
Abstract
Objective
Eldecalcitol (ELD) is an active form of vitamin D analog that has been approved for the treatment of osteoporosis in Japan. Over recent years, a number of multicenter, randomized controlled clinical trials have been conducted. Our goal is to comprehensively summarize the results from these studies.
Methods
We searched the databases MEDLINE, EMBASE, and Cochrane Central Register of Controlled Trials up to February 28, 2015. Each database was searched using search terms “Eldecalcitol” and “ED-71” and the results were combined. The retrieved data from three independent clinical trials included a total of 1,332 patients with osteoporosis. After the data were pooled from three trials, RevMan software was used to conduct meta-analyses to determine the effects of ELD on bone mineral density (BMD) and bone turnover marker (BTM) type I collagen amino-terminal telopeptide (NTX). Effects of ELD on some of the bone formation and bone resorption parameters, incidence of vertebral fractures at the lower spine, and health-related quality of life (HRQOL) in patients with osteoporosis were also summarized.
Results
With a test for overall effectZ=6.35, ELD could increase lumbar BMD (P<0.00001). In comparison with alphacalcidol, ELD suppressed the NTX level to a greater degree (test for overall effectZ=3.82,P<0.0001). ELD was also found to suppress bone alkaline phosphatase (BALP) by 19% (P<0.01) and osteocalcin by 19% (P<0.01) at the dose of 0.75 μg/day. Compared to alfacalcidol, ELD showed higher potency in suppressing serum BALP (26±9 vs 32±11 U/L,P<0.05) and amino-terminal propeptide of procollagen I (PINP) (42±15 vs 59±23 ng/mL,P<0.05). In addition, ELD was found to be more effective in reducing the incidence of vertebral fractures at the lower spine (P=0.029).
Conclusion
Our meta-analysis showed that ELD was more potent than alphacalcidol in reducing BTM (NTX). Clinical data together suggest that ELD is efficient in treating osteoporosis by increasing lumbar BMD; suppressing BTMs, including NTX, BALP, osteocalcin, and PINP; resulting in the reduction in the incidence of vertebral fractures at the lower spine; and increasing the HRQOL in patients with osteoporosis.
Introduction
Osteoporosis is a progressive systemic skeletal disease characterized by low bone mass and micro-architectural deterioration of bone tissue, with a consequent increase in bone fragility and susceptibility to fracture.Citation1 Changes in bone turnover with aging are responsible for bone loss and play a major role in osteoporosis. An imbalance in bone turnover impacts on bone strength as a result of reductions in bone volume and mineralization, loss of trabeculae, deterioration of trabecular connectivity, and the formation of resorption cavities and trabecular perforations. Therefore, an increase in bone turnover where resorption exceeds formation is not only inversely correlated with bone mineral density (BMD), but may also alter bone architecture and porosity, increasing the risk of fracture beyond that due to reduced BMD, and can therefore be an independent predictor of fracture risk.Citation2–Citation5
Bone density scanning using dual-energy X-ray absorpiometry is currently the most commonly used means of measuring BMD. It is typically used to diagnose and follow osteoporosis. The World Health Organization (WHO) has established criteria for making the diagnosis of osteoporosis, as well as determining levels that predict higher chances of fractures. These criteria are based on comparison of the BMD of the patient to that of a typical healthy, young female. BMD values that fall 2.5 standard deviations below the average for the healthy, young female’s BMD are diagnosed as osteoporotic. BMD values less than the healthy, young female, but not 2.5 standard deviations below the average are referred to as osteopenic. In addition to serial BMD measurements, biochemical markers of bone turnover are also widely used to monitor treatment response, since they are noninvasive and relatively cheap compared with dual-energy X-ray absorptiometry.
Formation markers are products from the action of osteoblasts. These include bone-specific alkaline phosphatase (BALP), procollagen type 1 amino-terminal propeptide (PINP), osteocalcin (or bone GLA-protein), and procollagen type 1 carboxy-terminal propeptide (P1CP). Resorption markers are products from the action of osteoclasts. These include carboxy-terminal telopeptide cross-linked type 1 collagen (CTX), type I collagen amino-terminal telopeptide (NTX), and urine deoxypyridinoline.
Vitamin D metabolism plays a critical role in the regulation of mineral and bone homeostasis.Citation6 The active form of vitamin D, 1α,25-dihydroxyvitamin D3 (1α,25-(OH)2D3), acts through the vitamin D receptor (VDR) present on target cells such as osteoblasts and osteoclastsCitation7,Citation8 to stimulate calcium absorption and reabsorption while blocking both the synthesis and secretion of another essential regulator of mineral balance, the parathyroid hormone (PTH).Citation9 At least two mechanisms are involved in vitamin D-mediated regulation of mineral and bone homeostasis: first, it binds to the VDR on osteoblastic cells and regulates osteoclastic activity via the osteoprotegerin (OPG)/receptor activator nuclear factor kB (RANK) system;Citation10 second, it secures a supersaturated state of calcium–phosphorus products in the blood, enabling osteoid mineralization.Citation11 Due to its calcemic activity and its potential role in promoting osteoclastic bone resorption, the use of vitamin D in the treatment of osteoporosis has been hindered.Citation12–Citation14 However, much effort has been made to synthesize compounds that would retain only the differentiation and antiproliferative effects of 1α,25-(OH)2D3 and allow for safer usage and less side effects.Citation15,Citation16 In fact, the active form of vitamin D (1α,25-dihydroxyvitamin D3, calcitriol) and its prodrug (1α-hydroxyvitamin D3, alfacalcidol) have been approved for the treatment of osteoporosis in Japan.Citation17 Both calcitriol and alfacalcidol have been shown to increase BMDCitation18,Citation19 and reduce the risk of vertebral and nonvertebral fractures.Citation20 –Citation22 Eldecalcitol (ELD), formerly known as ED-71 that was developed in the early 1980s, is an analog of 1α,25-(OH)2D3 bearing a hydroxypropyloxy residue at the 2β position. In a rat ovariectomized model of osteoporosis, ELD has been demonstrated to lower biochemical and histological parameters of bone resorption.Citation23 Further study showed that these effects on bone were observed without sustained hypercalcemia or hypercalciuria.Citation24 ELD has also been approved as a drug for treatment of osteoporosis in Japan. In the recent years, a few clinical trials have been conducted to examine the efficacy of ELD in treating osteoporosis. This study was aimed to summarize the results of these clinical trials and evaluating the clinical effects of ELD on lumbar and hip BMD, and bone turnover markers (BTMs) in patients with osteoporosis.
Methods
Literature search and study selection
Databases MEDLINE, EMBASE, and the Cochrane Central Register of Controlled Trials were searched till February 18, 2015 to identify all potential clinical trials using ELD for the treatment of osteoporosis. We performed the literature search using the following search term: (eldecalcitol OR ED-71). After excluding review articles, basic studies, animal studies, pharmacokinetic studies, articles in languages other than English, and conference abstracts, we identified a total of eleven clinical studies investigating the efficacy of ELD in treatment of osteoporosis. If the same study had been published in different articles, we selected the most recent publication or the publication covering most detailed information. Literature search was repeated using the same databases and search terms during the revision of this article and no new study was found.
Data extraction and quality assessment
For the meta-analysis study, we chose lumber BMD, hip BMD, and BTM NTX as the outcome measures. Data on severe vertebral fractures, BTMs BALP, osteocalcin, NTX, and serum PINP were also extracted for summary and discussion. Original data collection forms were used to abstract the following information from single studies: sample size, dose, and changes from base line. Two reviewers screened articles independently, and disagreements were resolved through discussion. The Cochrane Collaboration’s tool was used to assess risk of bias.
Evaluation of heterogeneity and statistics
RevMan software, version 5.3, was used for the calculation of heterogeneity parameter, quantitative meta-analyses, and generation of forest plots. TheI2 value was calculated to determine the degree of heterogeneity. AnI2 value from 50% to 75% represented moderate heterogeneity, and anI2 value above 75% was defined as high heterogeneity. In the presence of high heterogeneity, the random effect model was implemented. Risk ratios and their 95% confidence intervals (CIs) were calculated.
Results
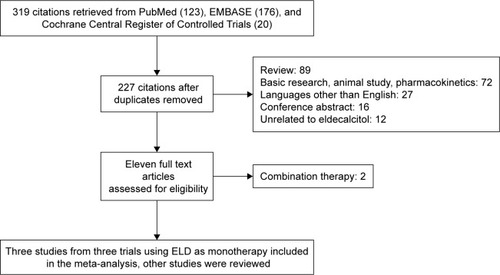
We identified 123 entries in MEDLINE, 176 entries in EMBASE, and 20 entries in Cochrane Central Register of Controlled Trials. As is shown in, a total of eleven studies were identified and analyzed. Among these studies, nine came from three independent trials using ELD as mono-therapy, involving 1,332 patients who were given placebo (n=53), alfacalcidol (n=546), or ELD (n=734). The first trial published in 2005 tested the effects of different doses of ELD on lumbar BMD, total hip BMD, and BTMs, including BALP, osteocalcin, NTX, BALP, and PINP.Citation24 The second trial published in 2010 compared between alfacalcidol and ELD the effects on BTMs BALP and NTX.Citation25 The third trial also compared the effects of alfacalcidol and ELD and the results were reported in multiple articles. In the report published in 2011, the effects of alfacalcidol and ELD on lumbar BMD and hip BMD were reported.Citation26 In the report published in 2012, their effects on NTX, BALP, and PINP were revealed.Citation27 The main features and their quantitative data synthesis are summarized in. Not all studies were included in, since some of them basically analyzed the same data from different angles.
Table 1 Basic characteristics and results of clinical trials
Figure 1 Flow diagram for study selection.
The risk of bias assessment for these trials is presented in. Trials 1, 2, and 3 were found to be at moderate, high, and low risk of bias, respectively. The common problem for all the three trails was inadequate description of the randomization method and the overall risk of bias for all the trials was rated as moderate. The other two trials used ELD as a component in combination therapies. Results from these trials were excluded from our meta-analysis.
Table 2 Assessment of risk of bias by The Cochrane Collaboration’s tool
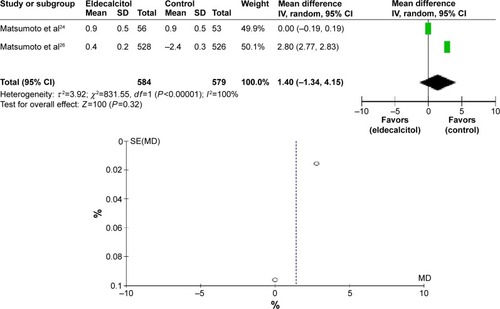
Among all parameters reported, only lumbar BMD, hip BMD, and NTX were examined in at least two independent trials. In the second trial, ELD increased the lumber and hip BMD by 3.1±0.7 and 0.9±0.5, respectively.Citation24 In the third trial, alfacalcidol increased the lumbar BMD by 0.2±0.4 but decreased hip BMD by 2.4±0.3, and ELD increased the lumber and hip BMD by 3.5±0.2 and 0.4±0.2, respectively.Citation26 Our meta-analyses found that at dose not less than 0.75 μg/day, ELD was able to significantly increase lumbar BMD with test for overall effectZ=6.35 (P<0.00001) (HTP<0.00001,τ2 =0.40,χ2 =58.5,df=1,I2=98%) (). Edecalcitol did not seem to increase total hip BMD though, with test for overall effectZ=1.00 (P=0.32) (Heterogeneity [HT]P<0.00001,τ2 =3.92,χ2 =831.55,df=1,I2=100%) ().
Figure 2 Eldecalcitol increases lumbar BMD, as compared with placebo.
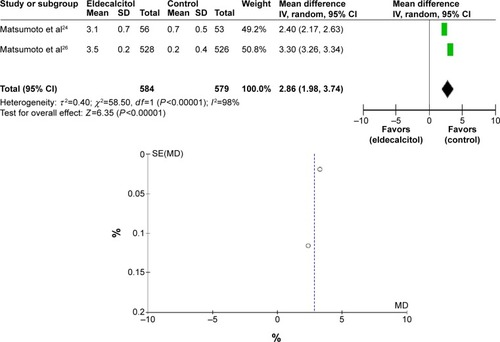
Figure 3 Eldecalcitol has no effect on hip BMD, as compared to placebo.
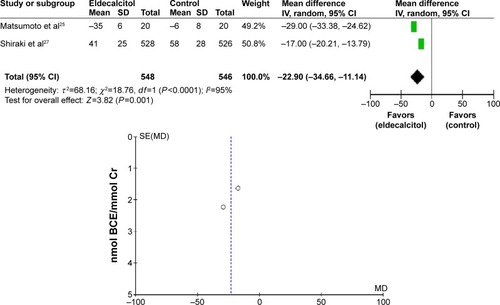
All the three trials examined the effects of ELD on BTM NTX. In the first trial involving 219 osteoporotic patients, 1 μg/day of edecalcitol decreased urinary NTX from the baseline with a median percentage of 19% (P<0.01).Citation24 In the second trial involving 59 Japanese postmenopausal women, suppression of urinary NTX was much stronger in both 0.5 and 1 μg ELD-treated groups than in 1 μg alfacalcidol-treated subjects, with urinary NTX decreasing by 6%, 30%, and 35% from the baseline, respectively.Citation25 In the third trial involving 1,054 patients, ELD-treated group (0.75 μg/day) was found to have lower urinary NTX than alfacalcidol-treated group (1 μg/day) (41±25 nmol vs 58±28 nmol,P<0.05).Citation27 Since the effects of NTX were reported as medians of changes from the baseline in the first trial, the second and third trials reported only the means of NTX. Therefore, we carried out the meta-analysis for NTX using data only from the second and third trials, and the result, with test for overall effectZ=3.82 (P=0.0001) (HTP<0.0001,τ2 =68.16,χ2 =18.76,df=1,I2=95%), suggested that ELD suppressed NTX to a greater degree when compared to alfacalcidol ().
Figure 4 Eldecalcitol suppressed NTX to a greater degree in comparison with alfacalcidol.
In addition to NTX, some other BTMs were also investigated in these studies. In the first trial, ELD was found to suppress BALP with median percentages of 24% (P<0.01), 19% (P<0.01), and 23% (P<0.01) and osteocalcin with median percentages of 30% (P<0.01), 19% (P<0.01), and 22% (P<0.01). In the third trial, 0.75 μg/day of edecalcitol was found to do better than 1 μg/day of alfacalcidol in lowering serum BALP (26±9 vs 32±11 U/L,P<0.05) and PINP (42±15 vs 59±23 ng/mL,P<0.05).Citation27
The third trial also compared the efficacy of 0.75 μg/day of edecalcitol and 1 μg/day of alfacalcidol in preventing osteoporotic fractures.Citation28 Their post hoc analyses found that ELD treatment reduced the incidence of osteoporotic fractures defined by the WHO Technical Report more than alfacalcidol treatment (18.6% vs 25.2%; hazard ratio [HR], 0.70; 95% CI, 0.54–0.93). ELD also decreased the incidence of major osteoporotic fractures defined in the WHO Fracture Risk Assessment Tool (FRAX) more than alfacalcidol (11.1% vs 16.3%; HR, 0.66; 95 % CI, 0.46–0.94).
The third trial further evaluated the effects of ELD on the spinal location of incident vertebral fractures, the severity of the fractures, and the changes in health-related quality of life (HRQOL) in comparison to those of alfacalcidol.Citation29 The incidence of vertebral fractures was evaluated based on the location on the spine (upper T4–T10; lower T11–L4). The severity of vertebral fractures was determined by using a semi-quantitative method, and the change in HRQOL was analyzed by using the Medical Outcomes Study Short-Form 36-Item questionnaire. The data showed that the incidence of vertebral fracture at the lower spine was less in the ELD group than in the alfacalcidol group (P=0.029), and the incidence of severe vertebral fracture (grade 3) was less in the ELD group than the alfacalcidol group (3.8% vs 6.7%,P=0.036). The data also revealed that both ELD and alfacalcidol improved HRQOL in osteoporotic patients. Although no significant differences in each HRQOL scores were observed between ELD and alfacalcidol during the observational period, overall improvement from baseline of HRQOL scores was clearly observed in the ELD group. In summary, compared to alfacalcidol, ELD could further reduce the incidences of lower spinal vertebral fractures and severe vertebral fractures. Furthermore, daily treatment with ELD was effective in improving HRQOL.
Conclusion and discussion
Vitamin D has long been regarded as a fundamental part of the prevention and treatment of osteoporosis. However, findings from observational studies showed inconsistent associations between BMD and vitamin D status.Citation30,Citation31 In fact, result from a recent meta-analysis of trials of vitamin D alone failed to show an association between supplementation and BMD.Citation32 In addition, results from meta-analyses of trials of vitamin D alone failed to show an association between supplementation and fracture prevention.Citation33,Citation34 Nevertheless, the active form of vitamin D, calcitriol, and its prodrug, alfacalcidol, have shown activities to increase BMD and reduce the risk of vertebral and nonvertebral fractures, and have been approved for the treatment of osteoporosis in Japan. Our current meta-analysis revealed that ELD was superior to alfacalcidol in suppressing NTX level. In fact, as was found in a recent clinical trial, alfacalcidol increased the lumbar BMD but decreased hip BMD, whereas ELD increased both the lumber and hip BMDs.Citation26 Our review of data from multiple clinical trials also showed that ELD performed better than alfacacidol in reducing incidence of severe vertebral fractures and suppressing BTMs, including serum BALP and PINP. Put together, current data have provided strong support to the notion that active vitamin D analogs could be tailored in ways to improve their beneficial effects while limiting the unwanted activities for treatment of diseases such as osteoporosis.
Other widely used drugs for osteoporosis include bisphosphonates, calcitonin, estrogen hormone, estrogen agonist/antagonist, PTH, and RANK ligand (RANKL)/RANKL inhibitor. Given the fact that the active analogs of vitamin D exert their pharmacological activities by mechanisms different from those of other current drugs, combination therapy with active vitamin D and other categories can be expected to offer more choices in osteoporosis treatment in the future. In fact, two such clinical trials have been conducted recently. In one trial, the effects of bisphosphonate alone on biochemical markers and muscle power in comparison with those of bisphosphonate combined with ELD were studied in postmenopausal women with osteoporosis. During the 6-month treatment period, while both treatments significantly reduced BTMs serum BALP and urinary NTX to a similar degree, combination therapy improved five-repetition chair-rising time to a significantly greater degree than monotherapy with bisphosphonate.Citation35 In another trial, efficacy of combination of alendronate and ELD was compared to that of combination of alendronate plus vitamin D and calcium in patients with primary osteoporosis. The results showed that alendronate combined with ELD was more effective in reducing the BTMs, including serum type I collagen C-telopeptide (sCTX), urine NTX, tartrate-resistant acid phosphatase 5b (TRACP-5b), BALP, and PINP and increasing the femoral neck BMD compared to alendronate treatment with vitamin D3 and calcium.Citation36 Therefore, ELD has shown promising potential in treatment of osteoporosis when combined with other existing antiosteoporotic drugs, and further exploration of ELD-based combination therapy is warranted.
Due to multiple reasons, our meta-analysis results should be interpreted and translated into clinical practice with caution. First of all, limited number of trials have been completed so far; second, risk of bias may be high in some of these trials; third, all trials have been conducted on Japanese patients, and the applicability of these data to other ethnic groups needs to be investigated; finally, data for some parameters were reported in different format in different trials (eg, interquartile in one study, but means in another study), making them less accurate and less comparable. However, over all clinical data that have been generated so far strongly support ELD as an effective treatment option for osteoporosis. Further clinical studies will surely reveal the full potential of ELD either as monotherapy or combination therapy for osteoporosis.
Disclosure
The authors report no conflicts of interest in this work.
References
- Consensus development conference: diagnosis, prophylaxis, and treatment of osteoporosisAm J Med1993946466508506892
- Funck-BrentanoTBiverEChopinFClinical utility of serum bone turnover markers in postmenopausal osteoporosis therapy monitoring: a systematic reviewSemin Arthritis Rheum20114115716921507464
- KunchurRNeedAHughesTGossAClinical investigation of C-terminal cross-linking telopeptide test in prevention and management of bisphosphonate-associated osteonecrosis of the jawsJ Oral Maxillofac Surg2009671167117319446200
- LewieckiEMBenefits and limitations of bone mineral density and bone turnover markers to monitor patients treated for osteoporosisCurr Osteoporos Rep20108152220425086
- OkamotoKInabaMFurumitsuYBeneficial effect of risedronate on arterial thickening and stiffening with a reciprocal relationship to its effect on bone mass in female osteoporosis patients: a longitudinal studyLife Sci20108768669120951147
- van LeeuwenJPvan DrielMvan den BemdGJPolsHAVitamin D control of osteoblast function and bone extracellular matrix mineralizationCrit Rev Eukaryot Gene Expr20011119922611693961
- LangubMCReinhardtTAHorstRLMallucheHHKoszewskiNJCharacterization of vitamin D receptor immunoreactivity in human bone cellsBone20002738338710962349
- MeeAPHoylandJABraidmanIPFreemontAJDaviesMMawerEBDemonstration of vitamin D receptor transcripts in actively resorbing osteoclasts in bone sectionsBone1996182952998726384
- BrommageRDeLucaHFEvidence that 1,25-dihydroxyvitamin D3 is the physiologically active metabolite of vitamin D3Endocr Rev198564915113000754
- KhoslaSMinireview: the OPG/RANKL/RANK systemEndocrinology20011425050505511713196
- DeLucaHFOverview of general physiologic features and functions of vitamin DAm J Clin Nutr2004801689S1696S15585789
- NishiiYActive vitamin D and its analogs as drugs for the treatment of osteoporosis: advantages and problemsJ Bone Miner Metab200220576511862526
- NishiiYRationale for active vitamin D and analogs in the treatment of osteoporosisJ Cell Biochem20038838138612520540
- NishiiYOkanoTHistory of the development of new vitamin D analogs: studies on 22-oxacalcitriol (OCT) and 2beta-(3-hydroxypropoxy) calcitriol (ED-71)Steroids20016613714611179721
- BouillonROkamuraWHNormanAWStructure-function relationships in the vitamin D endocrine systemEndocr Rev1995162002577781594
- OkudaNTakedaSShinomiyaKED-71, a novel vitamin D analog, promotes bone formation and angiogenesis and inhibits bone resorption after bone marrow ablationBone20074028129217049330
- OrimoHNakamuraTHosoiTJapanese 2011 guidelines for prevention and treatment of osteoporosis – executive summaryArch Osteoporos2012732023203733
- GallagherJCFowlerSEDetterJRShermanSSCombination treatment with estrogen and calcitriol in the prevention of age-related bone lossJ Clin Endocrinol Metab2001863618362811502787
- ShikariMKushidaKYamazakiKNagaiTInoueTOrimoHEffects of 2 years’ treatment of osteoporosis with 1 alpha-hydroxy vitamin D3 on bone mineral density and incidence of fracture: a placebo-controlled, double-blind prospective studyEndocr J1996432112209026268
- O’DonnellSMoherDThomasKHanleyDACranneyASystematic review of the benefits and harms of calcitriol and alfacalcidol for fractures and fallsJ Bone Miner Metab20082653154218979152
- PapadimitropoulosEWellsGSheaBMeta-analyses of therapies for postmenopausal osteoporosis. VIII: meta-analysis of the efficacy of vitamin D treatment in preventing osteoporosis in postmenopausal womenEndocr Rev20022356056912202471
- RingeJDSchachtEPotential of alfacalcidol for reducing increased risk of falls and fracturesRheumatol Int2009291177118519159932
- UchiyamaYHiguchiYTakedaSED-71, a vitamin D analog, is a more potent inhibitor of bone resorption than alfacalcidol in an estrogen-deficient rat model of osteoporosisBone20023058258811934649
- MatsumotoTMikiTHaginoHA new active vitamin D, ED-71, increases bone mass in osteoporotic patients under vitamin D supplementation: a randomized, double-blind, placebo-controlled clinical trialJ Clin Endocrinol Metab2005905031503615972580
- MatsumotoTTakanoTYamakidoSTakahashiFTsujiNComparison of the effects of eldecalcitol and alfacalcidol on bone and calcium metabolismJ Steroid Biochem Mol Biol201012126126420298784
- MatsumotoTItoMHayashiYA new active vitamin D3 analog, eldecalcitol, prevents the risk of osteoporotic fractures – a randomized, active comparator, double-blind studyBone20114960561221784190
- ShirakiMSaitoHMatsumotoTEldecalcitol normalizes bone turnover markers regardless of their pre-treatment levelsCurr Med Res Opin2012281547155222794117
- NakamuraTTakanoTFukunagaMShirakiMMatsumotoTEldecalcitol is more effective for the prevention of osteoporotic fractures than alfacalcidolJ Bone Miner Metab20133141742223575909
- HaginoHTakanoTFukunagaMShirakiMNakamuraTMatsumotoTEldecalcitol reduces the risk of severe vertebral fractures and improves the health-related quality of life in patients with osteoporosisJ Bone Miner Metab20133118318923129180
- Bischoff-FerrariHAKielDPDawson-HughesBDietary calcium and serum 25-hydroxyvitamin D status in relation to BMD among US adultsJ Bone Miner Res20092493594219113911
- MarwahaRKTandonNGargMKBone health in healthy Indian population aged 50 years and aboveOsteoporos Int2011222829283621271341
- ReidIRBollandMJGreyAEffects of vitamin D supplements on bone mineral density: a systematic review and meta-analysisLancet201438314615524119980
- DIPART (Vitamin D Individual Patient Analysis of Randomized Trials) GroupPatient level pooled analysis of 68 500 patients from seven major vitamin D fracture trials in US and EuropeBMJ2010340b546320068257
- AvenellAGillespieWJGillespieLDO’ConnellDVitamin D and vitamin D analogues for preventing fractures associated with involutional and post-menopausal osteoporosisCochrane Database Syst Rev2009CD00022719370554
- IwamotoJ1SatoY2Eldecalcitol improves chair-rising time in postmenopausal osteoporotic women treated with bisphosphonatesTher Clin Risk Manag201410515924476669
- SakaiAItoMTomomitsuTe-ADVANCED Study GroupEfficacy of combined treatment with alendronate (ALN) and eldecalcitol, a new active vitamin D analog, compared to that of concomitant ALN, vitamin D plus calcium treatment in Japanese patients with primary osteoporosisOsteoporos Int20152631193120225592133