
Abstract
Age-related macular degeneration (AMD), diabetic retinopathy and retinal vein occlusion represent some of the commonest degenerative conditions that lead to severe vision impairment in the developed countries. The gold standard treatment of complications associated with these conditions is the intravitreal administration of anti-vascular endothelial growth factor (VEGF) agents. Brolucizumab is a newly developed, humanised, single-chain fragment of a monoclonal antibody binding all VEGF-A isoforms, which was recently approved for the treatment of neovascular AMD. Intravitreal brolucizumab promises to reduce treatment burden for nAMD patients by achieving comparable therapeutic outcomes with fewer clinic visits. Promising also appears its use for the treatment of more challenging maculopathies like diabetic macular oedema (DMO). The aim of this review is to describe the special pharmacological properties of brolucizumab and display the outcomes of the most important clinical trials and real-world studies regarding its efficacy and safety for the management of degenerative macular disorders.
Introduction to Degenerative Macular Disorders and Their Management
Age Related Macular Degeneration
Age-related macular degeneration (AMD) is a chronic progressive disease of the macular region of the retina, which affects adults older than 65 years and leads to irreversible loss of central vision.Citation1 This ocular condition remains the leading cause of severe vision loss in the industrially developed world, accounting for 8.7% of global blindness.Citation2 It is estimated that AMD currently affects 196 million individuals worldwide, and, by 2040, this number is expected to reach 288 million cases.Citation2
AMD is classified into two types: neovascular AMD (nAMD) or wet and dry AMD. Although the neovascular form of AMD affects only 20% of AMD patients, it is responsible for the majority of cases with more severe and rapid vision loss.Citation3 The development of choroidal neovascularization (CNV) is the main characteristic of nAMD, consisting of new pathological and immature blood vessels. This pathological angiogenesis can result in infiltration of fluid that is accumulated intraretinally, subretinally or beneath the retinal pigment epithelium (RPE). Further clinical nAMD features include hard exudates, haemorrhages, RPE tears or the development of a disciform scar. Without the appropriate therapeutic intervention, these clinical deformities cause progressive damage to photoreceptors that results in reduced visual acuity.Citation4–8
AMD is multifactorial in aetiology with increased age being the strongest non-modifiable risk factor for the disease.Citation4 Environmental and lifestyle factors, such as diet and smoking, have been consistently associated with AMD risk. Hypertension and hyperlipidaemia are also likely to be involved in the development of AMD. Furthermore, there is strong genetic contribution, as many genetic variants have been implicated in AMD pathogenesis.Citation4
Treatment of nAMD targets on inhibiting angiogenesis and vascular leakage in order to achieve visual acuity maintenance or improvement.Citation9 Since vascular endothelial growth factor (VEGF) contributes significantly in the development of CNV,Citation6 the advent of VEGF inhibitors has demonstrated remarkable visual outcomes in nAMD patients.Citation3,Citation6 Until recently, three anti-VEGF agents (ranibizumab, aflibercept and bevacizumab) that block all VEGF-A isoforms, were the mainstay of nAMD treatment.Citation9 Although these medications were revolutionary, unmet needs in the management of this condition still exist. Treatment burden remains high for AMD patients due to the required frequent and indefinite evaluations.Citation10 Treatment response variability is another major concern, as many patients end up with lower vision related to subretinal fibrosis and scar formation or macular atrophy, despite anti-VEGF therapy. In addition, anti-VEGF drugs that were used so far for nAMD treatment had a short duration of therapeutic action.Citation11 For these reasons, brolucizumab, a newly developed longer-acting anti-VEGF agent, has now been added to our therapeutic options for nAMD in an effort to maintain the effectiveness of treatment while extending dosing intervals.Citation3
Polypoidal Choroidal Vasculopathy
Polypoidal choroidal vasculopathy (PCV) is considered a variant of nAMD characterised by polypoidal dilation with a branching neovascular network usually located between Bruch’s membrane and RPE.Citation12,Citation13 The presence of polypoidal lesions is best detected using indocyanine green angiography (ICGA).Citation14 Unlike typical AMD, drusen are absent in PCV and recurrent subretinal haemorrhages and serous retinal detachments are the most common clinical findings.Citation12,Citation13,Citation15
PCV is an ocular condition with greater prevalence in Asian populations that is presumably influenced by both genetic and environmental factors.Citation16,Citation17 Smoking, elevated C-reactive protein (CRP) levels, hypertension and history of central serous chorioretinopathy are some of the reported risk factors for PCV development.Citation16–18
Current options for the management of PCV include monotherapy with intravitreal anti-VEGF agents or combination with verteporfin photodynamic treatment (PDT).Citation18 Several studies have shown that brolucizumab has similar functional effects on PCV patients when compared with other anti-VEGF agents, along with significant polypoidal lesion regression on ICGA.Citation19,Citation20
Diabetic Macular Oedema
Diabetic macular edema (DMO) is the most common ocular complication leading to decreased vision among patients with diabetes mellitus. The breakdown of the inner blood-retinal barrier (BRB) associated with leakage from microaneurysms and capillary walls, is considered the main pathogenetic mechanism resulting in DMO formation.Citation21,Citation22
DMO occurs in both types of diabetic patients and its progression has been correlated with multiple risk factors, such as glycemic control, duration of diabetes, hypertension, dyslipidemia and renal status.Citation16,Citation23,Citation24 It is reported that chronic hyperglycemia causes oxidative injury to endothelial cells and a subsequent inflammatory response that leads to BRB disruption. This inflammatory response is characterised by the overexpression of different growth factors including VEGF.Citation25,Citation26
Management of diabetic patients aims primarily at the prevention of DMO by controlling all the associated systemic factors. Although laser photocoagulation had been an established treatment option for years, intravitreal anti-VEGF agents have become the treatment of choice for DMO.Citation16,Citation27 Brolucizumab is the latest anti-VEGF molecule being approved by the US Food and Drug Administration (FDA) for nAMD treatment that could be an additional therapeutic option in DMO patients, based on its encouraging functional and anatomical results.Citation28
Retinal Vein Occlusion
Retinal vein occlusion (RVO) is the second most common retinal vascular disorder after diabetic retinopathy that causes significant vision loss.Citation29 RVO can be classified into branch retinal vein occlusion (BRVO), hemiretinal vein occlusion (HRVO), and central retinal vein occlusion (CRVO) and prognosis depends on the site of obstruction.Citation30 Although all types of RVO are mainly associated with atherosclerosis, vein occlusions can also result from compression, vasoconstriction or inflammation.Citation31,Citation32 Systemic arterial hypertension, diabetes and arteriosclerosis are among the major reported risk factors for RVO occurrence.Citation29
Clinical features in RVO cases include venous tortuosity, cotton wool spots, retinal haemorrhages and optic nerve oedema that develop due to increased intravenous pressure. Vascular congestion and consequent impaired capillary exchange can lead to macular oedema (MO), which is the major cause of visual loss in RVO patients.Citation29,Citation30 Apparently, VEGF secretion represents a significant factor in MO pathogenesis resulting in increased vascular permeability and leakage.Citation16,Citation30
Because of the limitations that accompany laser and steroid treatment, MO following RVO has been mainly treated using intravitreal anti-VEGF agents.Citation16,Citation27 Brolucizumab, a newly FDA approved anti-VEGF drug, can be considered as an off-label treatment option, especially in cases with recurrent MO secondary to RVO.Citation33
Pharmacology of Brolucizumab: Molecular Characteristics, Pharmacokinetics
Drying off the affected retina through inhibiting angiogenesis and thereby the infiltration of fluid is the main goal of nAMD treatment.Citation3 Considering that VEGF has been identified as the primary contributor to CNV progression, CNV growth suppression has been displayed in monkey and mice neovascularisation models by VEGF blocking.Citation34–36 CNV regression can be achieved by the use of antibodies that impede VEGF binding to its receptor on vascular endothelial cells.Citation3
Pegaptanib sodium, an aptamer that blocks VEGF165, was the first anti-VEGF agent to be approved by the FDA in 2004.Citation37 Later in 2006, FDA approved ranibizumab following ANCHOR and MARINA trials. Ranibizumab is a fragment of an antibody binding all isoforms of VEGF-A.Citation38–40 Aflibercept was the next anti-VEGF preparation being approved for nAMD treatment in USA (2011) and Europe (2012) based on the VIEW 1 and 2 studies.Citation41 The PHOENIX study led to the approval of conbercept in China in 2013.Citation42 Both aflibercept and conbercept represent antibody fusion proteins.Citation42 In addition, bevacizumab and ziv-aflibercept are two anti-VEGF agents used “off-label”, without the approval of FDA or other similar authority.Citation43,Citation44
Current standard management for nAMD requires frequent anti-VEGF injections over a long period of time. Long-term intravitreal therapy can become a considerable burden not only for the patients but also the healthcare system that can result in undertreatment or even discontinuation with subsequent loss of vision.Citation3,Citation45 In an effort to overcome these challenges, alternative dosing regimens have been introduced, including pro re nata (PRN) and treat and extend.Citation9 In 2019, aiming in the same direction, FDA approved brolucizumab, a newly discovered anti-VEGF molecule for nAMD treatment that has demonstrated longer effect durability along with visual acuity improvement upon 12-week administration interval.Citation3
Brolucizumab is a humanised, single-chain fragment of a monoclonal antibody (scFv) blocking VEGF-A ().Citation46 ScFvs are autonomous agents with fully preserved binding capacity to their target without being dependent on a heavy molecular support structure. The variable chain domains of the monoclonal antibody (mAb), bound by a flexible linker, comprise the brolucizumab molecule. Because of their small molecular size and the lack of the Fc region, scFvs are beneficial for pharmacologic treatment.Citation47 In contrast to full-sized IgG, these binding agents have better tissue penetration and subsequently, greater local effect with longer duration and fewer adverse systemic events.Citation48,Citation49
Figure 1 Mechanism of action of Brolucizumab.
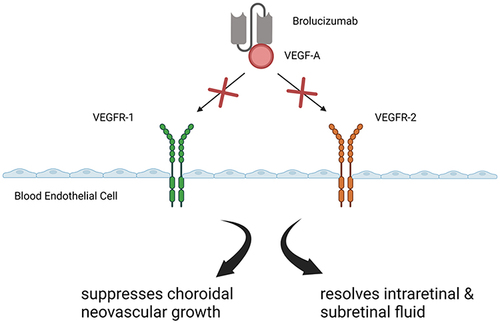
Recombinant DNA technology was used for the development of brolucizumab, the smallest VEGF antibody, with a molecular weight of 26 kDa.Citation46 The low molecular mass of brolucizumab, compared to the 115kDa of ranibizumab and 48kDa of aflibercept, along with its excellent solubility allows the production of a solution with a high concentration of 120 mg/mL. This level of concentration enables the administration of 6 mg of brolucizumab in a standard 50 μL intravitreal injection. By superiority of such characteristics, a larger number of brolucizumab molecules can be supplied intravitreally and the binding capacity to all VEGF-A isoforms are 11 to 22 times greater than aflibercept or ranibizumab. As a result, the therapeutic effect of the drug may be prolonged.Citation46 In vitro trials have also shown remarkably higher binding affinity of brolucizumab to VEGF-A isoforms than bevacizumab and blocking of binding to VEGF-A receptors VEGFR1 and VEGFR2 at considerably lower concentrations compared to ranibizumab ().Citation3,Citation45
Brolucizumab pharmacokinetics were studied in vivo, after intravitreal injection of 1 or 6 mg of the drug in both eyes of cynomolgus monkeys. Researchers estimated that brolucizumab concentration following administration was 42% and 18% of the vitreous concentration in the central retina and the choroid respectively. They also found that the mean half-life of the drug in all ocular tissues was 2.4±0.3 days. Maximum serum concentration of brolucizumab was noted to be approximately 3500 times lower than vitreous concentration and its serum clearance was 51.0 hours. These study results showed that brolucizumab reaches the choroid through the retina with minimal systemic penetration.Citation3 In further trials on monkeys, intravitreal application of brolucizumab revealed only minimal ocular inflammation without ocular or systemic toxicity. The pharmacokinetics of brolucizumab were additionally examined in cynomolgus monkeys upon intravenous administration of the drug at a concentration of 2 mg/kg. Similar to previous studies, it was found that systemic exposure of brolucizumab was minimal, as its serum half-life was determined at 5.6±1.5 hours.Citation3 It is hypothesised that the rapid systemic clearance exhibited by brolucizumab is attributed to its small molecular size and the lack of an Fc region.Citation45
These preclinical trials in non-human primate species present brolucizumab as an anti-VEGF agent with low systemic concentration and no toxicity, which would potentially relieve nAMD patients from treatment burden given that it may be administered less frequently.Citation3
Long-Term Efficacy
Neovascular AMD (nAMD)
The SEE study was the first Phase I/II, multicenter study to investigate the efficacy of a single intravitreal injection of brolucizumab (0.5, 3, 4.5, or 6 mg) compared with ranibizumab 0.5 mg in treatment naïve nAMD patients. It was found that brolucizumab 6 mg was non-inferior to ranibizumab in reducing central subfield thickness (CST) and led to greater best corrected visual acuity (BCVA) improvement. In addition, the study showed that 6 mg-brolucizumab had an efficacy duration of 75 days, which was significantly greater than the 45 days measured for ranibizumab.Citation46
The Phase II-OWL study (NCT01849692) demonstrated that brolucizumab was also efficient in improving CST and BCVA by using microvolume infusions.Citation50 Therefore, the development of a microvolume delivery system of brolucizumab that delivers fixed monthly doses over a 6-month period could possibly reduce treatment burden.Citation3
Based on the results of SEE study, regarding the more durable treatment effect of brolucizumab, the OSPREY Phase II study explored the efficacy of the drug compared with aflibercept, which is approved for q8-week dosing. During the 8-week treatment cycles, brolucizumab proved to be non-inferior to aflibercept concerning BCVA and brolucizumab-treated eyes showed greater fluid resolution. Furthermore, approximately 50% of brolucizumab-treated patients demonstrated adequate outcomes while being challenged with a 12-week dosing regimen. This key information contributed to the design of subsequent Phase III studies.Citation51
HAWK and HARRIER were the first Phase III studies to evaluate anti-VEGF therapy using 12-week treatment cycles. In these studies, which investigated the efficacy of brolucizumab versus aflibercept, brolucizumab group-patients were treated on a 12-week interval after the loading phase and adjusted to an 8-week interval in case they showed disease activity. On the other hand, patients in the aflibercept group were treated on fixed 8-week intervals according to administration protocol. Brolucizumab (q12/q8-week) exhibited noninferiority in BCVA mean change compared with aflibercept through the first year of studies. Nevertheless, brolucizumab achieved greater retinal thickness reduction and fluid resolution than aflibercept at week 48. Additionally, more than 50% of brolucizumab-treated patients were maintained on a 12-week dosing regimen throughout year 1.Citation52 Similar were the 96-week results from the HAWK and HARRIER studies, demonstrating that brolucizumab may lead to better control of nAMD and reduce treatment burden for this group of patients.Citation53 Singh et al conducted a post-hoc analysis of HAWK and HARRIER in order to investigate the effect of intravitreal brolucizumab versus aflibercept on nAMD patients with early residual fluid (ERF).Citation54 Results showed that, in ERF arm, brolucizumab achieved greater fluid resolution and CST reductions than aflibercept through week 96 of anti-VEGF therapy. Better anatomic outcomes were also associated with greater BCVA improvements in ERF patients treated with brolucizumab. This post hoc analysis suggests that the resolution of retinal fluid present at the end of loading phase may be beneficial for long-term visual outcomes in nAMD.Citation54
The MERLIN is another Phase III study initiated in 2018, evaluating the efficacy of 6 mg-brolucizumab compared to 2 mg-aflibercept administered in a 4-week dosing regimen after the loading phase in nAMD patients with persistent retinal fluid despite anti-VEGF treatment. One-year results from MERLIN revealed that brolucizumab was non-inferior to aflibercept in mean BCVA change and showed superior anatomic outcomes. However, 4-week treatment intervals were associated with higher reported frequency of serious ocular adverse events in the brolucizumab arm, such as intraocular inflammation (IOI), retinal vasculitis (RV) and retinal occlusion (RO). Therefore, Novartis announced the termination of the MERLIN study in May 2021 due to patient safety issues. Further analysis of this study data is in progress, and its results are expected to be presented at an upcoming medical meeting.Citation55
Treatment with brolucizumab includes a loading phase with three monthly injections followed by 12-week or 8-week dosing intervals and has been well studied in treatment naïve nAMD patients. Nevertheless, no clinical trial has so far explored whether loading dose is also beneficial for patients previously treated with anti-VEGF. The FALCON is a novel 52-week study in nAMD patients with unsatisfactory response to previous anti-VEGF therapy that aims to investigate the optimal initiation of brolucizumab treatment with or without loading phase. Results from the FALCON trial (NCT04679935), which is expected to be completed by 2024, will provide useful data on the necessity of loading dose in a switch situation. In addition, they will present whether switching to brolucizumab can result in optimal disease control and persistent fluid reduction.Citation56 Moreover, two more ongoing trials, the SWIFT trial (NCT04264819) and the PEREGRINE trial (NCT04697953) are looking at the efficiency of brolucizumab in patients with suboptimal anatomically controlled nAMD and in patients with nAMD with prior anti-VEGF exposure, respectively. The SWIFT trial is expected to be completed by 2023 and the PEREGRINE by 2025.
Polypoidal Choroidal Vasculopathy (PCV)
In a HAWK study subanalysis, Ogura et al presented the 96-week visual and anatomic outcomes of brolucizumab therapy compared to aflibercept in Japanese eyes diagnosed with PCV.Citation14 Subjects treated with 6 mg-brolucizumab in accordance with HAWK study treatment protocol exhibited significant visual gains, which were comparable to those achieved with aflibercept therapy on a fixed 8-week dosing regimen. In addition, greater fluid [intraretinal fluid (IRF), subretinal fluid (SRF), pigment epithelial detachment (PED)] resolution was observed in the brolucizumab group, indicating that polyps were inactive. This analysis also showed that 76% of the PCV participants in brolucizumab arm were maintained on a 12-week treatment interval after the loading dose through the first year of the study and 68% of them through the second year. Consequently, intravitreal brolucizumab could reduce treatment burden for PCV patients as well.Citation14
Diabetic Macular Oedema (DMO)
KESTREL and KITE were the first Phase III studies to evaluate the efficacy of brolucizumab versus aflibercept in DMO patients. Loading dose in brolucizumab arm included 5 injections every 6 weeks followed by a 12-week dosing regimen that adjusted to 8-week intervals in case disease activity was present. Aflibercept arm received 5 monthly injections followed by fixed 8-week treatment cycles, according to label protocol. Fifty-two -week results from KITE and KESTREL showed non-inferiority of 6 mg-brolucizumab in mean BCVA change from baseline compared to 2 mg-aflibercept. Anatomical outcomes in subjects treated with brolucizumab 6 mg were superior to those treated with aflibercept, with greater CST reductions and fluid resolution being observed. Additionally, more than 50% of 6 mg-brolucizumab subjects were maintained on a 12-week dosing regimen through year 1, with 87.6% of them in KESTREL and 95.1% in KITE remaining on a 12-week treatment interval after the first 12-week cycle. The 100-week results will give further information about the efficacy and safety of brolucizumab, which could constitute an additional therapeutic tool for DMO patients and reduce treatment burden.Citation28
Retinal Vein Occlusion (RVO)
The first Phase III clinical trials to investigate the efficacy of brolucizumab compared to aflibercept in patients with MO secondary to BRVO or CRVO were the RAPTOR and RAVEN studies respectively. Following a loading phase with 6 monthly injections of brolucizumab or aflibercept, subjects in both studies would enter a one-year individualised flexible treatment (IFT) phase. Disease stability would be evaluated at monthly visits during this phase and either an active or a sham injection would be administered on study subjects. Interruption of treatment with active injections would take place upon reaching disease stability.Citation57 The RAPTOR and RAVEN were 18-month studies that started in 2019, however Novartis announced their termination almost two years later, just before their completion, along with the MERLIN study. As mentioned above, the reason for the termination was the increased rate of serious ocular adverse events, including intraocular inflammation (IOI), retinal vasculitis (RV), and retinal vascular occlusion (RO), that were related to 4-week treatment intervals after the loading dose.Citation55
A summary of the key clinical trials is depicted in .
Table 1 Summary of the Clinical Trials on Βrolucizumab
Real-World Clinical Data
Neovascular AMD (nAMD)
Brolucizumab was approved for nAMD treatment by the FDA and the European Commission based on the pivotal Phase III HAWK and HARRIER studies. However, it was the BREW study followed by a case series by Enríquez et al, that first analysed early real-world experience with brolucizumab in eyes previously treated with other anti-VEGFs.Citation58,Citation59 Their analysis showed that brolucizumab therapy led to BCVA stabilisation as well as significant CST reduction. Additionally, this newly approved agent appeared to be effective in the resolution of persistent fluid in patients with recalcitrant nAMD.Citation58,Citation59 Similar findings regarding this group of patients in a single European clinical centre were presented by the SHIFT study.Citation60
The REBA study found that treatment-naïve and switch-therapy patients demonstrated very satisfactory visual and anatomic response to intravitreal administration of brolucizumab for nAMD that was maintained to significant extent throughout the follow-up period. Maintenance on a 12-week dosing regimen was also observed for a considerable number of eyes in both study groups.Citation61
The BRAILLE was the first study to report real-world clinical information about nAMD therapy with intravitreal brolucizumab in the Indian population. Treatment-naïve patients and those previously treated with other anti-VEGFs experienced significant visual and anatomical improvement with CST and fluid reduction.Citation62
The short-term results of loading dose therapy with brolucizumab in patients diagnosed with nAMD associated with type 1 CNV, who had not received prior treatment with other anti-VEGF agents, were presented by Matsumoto et al.Citation20 Remarkable BCVA gain was noted, along with significant reduction in macular and choroidal thickness after 3 monthly intravitreal injections of this newly approved drug.Citation20
Bilgic et al designed a study in an effort to estimate the efficacy of pro re nata (PRN) brolucizumab for the treatment of exudative AMD (PROBE study).Citation63 Study population included treatment-naïve patients that received PRN intravitreal brolucizumab without a loading dose at 8-week treatment intervals. Results revealed significant mean BCVA increase, CST reduction and fluid resolution in approximately 75% of eyes after two injections.Citation63 The same research team suggested that intravitreal brolucizumab may be beneficial for nAMD patients who develop an RPE tear, either as primary or switch therapy.Citation64
Montesel et al presented the short-term outcomes of brolucizumab therapy in treatment-naïve and switch patients with nAMD, following the treatment protocol of HAWK and HARRIER studies.Citation65 Although mean BCVA remained stable, a statistically significant reduction in macular thickness was observed, as well as fluid reduction in the different retinal compartments (IRF SRF, PED).Citation65
Since better anatomical and visual outcomes have been associated with the decrease in choroidal thickness after therapy with intravitreal aflibercept,Citation66 a multicenter study in Japan investigated the effect of brolucizumab on subfoveal choroidal thickness (SCT) of eyes with nAMD during the loading phase of treatment.Citation67 Their analysis showed remarkable SCT reduction in both treatment-naïve eyes and eyes previously treated with other anti-VEGFs. In subjects without prior treatment, greater SCT decrease was noted with intravitreal brolucizumab than that described with other anti-VEGFs, and this decrease was related to retinal fluid resolution.Citation67
Only one prospective study has so far explored the efficacy of brolucizumab after loading dose in nAMD patients that had not received prior treatment.Citation68 Its results are consistent with those reported in brolucizumab registration studies,Citation52 revealing improvements in visual acuity and macular thickness.Citation68
The efficacy of brolucizumab therapy has been further investigated in cases with chronic recalcitrant nAMD while being treated with other FDA-approved anti-VEGF agents. In a case series by Avaylon et al, this group of patients exhibited a positive response to the drug as a switch therapy, with a decline in macular thickness and fluid (IRF/SRF).Citation69 Switching to brolucizumab in eyes with insufficient response to aflibercept or ranibizumab, even at treatment intervals ≤6 weeks, proved beneficial in another prospective case series, with a reported increase in visual acuity, elongation of treatment interval and CST stability over a 6-month follow-up period.Citation70 Hussain et al showed that nAMD patients with persistent disease activity despite prior treatment with other anti-VEGFs benefited from the use of intravitreal brolucizumab in a treat-and-extend protocol.Citation71 In particular, a statistically significant CST reduction was observed in all eyes included in the study, along with complete resolution of SRF/IRF in approximately 30% of them.Citation71 Improvements in SRF and IRF, that were maintained for at least 6 months, were also noted by Awh et al after switching to brolucizumab therapy in nAMD patients refractory to ranibizumab or aflibercept.Citation72 Favourable anatomical outcomes with intravitreal brolucizumab could be attributed to better retinal tissue penetration and higher concentration per injection of the drug, which are related to its smaller molecular size. On the other hand, no statistically significant BCVA change was observed in most of the aforementioned studies, possibly due to chronic fluid presence and RPE atrophy resulting in photoreceptor damage.Citation69,Citation71
Polypoidal Choroidal Vasculopathy (PCV)
Matsumoto et al conducted a retrospective study in order to estimate the efficacy of the loading phase treatment with brolucizumab.Citation20 Participants were treatment-naïve nAMD patients with type 1 CNV including PCV. Analysis showed complete regression of polypoidal lesions in 78.9% of eyes with PCV, after 3 monthly injections of brolucizumab were administered. This regression rate was higher than that reported with aflibercept or ranibizumab monotherapy, but similar to that achieved by anti-VEGF injection combined with photodynamic therapy.Citation20
The efficacy of brolucizumab compared to aflibercept after 3 monthly intravitreal injections in treatment-naïve PCV patients was investigated by Fukuda et al.Citation19 Brolucizumab group exhibited complete fluid resolution at the 3-month visit, as well as significantly higher polypoidal lesion regression rate than the aflibercept group (78.6% vs 42.1%). However, the difference between the two treatment groups regarding BCVA improvement, macular and choroidal thickness reduction, was not statistically significant.Citation19
The regression of aneurysmal type 1 lesions after 2 intravitreal injections of brolucizumab was also described in a case report by Airaldi et al, suggesting that this new anti-VEGF agent could play an important role in aneurysmal type 1 neovascularisation management.Citation73
Diabetic Macular Oedema (DMO)
Following the encouraging first-year results of KITE and KESTREL, the efficacy of intravitreal brolucizumab in eyes with recalcitrant DMO was described in a real-world case series by Chakraborty et al.Citation27 Improvement and maintenance of visual acuity through the whole follow-up period of 16 weeks was noted in all cases. Imaging also demonstrated excellent anatomical outcomes that lasted up to 12 weeks after a single brolucizumab administration. Nevertheless, a second dose of the drug was planned in all eyes, as early fluid recurrence was observed at week 16.Citation27
In another retrospective single-centre study, patients with chronic DMO that did not respond to other approved therapies underwent off-label therapy with brolucizumab. After the first injection, a PRN treatment protocol was followed for the next injections and participants were examined monthly for at least 12 weeks. Analysis results showed statistically significant visual and anatomical improvement after the first dose that was maintained till week 12. In addition, more than 90% of the patients extended their treatment interval between 12 and 16 weeks.Citation74
Chakraborty et al were the first to report a case of contralateral response following intravitreal administration of brolucizumab in one eye of a patient with newly diagnosed bilateral DMO.Citation75 Bilateral visual gain with a reduction in macular thickness were revealed at one-month follow-up visit that were most probably associated with the phenomenon of systemic escape.Citation75
Retinal Vein Occlusion (RVO) and Other Ocular Disorders
The off-label use of intravitreal brolucizumab has been described in a case of BRVO with persistent cystoid macular oedema (CMO) that showed poor response in previous treatment with ranibizumab. After a single brolucizumab injection, the patient’s vision increased, macular fluid was completely resolved, and these favourable outcomes were reportedly maintained for 2 months.Citation33
Patel et al presented the first case of brolucizumab therapy combined with laser photocoagulation in a 9-year-old boy with advanced Coats’ disease.Citation76 Although the patient was initially treated with peripheral diode laser ablation along with intravitreal bevacizumab, SRF persisted and visual acuity had diminished. Thus, intravitreal brolucizumab was alternatively administered, resulting in acute visual acuity improvement and SRF resolution without any recurrence over a 21-week follow-up period.Citation76
Another case report demonstrated the efficacy of brolucizumab therapy in a patient with recalcitrant CMO associated with radiation maculopathy. A single injection of the drug led to visual gain and remarkable macular thickness reduction with minimal residual fluid that lasted for 8 weeks.Citation77
Murray et al studied the off-label use of intravitreal brolucizumab as a rescue therapy in a series of eyes with vision compromising macular oedema (MO) secondary to different ocular conditions, which had not responded to prior repetitive anti-VEGF or steroid treatment.Citation78 Analysis showed significant reduction of MO as well as marked BCVA improvement for all study participants following brolucizumab administration.Citation78
A summary of the real-world studies is depicted in .
Table 2 Summary of the Key Real-World Studies on Βrolucizumab
Safety and Tolerability
Neovascular AMD (nAMD)
To date, brolucizumab has been only approved by the FDA and the EMA for the treatment of nAMD, based on the findings from the HAWK and HARRIER studies.Citation53,Citation79 Except from efficacy, these Phase III clinical trials concluded that brolucizumab demonstrated an overall well-tolerated safety profile, similar to aflibercept.Citation53 Decreased visual acuity, conjunctival and retinal haemorrhage, vitreous floaters, eye pain, dry eye, cataract, and vitreous detachment were among the ocular adverse events (AEs) observed in <5% of the participants.Citation80 The incidence of IOI reported in HAWK and HARRIER 48-week results was 4.4%.Citation52,Citation79
Since the release of brolucizumab by Novartis, a number of post-marketing cases of retinal vasculitis and retinal artery occlusion leading to severe loss of vision have been reported after treatment. In February 2020, the American Society of Retina Specialists (ASRS) published an update regarding brolucizumab safety that reported 14 cases of vasculitis, the great majority of which were defined as occlusive retinal vasculitis.Citation81 Aiming to determine whether these post-marketing data indicated a safety signal for the drug, Novartis commissioned an external, independent safety review committee (SRC) to conduct a thorough review of the evidence from the phase III studies and evaluate the post-marketing reports.Citation79,Citation81
Post hoc analysis of HAWK and HARRIER by the SRC showed that the incidence of brolucizumab-related IOI was higher (4.6% vs 1.1% for eyes treated with aflibercept). Concomitant retinal vasculitis was reported in 36 of the overall 50 eyes with IOI (3.3%), 23 of which had concomitant retinal vascular occlusion (2.1%).Citation81 However, the proportion of eyes that lost ≥15 ETDRS letters was comparable between the brolucizumab (7.4%) and aflibercept (7.7%) treatment arms through week 96.Citation79,Citation81
The review committee also noted that 48% of the inflammatory cases associated with brolucizumab treatment were initially diagnosed in the first 3 months following therapy and 74% of the events were diagnosed within 6 months post-treatment. Some inflammatory events (12%) occurred between 12 and 18 months after the treatment and these patients had no reported visual acuity loss at the end of the study. Although the risk of inflammation is highest soon after the intravitreal injection is administered, ophthalmologists should apparently be vigilant for more than 12 months postinjection because inflammatory episodes may still occur within this period.Citation79,Citation81
Considering that clinical trial data on the features and outcomes of the inflammatory events following brolucizumab therapy are limited, real-world evidence may offer valuable information to ophthalmologists. Nguyen et al first published a case series of ocular adverse events from intravitreal brolucizumab.Citation82 Two cases of anterior uveitis (1.7%) were recorded, one case of panuveitis with retinal vasculitis (0.9%) and one case of central retinal artery occlusion (0.9%), while the total prevalence of ocular adverse effects was 3.5%. Although the sample size was small, their results were comparable to those presented in the HAWK trial.Citation79,Citation81
A retrospective case series that evaluated the characteristics of brolucizumab-related IOI with retinal vasculitis demonstrated that all eyes showed variable occlusion of small and large arteries as well as perivenular abnormalities. Occlusion of larger retinal arteries at the optic nerve or branches proximal to the macula was observed in some cases, leading to severe visual impairment.Citation83
The ASRS retrospectively analysed data from 25 patients diagnosed with retinal vasculitis following intravitreal brolucizumab for nAMD. More than 90% of the cases were associated with IOI with vasculitis showing a tendency for retinal arteries more than veins. Clinical examination and imaging revealed retinal vascular occlusion and/or ischemia in most eyes that were affected (83–88%). In terms of visual acuity at the most recent follow-up examination, almost half of the studied eyes (46%) lost 3 lines compared with baseline, 35% of eyes lost 6 lines or more and 46% of eyes had a BCVA of 20/200 or less.Citation84
A short-term multicenter study in Japanese patients found that brolucizumab-related IOI occurred in 9.4% of treated eyes, while the reported incidence of retinal vasculitis and retinal vascular occlusion was 3.1% and 1.6%, respectively. Three quarters of the inflammatory events developed at a mean of 23.2±9.3 days after the first injection and resolution of the active inflammation was observed within 2 months in all patients.Citation85
A cohort study that included approximately 20ʹ000 nAMD patients from the Intelligent Research in Sight (IRIS) Registry and Komodo Healthcare Map revealed an overall IOI and/or retinal occlusion incidence rate of 2.4%.Citation86 Additionally, analysis showed that the risk of developing IOI and/or retinal occlusion in the early months following the first brolucizumab administration was greater for eyes with a history of IOI and/or retinal occlusion in the 12 months preceding first brolucizumab injection.Citation85 Another study by Mukai et al concluded that the risk for emerging IOI after brolucizumab therapy was associated with female sex, older age and history of diabetes.Citation87 Female sex has been previously identified as a potential risk factor for brolucizumab-related IOI.Citation59,Citation83 Moreover, the rates of IOI, retinal vasculitis and retinal vascular occlusion were 2- to 3-fold higher among the 101 Japanese patients that participated in the HAWK study, indicating that the risk for inflammatory events after intravitreal brolucizimab could be related to patient race.Citation85
In the published reports on brolucizumab-associated ocular inflammatory events, the drug was immediately discontinued and the majority of patients were successfully treated with topical or systemic corticosteroids. However, additional administration of subtenon or intravitreal corticosteroids was required in some cases. Vitrectomy was also performed in a small number of eyes without offering any beneficial clinical outcome.Citation88
The rate of IOI with brolucizumab was higher in phase III clinical trials and according to the FDA compared to previous anti-VEGF agents (>4% vs <1%). Currently, there has been no proven explanation for this higher inflammation rate.Citation84 Presumably, the higher recorded rates of anti-brolucizumab antibodies during the HAWK and HARRIER studies could involve in the pathophysiology of brolucizumab-related IOI and vasculitis. Interestingly, 36–52% of enrolled patients had anti-brolucizumab antibodies even before the initiation of therapy. After initiation of brolucizumab treatment, these antibodies were found in 53–67% of patients, and by week 88, increased levels of anti-brolucizumab antibodies were detected in 23–25% of eyes. Researchers also observed that the percentage of inflammation was higher among patients tested positive for anti-drug antibodies (6%) than those without these antibodies (2%).Citation89 The time course and presentation of inflammation and vasculitis in most reported cases could be explained by a type III hypersensitivity reaction to the fragment of the drug antibody that leads to the aggregation and deposition of IgG/IgM complexes in retinal vessels. It has been also hypothesised that vascular occlusion could result from a type IV hypersensitivity reaction, where an intravascular inflammatory response occurs along the vessel wall, bringing the plasma in contact with the brolucizumab molecule.Citation82
Diabetic Macular Oedema (DMO)
Phase III clinical trials, KESTREL and KITE, reported an overall favourable safety profile of brolucizumab at the end of week 52. The most commonly observed ocular AEs were cataract, conjunctival haemorrhage, dry eye, vitreous floaters, vitreous detachment, diabetic retinal oedema, conjunctivitis and eye pain. The rates of ocular AEs were comparable between the treatment groups in both studies.Citation28
In both KITE and KESTREL, 17 brolucizumab-associated inflammatory events were noted in the 3 mg arm and 13 events in the 6 mg arm, whereas 5 inflammatory events were recorded in the aflibercept arm. One participant in the brolucizumab 6mg group of KESTREL experienced retinal vasculitis and retinal artery occlusion (RAO), while 3 cases of retinal vasculitis were reported in the brolucizumab 3 mg group. In KITE, RAO occurred in 1 subject from brolucizumab 6 mg arm and 1 subject from aflibercept arm, without any reported case of retinal vasculitis.Citation28
Although the incidence of IOI in the KESTREL study was similar to that reported in the HAWK and HARRIER studies, the rates of retinal vasculitis were lower. Lower IOI rates were also noted in the KITE study compared to brolucizumab registration trials for nAMD. This deviation in the number of inflammatory cases between DMO and nAMD studies could be probably attributed to the less intensive 6-week dosing regimen of the loading phase in KITE and KESTREL, differences between the studies or the underlying diseases of DMO and nAMD.
Other Ocular Disorders
As it has been mentioned, the increased rate of serious ocular adverse events, including IOI, retinal vasculitis and retinal vascular occlusion, during the RAPTOR and RAVEN studies led to the termination of these clinical trials that investigated the efficacy and safety of intravitreal brolucizumab for the treatment of MO secondary to RVO.
A HAWK study subanalysis in Japanese participants with PCV found that brolucizumab was well tolerated and the safety profile of the drug was similar to that reported for the overall HAWK population. Cataract and allergic conjunctivitis were the most frequent ocular AEs. The incidence of IOI was higher in the brolucizumab group (15.4%) compared with aflibercept therapy.Citation14 An increased rate of brolucizumab-associated inflammatory events was also noted in real-world studies that explored the outcomes of brolucizumab therapy in PCV patients.Citation19,Citation20
No signs of IOI or vasculitis were observed after treatment with brolucizumab in cases of advanced Coats’ disease and radiation maculopathy.Citation76,Citation77 Further long-term prospective studies are required in order to address the efficacy and safety of brolucizumab for these conditions.
Cost-Effectiveness
The treatment burden of nAMD is substantial from an economic aspect not only for the patients but also the health system. A survey in the United States showed that vision loss due to nAMD was significantly correlated with higher societal costs, including medical and nonmedical costs, as well as indirect costs resulting from lower salary or loss of employment.Citation90 Another study found that nAMD was associated with a decrease in quality of life. The rates of anxiety and depression were increased among nAMD patients who also needed assistance for their daily activities.Citation91
Yu et al were the first to evaluate the cost-effectiveness of brolucizumab therapy compared with ranibizumab and aflibercept. The results of their model revealed that brolucizumab was more cost-effective than the other anti-VEGF agents, based on the phase III treatment protocol of the drug.Citation92 Specifically, brolucizumab proved to be less costly than aflibercept and ranibizumab in the base case ($63,614 vs $72,189 and $128,163 respectively), but also over a 5-year time horizon ($44,644 vs $50,772 and $89,665) due to lower drug, administration and monitoring costs.Citation92
Similarly, an analysis from the Italian National Healthcare Service demonstrated that the cost-effectiveness of brolucizumab was superior to aflibercept, meaning that treatment with brolucizumab could reduce the economic burden of intravitreal injections and improve the quality of life in nAMD patients in the upcoming years.Citation93
Future Directions
As already discussed, intravitreal administration of anti-VEGF agents is the gold standard of nAMD treatment.Citation9 However, intravitreal therapy (IVT) is invasive, painful and may cause severe ocular and systemic complications.Citation94,Citation95 Furthermore, long-term IVT can drive patients into financial distress, while therapeutic response may be decreased because of repeated injections.Citation96 Brolucizumab is a new therapeutic tool in the management of nAMD that promises to reduce treatment burden. Clinical data show that brolucizumab-treated patients demonstrate superior anatomical improvement and can reach non-inferior visual outcomes with extended dosing intervals.Citation3
Although promising, brolucizumab holds the limitations of IVT. The intervention of nanotechnology brought a revolution in the treatment strategy of AMD, which currently requires continuous active release of the anti-VEGF agent in order to achieve maximal therapeutic effect and avoid the complications following multiple injections. Nanotechnology-based delivery systems that offer benefits including improved drug bioavailability, accumulation in target areas, controlled release and lower toxicity are being explored as future alternatives to IVT for nAMD treatment.Citation96
Aside from longer-acting anti-VEGFs like brolucizumab and sustained-release delivery systems, gene therapy and molecules targeting other factors involved in the angiogenesis cascade are among the most innovative approaches expected to play a major role in the future management of nAMD.
Conclusion
To date, phase III clinical trials and real-world studies have proven that brolucizumab is an effective therapeutic option for nAMD that could possibly reduce the treatment burden associated with the disease. Promising functional and anatomical results have been demonstrated with its use for DMO and other ocular conditions, such as PCV and MO secondary to RVO. Long-term, prospective, multicenter, world-wide studies need to be designed in order to better understand the treatment patterns and determine the safety of this new anti-VEGF agent.
Brolucizumab was also reported to be efficient for the treatment of less common diseases like Coats’ and radiation maculopathy. Obviously, further research is required on these topics, because no safe conclusion can be drawn based on individual cases.
Although brolucizumab appears as a valuable tool for the optimal management of nAMD, a number of serious post-marketing inflammatory events have been reported. Therefore, it is critical for ophthalmologists to monitor their patients and manage these AEs adequately. Moreover, practitioners should carefully weigh the potential risks against the demonstrated efficacy of brolucizumab when making decisions on nAMD treatment.
Citation
Karasavvidou EM, Tranos P, Panos GD. Brolucizumab for the treatment of degenerative macular conditions: a review of clinical studies.
Disclosure
The authors report no conflicts of interest in this work.
References
- Joussen AM, Bornfeld N. The treatment of wet age-related macular degeneration. Dtsch Arztebl Int. 2009;106(18):312–317. doi:10.3238/arztebl.2009.0312
- Wong WL, Su X, Li X, et al. Global prevalence of age-related macular degeneration and disease burden projection for 2020 and 2040: a systematic review and meta-analysis. Lancet Glob Health. 2014;2(2):e106–116. doi:10.1016/S2214-109X(13)70145-1
- Nguyen QD, Das A, Do DV, et al. Brolucizumab: evolution through preclinical and clinical studies and the implications for the management of neovascular age-related macular degeneration. Ophthalmology. 2020;127(7):963–976. doi:10.1016/j.ophtha.2019.12.031
- Mitchell P, Liew G, Gopinath B, Wong TY. Age-related macular degeneration. Lancet. 2018;392(10153):1147–1159. doi:10.1016/S0140-6736(18)31550-2
- Holz FG, Schmitz-Valckenberg S, Fleckenstein M. Recent developments in the treatment of age-related macular degeneration. J Clin Invest. 2014;124(4):1430–1438. doi:10.1172/JCI71029
- Bakri SJ, Thorne JE, Ho AC, et al. Safety and efficacy of anti-vascular endothelial growth factor therapies for neovascular age-related macular degeneration: a report by the American Academy of ophthalmology. Ophthalmology. 2019;126(1):55–63. doi:10.1016/j.ophtha.2018.07.028
- Ersoz MG, Karacorlu M, Arf S, Sayman Muslubas I, Hocaoglu M. Retinal pigment epithelium tears: classification, pathogenesis, predictors, and management. Surv Ophthalmol. 2017;62(4):493–505. doi:10.1016/j.survophthal.2017.03.004
- Daniel E, Grunwald JE, Kim BJ, et al. Visual and morphologic outcomes in eyes with hard exudate in the comparison of age-related macular degeneration treatments trials. Ophthalmol Retina. 2017;1(1):25–33. doi:10.1016/j.oret.2016.09.001
- Wykoff CC, Clark WL, Nielsen JS, Brill JV, Greene LS, Heggen CL. Optimizing anti-VEGF treatment outcomes for patients with neovascular age-related macular degeneration. J Manag Care Spec Pharm. 2018;24(2–aSuppl):S3–S15. doi:10.18553/jmcp.2018.24.2-A.s3
- Ferreira A, Sagkriotis A, Olson M, Lu J, Makin C, Milnes F. Treatment frequency and dosing interval of ranibizumab and aflibercept for neovascular age-related macular degeneration in routine clinical practice in the USA. PLoS One. 2015;10(7):e0133968. doi:10.1371/journal.pone.0133968
- Munk MR, Ceklic L, Ebneter A, Huf W, Wolf S, Zinkernagel MS. Macular atrophy in patients with long-term anti-VEGF treatment for neovascular age-related macular degeneration. Acta Ophthalmol. 2016;94(8):e757–e764. doi:10.1111/aos.13157
- Fenner BJ, Cheung CMG, Sim SS, et al. Evolving treatment paradigms for PCV. Eye. 2022;36(2):257–265. doi:10.1038/s41433-021-01688-7
- Goldhardt R, Rosen BS. Polypoidal Choroidal Vasculopathy. Curr Ophthalmol Rep. 2019;7(1):66–72. doi:10.1007/s40135-019-00201-4
- Ogura Y, Jaffe GJ, Cheung CMG, et al. Efficacy and safety of brolucizumab versus aflibercept in eyes with polypoidal choroidal vasculopathy in Japanese participants of HAWK. Br J Ophthalmol. 2021;106:994–999. doi:10.1136/bjophthalmol-2021-319090
- Koh AH, Expert PC, Chen LJ, et al. Polypoidal choroidal vasculopathy: evidence-based guidelines for clinical diagnosis and treatment. Retina. 2013;33(4):686–716. doi:10.1097/IAE.0b013e3182852446
- Triantafylla M, Massa HF, Dardabounis D, et al. Ranibizumab for the treatment of degenerative ocular conditions. Clin Ophthalmol. 2014;8:1187–1198. doi:10.2147/OPTH.S40350
- Wong CW, Yanagi Y, Lee WK, et al. Age-related macular degeneration and polypoidal choroidal vasculopathy in Asians. Prog Retin Eye Res. 2016;53:107–139. doi:10.1016/j.preteyeres.2016.04.002
- Cheung CMG, Lai TYY, Ruamviboonsuk P, et al. Polypoidal choroidal vasculopathy: definition, pathogenesis, diagnosis, and management. Ophthalmology. 2018;125(5):708–724. doi:10.1016/j.ophtha.2017.11.019
- Fukuda Y, Sakurada Y, Matsubara M, et al. Comparison of outcomes between 3 monthly brolucizumab and aflibercept injections for polypoidal choroidal vasculopathy. Biomedicines. 2021;9(9):1164. doi:10.3390/biomedicines9091164
- Matsumoto H, Hoshino J, Mukai R, Nakamura K, Akiyama H. Short-term outcomes of intravitreal brolucizumab for treatment-naive neovascular age-related macular degeneration with type 1 choroidal neovascularization including polypoidal choroidal vasculopathy. Sci Rep. 2021;11(1):6759. doi:10.1038/s41598-021-86014-7
- Bandello F, Battaglia Parodi M, Lanzetta P, et al. Diabetic macular edema. Dev Ophthalmol. 2017;58:102–138.
- Bresnick GH. Diabetic macular edema. A review. Ophthalmology. 1986;93(7):989–997. doi:10.1016/S0161-6420(86)33650-9
- Girach A, Lund-Andersen H. Diabetic macular oedema: a clinical overview. Int J Clin Pract. 2007;61(1):88–97. doi:10.1111/j.1742-1241.2006.01211.x
- Williams R, Airey M, Baxter H, Forrester J, Kennedy-Martin T, Girach A. Epidemiology of diabetic retinopathy and macular oedema: a systematic review. Eye. 2004;18(10):963–983. doi:10.1038/sj.eye.6701476
- Gardner TW, Antonetti DA, Barber AJ, LaNoue KF, Levison SW. Diabetic retinopathy: more than meets the eye. Surv Ophthalmol. 2002;47(Suppl 2):S253–262. doi:10.1016/S0039-6257(02)00387-9
- Grant MB, Afzal A, Spoerri P, Pan H, Shaw LC, Mames RN. The role of growth factors in the pathogenesis of diabetic retinopathy. Expert Opin Investig Drugs. 2004;13(10):1275–1293. doi:10.1517/13543784.13.10.1275
- Chakraborty D, Sheth JU, Boral S, Sinha TK. Off-label intravitreal brolucizumab for recalcitrant diabetic macular edema: a real-world case series. Am J Ophthalmol Case Rep. 2021;24:101197. doi:10.1016/j.ajoc.2021.101197
- Brown DM, Emanuelli A, Bandello F, et al. KESTREL and KITE: 52-week results from two phase III pivotal trials of brolucizumab for diabetic macular edema. Am J Ophthalmol. 2022;238:157–172. doi:10.1016/j.ajo.2022.01.004
- Ip M, Hendrick A. Retinal vein occlusion review. Asia Pac J Ophthalmol. 2018;7(1):40–45.
- Wong TY, Scott IU. Clinical practice. Retinal-vein occlusion. N Engl J Med. 2010;363(22):2135–2144. doi:10.1056/NEJMcp1003934
- O’Mahoney PR, Wong DT, Ray JG. Retinal vein occlusion and traditional risk factors for atherosclerosis. Arch Ophthalmol. 2008;126(5):692–699. doi:10.1001/archopht.126.5.692
- Yen YC, Weng SF, Chen HA, Lin YS. Risk of retinal vein occlusion in patients with systemic lupus erythematosus: a population-based cohort study. Br J Ophthalmol. 2013;97(9):1192–1196. doi:10.1136/bjophthalmol-2013-303265
- Panigrahi PK. Off label intravitreal Brolucizumab in treatment of recurrent macular edema due to branch retinal vein occlusion: a case report. Photodiagnosis Photodyn Ther. 2022;37:102694. doi:10.1016/j.pdpdt.2021.102694
- Campochiaro PA, Aiello LP, Rosenfeld PJ. Anti-vascular endothelial growth factor agents in the treatment of retinal disease: from bench to bedside. Ophthalmology. 2016;123(10):S78–S88. doi:10.1016/j.ophtha.2016.04.056
- Krzystolik MG, Afshari MA, Adamis AP, et al. Prevention of experimental choroidal neovascularization with intravitreal anti-vascular endothelial growth factor antibody fragment. Arch Ophthalmol. 2002;120(3):338–346. doi:10.1001/archopht.120.3.338
- Saishin Y, Saishin Y, Takahashi K, et al. VEGF-TRAP(R1R2) suppresses choroidal neovascularization and VEGF-induced breakdown of the blood-retinal barrier. J Cell Physiol. 2003;195(2):241–248. doi:10.1002/jcp.10246
- Group VISiONCT, Gragoudas ES, Adamis AP, Cunningham ET, Feinsod M, Guyer DR. Pegaptanib for neovascular age-related macular degeneration. N Engl J Med. 2004;351(27):2805–2816. doi:10.1056/NEJMoa042760
- Schmidt-Erfurth U, Chong V, Loewenstein A, et al. Guidelines for the management of neovascular age-related macular degeneration by the European Society of Retina Specialists (EURETINA). Br J Ophthalmol. 2014;98(9):1144–1167. doi:10.1136/bjophthalmol-2014-305702
- Brown DM, Kaiser PK, Michels M, et al. Ranibizumab versus verteporfin for neovascular age-related macular degeneration. N Engl J Med. 2006;355(14):1432–1444. doi:10.1056/NEJMoa062655
- Rosenfeld PJ, Brown DM, Heier JS, et al. Ranibizumab for neovascular age-related macular degeneration. N Engl J Med. 2006;355(14):1419–1431. doi:10.1056/NEJMoa054481
- Heier JS, Brown DM, Chong V, et al. Intravitreal aflibercept (VEGF trap-eye) in wet age-related macular degeneration. Ophthalmology. 2012;119(12):2537–2548. doi:10.1016/j.ophtha.2012.09.006
- Liu K, Song Y, Xu G, et al. Conbercept for treatment of neovascular age-related macular degeneration: results of the randomized phase 3 phoenix study. Am J Ophthalmol. 2019;197:156–167. doi:10.1016/j.ajo.2018.08.026
- Maguire MG, Martin DF, Ying G-S, et al.; Comparison of Age-related Macular Degeneration Treatments Trials Research Group. Five-year outcomes with anti-vascular endothelial growth factor treatment of neovascular age-related macular degeneration: the comparison of age-related macular degeneration treatments trials. Ophthalmology. 2016;123(8):1751–1761. doi:10.1016/j.ophtha.2016.03.045
- de Oliveira Dias JR, de Andrade GC, Novais EA, Farah ME, Rodrigues EB. Fusion proteins for treatment of retinal diseases: aflibercept, ziv-aflibercept, and conbercept. Int J Retina Vitreous. 2016;2:3. doi:10.1186/s40942-016-0026-y
- Tadayoni R, Sararols L, Weissgerber G, Verma R, Clemens A, Holz FG. Brolucizumab: a newly developed anti-VEGF molecule for the treatment of neovascular age-related macular degeneration. Ophthalmologica. 2021;244(2):93–101. doi:10.1159/000513048
- Holz FG, Dugel PU, Weissgerber G, et al. Single-chain antibody fragment VEGF inhibitor RTH258 for neovascular age-related macular degeneration: a randomized controlled study. Ophthalmology. 2016;123(5):1080–1089. doi:10.1016/j.ophtha.2015.12.030
- Miller BR, Demarest SJ, Lugovskoy A, et al. Stability engineering of scFvs for the development of bispecific and multivalent antibodies. Protein Eng Des Sel. 2010;23(7):549–557. doi:10.1093/protein/gzq028
- Yokota T, Milenic DE, Whitlow M, Schlom J. Rapid tumor penetration of a single-chain Fv and comparison with other immunoglobulin forms. Cancer Res. 1992;52(12):3402–3408.
- Borras L, Gunde T, Tietz J, et al. Generic approach for the generation of stable humanized single-chain Fv fragments from rabbit monoclonal antibodies. J Biol Chem. 2010;285(12):9054–9066. doi:10.1074/jbc.M109.072876
- Berger BB, Yanni SE, Wenzel A, Weichselberger A, Hubschman JP. Efficacy of RTH258 (ESBA1008), an anti-VEGF agent, applied by microvolume injection or infusion in subjects with neovascular AMD. The Annual Meeting of the Association for Research in Vision and Ophthalmology (ARVO); 2015; Denver, Colorado.
- Dugel PU, Jaffe GJ, Sallstig P, et al. Brolucizumab versus aflibercept in participants with neovascular age-related macular degeneration: a randomized trial. Ophthalmology. 2017;124(9):1296–1304. doi:10.1016/j.ophtha.2017.03.057
- Dugel PU, Koh A, Ogura Y, et al. HAWK and HARRIER: phase 3, multicenter, randomized, double-masked trials of brolucizumab for neovascular age-related macular degeneration. Ophthalmology. 2020;127(1):72–84. doi:10.1016/j.ophtha.2019.04.017
- Dugel PU, Singh RP, Koh A, et al. HAWK and HARRIER: ninety-six-week outcomes from the phase 3 trials of brolucizumab for neovascular age-related macular degeneration. Ophthalmology. 2021;128(1):89–99. doi:10.1016/j.ophtha.2020.06.028
- Singh RP, Jhaveri C, Wykoff CC, et al. Efficacy outcomes of brolucizumab versus aflibercept in neovascular age-related macular degeneration patients with early residual fluid. Ophthalmol Retina. 2022;6(5):377–386. doi:10.1016/j.oret.2021.12.014
- Novartis. Novartis reports one year results of Phase III MERLIN study evaluating Beovu® every four week dosing and provides update on Beovu clinical program; 2021. Available from: https://www.novartis.com/news/media-releases/novartis-reports-one-year-results-phase-iii-merlin-study-evaluating-beovu-every-four-week-dosing-and-provides-update-beovu-clinical-program. Accessed August 5, 2022.
- Holz FG, Schmitz-Valckenberg S, Wolf A, et al. A randomized, open-label, multicenter study of switching to brolucizumab with or without a loading dose for patients with suboptimal anatomically controlled neovascular age-related macular degeneration-the FALCON study. Graefes Arch Clin Exp Ophthalmol. 2022. doi:10.1007/s00417-022-05591-z
- Group RS. Assessing the efficacy and safety of brolucizumab versus aflibercept in patients with visual impairment due to macular edema secondary to branch retinal vein occlusion (RAPTOR); 2022. Available from: https://clinicaltrials.gov/ct2/show/NCT03802630. Accessed August 5, 2022.
- Sharma A, Kumar N, Parachuri N, et al. Brolucizumab-early real-world experience: BREW study. Eye. 2021;35(4):1045–1047. doi:10.1038/s41433-020-1111-x
- Enriquez AB, Baumal CR, Crane AM, et al. Early experience with brolucizumab treatment of neovascular age-related macular degeneration. JAMA Ophthalmol. 2021;139(4):441–448. doi:10.1001/jamaophthalmol.2020.7085
- Bulirsch LM, Sassmannshausen M, Nadal J, Liegl R, Thiele S, Holz FG. Short-term real-world outcomes following intravitreal brolucizumab for neovascular AMD: SHIFT study. Br J Ophthalmol. 2021;bjophthalmol-2020-318672. doi:10.1136/bjophthalmol-2020-318672
- Bilgic A, Kodjikian L, March de Ribot F, et al. Real-world experience with brolucizumab in wet age-related macular degeneration: the REBA study. J Clin Med. 2021;10(13):2758. doi:10.3390/jcm10132758
- Chakraborty D, Maiti A, Sheth JU, et al. Brolucizumab in neovascular age-related macular degeneration - Indian real-world experience: the BRAILLE study. Clin Ophthalmol. 2021;15:3787–3795. doi:10.2147/OPTH.S328160
- Bilgic A, Kodjikian L, Srivastava S, et al. Initial pro re nata brolucizumab for exudative AMD: the PROBE study. J Clin Med. 2021;10(18):4153. doi:10.3390/jcm10184153
- Bilgic A, Kodjikian L, Vasavada S, et al. Brolucizumab for choroidal neovascular membrane with pigment epithelial tear and subretinal fluid. J Clin Med. 2021;10(11):2425. doi:10.3390/jcm10112425
- Montesel A, Bucolo C, Sallo FB, Eandi CM. Short-term efficacy and safety outcomes of brolucizumab in the real-life clinical practice. Front Pharmacol. 2021;12:720345. doi:10.3389/fphar.2021.720345
- Koizumi H, Kano M, Yamamoto A, et al. Subfoveal choroidal thickness during aflibercept therapy for neovascular age-related macular degeneration: twelve-month results. Ophthalmology. 2016;123(3):617–624. doi:10.1016/j.ophtha.2015.10.039
- Tamashiro T, Tanaka K, Itagaki K, et al. Subfoveal choroidal thickness after brolucizumab therapy for neovascular age-related macular degeneration: a short-term multicenter study. Graefes Arch Clin Exp Ophthalmol. 2022;260(6):1857–1865. doi:10.1007/s00417-021-05517-1
- Michalska-Malecka K, Spiewak D, Luksa D. Three-month results of brolucizumab intravitreal therapy in patients with wet age-related macular degeneration. Int J Environ Res Public Health. 2021;18(16):8450. doi:10.3390/ijerph18168450
- Avaylon J, Lee S, Gallemore RP. Case series on initial responses to intravitreal brolucizumab in patients with recalcitrant chronic wet age-related macular degeneration. Int Med Case Rep J. 2020;13:145–152. doi:10.2147/IMCRJ.S252260
- Haensli C, Pfister IB, Garweg JG. Switching to brolucizumab in neovascular age-related macular degeneration incompletely responsive to ranibizumab or aflibercept: real-life 6 month outcomes. J Clin Med. 2021;10(12):2666. doi:10.3390/jcm10122666
- Hussain RM, Neal A, Yannuzzi NA, et al. Brolucizumab for persistent macular fluid in neovascular age-related macular degeneration after prior anti-VEGF treatments. Ther Adv Ophthalmol. 2021;13:25158414211055964. doi:10.1177/25158414211055964
- Awh CC, Davis EC, Thomas MK, Thomas AS. Short-term outcomes after interim treatment with brolucizumab: a retrospective case series of a single center experience. Retina. 2022;42(5):899–905. doi:10.1097/IAE.0000000000003418
- Airaldi M, Cozzi M, Staurenghi G. Regression of aneurysmal type 1 neovascularization after brolucizumab injections. Can J Ophthalmol. 2021. doi:10.1016/j.jcjo.2021.09.001
- Chakraborty D, Mondal S, Parachuri N, Kumar N, Sharma A. Brolucizumab-early experience with early extended interval regime in chronic centre involved diabetic macular oedema. Eye. 2022;36(2):358–360. doi:10.1038/s41433-021-01816-3
- Chakraborty S, Sheth JU. Contralateral effect following intravitreal brolucizumab injection in diabetic macular edema. Case Rep Ophthalmol Med. 2022;2022:3755249. doi:10.1155/2022/3755249
- Patel NA, Berrocal AM, Murray TG, Villegas VM. Advanced Coats’ disease treated with intravitreal brolucizumab combined with laser photocoagulation. Am J Ophthalmol Case Rep. 2020;19:100815. doi:10.1016/j.ajoc.2020.100815
- Corradetti G, Corvi F, Juhn A, Sadda SR. Short-term outcomes following treatment of recalcitrant cystoid macular edema secondary to radiation maculopathy using intravitreal brolucizumab. Am J Ophthalmol Case Rep. 2020;20:100981. doi:10.1016/j.ajoc.2020.100981
- Murray JE, Gold AS, Latiff A, Murray TG. Brolucizumab: evaluation of compassionate use of a complex anti-VEGF therapy. Clin Ophthalmol. 2021;15:4731–4738. doi:10.2147/OPTH.S339393
- Kilmartin DJ. Literature review and proposal of best practice for ophthalmologists: monitoring of patients following intravitreal brolucizumab therapy. Ir J Med Sci. 2022. doi:10.1007/s11845-022-02929-8
- Sharma A, Parachuri N, Kumar N, et al. Brolucizumab-key learnings from HAWK and HARRIER. Eye. 2020;34(8):1318–1320. doi:10.1038/s41433-020-0842-z
- Mones J, Srivastava SK, Jaffe GJ, et al. Risk of inflammation, retinal vasculitis, and retinal occlusion-related events with brolucizumab: post hoc review of HAWK and HARRIER. Ophthalmology. 2021;128(7):1050–1059. doi:10.1016/j.ophtha.2020.11.011
- Nguyen HV, Li AS, Silva AR, Leng T. Ocular adverse events following intravitreal brolucizumab for neovascular age-related macular degeneration at a single tertiary care center. Eur J Ophthalmol. 2021;11206721211059332. doi:10.1177/11206721211059332
- Baumal CR, Spaide RF, Vajzovic L, et al. Retinal vasculitis and intraocular inflammation after intravitreal injection of brolucizumab. Ophthalmology. 2020;127(10):1345–1359. doi:10.1016/j.ophtha.2020.04.017
- Witkin AJ, Hahn P, Murray TG, et al. Occlusive retinal vasculitis following intravitreal brolucizumab. J Vitreoretin Dis. 2020;4(4):269–279. doi:10.1177/2474126420930863
- Maruko I, Okada AA, Iida T, et al. Brolucizumab-related intraocular inflammation in Japanese patients with age-related macular degeneration: a short-term multicenter study. Graefes Arch Clin Exp Ophthalmol. 2021;259(9):2857–2859. doi:10.1007/s00417-021-05136-w
- Khanani AM, Zarbin MA, Barakat MR, et al. Safety outcomes of brolucizumab in neovascular age-related macular degeneration: results from the IRIS registry and komodo healthcare map. JAMA Ophthalmol. 2022;140(1):20–28. doi:10.1001/jamaophthalmol.2021.4585
- Mukai R, Matsumoto H, Akiyama H. Risk factors for emerging intraocular inflammation after intravitreal brolucizumab injection for age-related macular degeneration. PLoS One. 2021;16(12):e0259879. doi:10.1371/journal.pone.0259879
- Baumal CR, Bodaghi B, Singer M, et al. Expert opinion on management of intraocular inflammation, retinal vasculitis, and vascular occlusion after brolucizumab treatment. Ophthalmol Retina. 2021;5(6):519–527. doi:10.1016/j.oret.2020.09.020
- Witkin AJ, Hahn P, Murray TG, et al. Brolucizumab-associated intraocular inflammation in eyes without retinal vasculitis. J Vitreoretin Dis. 2021;5(4):326–332. doi:10.1177/2474126420975303
- Brown MM, Brown GC, Lieske HB, Tran I, Turpcu A, Colman S. Societal costs associated with neovascular age-related macular degeneration in the United States. Retina. 2016;36(2):285–298. doi:10.1097/IAE.0000000000000717
- Soubrane G, Cruess A, Lotery A, et al. Burden and health care resource utilization in neovascular age-related macular degeneration: findings of a multicountry study. Arch Ophthalmol. 2007;125(9):1249–1254. doi:10.1001/archopht.125.9.1249
- Yu JS, Carlton R, Agashivala N, Hassan T, Wykoff CC. Brolucizumab vs aflibercept and ranibizumab for neovascular age-related macular degeneration: a cost-effectiveness analysis. J Manag Care Spec Pharm. 2021;27(6):743–752. doi:10.18553/jmcp.2021.27.6.743
- Ferrante N, Ritrovato D, Bitonti R, Furneri G. Cost-effectiveness analysis of brolucizumab versus aflibercept for the treatment of neovascular age-related macular degeneration (nAMD) in Italy. BMC Health Serv Res. 2022;22(1):573. doi:10.1186/s12913-022-07972-w
- Mahaling B, Srinivasarao DA, Raghu G, Kasam RK, Bhanuprakash Reddy G, Katti DS. A non-invasive nanoparticle mediated delivery of triamcinolone acetonide ameliorates diabetic retinopathy in rats. Nanoscale. 2018;10(35):16485–16498. doi:10.1039/C8NR00058A
- Falavarjani KG, Nguyen QD. Adverse events and complications associated with intravitreal injection of anti-VEGF agents: a review of literature. Eye. 2013;27(7):787–794. doi:10.1038/eye.2013.107
- Sarkar A, Dyawanapelly S. Nanodiagnostics and nanotherapeutics for age-related macular degeneration. J Control Release. 2021;329:1262–1282. doi:10.1016/j.jconrel.2020.10.054