
Abstract
The outlook for patients with psoriasis has improved significantly over the last 10 years with the introduction of targeted therapies. Cytokines exert their effects by activating intracellular signaling and transcription pathways, among which there are Janus kinases (JAKs) and signal transducers and activators of transcription (STAT) pathways. JAKs are intracellular second messengers that are crucial for transmitting extracellular cytokine signals to the cell. JAK inhibition interrupts intracellular signaling and can suppress immune cell activation and inflammation in T-cell-mediated disorders, such as psoriasis. Consequently, JAKs are the subject of intensive research activity, since they represent possible therapeutic targets. Tofacitinib is an orally available compound belonging to a novel category of nonbiologic drugs, the “JAK inhibitors”, which target JAKs. Recently, oral and topical formulations of tofacitinib have been demonstrated to be safe and effective for the treatment of plaque psoriasis in randomized clinical trials. In particular, a 10 mg bid dose of tofacitinib was shown to be noninferior to etanercept 50 mg subcutaneously twice weekly. Questions remain unresolved regarding the safety risk beyond the 5 mg bid dose. This review, assessing the available scientific literature, focuses on the profile of tofacitinib, as investigational compound in the treatment of plaque psoriasis. An overview of the efficacy and safety data from randomized clinical trials is provided. In addition, the authors highlight future potential applications of tofacitinib in other skin diseases, in particular alopecia areata and vitiligo.
Introduction
Psoriasis is a highly heritable common, chronic inflammatory skin disease with a high familial recurrence risk.Citation1 It affects 1%–3% of the world’s population. Chronic plaque psoriasis is the most common form of the disease that is clinically characterized by well-delineated red and scaly plaques.
Psoriasis has a multifactorial origin. The central processes underlying its pathogenesis are inflammation and epidermal hyperproliferation, which are believed to be consequences of a dysregulated interaction of the innate and adaptive immune system in the context of skin epithelium and connective tissue.Citation2 The course of psoriasis in any individual patient is variable and difficult to predict with accuracy.Citation3 In patients with early onset, the disease often follows an irregular course with tendency to become severe and extensive.Citation4 Psoriasis is a major risk factor for the development of psoriatic arthritis, a heterogeneous inflammatory arthritis with a variable clinical course.Citation5 It belongs to the spondyloarthritis group and affects primarily the peripheral joints, the spine, and the entheses. Joint disease is characterized by systemic inflammation and extensive synovitis, resulting in erosions of articular cartilage leading to joint destruction. In patients with psoriasis, associated comorbidities may occur more frequently than expected. Psoriasis is an independent risk factor for cardiovascularCitation6–Citation8 and metabolic syndromes.Citation9,Citation10 The definition of psoriasis severity helps to classify treatment. Moderate-to-severe psoriasis is defined if the body surface involvement is >10% and/or if Psoriasis Area Severity Index (PASI) is >10, although particular clinical situations may change mild psoriasis to moderate-to-severe psoriasis according to involvement of visible areas or marked nail involvement.Citation11
Various conventional and biologic systemic agents may be chosen to treat patients with moderate-to-severe psoriasis. In the last decade, several cellular and molecular mediators in psoriasis have been identified. They included first tumor necrosis factor (TNF)-alpha, then interleukin 12 (IL-12) and IL-23 and more recently IL-17. Such cytokines are pivotal in the disease process. Limiting the interaction of specific cytokines with their specific receptors has been successfully exploited for therapeutic purposes through the development and characterization of monoclonal antibodies or soluble receptors. Consequently, biologic therapies targeting specific immune pathways have emerged for the treatment of moderate-to-severe plaque psoriasis.Citation12 Despite the availability of a broad spectrum of treatments, additional therapeutic options with distinctive mechanism of action may be advantageous for the management of the disease.Citation13,Citation14 Indeed, the overall efficacy of TNF-alpha inhibitors diminishes with time.Citation15–Citation17 The body mass index affects the long-term survival rate of TNF-alpha blockers in psoriatic patients.Citation18 Loss of efficacy can also occur over time with the use of biologics due to their potential immunogenicity.Citation19 Otherwise the injection schedule of treatment has been cited by patients as reasons contributing to treatment discontinuation.Citation20
Recently, attention has been addressed to new compounds, namely small molecular weight inhibitors. Such molecules target intracellular signaling pathways. Small molecular weight inhibitors have some interesting features in that, as synthetic compounds, they are relatively inexpensive to produce and can be administered orally.Citation21
The purpose of this review is to present updated data available on the pharmacology, efficacy, safety, and tolerability of tofacitinib, an orally available compound belonging to a novel class of drugs, the Janus kinase (JAK) inhibitors, in the treatment of plaque psoriasis. After introducing the mechanism of action, an overview of the efficacy and safety results from the randomized clinical trials of tofacitinib in patients affected by plaque psoriasis is presented. Further, future research directions in other skin diseases are highlighted.
Protein kinase family and Janus family of tyrosine kinases
Protein kinases are the second largest human protein family. They are involved in protein phosphorylation, a fundamental component of cell signaling. Aberrant kinase activity is linked either directly or indirectly to a consistent number of diseases. Therefore, kinases are viewed as potential drug targets.Citation22
A family of kinases are the JAKs, of which there are four members, JAK1, JAK2, JAK3, and tyrosine kinase 2 (TYK2).Citation23 JAKs are intracellular second messengers that are crucial for transmitting extracellular cytokine signals to the cell. They regulate cellular processes involved in cell growth, differentiation, and transformation through their association with cytokine receptors. The function of JAKs was discovered by the generation of cell lines resistant to the effects of interferons, whose defects could be balanced by expression of different JAKs.Citation24–Citation26 A large number of cytokines activate the JAK/signal transducers and activators of transcription (STAT) pathway.Citation27 JAK1 binds with γ-chain cytokines (IL-6, IL-10, IL-13, IL-22, granulocyte colony-stimulating factor, interferons). JAK3 binds to the common IL-2Rγ chain of the type I cytokine receptor family (IL-2, IL-4, IL-7, IL-9, IL-15, IL-21). All these cytokines are crucial for lymphocyte activation, proliferation, and function. Inhibition of their signaling may thus result in modulation of multiple aspects of the immune response.Citation28–Citation30 JAK2 is associated with hematopoietic growth factor receptors.Citation29 JAK1, JAK2, and TYK2 are expressed ubiquitously in mammals. The expression of JAK3 is limited to hematopoietically derived cells.Citation31 The deficiency or dysfunction of JAK3 correlates with impairment of lymphocyte development and function and leads to severe combined immunodeficiency.Citation32
JAKs are critical for both innate and adaptive immunity. The noticeable upregulation of JAK/STAT pathways in psoriasis and the recognition of multiple key mediators in psoriasis pathogenesis that signal through JAK/STAT pathways led to consider JAK proteins as potential therapeutic targets for psoriasis treatment as well.Citation33
JAK inhibitors and tofacitinib: mechanism of action
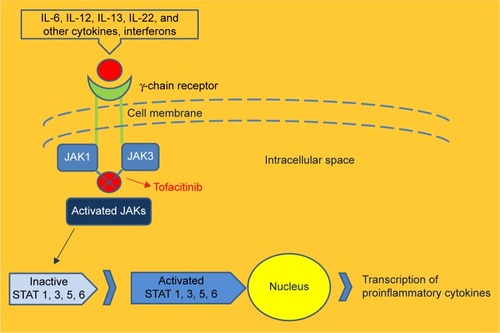
As stated earlier, psoriasis is characterized by activation of several different types of immune cells that infiltrate the skin, stimulating keratinocytes to proliferate and produce proinflammatory cytokines. Effective activation of immune cells needs integration of external stimuli through their surface receptors. The attachment between the receptor and its ligand results in activation of intracellular kinases.Citation34 Such enzymes phosphorylate downstream molecules, propagating a cascade that leads to transcription of genes coding effector molecules. Therefore, JAK inhibition can suppress immune cell activation and inflammation in psoriasis as wellCitation35 ().
Figure 1 Binding of cytokines to the receptor in turn activates an intracellular signaling cascade via JAKs with subsequent phosphorylation of STATs.
Abbreviations: IL, interleukin; JAK, Janus kinase; STAT, signal transducers and activators of transcription.
Tofacitinib, an orally available compound, is the first member of a novel class of medications, the JAK inhibitors. It inhibits phosphorylation of JAK1 and JAK3, IL-6-driven phosphorylation of STAT1 and STAT3, and STAT5.Citation30,Citation36 However, it is currently categorized as a pan-JAK inhibitor preferentially inhibiting JAK1 and JAK3 and, to a lesser extent, JAK2 with minimum effect on TYK2.Citation29,Citation37,Citation38 The primary targets of tofacitinib are dendritic cells, CD4(+) T-cells such as Th1 and Th17, and activated B-cells that lead to multicytokine targeting.Citation39 Tofacitinib is able to inhibit antigen-presentation and T-cell stimulatory capacity of dendritic cells by inhibiting type I interferon-mediated signaling.Citation39 Subsequently, the expression of costimulatory molecules such as CD80 and CD86 is reduced as well.Citation39 Tofacitinib is able to inhibit differentiation and antibody production of B-cells,Citation39 whereas it maintains B-cell regulatory function. Tofacitinib limits the production of IL-17A, IL-17F, and IL-22, the expression of the IL-23R as well as differentiation of Th1 cells.Citation29,Citation36 Since IL-23 is one of the key cytokines that shapes the development and function of Th17 cells, by suppressing the IL-23 receptor expression, the Th17 cell differentiation is consequently reduced.Citation36,Citation39–Citation42
Oral tofacitinib: clinical trials in psoriasis
The efficacy and safety of tofacitinib was investigated in placebo-controlled and head-to-head randomized clinical trials in patients with moderate-to-severe chronic plaque psoriasis.Citation43,Citation44 In two similarly designed Phase III placebo-controlled studies, higher response rates were seen with the 10 mg bid dosage regimen of tofacitinib.Citation43 After 16 weeks, 75% reduction in PASI 75 rates were 39.9% and 59.2%, respectively, for tofacitinib 5 and 10 mg bid (Opt Pivotal 1 study), 46.0%, and 59.6%, respectively, for tofacitinib 5 and 10 mg bid (Opt Pivotal 2 study) ().
Table 1 Results summary for primary outcomes of Phase III published trials of tofacitinib in moderate-to-severe psoriasis
In a head-to-head randomized clinical trial versus etanercept, tofacitinib was noninferior to etanercept only with the 10 mg bid dose.Citation44 The Phase III, double-dummy, placebo-controlled, 12-week trial, comparing two tofacitinib doses with high-dose etanercept or placebo enrolled 1,106 psoriatic patients with a PASI score of 12 or higher and a Physician Global Assessment (PGA) of moderate or severe who had failed to respond to, had a contraindication to, or were intolerant to at least one conventional systemic therapy. Eligible patients were randomly assigned to receive tofacitinib 5 or 10 mg bid, etanercept 50 mg subcutaneously twice weekly or placebo. The co-primary endpoints were the proportion of patients at week 12 with at least a 75% reduction in the PASI 75 response from baseline and the proportion of patients achieving a PGA score of “clear” or “almost clear”. At week 12, PASI 75 responses were recorded in 63.6% of patients in the tofacitinib 10 mg group, compared with 39.5% in the tofacitinib 5 mg group, 58.8% in the etanercept group, and 5.6% in the placebo group. A total of 68.2% of patients treated with tofacitinib 10 mg achieved the other primary endpoint of PGA score of clear or almost clear by week 12, compared with 66.3% of who received etanercept. Patients treated with the lower (5 mg) dose of tofacitinib had an inferior response, since 47.1% achieved clear or almost clear skin, compared with 15% of the placebo group. For both co-primary endpoints, the 10 mg dose of tofacitinib was noninferior to etanercept and superior to placebo, whereas the 5 mg tofacitinib dose did not meet the noninferiority criteria versus etanercept, but met the superiority criteria versus placebo ().Citation44
Another Phase III trial investigated outcomes following tofacitinib withdrawal with outcomes of continuation in patients who had achieved both ≥75% reduction in PASI score from baseline and PGA response. After initial treatment of 24-week duration, 33.5% and 55.2% achieved both PASI 75 and PGA responses with tofacitinib 5 and 10 mg bid, respectively. Following tofacitinib withdrawal, patients who received continuous treatment maintained a response more effectively when compared with placebo recipients. Of those patients who relapsed, up to 60% recaptured a response with tofacitinib.Citation45 Best response rate with oral tofacitinib were seen with the 10 mg bid dose in this study as well.
Safety
By blocking JAK signaling, tofacitinib modulates the immune response via downregulation of several cytokines, including IL-2, IL-4, IL-7, IL-9, IL-15, and IL-21, which are integral to lymphocyte development and function.Citation46 Safety considerations must be considered especially beyond the 5 mg bid dose.Citation43 The risk of tuberculosis and other opportunistic infections may potentially be elevated in tofacitinib-treated patients. Overall tuberculosis cases occurred in patients using the higher dose of 10 mg bid.Citation47 Decrease of hemoglobin, neutrophil, and lymphocyte counts, and increase from baseline in creatinine and alanine aminotransferase may occur, as well as dyslipidemia. Changes of mean serum creatinine levels do not appear to be associated with acute renal failure or progressive worsening of renal function.Citation48 Dyslipidemia is dose-related and affects total cholesterol, high-density lipoprotein cholesterol, and low-density lipoprotein cholesterol. Most of these abnormalities are transient and reversible either spontaneously or with discontinuation of the study drug.Citation43,Citation48
In Phase III clinical trials, the rate of adverse events were similar across the different groups investigatedCitation43,Citation44 and a safety profile similar to that of etanercept was observed in the short-term.Citation44 About infectious events, upper respiratory tract infections, sinusitis, nasopharyngitis, and herpes zoster were reported in patients treated with tofacitinib.Citation43 Information about long-term safety of tofacitinib may be indirectly extrapolated from long-term extension studies and systematic reviews of data of patients with moderate-to-severe active rheumatoid arthritis (RA).Citation48,Citation49 A dose-dependency for serious infections was observed. Rates for safety events were consistent with the published rates for TNF inhibitors and other biologic disease-modifying antirheumatic drugs in similar patient populations for mortality, serious infections, including opportunistic infections and tuberculosis, cardiovascular events, and malignancies.Citation48,Citation49 Since patient population studied was affected by RA, a potential impact of similarities and differences in the disease state, comorbidities, and treatment paradigms must be taken into account.
Interactions
Nonrenal elimination accounts for 70% of the total clearance of tofacitinib. The metabolism is primarily mediated by cytochrome P450 3A4 (CYP3A4) (53%) with minor contribution by CYP450 2C19 (CYP2C19) (17%). Therefore, potent inhibitors or inducers of CYP3A4 and CYP2C19 may potentially interact with tofacitinib. Indeed, potent inducers of CYP3A4, such as rifampin, may reduce the clinical efficacy of tofacitinib. Conversely, it is recommended that the dose of tofacitinib should not exceed 5 mg bid in patients who are receiving concomitant potent inhibitors of CYP3A4, such as ketoconazole, or CYP2C19, such as fluconazole.Citation50 A study by Gupta et alCitation51 did not confirm an inhibitive or inductive effect of tofacitinib on CYP3A4 activity in humans and, in conjunction with in vitro data, supported the conclusion that tofacitinib is unlikely to influence the CYP enzyme system as a whole.
Topical tofaticinib
Two randomized studies investigated the safety and efficacy of a topical solution of tofacitinib in patients with chronic plaque psoriasis.Citation52,Citation53 The first one, a Phase IIa study, met its primary endpoint of efficacy for one of the two ointments containing tofacitinib versus vehicle.Citation52 The second one, an intrasubject, left-right, controlled study, enrolled patients who were randomized to 2%, 0.2%, or 0.02% tofacitinib or vehicle solution once or twice daily.Citation53 Patients treated one plaque as per their randomization group and used vehicle to treat the contralateral plaque for 4 weeks. The primary efficacy endpoint, consisting of intrasubject, vehicle-adjusted mean percent change from baseline in Target Plaque Severity Score at week 4, was not substantially different from baseline for any treatment group. However, skin biopsy analyses detected tofacitinib in both tofacitinib- and vehicle-treated plaques of some patients, suggesting cross-contamination or solution misapplication. Thus, the authors hypothesized that lack of efficacy with tofacitinib relative to vehicle may be due to the intrasubject study design with unsupervised applications.Citation53
Tofacitinib in other diseases: future directions
Tofacitinib demonstrated superior efficacy to methotrexate and similar efficacy to adalimumab in RA.Citation54,Citation55 It gained approval from Food and Drug Administration and regulatory agencies of more than 20 countries,Citation56 becoming the first oral JAK inhibitor indicated for treatment of moderate-to-severe RA. In contrast, the European Medicine Agency adopted a negative opinion, recommending the refusal of the marketing authorization due to major concerns about the overall safety profile.
Interestingly, anecdotal clinical experiences suggest a potential effectiveness of tofacitinib in other dermatologic diseases. In particular, tofacitinib has shown success in treating alopecia areata and vitiligo.Citation57,Citation58 The immune path ways required for autoreactive T-cell activation in alopecia areata are not clearly defined, but the disease is driven by cytotoxic CD8+NKG2D+ T lymphocytes and reversed by JAK inhibition.Citation59 The inhibition of JAK/STAT signaling promotes hair growth by stimulating the activation and/or proliferation of hair follicle stem cells.Citation60 About vitiligo, interferon (IFN)-γ-chemokine axis is active in human disease. In particular, a critical role for the IFN-γ-induced chemokine CXCL10 in both the progression and maintenance of vitiligo has been suggested.Citation61 When IFN-γ binds to its receptor, it activates the JAK/STAT pathway, which in turn leads to production of CXCL10 in keratinocytes.Citation58 Therefore, a direct CXCL10 inhibition or a JAK/STAT pathway inhibition may represent attractive targets for new treatments strategies.
Recently, tofacitinib citrate was given to six consecutive patients with moderate-to-severe atopic dermatitis (AD) who had who failed to gain results with standard treatment.Citation62 Response to treatment was assessed using the scoring of AD index. Decreased body surface area involvement of dermatitis and decreased erythema, edema/papulation, lichenification, and excoriation were observed in all patients. The scoring of AD index decreased by 66.6% from 36.5 to 12.2 (P<0.05) during 8–29 weeks of treatment. No adverse events were observed.
Conclusion
Increased knowledge of the molecular regulatory mechanisms that impact the pathogenesis of psoriasis and other inflammatory diseases has created new chances for the development of targeted drug therapy. The antipsoriatic therapeutic spectrum could be extended in the future to a number of novel oral compounds, the JAK inhibitors. JAKs are intracellular second messengers that are essential for transmitting extracellular cytokine signals to the cell. JAK inhibition can suppress immune cell activation and inflammation. Tofacitinib is a current investigational drug in psoriasis. It is an orally available compound belonging to the group of JAK inhibitors. Oral and topical formulations of tofacitinib have been demonstrated to be safe and effective for the treatment of plaque psoriasis in Phase III clinical trials. If approved for psoriasis treatment by regulatory agencies, it will be interesting to define its place in the treatment algorithm. The available randomized clinical trials in psoriasis place tofacitinib in the same area of etanercept, as second-line agent alongside the TNF-alpha antagonists. The oral delivery route, and economic issues regarding potential better cost-effectiveness ratio with respect to biologics and biosimilars, may be tofacitinib strengths. Given the oral administration route, efficacy and safety of tofacitinib could be compared to available conventional antipsoriatic treatments, such as methotrexate or cyclosporine, in randomized clinical trials. Such studies could provide additional information about potential treatment strategies. About safety, questions remain unresolved. The Food and Drug Administration approved only the 5 mg bid dose in RA on the grounds that a higher dose was not considered to have an adequate risk-to-benefit ratio. Nevertheless investigational studies in psoriasis showed that 5 mg bid tofacitinib was less effective than etanercept.
Definitely, current studies show no substantial advantages of tofacitinib in terms of efficacy and safety over existing treatments for psoriasis. A Phase III study assessed its noninferiority (rather than superiority) at the higher dose to etanercept. In consideration of the plethora of emerging antipsoriatic drugs recently approved such as secukinumab or apremilast, or in the pipeline, such as anti-IL-23 antibodies, it seems desirable to further explore tofacitinib for promoting hair growth and/or repigmentation. Both alopecia areata and vitiligo are common diseases with big unmet medical needs. Clinical trials with selective JAK inhibitors are required to dissect key pathogenic pathways.
Disclosure
The authors report no conflicts of interest in this work.
References
- Di LerniaVFicarelliELallasARicciCFamilial aggregation of moderate to severe plaque psoriasisClin Exp Dermatol20143980180525156221
- BoehnckeWHEtiology and pathogenesis of psoriasisRheum Dis Clin North Am20154166567526476225
- Di LerniaVFicarelliECurrent therapeutic approaches of psoriasis are affected by age at disease onsetJ Dermatolog Treat201425151723210896
- HenselerTChristophersEPsoriasis of early and late onset: characterization of two types of psoriasis vulgarisJ Am Acad Dermatol1985134504564056119
- GladmanDDAntoniCMeasePCleggDONashPPsoriatic arthritis: epidemiology, clinical features, course, and outcomeAnn Rheum Dis200564Suppl 2ii14ii1715708927
- GelfandJMNeimannALShinDBWangXMargolisDJTroxelABRisk of myocardial infarction in patients with psoriasisJAMA2006112961735174117032986
- GisondiPDalle VedoveCGirolomoniGPatients with psoriasis have a higher prevalence of parental cardiovascular diseaseDermatology201122233033521701147
- GisondiPTargherGBardazziFPharmacological treatment of moderate-severe psoriasis in patients with cardio-metabolic comorbiditiesG Ital Dermatol Venereol2014149Suppl 2711
- GisondiPTessariGContiAPrevalence of metabolic syndrome in patients with psoriasis: a hospital-based case-control studyBr J Dermatol2007157687317553036
- RyanCKirbyBPsoriasis is a systemic disease with multiple cardiovascular and metabolic comorbiditiesDermatol Clin201533415525412782
- MrowietzUKragballeKReichKDefinition of treatment goals for moderate to severe psoriasis: a European consensusArch Dermatol Res201130311020857129
- GirolomoniGAltomareGAyalaFDifferential management of mild-to-severe psoriasis with biologic drugs: an Italian Delphi consensus expert panelJ Dermatolog Treat20152612813324708158
- WegerWCurrent status and new developments in the treatment of psoriasis and psoriatic arthritis with biological agentsBr J Pharmacol201016081082020590580
- DuboisDSPouliotRPromising new treatments for psoriasisScientific World J20132013980419
- GniadeckiRKragballeKDamTNSkovLComparison of drug survival rates for adalimumab, etanercept and infliximab in patients with psoriasis vulgarisBr J Dermatol20111641091109621219290
- YeungHWanJVan VoorheesASPatient-reported reasons for the discontinuation of commonly used treatments for moderate to severe psoriasisJ Am Acad Dermatol201368647222846688
- Di LerniaVRicciCLallasAFicarelliEClinical predictors of non-response to any tumor necrosis factor (TNF) blockers: a retrospective studyJ Dermatolog Treat201425737423621374
- Di LerniaVTasinLPellicanoRImpact of body mass index on retention rates of anti-TNF-alfa drugs in daily practice for psoriasisJ Dermatolog Treat20122340440921781016
- De SimoneCAmerioPAmorusoGImmunogenicity of anti-TNFα therapy in psoriasis: a clinical issue?Expert Opin Biol Ther2013131673168224107126
- ArmstrongAWRobertsonADWuJSchuppCLebwohlMGUndertreatment, treatment trends, and treatment dissatisfaction among patients with psoriasis and psoriatic arthritis in the United States: findings from the national psoriasis foundation surveys, 2003–2011JAMA Dermatol20131491180118523945732
- MansouriYGoldenbergGNew systemic therapies for psoriasisCutis20159515516025844781
- PattersonHNibbsRMcInnesISiebertSProtein kinase inhibitors in the treatment of inflammatory and autoimmune diseasesClin Exp Immunol201417611024313320
- MurrayPJThe JAK-STAT signaling pathway: input and output integrationJ Immunol20071782623262917312100
- VelazquezLFellousMStarkGRPellegriniSA protein tyrosine kinase in the interferon α/β signaling pathwayCell1992703133221386289
- MullerMBriscoeJLaxtonCThe protein tyrosine kinase JAK1 complements defects in interferon-alpha/beta and -gamma signal transductionNature19933661291358232552
- DarnellJEJrKerrIMStarkGRJak–STAT pathways and transcriptional activation in response to IFNs and other extracellular signalling proteinsScience1994264141514218197455
- O’SheaJJGadinaMSchreiberRDCytokine signaling in 2002: new surprises in the Jak/Stat pathwayCell2002109121131
- LeonardWJO’SheaJJJaks and STATs: biological implicationsAnnu Rev Immunol1998162933229597132
- LindstromTMRobinsonWHA multitude of kinases – which are the best targets in treating rheumatoid arthritis?Rheum Dis Clin North Am20103636738320510239
- GhoreschiKGadinaMJAKpot! New small molecules in autoimmune and inflammatoryExp Dermatol20142371124131352
- BorieDCO’SheaJJChangelianPSJAK3 inhibition, a viable new modality of immunosuppression for solid organ transplantsTrends Mol Med20041053254115519279
- MacchiPVillaAGilianiSMutations of Jak-3 gene in patients with autosomal severe combined immune deficiency (SCID)Nature199537765687659163
- ChiricozziAFaleriSSaracenoRTofacitinib for the treatment of moderate-to-severe psoriasisExpert Rev Clin Immunol20151144345525666451
- KyttarisVCKinase inhibitors: a new class of antirheumatic drugsDrug Des Devel Ther20126245250
- ChangBYZhaoFHeXJAK3 inhibition significantly attenuates psoriasiform skin inflammation in CD18 mutant PL/J miceJ Immunol20091832183219219596999
- GhoreschiKJessonMILiXModulation of innate and adaptive immune responses by tofacitinib (CP-690, 550)J Immunol20111864234424321383241
- FridmanJSScherlePACollinsRSelective inhibition of JAK1 and JAK2 is efficacious in rodent models of arthritis: preclinical characterization of INCB028050J Immunol20101845298530720363976
- BoyMGWangCWilkinsonBEDouble-blind, placebo-controlled, dose-escalation study to evaluate the pharmacologic effect of CP-690,550 in patients with psoriasisJ Invest Dermatol20091292299230219225543
- KuboSYamaokaKKondoMThe JAK inhibitor, tofacitinib, reduces the T cell stimulatory capacity of human monocyte-derived dendritic cellsAnn Rheum Dis2014732192219824013646
- GhoreschiKLaurenceAO’SheaJJJanus kinases in immune cell signallingImmunol Rev200922827328719290934
- HsuLArmstrongAWJAK inhibitors: treatment efficacy and safety profile in patients with psoriasisJ Immunol Res2014201428361724883332
- PesuMLaurenceAKishoreNZwillichSHChanGO’SheaJJTherapeutic targeting of Janus kinasesImmunol Rev200822313214218613833
- PappKAMenterMAAbeMTofacitinib, an oral Janus kinase inhibitor, for the treatment of chronic plaque psoriasis: results from two randomized, placebo-controlled, phase III trialsBr J Dermatol201517394996126149717
- BachelezHvan de KerkhofPCStrohalRTofacitinib versus etanercept or placebo in moderate-to-severe chronic plaque psoriasis: a phase 3 randomised non-inferiority trialLancet201538655256126051365
- BissonnetteRIversenLSofenHTofacitinib withdrawal and retreatment in moderate-to-severe chronic plaque psoriasis: a randomized controlled trialBr J Dermatol20151721395140625418186
- MeyerDMJessonMILiXAnti-inflammatory activity and neutrophil reductions mediated by the JAK1/JAK3 inhibitor, CP-690,550, in rat adjuvant-induced arthritisJ Inflamm (Lond)201074120701804
- WinthropKLParkSHGulATuberculosis and other opportunistic infections in tofacitinib-treated patients with rheumatoid arthritisAnn Rheum Dis Epub201582810.1136/annrheumdis-2015-207319
- WollenhauptJSilverfieldJLeeEBSafety and efficacy of tofacitinib, an oral janus kinase inhibitor, for the treatment of rheumatoid arthritis in open-label, long term extension studiesJ Rheumatol20144183785224692527
- StrandVAhadiehSFrenchJSystematic review and meta-analysis of serious infections with tofacitinib and biologic disease-modifying antirheumatic drug treatment in rheumatoid arthritis clinical trialsArthritis Res Ther20151736226669566
- XELJANZ® (tofacitinib) tablets [prescribing information]New YorkPfizer Labs2012 Available from:http://www.accessdata.fda.gov/drugsatfda_docs/label/2012/203214s000lbl.pdfAccessed 19 January, 2016
- GuptaPAlveyCWangRLack of effect of tofacitinib (CP-690,550) on the pharmacokinetics of the CYP3A4 substrate midazolam in healthy volunteers: confirmation of in vitro dataBr J Clin Pharmacol20127410911522233204
- PortsWCKhanSLanSA randomized phase 2a efficacy and safety trial of the topical Janus kinase inhibitor tofacitinib in the treatment of chronic plaque psoriasisBr J Dermatol201316913714523387374
- PortsWCFeldmanSRGuptaPRandomized pilot clinical trial of tofacitinib solution for plaque psoriasis: challenges of the intra-subject study designJ Drugs Dermatol20151477778426267721
- LeeEBFleischmannRHallSTofacitinib versus methotrexate in rheumatoid arthritisN Engl J Med20143702377238624941177
- van VollenhovenRFFleischmannRCohenSTofacitinib or adalimumab versus placebo in rheumatoid arthritisN Engl J Med201236750851922873531
- VivarNVan VollenhovenRFAdvances in the treatment of rheumatoid arthritisF1000Prime Rep201463124860653
- BrittanyGCraiglowKingBAKilling two birds with one stone: oral tofacitinib reverses alopecia universalis in a patient with plaque psoriasisJ Invest Dermatol20141342988299024940651
- CraiglowBGKingBATofacitinib citrate for the treatment of vitiligo: a pathogenesis-directed therapyJAMA Dermatol20151511110111226107994
- XingLDaiZJabbariAAlopecia areata is driven by cytotoxic T lymphocytes and is reversed by JAK inhibitionNat Med2014201043104925129481
- HarelSHigginsCACeriseJEPharmacologic inhibition of JAK-STAT signaling promotes hair growthSci Adv2015231e150097326601320
- RashighiMAgarwalPRichmondJMCXCL10 is critical for the progression and maintenance of depigmentation in a mouse model of vitiligoSci Transl Med20146223
- LevyLLUrbanJKingBATreatment of recalcitrant atopic dermatitis with the oral Janus kinase inhibitor tofacitinib citrateJ Am Acad Dermatol20157339539926194706