
Abstract
Background
Since coronavirus disease 2019 emergence, millions were infected and many were dying because of the virus. Clinical features and time to recovery of admitted clients vary across settings. Therefore showing clinical features and recovery time from COVID-19 in a different setting is necessary to design appropriate treatment and preventive measures. So, this study attempted to investigate the clinical features and time to recovery of admitted clients to Dilla University Referral Hospital treatment center, Ethiopia.
Methods
A retrospective study design was conducted in 220 patients confirmed by real time polymerase chain reaction and admitted to Dilla University Referral Hospital treatment center from September 2020 to July 2021. Data were collected from the patients’ record. Data entry was done by an Epi-Info version 7.2.1.0 and analyzed by Statistical Package for the Social Sciences version 25 software. Descriptive statistics were used for clinical features, and median time to recovery was computed by using Kaplan–Meier.
Results
Common clinical features were cough 209 (95%), shortness of breath 153 (69.5%), fever 133 (60.5%), headache 75 (34.1%), easy fatigue 68 (30.9%), joint pain 56 (25.5%), tachypnea 197 (89.5%), hypoxia 95 (43.2%), and tachycardia 83 (37.7%). The overall median recovery time for admitted cases was 5 days. There was significant difference between recovery probability of severe and moderate cases, severe and mild cases (p=0.00), who had normal body temperature and hypothermic (p=0.05), who had normal breathing rate and bradypnea patients (p= 0.014).
Conclusion
COVID-19 patients frequently show cough, shortness of breath, fever, headache, easy fatigue and joint pain. Median time to recovery was 5 days. Having a normal body temperature, normal breathing rate, and severe disease status had statistically significant association with median recovery time. So, close follow up is required for client admitted with severe disease.
Keywords:
Introduction
Coronaviruses are enveloped RNA viruses that infect humans and other animals. They were first described in 1966 by Tyrell and Bynoe.Citation1 The virus changes over time and some changes may affect the virus properties. Due to this change, different sub-families of the virus are emerging: alpha (B.1.1.7), beta (B.1.351), gamma (P.1) and delta (B.1.617.2) exist. Alpha and beta‐coronaviruses originate from mammals, in specific from bats,Citation2 while gamma and delta are from pigs and birds.Citation3,Citation4 Beside four variants, on November 24, 2021 the B.1.1.529 commonly called an Omicron variant of Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) virus that contains a high number of mutations was also detected.Citation5 These variants are now designated by the World Health Organization (WHO) as SARS-CoV-2 variants of concern.Citation6 There are also other variants named variants of interest, that include Epsilon variant, Zeta variant, Eta variant, Theta variant, Iota variant and Kappa variant.Citation7 The virus spread from human to human by droplets and contact routes, but some uncertainty about airborne, there is also fecal or intrauterine transmission.Citation8 Various SARS-CoV-2 variants are detected since the first covid-19 cases emerged in Wuhan, like that detected in United Kingdom (UK), South Africa, Brazil.Citation9,Citation10 The emerging variants appear to be more communicable than the wild-type SARS-CoV-2 that contains mutations in the spike protein, urging vaccine efficacy concerns.Citation11 Although some studies indicated no significant differences between the case fatality ratio of Delta and non-Delta variants,Citation12 but still not much is known about these variants.Citation13 The vaccine efficacy could be influenced by the emergence of new SARS-CoV-2 variants with a major antigenic drift. Some recent reports indicated that the harmful effect of RNA binding motive (RBM) mutations on the neutralization activity of vaccine-elicited antibodies.Citation14
Forty percent of people with COVID-19 develop only mild or moderate disease, while approximately 15% develop severe disease and 5% develop critical disease complications like respiratory failure, acute respiratory distress syndrome (ARDS), sepsis and septic.Citation15 Most of them show fever (83–99%), cough (59–82%), fatigue (44–70%), anorexia (40–84%), shortness of breath (31–40%), myalgia (11–35%),Citation16 other non-specific symptom like a sore throat, nasal congestion, headache, diarrhea, nausea and vomiting.Citation17
Age more than 60 years, underlying co-morbidities like diabetes, hypertension, cardiac disease, chronic lung disease, cerebrovascular disease, chronic kidney disease, immunosuppression and cancer have been associated with higher death and time to recovery.Citation18–21 The recovery time varies from person to person and affected by the severity of the disease.Citation22 Its case fatality rate was 6.3%, but it is different in different ages and countries.Citation23,Citation24 It shows the very strong risk stratification across age, socioeconomic factors, and clinical factors.Citation25–27 Long-term social isolation due to the COVID-19 infection sometimes leads to depression and post-traumatic stress.Citation28
SARS-CoV-2 has now spread to many other countries,Citation29 as a result Artificial Intelligence-driven tools should be implemented as cross-population train (test) model.Citation30 The collective number of cases reported worldwide is now nearly 216 million and the collective number of deaths is just 4.5 million.Citation31 Over 2.7 million new cases were reported globally, the Americas and Europe account for about 80% of new cases and new deaths reported worldwide, while it shows 10% prevalence in Africa.Citation32 There have been more than three hundred thousand confirmed cases of COVID-19 with more than five thousand deaths in Ethiopia.Citation33 The surge is increasing on international and local levels, causing rapid loss of life, joblessness, the decline of the healthcare systems, and both local and international economies.Citation34 Susceptibility to COVID-19 infection seems high across Ethiopia, mainly in Somali, Afar, Amhara, Oromia and Tigray regions.Citation35 The number of severe cases requiring admission to the Hospital and intensive care unit is high across Amhara, most parts of Oromia and some parts of the Southern Nations, Nationalities and Peoples’ Region.Citation36 The risk of COVID-19-related death is also high in the country’s border regions, where public health readiness is limited.Citation35,Citation37
The virus entry into human cell is mediated by the trimeric viral Spike glycol-protein that contains the exterior S1 and trans-membrane S2 subunits. The Spike is the main target of the cellular and humoral immune responses against SARSCoV-2 upon natural infection.Citation9,Citation38 Long lasting immune protection involves antibodies that recognize the viruses and neutralize them; different types of T cells that kill the pathogen.Citation39 Even though all immune components have been found in people who recover from this virus, sufficient information about immune response and how long it lasts after infection is unknown.Citation40 Most importantly, reports of reinfection with the virus have raised concerns that the immune response to it might not be durable.Citation41,Citation42 The appearance of new variants with the different capacity to evade polyclonal antibody responses could possibly lead to a rising number of reinfections.Citation9,Citation43,Citation44 Preventive measures for COVID-19 that include vaccination, wearing masks and social distancing are vital mainly for older or those who have several or severe health conditions. Some scientific research has been done in many features of COVID-19, but still need localized valid and reliable information is needed in order to intervene properly. Different studies have shown different median recovery time of COVID-19 admitted patients and it varies across disease status.Citation45 So, this study attempted to describe baseline clinical features and time to recovery of COVID-19 cases admitted to Dilla University Referral Hospital treatment center.Citation19
Methods and Materials
Operational Definitions
Time to recovery is the time when the patients were diagnosed positive for COVID19 to the time when the patients diagnosed negative by RT-PCR by two consecutive tests and being free of symptoms after admission to the Hospital. The event was recovery from the disease, while censored were the patients who were not developed an event; those who died or transferred out during the study period. Mild cases were symptomatic patients without evidence of viral pneumonia or hypoxia, moderate were the cases with clinical signs of non-severe pneumonia while severe cases were the cases with clinical signs of severe pneumonia like fever, cough, dyspnea and respiratory rate >30 breaths/minute or SPO2 <90%.
Data Collection
This study was conducted at the Dilla University Referral Hospital, South Ethiopia. A retrospective study design was used for all 220 COVID-19 confirmed patients by RT-PCR; who were admitted to Dilla University Referral Hospital treatment center from September 2020 to July 2021. All data related to socio-demographic information, clinical features and co-morbidities were collected from the patients’ record. General practitioners and Nurses who were working at treatment center were trained and then collected the data from the patients’ record.
Data Analysis
Data entry was done by an Epi-Info version 7.2.1.0 and analysis was done by Statistical Package for the Social Sciences (SPSS) version 25 software. Descriptive statistics were used for socio-demographic factors and clinical features, and median time to recovery was done by using Kaplan-Meier method. The cox regression analysis was used to determine factors associated with time to recovery for hospitalized COVVID-19 patients.
Ethical Approval
Ethical approval and waiver consent was obtained from the Institutional Review Board (IRB) of the Dilla University College of Medicine and Health sciences under the protocol unique number of duirb/002/21-10 before the data collection. The consent to participate in the study was not applicable because the study was retrospective and was conducted on the data collected from the patients’ medical records. Therefore, it was difficult to obtain consent from already discharged patients from the Hospital. However, the privacy and confidentiality of their personal information were protected according to ethical principles for medical research involving human subjects of the World Medical Association Declaration of Helsinki.
Results
Socio-Demographic Factors
Out of 220 study cases, 113 (51.4%) of them were above 50 years of age, and the mean age was 47 years. Most of the cases 123 (55.9%) were male, and house wife accounted for the largest number of cases 47 (21.4%) followed by unemployment 41 (18.6%), Government employees 31 (14.1%), farmers 30 (13.6%), self-employed 28 (12.7%), merchants 20 (9.1%) and students (6.8%) ().
Table 1 Socio-Demographic Factors of Hospitalized COVID-19 Patients (n=220) to Dilla University Referral Hospital, December 2021
Clinical Features and Co-Morbidity with Chronic Diseases
The most common clinical symptoms were cough 209 (95%), shortness of breath 153 (69.5%), fever 133 (60.5%), headache 75 (34.1%), easy fatigue 68 (30.9%) and joint pain 56 (25.5%). Most cases had tachypnea 197 (89.5%), while the others had hypoxia 95 (43.2%), tachycardia 83 (37.7%), and hypertension 36 (16.4%). Of all cases, 120 (54.5%) were severe, 89 (40.5%) were moderate and 11 (5.0%) were mild.
Among 133 (60.5%) cases that had chronic diseases, 27.3% were hypertensive, 20.9% had type II Diabetes Mellitus, 14.5% had Tuberculosis, 6.8% had Cardiac disease, 4.1% had renal disease, 2.3% were Asthmatic patients, 1.8% had (Human Immuno-Virus) HIV, 0.9% had type I Diabetes Mellitus, and 0.9% had chronic liver disease, 0.5% had prostate cancer, advanced cervical cancer, chronic lymphocytic leukemia, severe Diabetes keto-acidosis (DKA) respectively.
Of the 220 study cases, 167 (75.9%) cases were improved while 49 (22.3%) of them were died. Twenty nine (59.2%) of died cases were beyond the age of 50+ years while 11 (22.4%) were between the age group of 30–49 years and 9 (18.4%) were <30 years. Out of 220 admitted COVID-19 cases, 49 reported died, and of them, males accounted for 28 (57.1%) while the females were 21 (42.9%). Likewise, 31 (63.3%) had fever, 2 (4.1%) were hypothermic, 27 (55.1%) were tachycardia, 1 (2.0%) were bradycardic, 45 (91.8%) were tachypnea, 2 (4.1%) were bradypnea, 9 (19.1%) were hypertensive, 6 (12.8%) were hypotensive. Of the 32 (65.3%) that had a chronic disease, type II Diabetes mellitus (DM) accounted 10 (20.4%) and the others had cardiac disease 3 (6.1%), renal disease 1 (2.0%), Tuberculosis 7(14.3%), type 1 DM 2(4.1%), HIV 1 (2.0%), chronic lymphocytic leukemia 1 (2.0%). Most of the COVID-19 died cases that had co-morbidity with chronic diseases were severe 48 (98.0%), and the moderate 1 (2%) while 37 (75.5%) were with hypoxia.
Among 165 improved cases, 80 (48.5%) were beyond the age group of 50 years while 57 (34.5%) were between 30–49 and 28 (17.0%) were <30 years, and 96 (58.2%) were male. Of them, 101 (61.2%) had fever and 54 (32.7%) were tachycardia, 148 (89.7%) were tachypnea, 26 (16.3%) were hypertensive, 99 (60.0%) had chronic diseases: 12 (7.3%) had cardiac disease, 7 (4.2%) had renal disease, 25 (15.2%) had Tuberculosis, 35 (21.2%) had type II DM. 55 (33.3%) hypoxia, 70 (42.4%) were severe, 85 (51.5%) were moderate and 10 (6.1%) were mild cases (). The mean length of stay at Hospital was 5.65 (range, 1 to 30) days while it was 5.55 (range, 1 to 25) days for improved cases and 6.06 (1 to 30) days for died cases. Furthermore, the severe cases stay longer at Hospital than mild cases (AHR=0.356, p=0.002).
Table 2 Clinical Features of Hospitalized COVID-19 Patients (n=220) to Dilla University Referral Hospital, December 2021
Time to Recovery of COVID-19 Cases
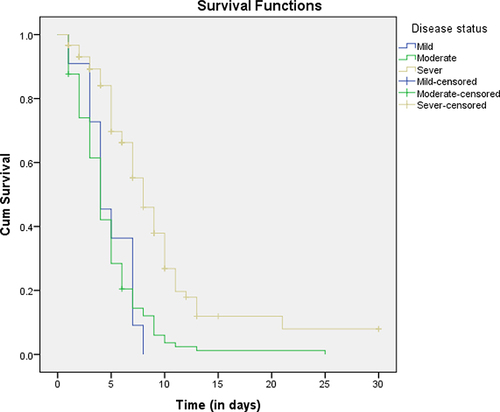
The overall median recovery time for admitted COVID-19 patients was 5 days. It was 8 days for severe cases, 4 days for moderate and mild cases. The Kaplan-Meier and Log rank test showed that there was a significant difference between recovery probability of severe and moderate cases, severe and mild cases (p=0.00). However, there was no significant difference between the recovery probability of moderate and mild cases (p=0.91), ().
Figure 1 Recovery of COVID-19 patients admitted to the Dilla University Referral Hospital Treatment Center by disease status at admission.
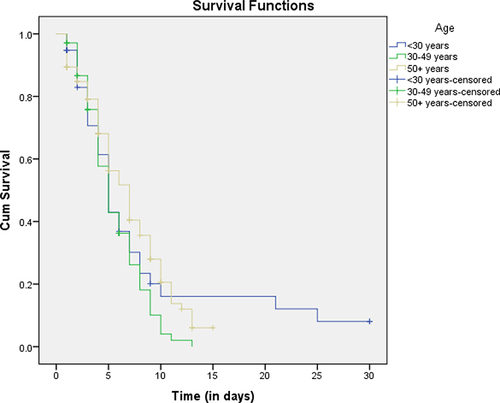
The median recovery time for the COVID-19 patients that had co-morbidity with chronic diseases was 6 days while it was 5 days for cases that had no chronic diseases. Furthermore, the Kaplan-Meier and Log rank test showed a statistically significant recovery probability difference between these cases (p=0.015), (). The median recovery time for female and male was 6 and 5 days respectively, with the overall 6 days median time. There was no statistically significant recovery probability difference between male and female (p=0.34), (). The median recovery time for <30, 30–49 and 50+ year age groups was 5, 5, and 7 days respectively. On the other hand, there was statistically significant recovery probability difference between the age group of above 50 and 30–49 years (p= 0.01), while no significant difference observed with the other age group (p=0.69), ().
Figure 2 Recovery curve of COVID-19 patients admitted to the Dilla University Referral Hospital Treatment Center by co-morbidity with chronic diseases.
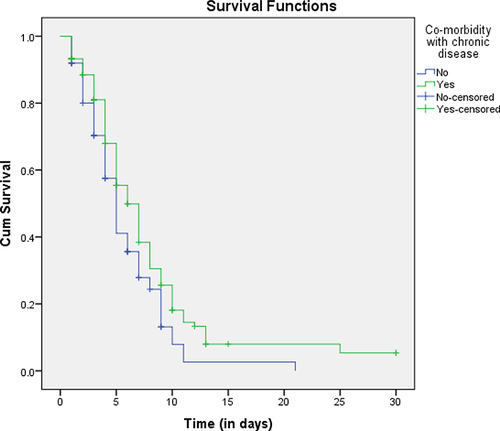
Figure 3 Recovery curve of COVID-19 patients admitted to the Dilla University Referral Hospital Treatment Center by sex.
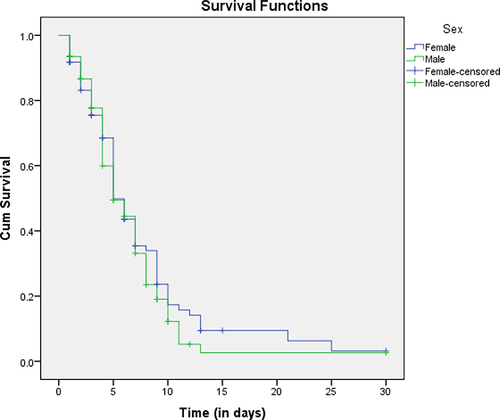
Figure 4 Recovery curve of COVID-19 patients admitted to the Dilla University Referral Hospital Treatment Center by age.
Factors Associated with Recovery Time of COVID-19 Cases
In bivariate co-regression analysis, factors like oxygen saturation, temperature, breathing rate, cough, easy fatigue, joint pain, co-morbidity with chronic disease, disease status showed a statistical association with median recovery time. However, by adjusting for confounders in multivariate cox-regression analysis, only having normal body temperature, breathing rate (normal), disease status (severe) remained statistically significant (AHR=0.52, 95% CI= 0.25–1.00, P=0.05), (AHR=5.37, 95% CI=1.40–20.57, p=0.014), and (AHR=0.33, 95% CI=0.16–0.6, P=0.002) respectively. That means that the patients who had a normal body temperature were 48% less recovery time as compared to those hypothermic clients. Furthermore, the patients who were detected with normal breathing rate had shorter recovery time than patients who showed bradypnea on admission time. Severe patients had longer recovery time as compared to those patients who had admitted with mild status ().
Table 3 Multivariate Cox-Regression Analysis Showing Adjusted Hazard Ratios of Clinical Features of COVID-19 Patients at Dilla University Referral Hospital, December 2021
Discussion
This study included all the 220 COVID-19 cases that were admitted to Dilla University Referral Hospital Covid-19 treatment center. The majority of the study cases were male (55.9%) and most of the study cases were above 50 years, and the mean age was 47 years. COVID-19 infected patients frequently show clinical symptoms like fever, cough, myalgia and shortness of breath and sore throat,Citation46,Citation47 and some may do not experience any symptom.Citation48 Similarly, our study indicated that the most common clinical symptoms were cough 209 (95%), shortness of breath 153 (69.5%), fever 133 (60.5%), headache (34.1%), easy fatigue (30.9%) and Joint pain (25.5%). This is high as compared to the study done in Kuyha COVID-19 Isolation and Treatment Centre, Mekelle University, North Ethiopia, where cough 354 (50.6%), myalgia 212 (31.1%), headache 196 (28.7%), fever 161 (23.6%) stated as the most frequently observed clinical symptoms.Citation49 Most importantly, the majority of the patients were also shown tachypnea (89.5%) hypoxia (43.2%), tachycardia (37.7%). This finding is lower than the study done in Addis Ababa, Ethiopia, which stated that hypoxia (60.5%) and tachycardia (52.9%),Citation16 were the major clinical features; even though tachypnea (89.5%) was also shown common in our study. This is may be due to the sample size difference.
Our findings also indicated that the most common co-morbidities of the COVID-19 patients were hypertension (27.3%), type II Diabetes Mellitus (20.9%), Tuberculosis (14.5%), chronic heart disease (6.8%), renal disease (4.1%), Asthma (2.3%) and HIV (1.8%) which is higher than the other study done in Ethiopia that showed hypertension (1.6%), HIV (1.6%), diabetes (1.1%), and chronic respiratory diseases (1.1%) were the main co-morbidities noted;Citation48 but lower than the study that suggested COVID-19 admitted cases had hypertension (45%), DM (30%) and cardiovascular (20%) diseases,Citation50 and also different the that suggested the most common comorbidity was DM, followed by hypertension and HIV.Citation16 This difference may be due to the sample size and age of the participants where most of current study cases were above 50 years.
On arrival to treatment center, most of the cases (79.2%) were severe to critical, while the rest (20.8%) were asymptomatic to mild.Citation16 In our study, however, 54.5% were severe, 40.5% were moderate and 5.0% were mild. This means most of the cases were severe and moderate, which also differ from the study done at the Bokoji Hospital COVID-19 treatment center that stated most of the admitted covid-19 cases were severe (36.5%), asymptomatic (22.5%) and mild (21.6%).Citation51 We also showed most of the cases (75.9%) were improved and 22.3% were died. Which is consistent with another study in Ethiopia that showed most of the admitted cases were improved (88.9%), while some of them died in the facility (11.1%).Citation51
Our findings also stated that 49/220 cases were died and most of died cases (59.2%) were beyond the age of 50 years while 22.4% were between 30–49 years and 18.4% were <30 years. Furthermore, 57.1% of died cases were males. This is higher than the study in Brazil that suggested most deaths occurred in males (55.4%).Citation52 This result is however, lower for males, but higher for females than the study done in Ethiopia that showed most deaths, 71% were males and 29% were females,Citation16 even though in both studies the number of died males were higher than females. This is may be due to Biological and sample size differences.
The overall median recovery time for treatment center admitted COVID-19 cases was 5 days. This is lower than the finding of the previous study that suggested the overall median recovery time of COVID-19 patients during treatment was 24 days.Citation51 This result is also different from result stated by the study done at the Wollega University Referral Hospital, which is 18 days.Citation53 This difference may be due to sample size, socio-demographic factors and severity of the disease. It was 8 days for severe cases, 4 days for moderate and mild cases. This indicates that it takes longer time to recover for severe cases than moderate and mild cases, which is consistent (in case of severe cases) with the previous study that stated the time needed for recovery was longer among patients with non mild disease (moderate and severe),Citation54 even though in our study both moderate and mild had the same median time. Furthermore, the severe cases stay longer at the treatment center than mild cases (AHR=0.356, p=0.002). There was statistically significant difference between recovery probability of severe and moderate cases, severe and mild cases (p=0.00). However, there was no significant difference between the recovery probability of moderate and mild cases (p=0.91).
Furthermore, the median recovery time for the Covid-19 patients that had co-morbidity with chronic diseases was 6 days while it was 5 days for cases that had no chronic diseases, and they have statistically significant recovery probability difference (p=0.015). This is different from the study done in Ethiopia at Millennium COVID-19 care center that stated the recovery time did not show statistically significant difference between those patients who had pre-existing co-morbidity and who do not have.Citation54 This may be due to the co-morbidity type difference between the two study cases.
Limitation
Since our study was a retrospective study, we used secondary data. We used also low sample sample size and we analyzed only base line data. So, further study should be done with full follow up data.
Conclusion
COVID-19 infected patients frequently show clinical symptoms such as cough, shortness of breath, fever, headache, easy fatigue and Joint pain. The majority of the patients were also shown tachypnea, hypoxia and tachycardia. The most common co-morbidities of the COVID-19 patients were hypertension, type II DM, Tuberculosis, Cardiac disease, renal disease and Asthma. On arrival to the treatment center, most of the cases were severe, and also there were many moderate cases while few of them were mild. Having a normal body temperature, normal breathing rate, and severe disease status had statistically significant association with median recovery time. COVID-19 patients who had co-morbidity with chronic diseases and those that had no chronic diseases had statistically significant recovery probability difference. There was also statistically significant recovery probability difference between the age group of above 50 and 30–49 years. So, close follow up is required for patients admitted with severe disease status, even though all COVID-19 cases need care. These findings could help in designing of appropriate management strategy for patients under treatment.
Abbreviations
AHR, adjusted hazard ratio; ARDS, acute respiratory distress syndrome; CHR, crude hazard ratio; COPD, chronic obstructive pulmonary disease; COVID-19, coronavirus disease 2019; DM, diabetes mellitus; HIV, human immuno-virus; IRB, Institutional Review Board; LDH, lactate dehydrogenase; MI, myocardial infarction; RBM, RNA binding motive; RT-PCR, real time polymerase chain reaction; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2; SNNPR, Southern Nations, Nationalities, and Peoples Region; SPSS, Statistical Package for the Social Sciences; UK, United Kingdom.
Ethics Approval and Consent to Participate
Ethical approval and waiver consent was obtained from the Institutional Review Board (IRB) of the Dilla University College of Medicine and Health sciences under the protocol unique number of duirb/002/21-10, and the permission from treatment center record room for data collection.
Data Sharing Statement
The datasets used during this study are available from the corresponding author when required.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execusion, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountale for all aspects of the work.
Disclosure
The authors declare that they have no conflicts of interest for this work.
Acknowledgments
We would like to thank the Dilla University Referral Hospital COVID-19 treatment center and Patients’ record room staffs for their cooperation. Our great thanks also extend to Dilla University College of Health Science and Medicine for supporting us to conduct this research.
Additional information
Funding
References
- Tyrrell D, Bynoe M. Cultivation of viruses from a high proportion of patients with colds. Lancet. 1966;287:76–77. doi:10.1016/S0140-6736(66)92364-6
- Morens DM, Breman JG, Calisher CH, et al. The origin of COVID-19 and why it matters. Am J Trop Med Hyg. 2020;103(3):955. doi:10.4269/ajtmh.20-0849
- Zhou P, Yang X-L, Wang X-G, et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature. 2020;579(7798):270–273. doi:10.1038/s41586-020-2012-7
- Naserghandi A, Allameh S, Saffarpour R. All about COVID-19 in brief. New Microbes New Infect. 2020;35:100678. doi:10.1016/j.nmni.2020.100678
- Jansen L, Tegomoh B, Lange K, et al. Investigation of a SARS-CoV-2 B.1.1.529 (Omicron) variant cluster —Nebraska, November–December 2021. Morbid Mortal Wkly Rep. 2016;70:28–36.
- Petersen E, Ntoumi F, Hui DS, et al. Emergence of new SARS-CoV-2 variant of concern Omicron (B. 1.1. 529)-highlights Africa’s research capabilities, but exposes major knowledge gaps, inequities of vaccine distribution, inadequacies in global COVID-19 response and control efforts. Int J Infect Dis. 2022;114:268–272. doi:10.1016/j.ijid.2021.11.040
- Parums DV. Revised World Health Organization (WHO) terminology for variants of concern and variants of interest of SARS-CoV-2. Med Sci Monit. 2021;27:e933622–1. doi:10.12659/MSM.933622
- Rothan HA, Byrareddy SN. The epidemiology and pathogenesis of coronavirus disease (COVID-19) outbreak. J Autoimmun. 2020;109:102433. doi:10.1016/j.jaut.2020.102433
- Prevost J, Finzi A. The great escape? SARS-CoV-2 variants evading neutralizing responses. Cell Host Microbe. 2021;29(3):322–324. doi:10.1016/j.chom.2021.02.010
- Davies NG, Abbott S, Barnard RC, et al. Estimated transmissibility and severity of novel SARS-CoV-2 Variant of Concern 202012/01 in England. 2021.
- Rita Rubin M. COVID-19 vaccines vs variants—determining how much immunity is enough. JAMA. 2021;325(13):1241–1243.
- Zhao S, Lou J, Cao L, et al. Differences in the case fatality risks associated with SARS-CoV-2 Delta and non-Delta variants in relation to vaccine coverage: an early ecological study in the United Kingdom. Infect Genet Evolut. 2022;97:105162. doi:10.1016/j.meegid.2021.105162
- Shiehzadegan S, Alaghemand N, Fox M, Venketaraman V. Analysis of the Delta Variant B.1.617.2 COVID-19. Clin Pract. 2021;11:778–784. doi:10.3390/clinpract11040093
- Wang Z, Schmidt F, Weisblum Y, et al. mRNA vaccine-elicited antibodies to SARS-CoV-2 and circulating variants. bioRxiv. 2021;592(7855):616–622.
- Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72,314 cases from the Chinese Center for Disease Control and Prevention. JAMA. 2020;323(13):1239–1242. doi:10.1001/jama.2020.2648
- Sultan M, Kene D, Waganew W, et al. Clinical characteristics of COVID-19 related deaths in Ethiopia. Ethiop J Health Sci. 2021;31(2):223–228. doi:10.4314/ejhs.v31i2.3
- FMOH E. National Comprehensive Covid19 Management Handbook. Ethiopian Federal Ministry of Health; 2020.
- Abrahim SA, Tessema M, Defar A, et al. Time to recovery and its predictors among adults hospitalized with COVID-19: A prospective cohort study in Ethiopia. PLoS ONE. 2020;15(12):e0244269. doi:10.1371/journal.pone.0244269
- CDC. COVID-19; Your Health; People with certain medical conditions; August 20, 2021. Available from: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/people-with-medical-conditions.html. Accessed February 27, 2022.
- Bhaskaran K, Bacon S, Evans SJ, et al. Factors associated with deaths due to COVID-19 versus other causes: population-based cohort analysis of UK primary care data and linked national death registrations within the OpenSAFELY platform. Lancet Region Health Europe. 2021;6:100109. doi:10.1016/j.lanepe.2021.100109
- World Health Organization. Public Health Surveillance for COVID-19: Interim Guidance, 7 August 2020. World Health Organization; 2020.
- Bhapkar HR, Mahalle PN, Dey N, Santosh KC. Revisited COVID-19 mortality and recovery rates: are we missing recovery time period? J Med Syst. 2020;44(202). doi:10.1007/s10916-020-01668-6
- Bulut C, Kato Y. Epidemiology of COVID-19. Turk J Med Sci. 2020;50(SI–1):563–570. doi:10.3906/sag-2004-172
- Wu J, Mafham M, Mamas MA, et al. Place and underlying cause of death during the COVID-19 pandemic: retrospective cohort study of 3.5 million deaths in England and Wales, 2014 to 2020. Mayo Clinic Proceedings; 2021: Elsevier.
- World Health Organization. Population-Based Age-Stratified Seroepidemiological Investigation Protocol for COVID-19 Virus Infection, 17 March 2020. World Health Organization; 2020.
- Adams ML, Grandpre J, Katz DL. Updated estimates of comorbidities associated with risk for COVID-19 complications based on US data [preprint]. medRxiv. 2020. doi:10.1101/2020.05.02.20088781
- Ioannidis JP. Global perspective of COVID‐19 epidemiology for a full‐cycle pandemic. Eur J Clin Invest. 2020;50(12):e13423. doi:10.1111/eci.13423
- Dey N, Mishra R, Fong SJ, Santosh KC, Tan S, Crespo RG. COVID-19: psychological and psychosocial impact, fear, and passion. Digit Govern Res Pract. 2020;2:1–4.
- Velavan TP, Meyer CG. The COVID‐19 epidemic. Trop Med Int Health. 2020;25(3):278. doi:10.1111/tmi.13383
- Santosh KC. AI-driven tools for coronavirus outbreak: need of active learning and cross-population train/test models on multitudinal/multimodal data. J Med Syst. 2020;44(93). doi:10.1007/s10916-020-01562-1
- WHO. Weekly epidemiological update on COVID-19–31 August 2021. 2021.
- WHO. Weekly Covid-19 report, 7 March 2021. 2021.
- WHO. Report of Covid-19 in Ethiopia, September 9, 2021. 2021.
- Haftom M, Petrucka P, Gemechu K, et al. Knowledge, attitudes, and practices towards covid-19 pandemic among quarantined adults in Tigrai region, Ethiopia. Infect Drug Resist. 2020;13:3727. doi:10.2147/IDR.S275744
- Alene KA, Gelaw YA, Fetene DM, et al. COVID-19 in Ethiopia: a geospatial analysis of vulnerability to infection, case severity and death. BMJ Open. 2021;11(2):e044606. doi:10.1136/bmjopen-2020-044606
- Shewasinad Yehualashet S, Asefa KK, Mekonnen AG, et al. Predictors of adherence to COVID-19 prevention measure among communities in North Shoa Zone, Ethiopia based on health belief model: a cross-sectional study. PLoS One. 2021;16(1):e0246006. doi:10.1371/journal.pone.0246006
- Gilbert M, Pullano G, Pinotti F, et al. Preparedness and vulnerability of African countries against importations of COVID-19: a modelling study. Lancet. 2020;395(10227):871–877. doi:10.1016/S0140-6736(20)30411-6
- Vankadari N, Wilce JA. Emerging COVID-19 coronavirus: glycan shield and structure prediction of spike glycoprotein and its interaction with human CD26. Emerg Microbes Infect. 2020;9(1):601–604. doi:10.1080/22221751.2020.1739565
- Spellberg B, Nielsen TB, Casadevall A. Antibodies, immunity, and COVID-19. JAMA Intern Med. 2020;24:460–462.
- Nalin D. Immunosenescence and SARS-CoV-2 vaccine development. J Infect Dis. 2020;222:2114. doi:10.1093/infdis/jiaa564
- WHO. What we know about the COVID-19 immune response. 2020.
- Iwasaki A. What reinfections mean for COVID-19. Lancet Infect Dis. 2021;21(1):3–5. doi:10.1016/S1473-3099(20)30783-0
- Jabbari P, Rezaei N. With risk of reinfection, is COVID-19 here to stay? Disaster Med Public Health Prep. 2020;14(4):e33–e. doi:10.1017/dmp.2020.274
- West J, Everden S, Nikitas N. A case of COVID-19 reinfection in the UK. Clin Med (Northfield Il). 2021;21(1):e52. doi:10.7861/clinmed.2020-0912
- Benoni R, Campagna I, Panunzi S, et al. Estimating COVID-19 recovery time in a cohort of Italian healthcare workers who underwent surveillance swab testing. Public Health. 2021;196:52e8. doi:10.1016/j.puhe.2021.05.014
- Yin Y, Wunderink RG. MERS, SARS and other coronaviruses as causes of pneumonia. Respirology. 2018;23(2):130–137. doi:10.1111/resp.13196
- Zhang H, Du F, Cao X-J, et al. Clinical characteristics of coronavirus disease 2019 (COVID-19) in patients out of Wuhan from China: a case control study. BMC Infect Dis. 2021;21(1):1–7. doi:10.1186/s12879-020-05706-z
- Alene G, Birhan A, Selamyhun T, Abebe G. Clinical characteristics of patients infected with SARS-CoV-2 in North Wollo Zone, North-East Ethiopia. Pan Afr Med J. 2021;38:217.
- Abraha HE, Gessesse Z, Gebrecherkos T, et al. Clinical features and risk factors associated with morbidity and mortality among patients with COVID-19 in northern Ethiopia. Int J Infect Dis. 2021;105:776–783. doi:10.1016/j.ijid.2021.03.037
- Rozenberg S, Vandromme J, Martin C. Are we equal in adversity? Does Covid-19 affect women and men differently? Maturitas. 2020;138:62–68. doi:10.1016/j.maturitas.2020.05.009
- Weya AK, Genemo GA, Hurrisa Z, Weya TK, Ali H, Hailu AD. Survival analysis of COVID-19 patients in Ethiopia: a hospital-based study [preprint]. PLoS One. 2021. doi:10.13140/RG.2.2.19298.86724
- Galvão MHR, Roncalli AG. Factors associated with increased risk of death from covid-19: a survival analysis based on confirmed cases. Revista Brasileira de Epidemiologia. 2021;23. doi:10.1590/1980-549720200106
- Tolossa T, Wakuma B, Seyoum Gebre D, et al. Time to recovery from COVID-19 and its predictors among patients admitted to treatment center of Wollega University Referral Hospital (WURH), Western Ethiopia: survival analysis of retrospective cohort study. PLoS One. 2021;16(6):e0252389. doi:10.1371/journal.pone.0252389
- Leulseged TW, Hassen IS, Maru EH, et al. Determinants of time to convalescence among COVID-19 patients at millennium COVID-19 care center in Ethiopia: a prospective cohort study [preprint]. medRxiv. 2020. doi:10.1101/2020.10.07.20208413