
Abstract
Background
Intensive care units (ICUs) are specialized units where patients with critical conditions are admitted for getting specialized and individualized medical treatment. High mortality rates have been observed in ICUs, but the exact reason and factors affecting the mortality rates have not yet been studied in the local population in Pakistan.
Aim
This study was aimed to determine rational use of antibiotic therapy in ICU patients and its impact on clinical outcomes and mortality rate.
Methods
This was a retrospective, longitudinal (cohort) study including 100 patients in the ICU of the largest tertiary care hospital of the capital city of Pakistan.
Results
It was observed that empiric antibiotic therapy was initiated in 68% of patients, while culture sensitivity test was conducted for only 19% of patients. Thirty-percent of patients developed nosocomial infections and empiric antibiotic therapy was not initiated for those patients (P<0.05). Irrational antibiotic prescribing was observed in 86% of patients, and among them, 96.5% mortality was observed (P<0.05). The overall mortality rate was 83%; even higher mortality rates were observed in patients on a ventilator, patients with serious drug–drug interactions, and patients prescribed with irrational antibiotics or nephrotoxic drugs. Adverse clinical outcomes leading to death were observed to be significantly associated (P<0.05) with irrational antibiotic prescribing, nonadjustment of doses of nephrotoxic drugs, use of steroids, and major drug–drug interactions.
Conclusion
It was concluded that empiric antibiotic therapy is beneficial in patients and leads to a reduction in the mortality rate. Factors including irrational antibiotic selection, prescribing contraindicated drug combinations, and use of nephrotoxic drugs were associated with high mortality rate and poor clinical outcomes.
Introduction
Intensive care units (ICUs), also known as intensive therapy units or critical care units, are special hospital wards that provide treatment and monitoring for critically ill patients. Since patients with critical infectious diseases are also managed in ICUs, they can become a major source of spreading infectious organisms which may lead to nosocomial infections. Such nosocomial infections are associated with increased morbidity, mortality, and health care costs.Citation1 Nosocomial infections are a serious patient safety concern in modern health care system, since it is the fifth leading cause of death among hospitalized patients. ICU patients are five to ten times more likely to acquire nosocomial infections than those in general ward.Citation2 Nosocomial infections occur worldwide and affect both developing and developed countries.Citation3
Empiric antibiotic administration is required in majority of ICU patients, but extensive use of both broad- and narrow-spectrum antibiotics may lead to development of resistant strains of bacteria and other pathogens.Citation4 The extensive and irrational use of antibiotics has also been reported to increase the risk of toxicity and drug interactions.Citation5
This study was aimed to determine the rational use of antibiotic therapy in ICU patients, its impact on clinical outcomes, and mortality rate. The study was also focused to identify factors affecting mortality rate in ICU patients undergoing antibiotic therapy.
Patients and methods
Ethical approval
Ethical approval was taken from the Ethics Review Board of Pakistan Institute of Medical Sciences, Hospital. Since this was a retrospective study in which all patients were either discharged after recovery or died during treatment, taking individual patient consent was not possible. Therefore, the Ethics Review Board waived the requirement of patient consent form. Patient data confidentiality and its compliance with the Declaration of Helsinki were ensured by the Ethics Review Board.
Study settings and design
This was a retrospective longitudinal (cohort) study including patients admitted in either medical or surgical ICU of the largest tertiary care hospital of the capital city of Pakistan.
Study sample
The study sample included all patients fulfilling the inclusion criteria and who were admitted and subsequently discharged/ died between September 2016 and April 2017 in the ICU of the largest tertiary care hospital of capital of Pakistan. Patients aged 2–60 years with <30 days of ICU stay were included in the study, since the accurate renal function cannot be determined using Cockroft–Gault (equation) method for patients <2 and >60 years of age.
Clinical evaluation
Daily clinical evaluation was performed for each patient using standard methods and approved guidelines. The difference in values of all studied variables was determined before and after the start of any therapy. The clinical outcomes were determined on the last day in terms of “discharge” or “death” after treatment. Renal function was determined using Cockroft– Gault equation,Citation6 and the need for dose adjustment and required dose after adjustment was determined using guidelines from the Physician Desk Reference,Citation7 British National Formulary,Citation8 and Renal Pharmacotherapy.Citation9 The adverse events for every administered drug were enlisted from clinical drug literatures approved by the US Food and Drug Administration, the Medicine and Healthcare Products Regulatory Agency, UK and the European Medicine Agency. Drug–drug interactions were determined by Stockley’s drug interaction.Citation10 The control of infection was determined using reduction in white blood cell (WBC) count and fever, and the appropriateness of the antibiotic therapy was determined using the results of culture sensitivity test (CST) and the American Society of Infectious Diseases (IDSA) guidelines.
Study tool (evidence-based clinical checklist)
An evidence-based clinical checklist was adapted from an already developed clinical checklist.Citation11 The variables included in the checklist were also compared with previous reported studies and discussed among a focus group of clinical researchers and practitioners. The finally developed checklist was also subjected to content validity through a pilot study on 20 patients and to focus group discussion to identify any missed variable or clinical scenario. After validation, the final version of the checklist was used during the study.
Statistical analysis
All the data collected through clinical checklist were transcribed on a spreadsheet in SPSS after carefully defining all the variables under study. The analysis was performed in two steps including a descriptive analysis in which patient clinical situation and various variables were studied for their respective frequencies, percentages, and measure of central tendencies. Later, in the second step, inferential statistics was employed to determine the associations among patient- and therapy-related variables, clinical outcomes, and mortality rate using Pearson’s chi-squared test, and P-value <0.05 was considered statistically significant.
Results
This study involved 100 patients which fulfilled the inclusion criteria and were discharged from the ICU between September 2016 and April 2017, including both males (43%) and females (57%). Twenty patients were between 2 and 20 years age, while 44 patients were between 21 and 40 years old and 36 patients were in the age group of 41–60 years. The length of the ICU stay for all the patients under investigation was from 2 to 30 days.
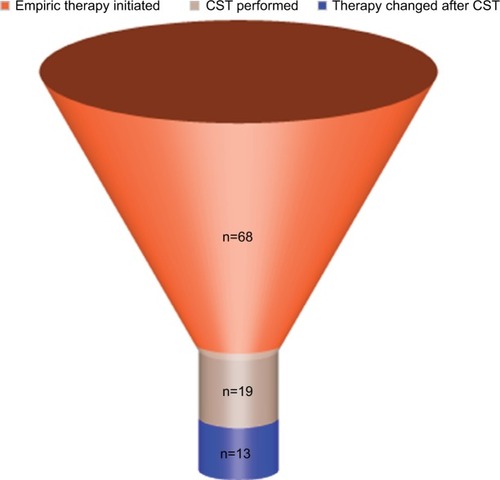
In our study, 68% patients were being administered empiric therapy with broad-spectrum antibiotics; among them, samples for CST were drawn in only 7% of the patients (P=0.001). Antibiotic therapy was changed in 13% patients (P=0.000) after the CST reports were received. The concept of de-escalation therapyCitation12 was not followed in this hospital, and none of the initiated antibiotics were de-escalated or stopped; instead, new antibiotics were added after the CST results. The results are presented in and .
Table 1 Frequency of various scenarios while prescribing empiric antibiotics
Figure 1 Funnel graph showing the frequency (n) of changes in antibiotic therapy after initiation of empiric therapy.
Abbreviation: CST, culture sensitivity test.
During our investigation period, 30% of the patients developed infections 3 days after their admission in hospital ICU, and therefore, it was declared that they had nosocomial infection.Citation13 The pattern of nosocomial infection was statistically insignificant among the gender and age groups. It was observed that nosocomial infection developed in every patient who was not administered empiric antibiotic therapy (P=0.0002), as shown in . In our study, 29 patients were on ventilator, and among them, 10 (34.5%) patients developed nosocomial infections with very high mortality rate (89.7%). Other than the common broad-spectrum antibiotics, some narrow-spectrum antibiotics were also prescribed ().
Table 2 Cross-tabulation of development of NIs against initiation of empiric antibiotic therapy
Table 3 Frequency of prescription of narrow-spectrum antibiotics
Since the study was carried out in ICU where patients are brought due to multiple reasons, one of the important factors while selecting a drug therapy to be prescribed is the route of metabolism and excretion of the drug and the renal/ hepatic profile of the patients.Citation14 Since a majority of the drugs are excreted through kidneys, assessing the kidney function is a key factor in ensuring administration of safe and effective therapy.Citation15
In our study, it was determined that 41% of the patients were renally compromised, and they needed careful administration of renally excreted drugs.Citation16 The use of nonsteroidal anti-inflammatory drugs was not seen in any of the patient, and instead, steroidal analgesics were used. Use of vancomycin, aminoglycoside, steroids, and proton pump inhibitors (PPIs) was observed, which need to be avoided or administered carefully among renally compromised patients. The use of PPI was high (P=0.008) in renally compromised patients as compared to those with normal renal function. The results of the frequency of nephrotoxic drugs prescribed are provided in .
Table 4 Frequency of prescribing potentially nephrotoxic drugs among renally compromised patients
Out of 41 renally compromised patients, 38 were being prescribed with nephrotoxic drugs for which dose adjustments were required. No renal dose adjustments were made in any of the patients and among the 41 renally compromised patients, 85.4% died at the end of the study.
In our study, only 14% patients were prescribed antibiotics as per the recommendations of IDSA and all these patients were discharged after recovery. Also, among the 86% patients in whom IDSA recommendations were not followed, statistically significant (P=0.000) mortality rate (96.5%) was observed. The results are presented in .
Table 5 Association of various clinical variables with appropriateness of antibiotic therapy
Among patients having recurrent infection even after antibiotic administration, 85% of them were initially prescribed with in appropriate antibiotics. Appropriate antibiotic therapy was not administered in majority (26 [89.7%]) of the ventilator patients. One hundred percent mortality rate was observed among all such patients on ventilator for whom appropriate antibiotic therapy had not been administered.
The signs of infection including raised WBC count and/ or feverCitation17 were observed in 60% of patients already on antibiotic therapy, with a mean WBC count of 41.6 in the infected patient group. The fever was well controlled in most of the patients, with only 15 patients having a temperature >100°F and only 2 patients having above 102°F, with a mean value of 98.54°F.
The associations of various factors affecting the end outcome in ICU patients were determined using chi-squared test. These associations are provided in .
Table 6 Clinical variables and their associations with end outcomes in ICU patients
It was found that patients treated with appropriate antibiotics were discharged from the hospital. CST was performed in 19 patients; but due to various other factors including renally compromised state of the patients, 17 (89.5%) died at the end of treatment. Renal dose adjustment is necessary in renally compromised patients, but it was not performed in 77 (89.5%) patients and all of them died at the end. Steroids should be used with caution in renally compromised patients,Citation18 and in our study, 52 (91.2%) patients who were on steroid therapy died.
It was observed that major drug–drug interactions including fatal particulate precipitation occurred in the lungs due to co-administration of ceftriaxone along with calcium-containing intravenous solutions.Citation19 Since drug therapy was not reviewed by any specialized clinical pharmacist, drug– drug interactions could not be reported, thus leading to high mortality rate.
An overall 83% mortality rate was observed in this study, while the mortality rate among various specified clinical conditions is provided in and .
Table 7 Mortality rate in various clinical scenarios
Figure 2 Mortality rate (%) in various clinical scenarios.
Abbreviation: CST, culture sensitivity test.
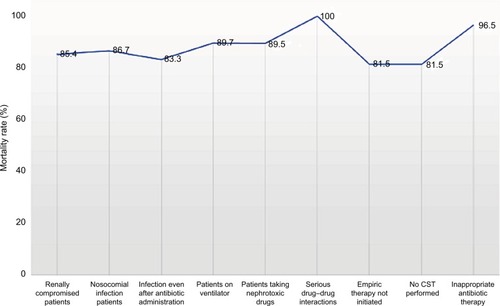
It was observed that the mortality rate was affected by inappropriate use of antibiotics, failure to perform renal dose adjustments, presence of major drug–drug interactions, and use of nephrotoxic drugs without any control or dose adjustments.
Discussion
In the current study, empiric therapy with broad-spectrum antibiotics was administered in 68% of the patients. Since all ICU patients are at high risk for developing infections due to intense pathological/surgical conditions, all measures are usually taken to prevent the spread of infection.Citation20 The hospital under study caters for the medical needs of ~6–7.5 million population,Citation21 and due to high patient influx, the hygienic conditions were poor and proper sterilization and disinfection could not be attained at all levels.Citation22,Citation23 Certain previous studies have also reported the use of empiric antibiotic therapy in the ICU when the hygienic conditions are poor.Citation24–Citation26 Before initiation of empiric antibiotic therapy, samples for CST were drawn in very few, that is, only 7%, patients. CST samples can give false results if empiric antibiotic therapy has been initiated. After the results of CST were obtained, antibiotic therapy was modified in only 13% of patients, that too, without following the principles of de-escalation, which are very important to consider while treating patients with acute infections.Citation12 The frequency of nosocomial infections in our study was found to be 30%, with the highest number of infections (ie, 34.5%) associated with ventilator since they are most difficult to manage.Citation27,Citation28 The frequency of ventilator-acquired nosocomial infection in our study was quite similar with previously reported data in Pakistan.Citation29 The practice of initiating empiric antimicrobial therapy among ICU patients was found to be associated with reduction in incidence of nosocomial infections, since none of the patients undergoing empiric therapy developed nosocomial infection. This practice was in accordance with previously reported benefits from initiation of empiric therapy in reducing nosocomial infection.Citation24 Since there was no antibiotic control or stewardship program in this hospital and none of the prescribed therapy was reviewed by infectious disease specialist or clinical pharmacist specialized in infectious diseases, appropriate therapy was prescribed in only 14% of patients, which is very low as compared to already reported data,Citation30 while the drug therapy in the remaining 86% of patients had errors such as inappropriate drug or dose selection, serious interactions, and unwanted adverse reactions.
In this study, overall, 83% mortality rate was observed, which is very high as compared to previously reported literature.Citation31 Mortality rate among patients with nosocomial infection was found to be 89.7%, which is quite high as compared to previous literature data.Citation32,Citation33 Very high mortality rate (85.4%) was observed in renally compromised patients prescribed with potentially nephrotoxic drugs as compared to previously reported studies.Citation34,Citation35 Among patients for whom appropriate antibiotics were not prescribed in adequate doses, a mortality rate of 96.5% was observed, which is very high as compared to previous study reports.Citation36 This high mortality rate, especially with inappropriate use of antibiotics, is a point of concern and should be addressed with appropriate measures by the concerned authorities.
High mortality rates, poor clinical outcomes, and poor hygienic conditions were observed among ICU patients of the largest tertiary care hospital of the capital city of Pakistan, which indicates lack of interest and commitment of higher officials and policymakers. Regardless of such high mortality rates, no measures for infection control have been taken and no protocols for antibiotic prescribing have been developed. The spread of infections and resistant strains is also putting health care providers at risk.
Conclusion
Empiric antibiotic therapy is beneficial in patients and leads to reduction in mortality rate. Irrational antibiotic prescribing along with co-administration of contraindicated drugs and use of nephrotoxic drugs without dose adjustments were found to be associated with high mortality rate and poor clinical outcomes. Medication review under the supervision of clinical pharmacist specialized in intensive care can help reduce various factors affecting mortality rate. Antibiotic control programs including stewardship and prescribing under the supervision of infectious disease specialist can further help to improve clinical outcomes and reduce mortality. It is time that health authorities of the capital of Pakistan take serious measures to control the mortality rate by implementing stewardship program, hiring competent infectious disease specialist and clinical pharmacists specialized in infectious disease, and training the medical staff regarding use and deescalation of antibiotic therapy.
Disclosure
The authors report no conflicts of interest in this work.
References
- JarvisWRSelected aspects of the socioeconomic impact of nosocomial infections: morbidity, mortality, cost, and preventionInfect Control Hosp Epidemiol19961785525578875302
- MauldinPDSalgadoCDHansenISDurupDTBossoJAAttributable hospital cost and length of stay associated with health care-associated infections caused by antibiotic-resistant gram-negative bacteriaAntimicrob Agents Chemother201054110911519841152
- DucelGFabryJNicolleLPrevention of Hospital-Acquired Infections: A Practical Guide2nd edGenevaWorld Health Organization2002
- SarrafDPhunyalbMMandalsMRauniarGUtilization pattern of antimicrobial agents and its culture sensitivity pattern in intensive care units in a tertiary care center in eastern NepalNepal Med Coll J2015173–4107112
- EmmersonMAntibiotic usage and prescribing policies in the intensive care unitIntensive Care Med2000261S026S030
- CockcroftDWGaultHPrediction of creatinine clearance from serum creatinineNephron197616131411244564
- StaffPDRPhysicians’ Desk Reference66th edNew YorkThomson Healthcare2011
- Royal Pharmaceutical SocietyMedicinesComplete [homepage] Available from: https://about.medicinescomplete.com/Accessed June 7, 2016
- GolightlyLKRenal pharmacotherapyDosage Adjustment of Medications Eliminated by the KidneysNew YorkSpringers2003
- PrestonCLStockley’s drug interactionRoyal Pharmaceutical SocietyLondonPharmapress2015
- FarrukhMJHishamSABin ZainalZAPharmaceutical care issues in patients with atrial fibrillation receiving thromboprophylaxisAm J Pharmacol Sci20145B1216
- MastertonRGAntibiotic de-escalationCrit Care Clin201127114916221144991
- GarnerJSJarvisWREmoriTGHoranTCHughesJMCDC definitions for nosocomial infections, 1988Am J Infect Control19881631281402841893
- UdyAARobertsJALipmanJClinical implications of antibiotic pharmacokinetic principles in the critically illIntensive Care Med201339122070208224045886
- RobertsJALipmanJAntibacterial dosing in intensive careClin Pharmacokinet200645875577316884316
- MahmoodIInterspecies scaling of renally secreted drugsLife Sci19986326236523719877226
- HighKPBradleySFGravensteinSClinical practice guideline for the evaluation of fever and infection in older adult residents of long-term care facilities: 2008 update by the infectious diseases Society of AmericaClin Infect Dis200948214917119072244
- PazhayattilGSShiraliACDrug-induced impairment of renal functionInt J Nephrol Renovasc Dis2014745725540591
- MurneyPTo mix or not to mix – compatibilities of parenteral drug solutionsAust Prescr200831498101
- ErogluAFactors impacting the likelihood of death in patients in intensive care unitInt J Anesthesiol Res201644225228
- 6th Population & Housing Census 2017, Bureau of Statistics Pakistan Available from: http://www.pbscensus.gov.pk/Accessed March 15, 2018
- IkramAHussain ShahSINaseemSStatus of hospital infection control measures at seven major tertiary care hospitals of northern PunjabJ Coll Physicians Surg Pak201020426627020392405
- AkhtarNHospital acquired infections in a medical intensive care unitJ Coll Physicians Surg Pak201020638639020642968
- KollefMAppropriate empirical antibacterial therapy for nosocomial infections: getting it right the first timeDrugs200363202157216814498753
- BorCDemiragKOkcuOCankayaliIUyarMVentilator-associated pneumonia in critically ill patients with intensive antibiotic usagePak J Med Sci2015316144126870112
- MalikMIAntimicrobial susceptibility pattern of bacteria isolated from tracheal secretions in intensive care units admitted patients of Lahore General HospitalPak J Chest Med20182427277
- KalanuriaAAZiaiWZaiWMirskiMVentilator-associated pneumonia in the ICUCrit Care201418220825029020
- MaqboolMShabirANaqashHAminAKoulRKShahPVentilator associated pneumonia – incidence and outcome in adults in medical intensive care unit of a tertiary care hospital of North IndiaInt J Sci Study20174107376
- ShaikhJMDevrajaniBRShahSZAkhundTBibiIFrequency, pattern and etiology of nosocomial infection in intensive care unit: an experience at a tertiary care hospitalJ Ayub Med Coll Abbottabad2008204374019999200
- BaqiSDamaniNNShahSAKhananiRInfection control at a government hospital in PakistanInt J Infect Control20095117
- RosenthalVDGuzmanSOrellanoPWNosocomial infections in medical–surgical intensive care units in Argentina: attributable mortality and length of stayAm J Infect Control200331529129512888765
- PittetDTararaDWenzelRPNosocomial bloodstream infection in critically ill patients, excess length of stay, extra costs, and attributable mortalityJ Am Med Assoc19942712015981601
- Bueno-CavanillasADelgado-RodríguezMLópez-LuqueASchaffino-CanoSGálvez-VargasRInfluence of nosocomial infection on mortality rate in an intensive care unitCrit Care Med199422155608124975
- MandelbaumTScottDJLeeJOutcome of critically ill patients with acute kidney injury using the acute kidney injury network criteriaCrit Care Med201139122659266421765352
- OstermannMChangRRiyadh ICU Program Users GroupRenal failure in the intensive care unit: acute kidney injury compared to end-stage renal failureCrit Care200812543218983713
- PradhanNPBhatSMGhadageDPNosocomial infections in the medical ICU: a retrospective study highlighting their prevalence, microbiological profile and impact on ICU stay and mortalityJ Assoc Physicians India201462101821