
Abstract
Non-Alcoholic Fatty Pancreas disease (NAFPD), characterized by fat accumulation in pancreatic tissue, is an emerging clinical entity. However, the clinical associations, the underlying molecular drivers, and the pathophysiological mechanisms of NAFPD have not yet been characterized in detail. The NAFPD spectrum not only includes infiltration and accumulation of fat within and between pancreatic cells but also involves several inflammatory processes, dysregulation of physiological metabolic pathways, and hormonal defects. A deeper understanding of the underlying molecular mechanisms is key to correlate NAFPD with clinical entities including non-alcoholic fatty liver disease, metabolic syndrome, diabetes mellitus, atherosclerosis, as well as pancreatic cancer and pancreatitis. The aim of this review is to examine the pathophysiological mechanisms of NAFPD and to assess the possible causative/predictive risk factors of NAFPD-related clinical syndromes.
Introduction
Pancreatic fat deposition in the absence of excessive alcohol intake, described as non-alcoholic fatty pancreas disease (NAFPD),Citation1 is an emerging clinical entity.Citation2 Despite the higher susceptibility to fat deposition of the pancreas compared to the liver,Citation3,Citation4 the clinical relevance and underlying pathophysiological mechanisms of pancreatic fat infiltration remain unclear in the medical literature. Robertson F. Ogilvie was the first to describe pancreatic fat deposition in obese cadavers, reporting 17% of pancreatic fat storage, as compared to 9% in lean ones.Citation5 Since then, excessive storage of fat in pancreatic tissue has been described with various terms, including pancreatic lipomatosis, pancreatic steatosis, lipomatous pseudohypertrophy, fatty pancreas, and more.Citation6,Citation7 Currently, NAFPD is the widely accepted term, and its prevalence varies significantly among populations.Citation8–11
There are many sophisticated imaging techniques used as diagnostic tools to evaluate the pancreas, with transcutaneous ultrasound being the most common,Citation10,Citation12 since it is noninvasive, inexpensive, and easily performed. Nonetheless, endoscopic ultrasound (EUS),Citation10,Citation13 abdominal computed tomography (CT),Citation14 or magnetic resonance-based techniques including abdominal magnetic resonance imaging (MRI),Citation15,Citation16 and magnetic resonance spectroscopy (MRS)Citation17 can be used to quantify pancreatic fat content with accuracy. A direct comparison of these methods has not been performed yet. MRI enables noninvasive assessment of fat content in solid organs,Citation18 and with the Iterative Decomposition with Echo Asymmetry and Least squares estimation (IDEAL) method,Citation19 fat and water can be separated for a more precise organ assessment. EUS allows for a closer access to the pancreas; nonetheless, it is invasive and unsuitable for quantification of the entire pancreatic fat content.Citation10,Citation13 In the general population and in routine medical checkup settings, invasiveness and cost-effectiveness should always be considered before examining the pancreas. As far as physiological values are concerned, the highest limit of normal pancreatic fat is 10 4% when assessed by MRI/MRS.Citation9 However, a meta-analysis showed that the upper normal limit of pancreatic fat in healthy individuals, who participated in MRI studies, was 6.2%,Citation20 a threshold that is recommended for future research use.
The aim of this review is to explore the pathophysiological mechanisms of NAFPD and its clinical associations, as well as to examine which of these parameters are possible causative or predictive risk factors of NAFPD.
Pathogenesis
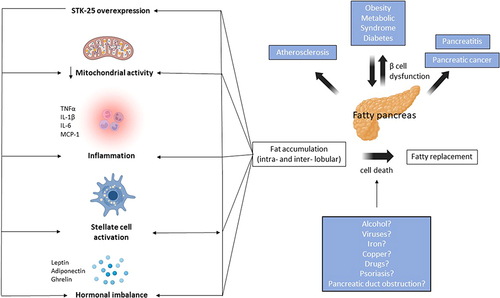
NAFPD is the result of several pathophysiological processes that act simultaneously (). These processes are generated mainly from excessive deposition of fat on pancreatic cells and include the following; (1) immediate cellular damage due to direct interaction of fatty tissue with pancreatic cells, with subsequent release of free fatty acids,1,Citation21–23 (2) chronic oxidative stressCitation24,Citation25 and local secretion of detrimental inflammatory markers,1,Citation26–28 (3) pathological activation or alterations in lipid-glucose metabolism, beta-oxidation, and other regulators,Citation29–31 and (4) an imbalance of hormone homeostasis.Citation32,Citation33
Figure 1 Pathogenetic mechanisms behind fatty pancreas. The main pathogenetic mechanism behind non-alcoholic fatty pancreas diseases (NAFPD) is fatty accumulation (intra- or inter- lobular), followed by fatty replacement and, ultimately, β cell dysfunction. The main risk factors associated with NAFPD are obesity and metabolic syndrome (including dyslipidemia), while alcohol, viruses, iron deposition, drugs, gut hormones, psoriasis and pancreatic duct obstruction represent potential secondary;hits’ which participate in cell death and replacement of pancreatic tissue with fat. Mechanisms associated with fat accumulation include reduction in mitochondrial activity, inflammatory cell infiltration with production of inflammatory cytokines (eg TNFα, ΙL-1β, IL-6, MCP-1), activation of stellate cells, hormonal imbalance (with perturbed leptin and adiponectin levels), as well as STK-25 pathway overexpression, which further exacerbates all the aforementioned mechanisms. NAFPD, in turn, is associated with various conditions including diabetes, pancreatitis, pancreatic cancer, as well as atherosclerosis.
Fat Replacement and Fat Accumulation
The main pathogenetic mechanism of NAFPD involves fatty replacement, which can either be intralobular or interlobular, followed by fat accumulation within the pancreatic tissue.Citation21 In most cases, excessive weight gain gradually leads to the storage of surplus adipose tissue in non-adipose organs, including the pancreas, where fat accumulates intracellularly in both acinar and pancreatic islet cells, causing dysfunction.Citation21 The fatty replacement phase is characterized by an accumulation of intralobular fat in the form of lipid droplets in both endocrine and acinar cells,Citation34,Citation35 provoking acinar cell death and their consecutive replacement by adipocytes, while pancreatic β-cells decrease and become dysfunctional.Citation1,Citation3,Citation36–41 Hence, fatty accumulation follows fatty replacement and acinar cell necrosis.Citation7,Citation34,Citation41,Citation42 Fatty replacement occurs unevenly throughout the pancreatic tissue, with the anterior aspect being more prone.Citation7 Of note, the term fatty replacement denotes irreversible damage, not fully correctable with medications or weight reduction.Citation43 In parallel, interlobular fat, that is fat around large vessels and ducts, involves adipocytes and lipid droplets in inactive stellate cells, which become stimulated.Citation22,Citation34 In addition, deposition of pancreatic fat ensues secondary to increased levels of free fatty acids in the plasma,Citation1 a process similar to the hepatic free fatty acid influx noted in non-alcoholic fatty liver disease (NAFLD).Citation44 Following such pancreatic insults, acinar cell apoptosis leads to rapid pancreatic volume decrease, but eventually, fatty restoration causes volume replacement until the pancreas becomes prominent and enlarged. In an animal model study, accumulation of fat tissue in the pancreas induced apoptosis, stellate cell activation, fibrosis, and, ultimately, a decrease in β/α islet cell ratio with loss of architecture.Citation45 Likewise, in another animal study, where obese mice were investigated for pancreatic cellular changes, intralobular and interlobular fat storage was responsible for a heavier pancreas, larger pancreatic islet cells, and atypical cellular structure.Citation28 These modifications may have occurred in an attempt of β-cells for compensation; β-cells compensate against initial cellular and metabolic fluctuations, presenting an enhancement in their secretory activity, an expansion of their β-cell mass, or both.Citation29 Overall, this might explain why pancreatic cells with chronically elevated fat content will become hypertrophic and hyperplastic.Citation46 Deposition of fat tissue in the pancreas, in combination with free circulating fatty acids, causes β-cell dysfunction,Citation23 with a baseline increase in insulin release, an impaired glucose-stimulated insulin secretion of β-cellsCitation29,Citation47,Citation48 and the generation of oxidative stress with consequent organ injuries.Citation1,Citation23,Citation49 After the increase of basal insulin secretion, there is a subsequent decrease, a state that cannot be repealed with the induction of compensatory proinsulin biosynthesis.Citation50 Therefore, clinical conditions, such as insulin secretion impairment and diabetes, might arise.Citation23,Citation46 Many of these mechanisms are supported in a human study, where Tushuizen et alCitation17 showed a negative correlation between pancreatic fat content with β-cell function in subjects without diabetes.
Oxidative Stress and Inflammatory Processes
Chronic oxidative stress is implicated in metabolic syndrome, diabetes mellitus and atherosclerosis. Indeed, oxidative stress is referred to as a “second hit” in cases of steatohepatitis,Citation12 so a similar process in the case of NAFPD may be hypothesized.Citation51
Increased body weight provokes chronic cortisol releaseCitation24 and activation of the hypothalamic-pituitary-adrenal (HPA) axis,Citation24,Citation25 thus increasing metabolic syndrome and atherosclerotic disease risk.Citation52 Fat storage induces local pancreatic inflammatory cell infiltration,Citation26 further inducing β-cell function deterioration and destruction. Pro-inflammatory cytokines, including tumor necrosis factor-alpha (TNF-α), interleukin-1β (ΙL-1β) and 6 (IL-6), monocyte chemotactic protein-1 (MCP-1) are released, leading to inflammation, fibrosis, and insulin resistance.Citation1 Free fatty acids are released via lipolysis of visceral adipose tissue,Citation22,Citation27,Citation28,Citation53 but also due to inflammatory responses,Citation27 altogether resulting in histopathological alterations and secondary pancreatic acinar cell atrophy and fibrosis.Citation38,Citation54 Of importance, the role of copper in pancreatic disease was investigated in an animal study.Citation55 The authors stated that pancreatic atrophy is more pronounced in males compared with females, while the endocrine male pancreas is also more susceptible to dietary copper deprivation than the female rat.Citation55 Similarly, copper is also important in NAFLD. In a cross-sectional study that included 100 obese patients with hepatic steatosis detected by ultrasound, it was shown that an altered copper bioavailability predicts early atherosclerosis.Citation56 Moreover, older studies demonstrated that pancreatic fatty deposition is also accompanied by leukocyte infiltration,Citation57 although more recent ones did not corroborate these findings.Citation1
Dysregulation of Metabolic Pathways
In terms of dysregulated pathways, fatty accumulation of the pancreas influences multiple regulatory pathways. First, fat deposition impairs pancreatic β-cell cAMP production and, as a result, it inhibits islet cell adaptation to the disturbed metabolic milieu.Citation29,Citation30 Another probable mechanism is the augmented phospholipid saturation of the mitochondrial membrane, which results in diminished mitochondrial function,Citation58 peroxisomal fatty acid metabolism, cytochrome P450 CYP-2E1 induction, and the subsequent production of free oxygen radicals, as in the case of NAFLD.Citation59,Citation60 This leads to further activation of stellate cells that attract neutrophils and cause an inflammatory reaction.Citation61 Additionally, in the context of chronic fatty pancreas accumulation, overexpression of the serine/threonine-protein kinase 25 (STK-25), a novel negative regulator of lipid and glucose metabolism, occurs.Citation62 STK-25 can be overexpressed when feeding mice with high-fat diets, aggravating lipid accumulation in cells and impairing skeletal muscle mitochondrial function, thereby diminishing insulin sensitivity.Citation62–64 In skeletal myocytes of patients with type 2 diabetes mellitus, STK-25 mRNA levels were significantly elevated, compared with healthy controls.Citation62 The overexpression of STK25 in NAFPD exacerbates all the aforementioned pathophysiological mechanisms, including inflammatory pancreas infiltration,Citation45,Citation65 stellate cell activation, β-cell loss, and pancreatic destruction.Citation45 Indeed, STK25 is considered to play a key role in both the pathogenesis and progression of NAFLD.Citation66 Overexpression of STK25 induces lipogenesis, triglyceride secretion and suppressed beta-oxidation.Citation66 A similar mechanism may be adopted by pancreatic cells in cases of STK25 overstimulation highlighting that NAFLD and NAFPD are two closely related conditions. Beta-oxidation is severely impaired during fatty accumulation.Citation31 When there is an impediment in fatty acid catabolism, fat will also accumulate in zone 3 of hepatocytes, giving rise to NAFLD.Citation12 In pancreatic tissue, parameters like hyperglycemia and hypertriglyceridemia induce cellular free fatty acid increase, loss of β-cell mass, as well as decreased beta-oxidation.Citation53 Increased glucose levels augment malonyl-coenzyme A via the tricarboxylic acid cycle, thus inhibiting carnitine palmitoyltransferase-1 and diminishing mitochondrial β-oxidation while stimulating triglyceride production in β-cells.Citation53 In correlation with that, when obese mice were studied,Citation1 accumulation of cholesterol and free fatty intoxication were observed. Through this process, triglyceride accumulation in β-cells is promoted, which, in combination with lipid peroxidation, leads acinar and islet cells to destruction.Citation27,Citation28,Citation53 When triglycerides continue to accumulate inside pancreatic cells, insulin gene expression is downregulated, and glucose-stimulated insulin secretion is impaired.Citation22,Citation28,Citation53
Dysregulation of Hormonal Homeostasis
Adipocytokines, which consist of adipose tissue released cytokines, adipokines and chemokines, are valuable bioactive substances that maintain metabolic homeostasis and protect against metabolic overload.Citation32,Citation33 Decreased levels of adiponectin in obese patients signify the loss of insulin sensitivity modulation, and the decrease of fatty acid oxidation in body tissues.Citation33 In contrast, regulation of leptin levels in obese patients is a more complex pathway. It is thought that leptin levels and obesity are reversibly correlated; when leptin increases, it leads to the expression of suppressor-of-cytokine-signaling (SOCS-3) pathway, which thereafter inhibits leptin signaling.Citation67 In obesity, adipocytokines like leptin and adiponectin may differentially affect pancreatic tissue.Citation33 It has been shown that adiponectin levels are positively correlated with plasma insulin and negatively associated with plasma triglycerides and insulin resistance.Citation68
Notably, it has been demonstrated that the gut-brain axis may also play a role in NAFPD, and more specifically overexpression of ghrelin may contribute to increased intra-pancreatic fat deposition in individuals with acute pancreatitis.Citation69 Similarly, gut hormones may contribute to NAFLD pathogenesis, but the association between intrahepatic fat deposition and gut hormones remains to be elucidated.Citation70
Human-Based Studies and Correlation with Molecular Abnormalities
Even though the pathophysiological mechanisms between fatty pancreas and β-cell dysfunction/apoptosis have been thoroughly discussed, recent findings from human studies do not come in accordance with previous conclusions. In a recent large cohort study of adult Chinese subjects, who had undergone fatty pancreas evaluation by MRI, an association of fatty pancreas and β-cell function was found.Citation9 However, this association disappeared after adjusting for BMI and intrahepatic triglycerides. Although this cohort did not show an independent association between fatty pancreas and β-cell function, pancreatic fat accumulation was still associated with insulin resistance, even after adjusting for hepatic fat content and BMI.Citation9 Likewise, in another human-based comprehensive analysis of interlobular, intralobular and parenchymal pancreatic fat and their effects on β-cell performance, no relationship was found between total and intralobular pancreatic adipose tissue infiltration with β-cell function.Citation71 In some small case series that compared pancreatic fat among patients with diabetes with that of normal controls, an association of fatty pancreas with weakened β-cell function and insulin secretion was noted.Citation17,Citation72 Nevertheless, we cannot conclude whether this β-cell dysfunction was established beforehand or if it was a direct consequence of fatty accumulation. Ozturk et al,Citation73 while studying the association between NAFLD and atherosclerosis, emphasized that insulin resistance appeared among their study population in the absence of obesity and diabetes mellitus. In a study of 106 subjects with new-onset of type 2 diabetes, no significant correlation was noted between the amount of pancreatic fat deposition and islet cell function.Citation74 The controversial results of previous studies either drive us towards the existence of more pathophysiological cascades that make fatty accumulation a causative factor of β-cell dysfunction, or to genetic polymorphisms, which are not yet under investigation. Other “hits” that can lead to pancreatic cell death include fibrosis of the pancreas, extreme alcohol intake, viral infections, iron overload, medications, or an obstruction of the pancreatic duct.Citation42
Clinical Associations of NAFPD
Nonalcoholic Fatty Liver Disease
Nonalcoholic fatty liver disease (NAFLD) occurs when hepatocytes are infiltrated with fat, in the absence of excessive alcohol consumption.Citation75 As mentioned above, obesity is the main causative risk factor, not only for NAFPD but also for NAFLD,Citation75 making these two clinical syndromes closely related. In general, fat deposition is linked to multiple diseases like metabolic syndrome, diabetes, and atherosclerosis.Citation2,Citation76
In a large cross-sectional study where NAFPD and its risk factors were examined, authors compared pancreatic echogenicity with that of the liver and demonstrated that fatty pancreas and fatty liver composition were found in combination in almost 26% of patients, whereas fatty pancreas alone was found in 16%.Citation11 In a prospective study almost 68% of the included patients with fatty pancreas presented with fatty liver, but 97% of patients initially diagnosed with fatty liver presented concurrently with a fatty pancreas, making fatty liver a strong predictive factor of fatty pancreas disease.Citation8 In a Chinese study, 67% of non-diabetic subjects with fatty pancreas had simultaneous fatty liver changes.Citation8 In this study, fatty liver was an independent risk factor for NAF-PD.8 Likewise, in another analysis among 60 patients with hepatic steatosis, 57% were found with NAFPD.Citation12 The amount of fat in liver tissue is significantly correlated with pancreatic fat in numerous other studies,Citation77–79 signifying that both clinical entities share similar risk factors, pathogenetic mechanisms and disease progression pathways. In a clinical trial including 121 obese/overweight children and adolescents, 48% of those with confirmed fatty liver disease of any severity exhibited NAFPD, while, in subjects with steatohepatitis the percentage of NAFPD increased to 80%.Citation78
On the contrary, some studies did not manage to find an association between pancreatic fat and liver fat.Citation4,Citation17,Citation72,Citation80 In a study of subjects with and without diabetes,Citation17 those with diabetes had higher liver fat content, but there was no statistically significant association between liver and pancreatic fat content. These contradictory results focusing on the correlation between NAFLD and NAFPD might imply that, despite that both syndromes share similar pathological mechanisms, organ fat accumulation may be distributed differently due to unknown mechanisms.
It is worth mentioning that, based on recent evidence, the association between NAFPD and NAFLD is also mediated via a systemic autoimmune comorbidity, namely psoriasis. Psoriasis is well associated with metabolic disturbances, including obesity, metabolic syndrome and type 2 diabetes, all of which consist risk factors for both NAFPD and NAFLD.Citation81–83 In psoriatic patients, chronic inflammation, mediated by pro-inflammatory cytokines and adipokines (especially TNF-α), drives insulin resistance and plays a crucial role not only in hepatic steatosis but potentially also in pancreatic steatosis.Citation84 Additionally, it has been suggested that psoriasis is associated with pancreatic diseases, such as pancreatitis and pancreatic cancer, as evident in recent published data.Citation85
Obesity and Metabolic Syndrome
Obesity is a multifactorial clinical entity that can lead to the excessive and pathological accumulation of adipose tissue in non-adipose tissues such as the pancreas, liver, heart, skeletal muscle and is associated with diabetes mellitus, cardiovascular disease, hypertension, and hyperlipidemia.Citation86–88 Since the term NAFPD describes the accumulation of fat into the pancreas, obesity is the main driver of this condition.Citation75 A large number of studies link central obesity and/or increased BMI to fatty deposition of the pancreas.Citation9,Citation10,Citation20
Metabolic syndrome is defined as the presence of at least three of the following risk factors: high blood glucose, increased levels of triglycerides, low levels of HDL cholesterol, large waist circumference and hypertension.Citation89 Many studies focusing on patients’ metabolic abnormalities try to correlate these with the existence of fatty pancreas. In 2009, Lee at al. studied 293 individuals from an obesity clinic with a confirmed diagnosis of pancreatic fat accumulation of various severity.Citation90 More than half of the patients (61.4%) were diagnosed with fatty pancreas. Results positively correlated pancreatic fat infiltration with metabolic risk factors, such as increased visceral fat and waist circumference, triglycerides, insulin resistance, correlating fatty pancreas with metabolic syndrome. Similarly, a case–control study showed that fatty pancreas was strongly associated with hypertension, increased blood glucose levels, central obesity, and increased triglycerides, but reported no association with HDL values.Citation91 A more recent study that systematically reviewed and analyzed data from 2675 individuals found that approximately 33% of them had NAFPD.Citation20 Among individuals with NAFPD, 44% of them met the criteria for metabolic syndrome.Citation20 In a prospective study by Sepe et al, fatty pancreas was observed in 27.8% of participants that underwent EUS for various purposes.Citation10 Notably, the presence of any component of metabolic syndrome was associated with a significant 37% increase in the prevalence of fatty pancreas. Individuals who fulfilled the criteria for metabolic syndrome had a 40% prevalence of fatty pancreas, rendering metabolic syndrome a strong predictive factor of NAFPD. Interestingly, a high-fat diet is associated with triglyceride accumulation mainly in pancreatic cells, rather than hepatocytes, making pancreatic steatosis an early consequence of metabolic syndrome.Citation3
On the other hand, Wong et al,9 showed that, among all metabolic syndrome components, only central obesity and hypertriglyceridemia were independent risk factors of NAFPD. A Turkish clinical trial also reported an association of fatty pancreas with metabolic syndrome, which was influenced, however, by other factors such as BMI and NAFLD.Citation92
Insulin Resistance - Prediabetes - Diabetes
Pancreas has an essential role in regulating glucose metabolism and glandular secretion under various metabolic circumstances. The pathogenesis of type 2 diabetes is characterized by peripheral insulin resistance and impaired glucose secretion, gradually leading to a decline in β-pancreatic cells and, later, to their gradual destruction. A disproportionate accumulation of visceral adipose tissue is a strong risk factor for insulin resistance.Citation93–95 However, study results remain controversial for the association between fatty pancreas and diabetes mellitus.
In numerous animal studies, islet cell abnormalities are related to pancreatic lipomatosis, and result in increased blood glucose levels.Citation48,Citation96 A human study reported an almost 12% incidence of diabetes in the NAFPD cohort versus a 5% incidence in the non-NAFPD group. NAFPD patients had an 108% increased risk of diabetes mellitus. Pancreatic fat was also found to be negatively associated with insulin secretion in other analyses,Citation72 as well as with hyperglycemia and occurrence of diabetes.Citation17,Citation72,Citation97 Of note, individuals presenting with both fatty pancreas and fatty liver, had the highest levels of insulin resistance compared to those with either condition alone.Citation9
Another analysis indicated that fatty pancreas at baseline is associated with an increased incidence of diabetes. However, this finding was not significant in multivariate analyses.Citation98 This was in line with results from a large cohort study, where, despite the high frequency of fatty pancreas in diabetes, their association did not reach statistical significance.Citation11 Other investigations did not support the association between fatty pancreas and diabetes mellitus or impairments in glucose levels as well.Citation10,Citation90
Conclusively, pancreatic steatosis may be an early event in the pathogenesis of diabetes,Citation99 but evidence pointing to an independent association is limited.
Atherosclerosis
NAFPD has been linked with atherosclerosis risk factors including advanced age, BMI, hypertension, and hyperlipidemiaCitation9,Citation28,Citation72,Citation90,Citation91 The effect of fatty pancreas on glucose and insulin metabolism, chronic low-grade inflammation and chronic stress may increase cardiovascular disease (CVD) risk.Citation100 This is amplified by the accumulation of lipids in coronary and peripheral blood vessels.
Carotid intima-media thickness (IMT) and carotid-femoral pulse wave velocity (cf-PWV) are widely used as indicators of subclinical atherosclerosis by detecting early functional and structural changes of the vascular wall.Citation101,Citation102 It has been shown that NAFLD, especially in advanced stages, is correlated with increased risk of atherosclerosis and, potentially, cardiovascular events.Citation103–107 However, it remains to be answered whether fatty pancreas is a predictive CVD factor. A study that included patients with biopsy-proven NAFLD and healthy controls showed that patients with fatty pancreas had significantly higher cf-PWV levels, whereas no association was found with carotid IMT. The link between cf-PWV/carotid IMT levels and fatty pancreas, nevertheless, was not observed upon adjusting for relevant variables.Citation92 In another case–control study, epicardial adipose tissue and aortic IMT were higher among NAFPD subjects, compared to those without NAFPD, while both epicardial adipose tissue and aortic IMT were independent risk factors of subclinical atherosclerosis.Citation108
Pancreatitis
Chronic high-fat dietary intake is associated with inter- as well as intra-pancreatic fat accumulation. As such, NAFPD progression may lead to chronic pancreatitis, and this association is expressed by the term “non-alcoholic steatopancreatitis” (NASP).Citation1,Citation109 In favor of this hypothesis, a study showed that obese mice are more likely to develop severe forms of pancreatitis than lean ones.Citation110 Additionally, in a review by Smith et al, preliminary data link acute pancreatitis with NASP.Citation7 According to the authors, the uneven secretion of proinflammatory cytokines creates an inflammatory environment which promotes bouts of acute pancreatitis.Citation7 Finally, a recent pilot study of 189 subjects indicated that fatty pancreas is a risk factor of acute pancreatitis.Citation111
Pancreatic Cancer
Obesity is strongly associated with pancreatic steatosis and inconsistently associated with pancreatic cancer; this raises concerns for a potential relationship between fatty pancreas and pancreatic cancer.
A meta-analysis of 4400 patients showed a positive association between increased BMI and risk of pancreatic cancer in both sexes, while central obesity was associated with an increased risk of pancreatic cancer only in women.Citation112 It has been described that NAFPD can lead to NASP and sequentially to pancreatic cancer.Citation113 In a study of 102 cases of pancreatic ductal adenocarcinoma, fatty pancreas was significantly higher in cases compared to healthy individuals.Citation114 Findings of a retrospective cross-sectional study analyzing data from patients with pancreatic carcinoma further supported the role of fatty pancreas in the development of pancreatic cancer.Citation115 According to Lesmana et al, NAFPD is the only significant risk factor when it comes to pancreatic cancer, while factors like age, gender, diabetes, and pancreatitis failed to show a causative role.Citation113 Indeed, in a case–control study of patients who underwent total resection due to pancreatic adenocarcinoma, patients with fatty pancreas had higher mortality.Citation116
At present, however, there is not enough evidence to decisively support the relationship between NAFPD and pancreatic cancer, and several studies have failed to detect an association. A study by Sepe et al did not find an association between fatty pancreas and pancreatic malignancy.Citation10 Wu et al also found no association between pancreatic carcinoma markers and NAFPD.Citation91
Pathogenetic Mechanisms and Clinical Entities Associated with NAFPD
The main risk factors associated with NAFPD are obesity and metabolic syndrome (including dyslipidemia), while alcohol, viruses, iron deposition, drugs and pancreatic duct obstruction represent potential secondary;hits’ which participate in cell death and replacement of pancreatic tissue with fat.Citation41,Citation90,Citation91,Citation100 The main pathogenetic mechanism of NAFPD is fatty replacement, followed by fatty accumulation (intra- or inter-lobular) and, ultimately, β-cell dysfunction.Citation21 Mechanisms associated with fat accumulation include reduction in mitochondrial activity, inflammatory cell infiltration with production of inflammatory cytokines (eg, TNFα, IL-1β, IL-6, MCP-1), activation of stellate cells, hormonal imbalance (with perturbed leptin and adiponectin levels, overexpression of ghrelin), as well as STK-25 pathway overexpression, which further exacerbate all the aforementioned mechanisms.Citation34,Citation70 B-cell dysfunction, as well as hormonal imbalance, in turn, can lead to insulin resistance, prediabetes and diabetes, while reduction in mitochondrial activity, inflammatory cell infiltration and activation of stellate cells, can lead to pancreatitis and pancreatic cancer.
Treatment of NAFPD
Despite the growing prevalence of NAFPD, its understanding remains limited and effective management strategies are still being explored. The effectiveness of current treatments for NAFPD is limited, as there is no approved pharmacologic therapy. To date, the most effective treatments are lifestyle modifications, including dietary changes, regular exercise, and weight-management programs.Citation117 Calorie restriction has been suggested as the potential means of normalizing β-cell function and reducing pancreatic fat content.
Troglitazone, a member of the thiazolidinedione class with insulin-sensitizing and anti-inflammatory propertiesCitation118 which has been withdrawn from the market,Citation119 has been implicated in NAFPD. Specifically, animal models have shown that troglitazone can reverse changes in tissue structure such as fibrosis and fatty accumulation, while reducing infiltration of inflammatory cells.Citation120 However, this effect has not been assessed by clinical trials. Glucagon-like peptide-1 (GLP-1) agonists have the potential to lessen the severity of NAFPD, by modulating the ER stress pathway and the subsequent signaling of apoptosis in mice models, and to alter regional adiposity in humans.Citation121,Citation122 Moreover, the synergistic activity of sitagliptin, a dipeptidyl peptidase (DPP) 4 inhibitor which prolongs the action of GLP-1 and insulin secretion from pancreatic β-cells, with telmisartan, which modulates inflammatory responses and improves endothelial function, exhibits remarkable efficacy in effectively managing the progression of NAFPD in mice.Citation123 Based on evidence from experimental models, GLP-1 agonists consist the most promising class of drugs for the treatment of NAFPD122 and prospective trials are needed to verify these data.
It has also demonstrated that bariatric surgery can lead to significant reductions in fat accumulation within the pancreas.Citation124 Nonetheless, education regarding healthy dietary habits and regular exercise should be the mainstay for reducing the NAFPD risk, as well as for treating those already diagnosed with it.
Nomenclature of NAFPD
The term “non-alcoholic fatty pancreas disease” is misleading, since many subjects with obesity may simultaneously consume alcohol, while it may also be stigmatizing. Similar to a recent proposal for NAFLD nomenclature,Citation125–127 we propose the term “Steatotic Pancreatic Disease” (SPD) in order to generally describe the accumulation of fat within pancreatic tissue, and the term “Metabolic dysfunction-associated Steatotic Pancreatic Disease” (MASPD) for describing the accumulation of fat within pancreatic tissue when this is associated with obesity or the metabolic syndrome.
Conclusion
NAFPD has been associated with a number of clinical entities, including metabolic syndrome, diabetes mellitus and atherosclerosis, but also with pancreatitis and pancreatic cancer. Similar clinical associations are observed in NAFLD. However, due to the scarcity of data on NAFPD, further studies are awaited to better determine related biological processes and metabolic sequelae.
Disclosure
Theodosios D. Filippatos reports participation in advisory boards for Lilly and lecture honoraria from Boehringer Ingelheim, Mylan, Astra Zeneca, Lilly, Recordati, Bausch Health, Servier, Viatris, Omega-Pharma and Innovis; personal fees from Perrigo, Innovis, and Servier, outside the submitted work. The remaining authors, Antonia Pagkali, Anastasios Makris, Kalliopi Brofidi, and Aris P. Agouridis have no conflict of interest to declare.
References
- Mathur A, Marine M, Lu D, et al. Nonalcoholic fatty pancreas disease. HPB. 2007;9(4):312–318. doi:10.1080/13651820701504157
- Filippatos TD. Non-Alcoholic Fatty Pancreas Disease: a Diagnosis of Increasing Importance. Angiology. 2022;73(6):495–496. doi:10.1177/00033197211053902
- Pinnick KE, Collins SC, Londos C, Gauguier D, Clark A, Fielding BA. Pancreatic ectopic fat is characterized by adipocyte infiltration and altered lipid composition. Obesity (Silver Spring). 2008;16(3):522–530. doi:10.1038/oby.2007.110
- Kovanlikaya A, Mittelman SD, Ward A, Geffner ME, Dorey F, Gilsanz V. Obesity and fat quantification in lean tissues using three-point Dixon MR imaging. Pediatr Radiol. 2005;35(6):601–607. doi:10.1007/s00247-005-1413-y
- Ogilvie RF. The islands of Langerhans in 19 cases of obesity. J Pathol Bacteriol. 1933;37(3):473–481. doi:10.1002/path.1700370314
- Paul J, Shihaz AVH. Pancreatic Steatosis: a New Diagnosis and Therapeutic Challenge in Gastroenterology. Arq Gastroenterol. 2020;57(2):216–220. doi:10.1590/s0004-2803.202000000-27
- Smits MM, van Geenen EJ. The clinical significance of pancreatic steatosis. Nat Rev Gastroenterol Hepatol. 2011;8(3):169–177. doi:10.1038/nrgastro.2011.4
- Wang CY, Ou HY, Chen MF, Chang TC, Chang CJ. Enigmatic ectopic fat: prevalence of nonalcoholic fatty pancreas disease and its associated factors in a Chinese population. J Am Heart Assoc. 2014;3(1):e000297. doi:10.1161/JAHA.113.000297
- Wong VW, Wong GL, Yeung DK, et al. Fatty pancreas, insulin resistance, and beta-cell function: a population study using fat-water magnetic resonance imaging. Am J Gastroenterol. 2014;109(4):589–597. doi:10.1038/ajg.2014.1
- Sepe PS, Ohri A, Sanaka S, et al. A prospective evaluation of fatty pancreas by using EUS. Gastrointest Endosc. 2011;73(5):987–993. doi:10.1016/j.gie.2011.01.015
- Lesmana CR, Pakasi LS, Inggriani S, Aidawati ML, Lesmana LA. Prevalence of Non-Alcoholic Fatty Pancreas Disease (NAFPD) and its risk factors among adult medical check-up patients in a private hospital: a large cross sectional study. BMC Gastroenterol. 2015;15:174. doi:10.1186/s12876-015-0404-1
- Al-Haddad M, Khashab M, Zyromski N, et al. Risk factors for hyperechogenic pancreas on endoscopic ultrasound: a case-control study. Pancreas. 2009;38(6):672–675. doi:10.1097/MPA.0b013e3181a9d5af
- Muftah AA, Pecha RL, Riojas Barrett M, et al. Pancreatic parenchymal changes seen on endoscopic ultrasound are dynamic in the setting of fatty pancreas: a short-term follow-up study. Pancreatology. 2022;22(8):1187–1194. doi:10.1016/j.pan.2022.10.006
- Ahbab S, Ünsal A, Ataoğlu HE, Can TS, Kayaş D, Savaş Y. Prediabetes and Type 2 Diabetes are Independent Risk Factors for Computed Tomography-Estimated Nonalcoholic Fatty Pancreas Disease. Clinics. 2019;74:e1337. doi:10.6061/clinics/2019/e1337
- Li J, Xie Y, Yuan F, Song B, Tang C. Noninvasive quantification of pancreatic fat in healthy male population using chemical shift magnetic resonance imaging: effect of aging on pancreatic fat content. Pancreas. 2011;40(2):295–299. doi:10.1097/MPA.0b013e318201669f
- Patel NS, Peterson MR, Brenner DA, Heba E, Sirlin C, Loomba R. Association between novel MRI-estimated pancreatic fat and liver histology-determined steatosis and fibrosis in non-alcoholic fatty liver disease. Aliment Pharmacol Ther. 2013;37(6):630–639. doi:10.1111/apt.12237
- Tushuizen ME, Bunck MC, Pouwels PJ, et al. Pancreatic fat content and beta-cell function in men with and without type 2 diabetes. Diabetes Care. 2007;30(11):2916–2921. doi:10.2337/dc07-0326
- Ma J. Dixon techniques for water and fat imaging. J Magn Reson Imaging. 2008;28(3):543–558. doi:10.1002/jmri.21492
- Reeder SB, Pineda AR, Wen Z, et al. Iterative decomposition of water and fat with echo asymmetry and least-squares estimation (IDEAL): application with fast spin-echo imaging. Magn Reson Med. 2005;54(3):636–644. doi:10.1002/mrm.20624
- Singh RG, Yoon HD, Wu LM, Lu J, Plank LD, Petrov MS. Ectopic fat accumulation in the pancreas and its clinical relevance: a systematic review, meta-analysis, and meta-regression. Metabolism. 2017;69:1–13. doi:10.1016/j.metabol.2016.12.012
- Catanzaro R, Cuffari B, Italia A, Marotta F. Exploring the metabolic syndrome: nonalcoholic fatty pancreas disease. World J Gastroenterol. 2016;22(34):7660–7675. doi:10.3748/wjg.v22.i34.7660
- Rugivarodom M, Geeratragool T, Pausawasdi N, Charatcharoenwitthaya P. Fatty Pancreas: linking Pancreas Pathophysiology to Nonalcoholic Fatty Liver Exploring the metabolic syndrome: nonalcoholic fatty pancreas disease Disease. J Clin Transl Hepatol. 2022;10(6):1229–1239. doi:10.14218/JCTH.2022.00085
- Guglielmi V, Sbraccia P. Type 2 diabetes: does pancreatic fat really matter? Diabetes Metab Res Rev. 2018;34(2). doi:10.1002/dmrr.2955
- Tannenbaum BM, Brindley DN, Tannenbaum GS, Dallman MF, McArthur MD, Meaney MJ. High-fat feeding alters both basal and stress-induced hypothalamic-pituitary-adrenal activity in the rat. Am J Physiol. 1997;273(6):E1168–1177. doi:10.1152/ajpendo.1997.273.6.E1168
- Kyrou I, Tsigos C. Stress mechanisms and metabolic complications. Horm Metab Res. 2007;39(6):430–438. doi:10.1055/s-2007-981462
- Fraulob JC, Ogg-Diamantino R, Fernandes-Santos C, Aguila MB, Mandarim-de-Lacerda CA. A Mouse Model of Metabolic Syndrome: insulin Resistance, Fatty Liver and Non-Alcoholic Fatty Pancreas Disease (NAFPD) in C57BL/6 Mice Fed a High Fat Diet. J Clin Biochem Nutr. 2010;46(3):212–223. doi:10.3164/jcbn.09-83
- Zhang X, Cui Y, Fang L, Li F. Chronic high-fat diets induce oxide injuries and fibrogenesis of pancreatic cells in rats. Pancreas. 2008;37(3):e31–38. doi:10.1097/MPA.0b013e3181744b50
- Filippatos TD, Alexakis K, Mavrikaki V, Mikhailidis DP. Nonalcoholic Fatty Pancreas Disease: role in Metabolic Syndrome, “Prediabetes”, Diabetes and Atherosclerosis. Dig Dis Sci. 2022;67(1):26–41. doi:10.1007/s10620-021-06824-7
- Yoshikawa H, Tajiri Y, Sako Y, Hashimoto T, Umeda F, Nawata H. Effects of free fatty acids on beta-cell functions: a possible involvement of peroxisome proliferator-activated receptors alpha or pancreatic/duodenal homeobox. Metabolism. 2001;50(5):613–618. doi:10.1053/meta.2001.22565
- Walz HA, Harndahl L, Wierup N, et al. Early and rapid development of insulin resistance, islet dysfunction and glucose intolerance after high-fat feeding in mice overexpressing phosphodiesterase 3B. J Endocrinol. 2006;189(3):629–641. doi:10.1677/joe.1.06522
- Houten SM, Wanders RJ. A general introduction to the biochemistry of mitochondrial fatty acid beta-oxidation. J Inherit Metab Dis. 2010;33(5):469–477. doi:10.1007/s10545-010-9061-2
- Juge-Aubry CE, Henrichot E, Meier CA. Adipose tissue: a regulator of inflammation. Best Pract Res Clin Endocrinol Metab. 2005;19(4):547–566. doi:10.1016/j.beem.2005.07.009
- Greenberg AS, Obin MS. Obesity and the role of adipose tissue in inflammation and metabolism. Am J Clin Nutr. 2006;83(2):461S–465S. doi:10.1093/ajcn/83.2.461S
- Matsuda A, Makino N, Tozawa T, et al. Pancreatic fat accumulation, fibrosis, and acinar cell injury in the Zucker diabetic fatty rat fed a chronic high-fat diet. Pancreas. 2014;43(5):735–743. doi:10.1097/MPA.0000000000000129
- Horii T, Kozawa J, Fujita Y, et al. Lipid droplet accumulation in beta cells in patients with type 2 diabetes is associated with insulin resistance, hyperglycemia and beta cell dysfunction involving decreased insulin granules. Front Endocrinol. 2022;13:996716. doi:10.3389/fendo.2022.996716
- Petrov MS, Taylor R. Intra-pancreatic fat deposition: bringing hidden fat to the fore. Nat Rev Gastroenterol Hepatol. 2022;19(3):153–168. doi:10.1038/s41575-021-00551-0
- Altinel D, Basturk O, Sarmiento JM, et al. Lipomatous pseudohypertrophy of the pancreas: a clinicopathologically distinct entity. Pancreas. 2010;39(3):392–397. doi:10.1097/MPA.0b013e3181bd2923
- Yan MX, Li YQ, Meng M, Ren HB, Kou Y. Long-term high-fat diet induces pancreatic injuries via pancreatic microcirculatory disturbances and oxidative stress in rats with hyperlipidemia. Biochem Biophys Res Commun. 2006;347(1):192–199. doi:10.1016/j.bbrc.2006.06.063
- Lee Y, Lingvay I, Szczepaniak LS, Ravazzola M, Orci L, Unger RH. Pancreatic steatosis: harbinger of type 2 diabetes in obese rodents. Int J Obes Lond. 2010;34(2):396–400. doi:10.1038/ijo.2009.245
- Lopez JM, Bombi JA, Valderrama R, et al. Effects of prolonged ethanol intake and malnutrition on rat pancreas. Gut. 1996;38(2):285–292. doi:10.1136/gut.38.2.285
- Chang ML. Fatty Pancreas-Centered Metabolic Basis of Pancreatic Adenocarcinoma: from Obesity, Diabetes and Pancreatitis to Oncogenesis. Biomedicines. 2022;10(3). doi:10.3390/biomedicines10030692
- Silva L, Fernandes MSS, Lima EA, Stefano JT, Oliveira CP, Jukemura J. Fatty Pancreas: disease or Finding? Clinics (Sao Paulo). 2021;76:e2439. doi:10.6061/clinics/2021/e2439
- Patel S, Bellon EM, Haaga J, Park CH. Fat replacement of the exocrine pancreas. AJR Am J Roentgenol. 1980;135(4):843–845. doi:10.2214/ajr.135.4.843
- den Boer M, Voshol PJ, Kuipers F, Havekes LM, Romijn JA. Hepatic steatosis: a mediator of the metabolic syndrome. Lessons from animal models. Arterioscler Thromb Vasc Biol. 2004;24(4):644–649. doi:10.1161/01.ATV.0000116217.57583.6e
- Nunez-Duran E, Chanclon B, Sutt S, et al. Protein kinase STK25 aggravates the severity of non-alcoholic fatty pancreas disease in mice. J Endocrinol. 2017;234(1):15–27. doi:10.1530/JOE-17-0018
- Pinte L, Balaban DV, Baicus C, Jinga M. Non-alcoholic fatty pancreas disease - practices for clinicians. Rom J Intern Med. 2019;57(3):209–219. doi:10.2478/rjim-2019-0005
- Nascimento FA, Barbosa-da-silva S, Fernandes-Santos C, Mandarim-de-Lacerda CA, Aguila MB. Adipose tissue, liver and pancreas structural alterations in C57BL/6 mice fed high-fat-high-sucrose diet supplemented with fish oil (n-3 fatty acid rich oil). Exp Toxicol Pathol. 2010;62(1):17–25. doi:10.1016/j.etp.2008.12.008
- Lee Y, Hirose H, Ohneda M, Johnson JH, McGarry JD, Unger RH. Beta-cell lipotoxicity in the pathogenesis of non-insulin-dependent diabetes mellitus of obese rats: impairment in adipocyte-beta-cell relationships. Proc Natl Acad Sci U S A. 1994;91(23):10878–10882. doi:10.1073/pnas.91.23.10878
- Chitturi S, Abeygunasekera S, Farrell GC, et al. NASH and insulin resistance: insulin hypersecretion and specific association with the insulin resistance syndrome. Hepatology. 2002;35(2):373–379. doi:10.1053/jhep.2002.30692
- Bollheimer LC, Skelly RH, Chester MW, McGarry JD, Rhodes CJ. Chronic exposure to free fatty acid reduces pancreatic beta cell insulin content by increasing basal insulin secretion that is not compensated for by a corresponding increase in proinsulin biosynthesis translation. J Clin Invest. 1998;101(5):1094–1101. doi:10.1172/JCI420
- Lin M, Weng SY, Chai KF, Mao ZJ. Lipidomics as a tool of predicting progression from non-alcoholic fatty pancreas disease to type 2 diabetes mellitus. RSC Adv. 2019;9(71):41419–41430. doi:10.1039/c9ra07071k
- Bonora E. The metabolic syndrome and cardiovascular disease. Ann Med. 2006;38(1):64–80. doi:10.1080/07853890500401234
- Yu TY, Wang CY. Impact of non-alcoholic fatty pancreas disease on glucose metabolism. J Diabetes Investig. 2017;8(6):735–747. doi:10.1111/jdi.12665
- Fernandes-Santos C, Evangelista Carneiro R, de Souza Mendonca L, Barbosa Aguila M, Mandarim-de-Lacerda CA. Rosiglitazone aggravates nonalcoholic Fatty pancreatic disease in C57BL/6 mice fed high-fat and high-sucrose diet. Pancreas. 2009;38(3):e80–86. doi:10.1097/MPA.0b013e3181987d9d
- Fields M, Lewis CG. Impaired endocrine and exocrine pancreatic functions in copper-deficient rats: the effect of gender. J Am Coll Nutr. 1997;16(4):346–351. doi:10.1080/07315724.1997.10718696
- Tarantino G, Porcu C, Arciello M, Andreozzi P, Balsano C. Prediction of carotid intima-media thickness in obese patients with low prevalence of comorbidities by serum copper bioavailability. J Gastroenterol Hepatol. 2018;33(8):1511–1517. doi:10.1111/jgh.14104
- Walters MN. Adipose atrophy of the exocrine pancreas. J Pathol Bacteriol. 1966;92(2):547–557. doi:10.1002/path.1700920232
- de Wilde J, Mohren R, van den Berg S, et al. Short-term high fat-feeding results in morphological and metabolic adaptations in the skeletal muscle of C57BL/6J mice. Physiol Genomics. 2008;32(3):360–369. doi:10.1152/physiolgenomics.00219.2007
- Emery MG, Fisher JM, Chien JY, et al. CYP2E1 activity before and after weight loss in morbidly obese subjects with nonalcoholic fatty liver disease. Hepatology. 2003;38(2):428–435. doi:10.1053/jhep.2003.50342
- Chtioui H, Semela D, Ledermann M, Zimmermann A, Dufour JF. Expression and activity of the cytochrome P450 2E1 in patients with nonalcoholic steatosis and steatohepatitis. Liver Int. 2007;27(6):764–771. doi:10.1111/j.1478-3231.2007.01524.x
- Ikejima K, Okumura K, Kon K, Takei Y, Sato N. Role of adipocytokines in hepatic fibrogenesis. J Gastroenterol Hepatol. 2007;22(Suppl 1):S87–92. doi:10.1111/j.1440-1746.2007.04961.x
- Nerstedt A, Cansby E, Andersson CX, et al. Serine/threonine protein kinase 25 (STK25): a novel negative regulator of lipid and glucose metabolism in rodent and human skeletal muscle. Diabetologia. 2012;55(6):1797–1807. doi:10.1007/s00125-012-2511-7
- Chursa U, Nunez-Duran E, Cansby E, et al. Overexpression of protein kinase STK25 in mice exacerbates ectopic lipid accumulation, mitochondrial dysfunction and insulin resistance in skeletal muscle. Diabetologia. 2017;60(3):553–567. doi:10.1007/s00125-016-4171-5
- Amrutkar M, Cansby E, Chursa U, et al. Genetic Disruption of Protein Kinase STK25 Ameliorates Metabolic Defects in a Diet-Induced Type 2 Diabetes Model. Diabetes. 2015;64(8):2791–2804. doi:10.2337/db15-0060
- Amrutkar M, Cansby E, Nunez-Duran E, et al. Protein kinase STK25 regulates hepatic lipid partitioning and progression of liver steatosis and NASH. FASEB J. 2015;29(4):1564–1576. doi:10.1096/fj.14-264937
- Amrutkar M, Chursa U, Kern M, et al. STK25 is a critical determinant in nonalcoholic steatohepatitis. FASEB J. 2016;30(10):3628–3643. doi:10.1096/fj.201600562R
- Munzberg H, Flier JS, Bjorbaek C. Region-specific leptin resistance within the hypothalamus of diet-induced obese mice. Endocrinology. 2004;145(11):4880–4889. doi:10.1210/en.2004-0726
- Akagiri S, Naito Y, Ichikawa H, et al. A Mouse Model of Metabolic Syndrome; Increase in Visceral Adipose Tissue Precedes the Development of Fatty Liver and Insulin Resistance in High-Fat Diet-Fed Male KK/Ta Mice. J Clin Biochem Nutr. 2008;42(2):150–157. doi:10.3164/jcbn.2008022
- Al-Ani Z, Ko J, Petrov MS. Intra-pancreatic fat deposition across the pancreatitis spectrum and the influence of gut hormones. Dig Liver Dis. 2023;55(8):1081–1090. doi:10.1016/j.dld.2023.02.013
- Finelli C, Padula MC, Martelli G, Tarantino G. Could the improvement of obesity-related co-morbidities depend on modified gut hormones secretion? World J Gastroenterol. 2014;20(44):16649–16664. doi:10.3748/wjg.v20.i44.16649
- Begovatz P, Koliaki C, Weber K, et al. Pancreatic adipose tissue infiltration, parenchymal steatosis and beta cell function in humans. Diabetologia. 2015;58(7):1646–1655. doi:10.1007/s00125-015-3544-5
- Heni M, Machann J, Staiger H, et al. Pancreatic fat is negatively associated with insulin secretion in individuals with impaired fasting glucose and/or impaired glucose tolerance: a nuclear magnetic resonance study. Diabetes Metab Res Rev. 2010;26(3):200–205. doi:10.1002/dmrr.1073
- Ozturk K, Uygun A, Guler AK, et al. Nonalcoholic fatty liver disease is an independent risk factor for atherosclerosis in young adult men. Atherosclerosis. 2015;240(2):380–386. doi:10.1016/j.atherosclerosis.2015.04.009
- Li YX, Sang YQ, Sun Y, et al. Pancreatic Fat is not significantly correlated with beta-cell Dysfunction in Patients with new-onset Type 2 Diabetes Mellitus using quantitative Computed Tomography. Int J Med Sci. 2020;17(12):1673–1682. doi:10.7150/ijms.46395
- van Geenen EJ, Smits MM, Schreuder TC, van der Peet DL, Bloemena E, Mulder CJ. Nonalcoholic fatty liver disease is related to nonalcoholic fatty pancreas disease. Pancreas. 2010;39(8):1185–1190. doi:10.1097/MPA.0b013e3181f6fce2
- Wu S, Wu F, Ding Y, Hou J, Bi J, Zhang Z. Association of non-alcoholic fatty liver disease with major adverse cardiovascular events: a systematic review and meta-analysis. Sci Rep. 2016;6:33386. doi:10.1038/srep33386
- Sijens PE, Edens MA, Bakker SJ, Stolk RP. MRI-determined fat content of human liver, pancreas and kidney. World J Gastroenterol. 2010;16(16):1993–1998. doi:10.3748/wjg.v16.i16.1993
- Della Corte C, Mosca A, Majo F, et al. Nonalcoholic fatty pancreas disease and Nonalcoholic fatty liver disease: more than ectopic fat. Clin Endocrinol (Oxf). 2015;83(5):656–662. doi:10.1111/cen.12862
- Patel NS, Peterson MR, Lin GY, et al. Insulin Resistance Increases MRI-Estimated Pancreatic Fat in Nonalcoholic Fatty Liver Disease and Normal Controls. Gastroenterol Res Pract. 2013;2013:498296. doi:10.1155/2013/498296
- Schwenzer NF, Machann J, Martirosian P, et al. Quantification of pancreatic lipomatosis and liver steatosis by MRI: comparison of in/opposed-phase and spectral-spatial excitation techniques. Invest Radiol. 2008;43(5):330–337. doi:10.1097/RLI.0b013e31816a88c6
- Rathod A, Neema S, Radhakrishnan S, Vendhan S, Tripathy DM, Vasudevan B. Palmoplantar Plaque Psoriasis is Associated with Diabetes, Hypertension, Obesity, and Metabolic Syndrome-A Case-Control Study. Indian Dermatol Online J. 2022;13(5):606–610. doi:10.4103/idoj.idoj_59_22
- Jensen P, Skov L. Psoriasis and Obesity. Dermatology. 2016;232(6):633–639. doi:10.1159/000455840
- Hao Y, Zhu YJ, Zou S, et al. Metabolic Syndrome and Psoriasis: mechanisms and Future Directions. Front Immunol. 2021;12:711060. doi:10.3389/fimmu.2021.711060
- Balato N, Napolitano M, Ayala F, Patruno C, Megna M, Tarantino G. Nonalcoholic fatty liver disease, spleen and psoriasis: new aspects of low-grade chronic inflammation. World J Gastroenterol. 2015;21(22):6892–6897. doi:10.3748/wjg.v21.i22.6892
- Białecka A. Evaluation of pancreatic function in patients with plaque psoriasis. Postepy Dermatol Alergol. 2023;40(3):372–376. doi:10.5114/ada.2023.129400
- Haslam DW, James WP. Obesity. Lancet. 2005;366(9492):1197–1209. doi:10.1016/S0140-6736(05)67483-1
- Van Gaal LF, Mertens IL, De Block CE. Mechanisms linking obesity with cardiovascular disease. Nature. 2006;444(7121):875–880. doi:10.1038/nature05487
- Panuganti KK, Nguyen M, Kshirsagar RK. Obesity. Statpearls, Treasure Island. 2022.
- Grundy SM, Cleeman JI, Daniels SR, et al. Diagnosis and management of the metabolic syndrome: an American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement. Circulation. 2005;112(17):2735–2752. doi:10.1161/CIRCULATIONAHA.105.169404
- Lee JS, Kim SH, Jun DW, et al. Clinical implications of fatty pancreas: correlations between fatty pancreas and metabolic syndrome. World J Gastroenterol. 2009;15(15):1869–1875. doi:10.3748/wjg.15.1869
- Wu WC, Wang CY. Association between non-alcoholic fatty pancreatic disease (NAFPD) and the metabolic syndrome: case-control retrospective study. Cardiovasc Diabetol. 2013;12:77. doi:10.1186/1475-2840-12-77
- Ozturk K, Dogan T, Celikkanat S, et al. The association of fatty pancreas with subclinical atherosclerosis in nonalcoholic fatty liver disease. Eur J Gastroenterol Hepatol. 2018;30(4):411–417. doi:10.1097/MEG.0000000000001059
- Seppala-Lindroos A, Vehkavaara S, Hakkinen AM, et al. Fat accumulation in the liver is associated with defects in insulin suppression of glucose production and serum free fatty acids independent of obesity in normal men. J Clin Endocrinol Metab. 2002;87(7):3023–3028. doi:10.1210/jcem.87.7.8638
- Gabriely I, Ma XH, Yang XM, et al. Removal of visceral fat prevents insulin resistance and glucose intolerance of aging: an adipokine-mediated process? Diabetes. 2002;51(10):2951–2958. doi:10.2337/diabetes.51.10.2951
- Kotronen A, Seppala-Lindroos A, Bergholm R, Yki-Jarvinen H. Tissue specificity of insulin resistance in humans: fat in the liver rather than muscle is associated with features of the metabolic syndrome. Diabetologia. 2008;51(1):130–138. doi:10.1007/s00125-007-0867-x
- Milburn JL Jr, Hirose H, Lee YH, et al. Pancreatic beta-cells in obesity. Evidence for induction of functional, morphologic, and metabolic abnormalities by increased long chain fatty acids. J Biol Chem. 1995;270(3):1295–1299. doi:10.1074/jbc.270.3.1295
- Lingvay I, Esser V, Legendre JL, et al. Noninvasive quantification of pancreatic fat in humans. J Clin Endocrinol Metab. 2009;94(10):4070–4076. doi:10.1210/jc.2009-0584
- Yamazaki H, Tsuboya T, Katanuma A, et al. Lack of Independent Association Between Fatty Pancreas and Incidence of Type 2 Diabetes: 5-Year Japanese Cohort Study. Diabetes Care. 2016;39(10):1677–1683. doi:10.2337/dc16-0074
- Raeder H, Haldorsen IS, Ersland L, et al. Pancreatic lipomatosis is a structural marker in nondiabetic children with mutations in carboxyl-ester lipase. Diabetes. 2007;56(2):444–449. doi:10.2337/db06-0859
- Lim S, Meigs JB. Links between ectopic fat and vascular disease in humans. Arterioscler Thromb Vasc Biol. 2014;34(9):1820–1826. doi:10.1161/ATVBAHA.114.303035
- Chung GE, Choi SY, Kim D, et al. Nonalcoholic fatty liver disease as a risk factor of arterial stiffness measured by the cardioankle vascular index. Medicine (Baltimore). 2015;94(12):e654. doi:10.1097/MD.0000000000000654
- Ozturk K, Guler AK, Cakir M, et al. Pulse Wave Velocity, Intima Media Thickness, and Flow-mediated Dilatation in Patients with Normotensive Normoglycemic Inflammatory Bowel Disease. Inflamm Bowel Dis. 2015;21(6):1314–1320. doi:10.1097/MIB.0000000000000355
- Rasool A, Dar W, Latief M, Dar I, Sofi N, Khan MA. Nonalcoholic fatty liver disease as an independent risk factor for carotid atherosclerosis. Brain Circ. 2017;3(1):35–40. doi:10.4103/bc.bc_28_16
- Fracanzani AL, Tiraboschi S, Pisano G, et al. Progression of carotid vascular damage and cardiovascular events in non-alcoholic fatty liver disease patients compared to the general population during 10 years of follow-up. Atherosclerosis. 2016;246:208–213. doi:10.1016/j.atherosclerosis.2016.01.016
- Li N, Zhang GW, Zhang JR, et al. Non-alcoholic fatty liver disease is associated with progression of arterial stiffness. Nutr, Metab Cardiovasc Dis. 2015;25(2):218–223. doi:10.1016/j.numecd.2014.10.002
- Zheng J, Zhou Y, Zhang K, et al. Association between nonalcoholic fatty liver disease and subclinical atherosclerosis: a cross-sectional study on population over 40 years old. BMC Cardiovasc Disord. 2018;18(1):147. doi:10.1186/s12872-018-0877-2
- Sahin S, Yerlikaya MG, Ozderya A, et al. Non-Alcoholic Fatty Pancreas Disease is Associated with SYNTAX Score in Acute Coronary Syndrome. Acta Cardiol Sin. 2022;38(6):683–690. doi:10.6515/ACS.202211_38(6).20220424A
- Kul S, Karadeniz A, Dursun I, et al. Non-Alcoholic Fatty Pancreas Disease is Associated with Increased Epicardial Adipose Tissue and Aortic Intima-Media Thickness. Acta Cardiol Sin. 2019;35(2):118–125. doi:10.6515/ACS.201903_35(2).20181009A
- Pitt HA. Hepato-pancreato-biliary fat: the good, the bad and the ugly. HPB. 2007;9(2):92–97. doi:10.1080/13651820701286177
- Zyromski NJ, Mathur A, Pitt HA, et al. A murine model of obesity implicates the adipokine milieu in the pathogenesis of severe acute pancreatitis. Am J Physiol Gastrointest Liver Physiol. 2008;295(3):G552–558. doi:10.1152/ajpgi.90278.2008
- Sbeit W, Khoury T. Fatty Pancreas Represents a Risk Factor for Acute Pancreatitis: a Pilot Study. Pancreas. 2021;50(7):990–993. doi:10.1097/MPA.0000000000001867
- Arslan AA, Helzlsouer KJ, Kooperberg C, et al. Anthropometric measures, body mass index, and pancreatic cancer: a pooled analysis from the Pancreatic Cancer Cohort Consortium (PanScan). Arch Intern Med. 2010;170(9):791–802. doi:10.1001/archinternmed.2010.63
- Lesmana CRA, Gani RA, Lesmana LA. Non-alcoholic fatty pancreas disease as a risk factor for pancreatic cancer based on endoscopic ultrasound examination among pancreatic cancer patients: a single-center experience. JGH Open. 2018;2(1):4–7. doi:10.1002/jgh3.12032
- Hori M, Takahashi M, Hiraoka N, et al. Association of pancreatic Fatty infiltration with pancreatic ductal adenocarcinoma. Clin Transl Gastroenterol. 2014;5(3):e53. doi:10.1038/ctg.2014.5
- Khoury T, Sbeit W. Fatty Pancreas and Pancreatic Cancer: an Overlooked Association? J Clin Med. 2022;11(3). doi:10.3390/jcm11030763
- Mathur A, Zyromski NJ, Pitt HA, et al. Pancreatic steatosis promotes dissemination and lethality of pancreatic cancer. J Am Coll Surg. 2009;208(5):989–994. doi:10.1016/j.jamcollsurg.2008.12.026
- Zhang CL, Wang JJ, Li JN, Yang Y. Nonalcoholic fatty pancreas disease: an emerging clinical challenge. World J Clin Cases. 2021;9(23):6624–6638. doi:10.12998/wjcc.v9.i23.6624
- Rizos CV, Liberopoulos EN, Mikhailidis DP, Elisaf MS. Pleiotropic effects of thiazolidinediones. Expert Opin Pharmacother. 2008;9(7):1087–1108. doi:10.1517/14656566.9.7.1087
- Gottlieb S. Company played down drug’s risks, report says. BMJ. 2001;322(7288).
- Jia DM, Fukumitsu KI, Tabaru A, Akiyama T, Otsuki M. Troglitazone stimulates pancreatic growth in congenitally CCK-A receptor-deficient OLETF rats. Am J Physiol Regul Integr Comp Physiol. 2001;280(5):R1332–1340. doi:10.1152/ajpregu.2001.280.5.R1332
- Fang T, Huang S, Chen Y, Chen Z, Chen J, Hu W. Glucagon Like Peptide-1 Receptor Agonists Alter Pancreatic and Hepatic Histology and Regulation of Endoplasmic Reticulum Stress in High-fat Diet Mouse Model. Exp Clin Endocrinol Diabetes. 2021;129(9):625–633. doi:10.1055/a-1240-4936
- Akoumianakis I, Zagaliotis A, Konstantaraki M, Filippatos TD. GLP-1 analogs and regional adiposity: a systematic review and meta-analysis. Obes Rev. 2023;e13574. doi:10.1111/obr.13574
- Souza-Mello V, Gregório BM, Relvas-Lucas B, da Silva Faria T, Aguila MB, Mandarim-de-Lacerda CA. Pancreatic ultrastructural enhancement due to telmisartan plus sitagliptin treatment in diet-induced obese C57BL/6 mice. Pancreas. 2011;40(5):715–722. doi:10.1097/MPA.0b013e3182153922
- Salman AA, Salman MA, Said M, et al. Improvement of Pancreatic Steatosis and Indices of Insulin Resistance After Metabolic Surgery. Front Med Lausanne. 2022;9:894465. doi:10.3389/fmed.2022.894465
- Rinella ME, Lazarus JV, Ratziu V, et al. A multi-society Delphi consensus statement on new fatty liver disease nomenclature. Ann Hepatol. 2023:101133. doi:10.1016/j.aohep.2023.101133
- Rinella ME, Lazarus JV, Ratziu V, et al. A multi-society Delphi consensus statement on new fatty liver disease nomenclature. J Hepatol. 2023. doi:10.1016/j.jhep.2023.06.003
- Rinella ME, Lazarus JV, Ratziu V, et al. A multi-society Delphi consensus statement on new fatty liver disease nomenclature. Hepatology. 2023. doi:10.1097/hep.0000000000000520