritis. J Ethnopharmacol. 2021;279:114213. doi:10.1016/j.jep.2021.114213
- Yang Y, Shi GN, Wu X, et al. Quercetin impedes Th17 cell differentiation to mitigate arthritis involving ppargamma-driven transactivation of SOCS3 and redistribution corepressor SMRT from PPARgamma to STAT3. Mol Nutr Food Res. 2022:e2100826. doi:10.1002/mnfr.202100826
- Haleagrahara N, Miranda-Hernandez S, Alim MA, Hayes L, Bird G, Ketheesan N. Therapeutic effect of quercetin in collagen-induced arthritis. Biomed Pharmacother. 2017;90:38–46. doi:10.1016/j.biopha.2017.03.026
- Mamani-Matsuda M, Kauss T, Al-Kharrat A, et al. Therapeutic and preventive properties of quercetin in experimental arthritis correlate with decreased macrophage inflammatory mediators. Biochem Pharmacol. 2006;72(10):1304–1310. doi:10.1016/j.bcp.2006.08.001
- El-Said KS, Atta A, Mobasher MA, Germoush MO, Mohamed TM, Salem MM. Quercetin mitigates rheumatoid arthritis by inhibiting adenosine deaminase in rats. Mol Med. 2022;28(1):24. doi:10.1186/s10020-022-00432-5
- Saccol R, da Silveira KL, Adefegha SA, et al. Effect of quercetin on E-NTPDase/E-ADA activities and cytokine secretion of complete Freund adjuvant-induced arthritic rats. Cell Biochem Funct. 2019;37(7):474–485. doi:10.1002/cbf.3413
- Yuan K, Zhu Q, Lu Q, et al. Quercetin alleviates rheumatoid arthritis by inhibiting neutrophil inflammatory activities. J Nutr Biochem. 2020;84:108454. doi:10.1016/j.jnutbio.2020.108454
- Costa ACF, de Sousa LM, Dos Santos Alves JM, et al. Anti-inflammatory and hepatoprotective effects of quercetin in an experimental model of rheumatoid arthritis. Inflammation. 2021;44:2033–2043. doi:10.1007/s10753-021-01479-y
- Ibrahim SSA, Kandil LS, Ragab GM, El-Sayyad SM. 26b, 20a inversely correlate with GSK-3 beta/NF-kappaB/NLRP-3 pathway to highlight the additive promising effects of atorvastatin and quercetin in experimental induced arthritis. Int Immunopharmacol. 2021;99:108042. doi:10.1016/j.intimp.2021.108042
- Gardi C, Bauerova K, Stringa B, et al. Quercetin reduced inflammation and increased antioxidant defense in rat adjuvant arthritis. Arch Biochem Biophys. 2015;583:150–157. doi:10.1016/j.abb.2015.08.008
- Zamani B, Jamali R, Jamali A. Serum adenosine deaminase may predict disease activity in rheumatoid arthritis. Rheumatol Int. 2012;32(7):1967–1975. doi:10.1007/s00296-011-1912-0
- Yang W, Wang X, Xu L, Li H, Wang R. LOX inhibitor HOEC interfered arachidonic acid metabolic flux in collagen-induced arthritis rats. Am J Transl Res. 2018;10(8):2542–2554.
- Sato M, Miyazaki T, Kambe F, Maeda K, Seo H. Quercetin, a bioflavonoid, inhibits the induction of interleukin 8 and monocyte chemoattractant protein-1 expression by tumor necrosis factor-alpha in cultured human synovial cells. J Rheumatol. 1997;24(9):1680–1684.
- Sun HT, Li JP, Qian WQ, Yin MF, Yin H, Huang GC. Quercetin suppresses inflammatory cytokine production in rheumatoid arthritis fibroblast-like synoviocytes. Exp Ther Med. 2021;22(5):1260. doi:10.3892/etm.2021.10695
- Sung MS, Lee EG, Jeon HS, et al. Quercetin inhibits IL-1beta-induced proliferation and production of MMPs, COX-2, and PGE2 by rheumatoid synovial fibroblast. Inflammation. 2012;35(4):1585–1594. doi:10.1007/s10753-012-9473-2
- Wright HL, Moots RJ, Bucknall RC, Edwards SW. Neutrophil function in inflammation and inflammatory diseases. Rheumatology. 2010;49(9):1618–1631. doi:10.1093/rheumatology/keq045
- Mateen S, Moin S, Zafar A, Khan AQ. Redox signaling in rheumatoid arthritis and the preventive role of polyphenols. Clin Chim Acta. 2016;463:4–10. doi:10.1016/j.cca.2016.10.007
- Hassan MQ, Hadi RA, Al-Rawi ZS, Padron VA, Stohs SJ. The glutathione defense system in the pathogenesis of rheumatoid arthritis. J Appl Toxicol. 2001;21(1):69–73. doi:10.1002/jat.736
- Saccol R, da Silveira KL, Manzoni AG, et al. Antioxidant, hepatoprotective, genoprotective, and cytoprotective effects of quercetin in a murine model of arthritis. J Cell Biochem. 2019;121:2792–2801. doi:10.1002/jcb.29502
- Bustamante MF, Garcia-Carbonell R, Whisenant KD, Guma M. Fibroblast-like synoviocyte metabolism in the pathogenesis of rheumatoid arthritis. Arthritis Res Ther. 2017;19(1):110. doi:10.1186/s13075-017-1303-3
- Pan F, Zhu L, Lv H, Pei C. Quercetin promotes the apoptosis of fibroblast-like synoviocytes in rheumatoid arthritis by upregulating lncRNA MALAT1. Int J Mol Med. 2016;38(5):1507–1514. doi:10.3892/ijmm.2016.2755
- Xiao P, Hao Y, Zhu X, Wu X. p53 contributes to quercetin-induced apoptosis in human rheumatoid arthritis fibroblast-like synoviocytes. Inflammation. 2013;36(2):272–278. doi:10.1007/s10753-012-9543-5
- Firestein GS, Nguyen K, Aupperle KR, Yeo M, Boyle DL, Zvaifler NJ. Apoptosis in rheumatoid arthritis: p53 overexpression in rheumatoid arthritis synovium. Am J Pathol. 1996;149(6):2143–2151.
- Vaseva AV, Moll UM. The mitochondrial p53 pathway. Biochim Biophys Acta. 2009;1787(5):414–420. doi:10.1016/j.bbabio.2008.10.005
- Zhao H, Traganos F, Darzynkiewicz Z. Phosphorylation of p53 on Ser15 during cell cycle caused by Topo I and Topo II inhibitors in relation to ATM and Chk2 activation. Cell Cycle. 2008;7(19):3048–3055. doi:10.4161/cc.7.19.6750
- Zhao J, Chen B, Peng X, et al. Quercetin suppresses migration and invasion by targeting miR-146a/GATA6 axis in fibroblast-like synoviocytes of rheumatoid arthritis. Immunopharmacol Immunotoxicol. 2020;42(3):221–227. doi:10.1080/08923973.2020.1742732
- Cope AP. T cells in rheumatoid arthritis. Arthritis Res Ther. 2008;10(Suppl 1):S1. doi:10.1186/ar2412
- Dorner T, Radbruch A, Burmester GR. B-cell-directed therapies for autoimmune disease. Nat Rev Rheumatol. 2009;5(8):433–441. doi:10.1038/nrrheum.2009.141
- Kim HR, Kim BM, Won JY, et al. Quercetin, a plant polyphenol, has potential for the prevention of bone destruction in rheumatoid arthritis. J Med Food. 2019;22(2):152–161. doi:10.1089/jmf.2018.4259
- Becker LV, Rosa CS, Souza Vdo C, et al. Activities of enzymes that hydrolyze adenine nucleotides in platelets from patients with rheumatoid arthritis. Clin Biochem. 2010;43(13–14):1096–1100. doi:10.1016/j.clinbiochem.2010.06.011
- Dos Santos Jaques JA, Becker LV, Souza Vdo C, et al. Activities of enzymes that hydrolyze adenine nucleotides in lymphocytes from patients with rheumatoid arthritis. Cell Biochem Funct. 2013;31(5):395–399. doi:10.1002/cbf.2910
- Schett G, Gravallese E. Bone erosion in rheumatoid arthritis: mechanisms, diagnosis and treatment. Nat Rev Rheumatol. 2012;8(11):656–664. doi:10.1038/nrrheum.2012.153
- Rannou F, Francois M, Corvol MT, Berenbaum F. Cartilage breakdown in rheumatoid arthritis. Joint Bone Spine. 2006;73(1):29–36. doi: 10.1016/j.jbspin.2004.12.013
- Marcucci E, Bartoloni E, Alunno A, et al. Extra-articular rheumatoid arthritis. Reumatismo. 2018;70(4):212–224. doi:10.4081/reumatismo.2018.1106
- Piovezana Bossolani GD, Silva BT, Colombo Martins Perles JV, et al. Rheumatoid arthritis induces enteric neurodegeneration and jejunal inflammation, and quercetin promotes neuroprotective and anti-inflammatory actions. Life Sci. 2019;238:116956. doi:10.1016/j.lfs.2019.116956
- Javadi F, Eghtesadi S, Ahmadzadeh A, et al. The effect of quercetin on plasma oxidative status, C-reactive protein and blood pressure in women with rheumatoid arthritis. Int J Prev Med. 2014;5(3):293–301.
- Javadi F, Ahmadzadeh A, Eghtesadi S, et al. The effect of quercetin on inflammatory factors and clinical symptoms in women with rheumatoid arthritis: a double-blind, randomized controlled trial. J Am Coll Nutr. 2017;36(1):9–15. doi:10.1080/07315724.2016.1140093
- Quinonez-Flores CM, Gonzalez-Chavez SA, Del Rio Najera D, Pacheco-Tena C. Oxidative stress relevance in the pathogenesis of the rheumatoid arthritis: a systematic review. Biomed Res Int. 2016;2016:6097417. doi:10.1155/2016/6097417