
Abstract
Non-communicable diseases (NCDs) are the leading cause of death globally, the majority of these being due to cardiovascular disease, cancer, chronic respiratory diseases, or diabetes. Mortality from many NCDs continues to increase worldwide, with a disproportionately larger impact in low-middle income countries (LMIs), where almost 75% of global deaths occur from these causes. As a low-income African country that consistently ranks amongst the world’s poorest nations, Malawi as a case study demonstrates how transition due to societal change and increasing urbanization is often accompanied by a rise in the rate of NCDs. Other factors apart from changing lifestyle factors can explain at least some of this increase, such as the complex relationship between communicable and NCD and growing environmental, occupational, and cultural pressures. Malawi and other LMIs are struggling to manage the increasing challenge of NCDs, in addition to an already high communicable disease burden. However, health care policy implementation, specific health promotion campaigns, and further epidemiological research may be key to attenuating this impending health crisis, both in Malawi and elsewhere. This review aims to examine the effects of the major NCDs in Malawi to help inform future public health care policy in the region.
Introduction
Non-communicable diseases (NCDs) are globally responsible for more deaths than all other causes combined, with 4 NCDs (cardiovascular disease [CVD], cancer, chronic respiratory diseases [CRD], and diabetes) responsible for 84% of this mortality.
Almost three quarters of deaths from NCDs occur in low-middle income countries (LMIs) that already experience challenges in managing significant epidemics of infectious disease such as HIV/AIDS and tuberculosis (TB). With many LMIs undergoing rapid epidemiological transition, the emergence of NCDs as a major cause of death risks overwhelming their health systems with a double burden of disease.Citation1
NCDs in Malawi
Malawi is a small country in South-Eastern Africa with approximately 17 million people and consistently ranks amongst the world’s poorest nations.Citation2 NCDs are estimated to account for 28% of deaths in Malawi, a figure that continues to rise in countries throughout Sub-Saharan Africa (SSA).Citation1,Citation3 Trends in NCDs and factors associated with their development in Malawi are discussed in the following sections. By examining their effects, this review aims to raise awareness of this bourgeoning issue in LMIs and help to inform future public health care policy.
Cardiovascular disease
CVD (including peripheral vascular disease and stroke) has a prevalence of 8.9% in Malawi and is responsible for 12% of all deaths. There is a higher age-standardized mortality rate for CVD in Malawi than in many developed countries, including the UK which has an ASMR of 100–175 per 100,000 compared to Malawi’s 250–325.Citation4 When using age adjusted incidence rates, Malawi also has a greater rate than the UK of both ischaemic heart disease (2166.8 per 100,000 population vs 1098.6) and stroke (1550.1 vs 452.5).Citation5 A 2009 STEPwise approach to surveillance (STEPS) survey examined the prevalence of some cardiovascular risk factors in a Malawian population and reported that despite high CVD mortality, many “traditional” risk factors remain relatively uncommon in the Malawian adult population. The prevalence of obesity (7.4%), raised cholesterol >5 mmol/L (8.7%), and smoking (14.1%) are low, especially in comparison to the figures from the high-income Western countries such as the UK (26.9%, ~55.5%, and 17.2% respectively).Citation6–Citation9
However, some of these figures mask statistically significant sex disparities (p<0.05), with obesity rates in women over 3 times the rate in men (7.3% vs 2.0%) and contrariwise for smoking where over a quarter of men (25.9%) were smokers compared to only 2.9% of women. The appreciation of these significant differences between demographic groups is essential when considering data regarding NCDs in LMIs to help explain high disease incidence in the setting of apparently low risk factor prevalence.Citation9
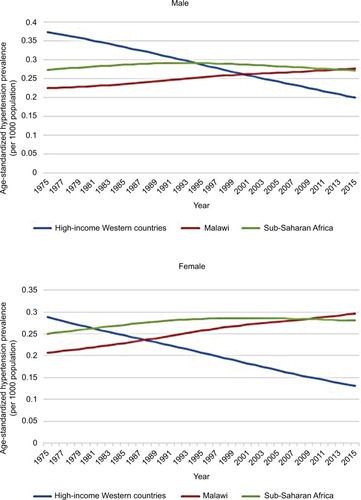
Hypertension is highly prevalent in Malawi with nearly a third of 25- to 64-year-olds having raised blood pressure or taking antihypertensive medication.Citation9 This is consistent with data that suggest an increasing prevalence throughout the African region with a marked rural-urban gradient implicating changes in lifestyle as a key contributor.Citation10 demonstrates how age-standardized prevalence rates of hypertension in Malawi and SSA have increased over the past 40 years and now exceed the falling rates in high-income Western countries.Citation11,Citation12
Figure 1 Age-standardized hypertension prevalence in SSA, Malawi and high-income Western countries 1975–2015, according to data from the NCD Risk Factor Collaboration.
Abbreviation: SSA, Sub-Saharan Africa.
The global risk factor analysis carried out by the INTERSTROKE study estimated the population attributable risk resulting from hypertension for all types of stroke to be 90.3%.Citation13 This may help to explain the WHO statistics that attribute the majority of Malawi’s CVD mortality to stroke; 5.7% of all deaths, compared to 3.3% for ischemic heart disease. One study from a large tertiary hospital in the northern region of Malawi reported that patients with hypertensive heart disease accounted for almost a quarter (24%) of those attending outpatient cardiology clinics.Citation14,Citation15
Many studies have shown preponderance for people of Afro-Caribbean ethnicity to develop hypertension and hypertension-related complications earlier and more frequently than Caucasian people, which are attributed to several proposed physiological differences. These include a reduced suppression of the renin-angiotensin-aldosterone system in the setting of high sodium intake and a lower threshold for pressure-mediated vascular dysfunction.Citation15 Studies demonstrating these ethnic differences have reported a higher stroke rate in African participants but a lower risk of coronary artery disease.Citation16,Citation17 However, these studies are often confounded by marked socioeconomic differences between the 2 groups.
Smoking-related mortality from CVD in Malawi has increased by 20% over the 23-year period from 1990 to 2013, though this in fact constituted a 31% increase in males and a 3% decrease in females. Despite these figures – and despite a commensurate increase in CVD mortality – CVD mortality rate in men is less than in women.Citation4 This indicates that cardiovascular risk in Malawi is truly multifactorial, whereby certain factors such as obesity and raised cholesterol that are significantly more prevalent in women may outweigh the increased risk in men caused by a higher smoking rate. The poor affordability of cigarettes and the typically high nicotine content of Malawian tobacco mean that fewer cigarettes are smoked per day by the average “smoker” than in a developed country (rarely more than 5). This may make smoking tobacco a weaker risk factor for CVD in this population.Citation9,Citation18
Dietary factors like low seed, nut, and vegetable intake and high sodium intake are regarded as risk behaviors contributing to the increase of CVDs across SSA.Citation19,Citation20
Sodium intake is increasing, with every published sodium consumption study in Tanzania (with which Malawi shares a border to the north-east) reporting consumption greater than the WHO set guidance limits of 2 g/day. Data from Malawi are scarce, with only 1 study published in 1986, which although it demonstrated intake below the 2 g limit, also demonstrated that intake in urban areas was almost double that of rural areas (0.86 g vs 1.65 g).Citation21 Globally, 1.7 million CVD deaths each year are estimated to be due to excess sodium intake.Citation1
Multiple meta-analyses have demonstrated the correlation between low fruit and vegetable intake and an increase in both all-cause and cardiovascular mortality, often attributed to the deficiency in protective compounds contained in them including vitamin C and flavonoids, which may help to reduce oxidant vascular damage. The paucity of data on this subject in Africa is evident and no meta-analyses on this subject include studies from the region.Citation22,Citation23
Obesity can be regarded as a disorder of chronic inflammation and is likely to contribute to CVD by additional mechanisms independent of its contribution to a state of insulin resistance (explained in the following text).Citation24
Chronic respiratory diseases
CRD include chronic obstructive pulmonary disease (COPD), asthma, and occupational lung diseases. Although endemic in Malawi, these diseases are often overlooked, and data are scarce due to much of the focus being on the much larger burden of communicable lung diseases such as TB, childhood pneumonia, and HIV-related lung diseases such as pneumocystis pneumonia.Citation25
Malawi has a low prevalence of asthma of approximately 5%, especially when compared to the UK, which has one of the world’s highest prevalence rates of >12%.Citation26,Citation27 Despite this, it is likely that asthma remains underdiagnosed and under-treated in Malawi, evidenced by an asthma age-standardized mortality rate higher than that of the UK. As well as this, the ISAAC study series has shown a trend of increasing incidence across the African region indicating that the epidemiological transition may be accompanied by a commensurate rise in asthma rates consistent with the “hygiene hypothesis” of asthma pathogenesis.Citation28
Smoking epidemiology is described previously; more men and fewer women smoke in Malawi than the average number in low-income countries.Citation29 The major obstacles that Malawi faces in combating smoking rates and related mortality are related to being one of the most tobacco-dependent economies in the world, with little regulation on the sale and advertisement of tobacco products. An economy so dependent on an industry with a combined revenue far in excess of Malawi’s GDP weakens the ability to legislate to enforce effective public health policies against tobacco consumption.Citation30,Citation31 The financial and political pressure exerted by the tobacco industry has been highlighted in recent years by high-profile cases like the 2010 legal case “Phillip Morris vs Uruguay” where a large tobacco multinational company attempted to sue a country for brand devaluation due to the introduction of anti-smoking legislation.Citation32 Recent reports have revealed court cases against African countries by multinational companies including Uganda, Kenya, and the Democratic Republic of Congo.Citation33
Asthma allergens and risk factors implicated in asthma differ from those established in North-America and Europe, though mostly due to differences in occupational exposures and local fauna rather than differing pathogenesis.Citation34 Some studies have suggested that infections with helminths such as Schistosoma, which is found in abundance in Lake Malawi, may attenuate the atopic response to allergens. A study in Gabonese children found that those with urinary schistosomiasis reacted to dust-mite allergen skin prick less frequently than those without.Citation35
Occupational lung disease in Malawi is not well researched but certain workers are recognized to be at risk, namely those in the textiles, wood-cutting, tea and coffee processing, and tobacco industries.Citation24 Malawi is one of the top 10 exporters of tobacco worldwide and there is likely to be an underappreciated burden of occupational disease associated with its production.Citation30 “Tobacco Worker’s Lung” is an extrinsic allergic alveolitis in response to the Aspergillus fungus that is often found in fields and factories; there are no data on the incidence in Malawi.Citation36
Ambient air pollution is recognized as a global risk factor for respiratory disease and is emerging as a previously under-appreciated risk factor for CVD. Two industrializing African urban centers, Kaduna (Nigeria) and Kampala (Uganda), were highlighted in a recent study where harm from inhaled particulate matter was estimated to negate the health benefits of cycling after 105 and 90 minutes, respectively. The high levels of particulate matter in these cases are usually attributable to unregulated industrial emissions, low-quality fuel combustion, and the burning of waste material for disposal.Citation37 Levels of such particulate matter are low in Malawi with its small industrial sector, reliance on renewable energy (95% of national grid electricity coming from a hydroelectric source), and 85% of the population living in rural areas. However, the population may instead be at increased risk from high levels of “indoor” air pollution.
Only 9% of the Malawian population is connected to the power grid, with this minority also experiencing regular power cuts. This means 95% of people rely on burning wood or other plant materials as their main source of domestic energy. In a 2008 study of 62 Malawian homes, 100% had fine particulate matter levels that exceeded WHO limits for outdoor air.Citation38 Although no studies exist in Malawi, biomass fuel use is an established risk factor for the development of COPD and may in fact be the most important risk factor worldwide.Citation39,Citation40 Indoor pollution in Malawi may be a more significant problem in females, especially due to the cultural practice of spending more time cooking with biomass in poorly ventilated homes. This may explain a Ugandan study that described similar COPD prevalence in both sexes despite more than double the proportion of women with COPD being never smokers (74% vs 31%).Citation41 It has been suggested that biomass-related COPD represents a separate disease phenotype with a younger age of onset (earlier exposure), more frequent symptomatic wheeze, and less parenchymal damage.Citation42
Cancer
The large burden of infectious disease has a significant effect on the epidemiology of cancer in Malawi. Worldwide, cancer is predominantly a disease of later life; with life expectancy in Malawi averaging 59 years for males and 60 years for females, a low incidence of cancer could be expected. However, for some types of cancer Malawi has some of the highest incidence rates in the world.Citation2,Citation43
Infectious agents have a role in the pathogenesis of many cancers in Malawi, and the endemic nature of these infections, in addition to a high number of immunocompromised individuals due to coexisting HIV infection (1 in 10 people), is likely to contribute to these high rates.Citation44 Cancer surgery with curative intent is very limited in Malawi, and management of most solid tumors is palliative.Citation43
Overall, the age-standardized incidence rates for all cancers in Malawi is 156 cases per 100,000, which although higher than the average for SSA of 121 is still much lower than the rates in high-income Western countries, the EU average standing at 278 and the USA at 318.Citation45
Esophageal cancer incidence rates in Malawi are the highest in the world at 24.2 cases per 100,000 with no single identifiable causative risk factor. The current consensus is that the excess risk is multifactorial and may be a combination of high levels of aflatoxin in the diet (a mycotoxin found in improperly stored maize, the staple crop in Malawi), high strength alcohol consumption and tobacco consumption.Citation46 There has been specific interest in the homebrewed maize spirit known as Kachasu due to its high alcohol percentage (up to 70%) and high levels of nitrosamines and contaminants such as zinc.Citation47
There is an indication that HIV infection may have a role in esophageal carcinogenesis, with 1 study noting that esophageal cancer rates have paralleled those of Kaposi’s sarcoma.Citation46
Kaposi’s sarcoma is the most common cancer in Malawi, constituting over 50% of all cancer diagnoses. The pathogenesis of Kaposi’s sarcoma is related to infection with human herpesvirus-8 in HIV-positive patients with low CD4 counts.Citation46
Bladder cancer mortality rates in Malawi are the 3rd highest in Africa. As previously mentioned, infection with the helminths Schistosoma haematobium and Schistosoma mansoni is common in Malawi, with a systematic review finding reports of prevalence in some areas as high as 94.9% and 67.0%, respectively.Citation48 Schistosomal infection of the bladder is a recognized risk factor for the development of squamous cell carcinoma of the bladder (SCC) with egg deposition in the bladder wall causing local inflammation and enabling some schistosomal antigens to inhibit host cell apoptosis. Unlike the predominantly transitional cell tumors seen in developed countries, schistosomal-associated SCC is usually well differentiated and only locally invasive.Citation49 Despite this, late presentation and few facilities for resection mean that mortality in Malawi remains high.Citation50
Cervical cancer incidence and mortality in Malawi are the highest in the world and it is the most commonly diagnosed cancer in Malawian females at 75.9 cases per 100,000. This is attributed to the high prevalence of human papillomavirus (HPV) infection, which is known to lead to dyskaryosis and malignant change of the cervical epithelium.Citation50,Citation51 HPV and HIV are both thought to predispose to infection with each other, and HIV co-infection is believed to accelerate the rate of malignant transformation in those with HPV-related dyskaryosis; the high levels of both viruses in the population act synergistically to produce the high incidence rates of cervical cancer.Citation52
In Malawi, non-Hodgkin’s lymphoma (NHL) is the third most commonly diagnosed cancer. These are predominantly cases of Burkitt lymphoma (BL), a B-cell lymphoma that is characterized by a range of chromosomal translocations and genetic mutations; particularly of the c-myc oncogene.Citation43,Citation53 Epstein-Barr virus (EBV) is believed to have a role in the deregulation of this oncogene as well as promoting the survival of malignant cells. Epidemiological clustering of both diseases suggests an association between BL and Plasmodium falciparum infection, though a definitive role and interaction with EBV has not been established.Citation54 Certain plant toxins such as those from the Euphorbiaceae family have been suggested as co-factors in BL development and have been shown to induce EBV-associated chromosomal abnormalities in vitro. A 1993 case-control study from Malawi reported that people with BL were significantly more likely to have Euphorbiaceae plants at their homes.Citation55 The occurrence rate of BL is also increased in people with concurrent HIV infection, which increases the occurrence of all types of NHL by a factor of 60–200.Citation56
Diabetes
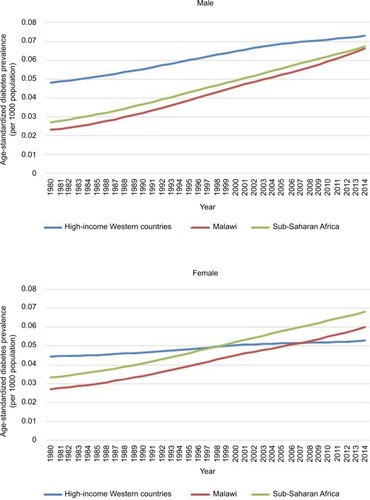
Diabetes prevalence is increasing throughout SSA, with the age-standardized prevalence rates for men in Malawi and SSA approaching those rates in high-income Western countries and rates in women surpassing them (). Much of this increase is due to the rise in type 2 diabetes, although epidemiological studies do not differentiate between type 1 and 2.Citation57 The paucity of data from throughout the African region means that prevalence and trends are based on estimation calculations using low-quality epidemiological studies; in a Lancet worldwide diabetes study “21 (39%) of the 54 countries without data were in sub-Saharan Africa”.Citation58 Estimates of prevalence in Malawi range from 2.3% (updated figures seen when URL was updated) (IDF) to 5.7% (2009 STEPS Survey), the latter approaching the prevalence in the UK (6%) despite having less than half of the percentage of people classed as overweight or obese (21.9% vs 62.9%).Citation6,Citation9,Citation59
Figure 2 Age-standardized diabetes prevalence in SSA, Malawi and high-income Western countries 1980–2014, according to data from the NCD Risk Factor Collaboration.
Abbreviation: SSA, Sub-Saharan Africa.
The dominant theory of diabetes risk is one of “lifestyle factors” whereby an increasingly sedentary lifestyle with concurrent calorie excess predisposes to the development of the “metabolic syndrome”. Diabetes epidemiology in SSA shows a 2–5 times increased risk for diabetes or impaired fasting glucose in urban areas, which are more associated with these lifestyle risk factors.Citation60 With rural to urban migration forming part of the wider epidemiological transition across the region (SSA has the fastest urbanization rate in the world), this trend is likely to continue.Citation61
Adiposity
In keeping with worldwide trends, studies across Africa show a significant positive correlation between increased body mass index (BMI) and diabetes risk.Citation62 More than 1 in 5 Malawians are overweight or obese, with the rate in females significantly greater than in males (28.1% vs 16.1%).Citation9 Debate remains over the best measure of adiposity in African populations due to a lack of data. Some studies have suggested that African populations may have a lower percentage body fat than Europid populations at the same BMI, although epidemiological data for the SSA regions indicated that they may develop diabetes at lower BMIs on average.Citation63,Citation64 Roles for other measurements like waist circumference (WC) and waist hip ratio (WHR) have not been established but in a small study in northern Malawi, WHR was found to have a greater sensitivity to detect diabetes patients than BMI and WC when using WHO-recommended cutoffs.Citation65 It appears that the central distribution of this more hormonally active fat is important, with 1 study including Afro-Caribbean participants finding that WC was associated with metabolic syndrome clustering, independent of BMI.Citation66
Physical activity
Growing service sector industries and changing leisure activities across SSA mean people are engaging in less physical activity. Job transition from agricultural to service sectors typically is associated with a decrease in physical activity, and recreational exercise is a culturally uncommon pastime, perhaps due to the historically strenuous nature of subsistence farming.Citation67 One Cameroonian study reported significantly decreased energy expenditure in urban dwellers compared to rural dwellers as well as a significantly increased rate of diabetes. Urban dwellers recorded shorter walking and cycling times per week and “lighter intensity” occupations.Citation68 The trend of decreasing physical activity as SSA undergoes further economic development will likely worsen the “energy imbalance” associated with the obesity epidemic whilst also increasing diabetes risk by mechanisms independent of weight gain. A number of prospective and cross-sectional studies have shown even moderate exercise to reduce the risk of developing diabetes across numerous ethnic groups, believed to be due to exercise-induced augmentation of insulin action.Citation69
Diet
Aside from calorie excess, additional dietary factors have been associated with diabetes risk and are prevalent in Malawi. Data from the Nurses’ Health Study showed that participants with a diet of high glycemic load or glycemic index in addition to low cereal fiber intake had an approximately 50% increased risk of developing diabetes.Citation70 In Malawi, the staple carbohydrate dish Nsima is made from ground maize (cornmeal) and water; it has both a high glycemic index (94.06 in 1 study) and low cereal fiber content. Nsima can be made from flour of various particle sizes according to grinding. Smaller particle flour increases the glycemic index of the meal and the ability to adjust the level of grinding, and therefore adjustment of the glycemic profile of the meal presents an opportunity to reduce dietary risk with simple changes to food preparation.Citation71
Fiber and antioxidant (especially vitamin C) intake from fruit and vegetables has shown associations with decreased diabetes risk in observational studies but the exact significance is unclear. In the Malawi STEPS survey, fruit and vegetable intake was low with 97.5% of people eating fewer than 5 servings of fruit and vegetables per day, the average being 2.1 servings a day.Citation9
Sugar sweetened beverages (SSBs) or “soft drinks” are widely consumed in Malawi and are available for lower prices than bottled water at many retailers.Citation72 Consumption is increasing – especially in young people, with 1 study of Malawian schoolchildren reporting that 50 out of 60 (83.3%) were consuming SSBs at least once a day.Citation73 A meta-analysis of 11 studies showed that people consuming this level of SSB had a 26% greater risk of developing metabolic syndrome or diabetes than those consuming <1 a month, proposed to be the effect of the added dietary glycemic load.Citation74
Iatrogenic causes
Hypertension in Malawi is most often managed using thiazide diuretics due to their low cost and widespread availability. Insulin resistance and hyperglycemia are recognized side effects of thiazide medications and widespread use may be contributing to diabetes risk.Citation75,Citation76
Relationship between communicable and non-communicable diseases
As is clear in the case of cancer, often a distinction between communicable diseases and NCDs is not possible – especially in a population where HIV is endemic. HIV is increasingly recognized as a risk factor for CVD, with a meta-analysis of 20 studies reporting the relative risk of CVD, in HIV-infected patients compared to uninfected patients, to be 1.61. Antiretroviral drugs used to treat HIV can cause hypertriglyceridemia, hypercholesterolemia, and hyperglycemia; in the same study, the relative risk for HIV patients taking ART treatment was higher at 2.00.Citation77 The hyperglycemia side effect – especially from protease inhibitors – may also contribute to diabetes risk. Reciprocally, NCDs may increase the burden of communicable disease, for example diabetes patients are over 3 times more likely to become infected with TB. These findings are the basis of the bidirectional screening programs that are being established in some low-middle income countries.Citation78,Citation79
Where is intervention most needed?
Early intervention in Malawi’s NCD epidemic may be more effective in reducing risk behaviors and adjusting how health care infrastructure is developed. For example, taxation to deter the purchase of calorie dense convenience foods and SSBs is likely to be more politically acceptable and effective if introduced before consumption becomes more widespread.Citation80
Two important primary steps to address NCD rates in Malawi would be to gather more epidemiological data, especially regarding prevalence, and establish a health promotion strategy to raise awareness about the most common NCDs, to health care providers and the public. Electronic registries to collect data on NCDs would be relatively simple to set up with the ability to attach additional modules to existing systems already used to manage and monitor HIV patients.Citation65
A campaign of health promotion is essential to help control rates of all NCDs in Malawi, from CVD where almost all dietary sodium is added during the cooking process, to respiratory disease and cancer where the health implications of tobacco are poorly publicized, especially on packaging.Citation21,Citation29 Promoting better ventilation whilst using wood burning stoves inside the home, such as using the stove in doorways or next to windows, is a simple way to help reduce the exposure to indoor air pollution.
Health promotion strategies for the public can be modeled on those currently used for HIV where print materials, television broadcasts, and public billboards have all been utilized to good effect.Citation81 SMS-based health promotion is also emerging as an effective way to deliver health education in an inexpensive and widespread manner as mobile phone ownership continues to increase rapidly across SSA.Citation82
In the case of diabetes and CVD, cultural beliefs regarding what constitutes a health body weight may be contributing toward rising obesity rates. In a small outpatient survey of 40 patients in northern Malawi, 57.4% of respondents selected a BMI of 40 kg/m2 as the “healthiest body weight” when presented with 5 images corresponding to BMIs ranging from 18 to 40 kg/m2.Citation65 The reasons for this are complex; it is a combination of the cultural perceptions of body image in addition to obesity reflecting wealth and status and weight loss being associated with the wasting from AIDS and malnutrition. In this instance, educational initiatives targeted at schoolchildren and already effectively employed in HIV education can begin to challenge these beliefs about body weight. National standards could be set for school curricula to focus on dietary education, for example teaching portion control by using tangible measurements like a fist. There could also be a greater emphasis on structured recreational sports to help make exercise a more normal part of daily life from an early age. Governmental funding for such schemes is low, and these public health campaigns are usually provided by non-governmental organizations and charities. Although taking on an additional educational initiative could be an overwhelming workload, the current HIV campaign is becoming increasingly self-sufficient within the involved schools and it is important to utilize the existing infrastructure to promote awareness of other diseases.
Conclusion
In Malawi and across SSA, the incidence and mortality of NCDs are rising. The paucity of data regarding NCD risk factors in the region severely affects the ability to interpret disease trends and plan population specific interventions, and more high-quality epidemiological data are essential. As public health interventions are ultimately data driven, carrying out such surveys is fundamental to motivating change.
However, what is clear is that a comprehensive campaign of health promotion is required to begin to address the development of risk behaviors – especially those associated with an increasingly sedentary, calorie-rich, and “Westernized” urban lifestyle – that are contributing to a rapidly increasing burden of NCD throughout LMIs.
Acknowledgments
The authors are grateful to the Wellcome Trust ISSF at Imperial College London for funding support and to the United Kingdom National Institute for Health Research Biomedical Facility at Imperial College London for infrastructure support. All the authors acknowledge the support of Mzuzu Central Hospital and Luke International Norway for research support in Malawi.
Disclosure
The authors report no conflicts of interest in this work.
References
- WHOGlobal Action Plan for the Prevention and Control of Noncommunicable Diseases 2013–20202013 Available from: http://www.who.int/nmh/publications/ncd_action_plan/en/Accessed April 1, 2017
- Central Intelligence AgencyThe World Factbook 2016: Malawi Available from: https://www.cia.gov/library/publications/the-world-factbook/geos/mi.htmlAccessed April 1, 2017
- WHONoncommunicable Diseases (NCD) Country Profiles: Malawi2014 Available from: http://www.who.int/nmh/countries/mwi_en.pdfAccessed April 1, 2017
- Institute for Health Metrics and EvaluationCountries profiles-Malawi Available from http://www.healthdata.org/malawiAccessed May 30, 2018
- RothGAHuffmanMDMoranAEGlobal and regional patterns in cardiovascular mortality from 1990 to 2013Circulation2015132171667167826503749
- Public Health EnglandAbout obesity2017 Available from: http://webarchive.nationalarchives.gov.uk/20170110165525/https://www.noo.org.uk/NOO_about_obesityAccessed April 1, 2017
- British Heart FoundationCardiovascular disease statistics2014 Available from: https://www.bhf.org.uk/publications/statistics/cardiovascular-disease-statistics-2014Accessed April 1, 2017
- Office for National StatisticsAdult smoking habits in the UK2016 Available from: https://www.ons.gov.uk/peoplepopulationandcom-munity/healthandsocialcare/healthandlifeexpectancies/bulletins/adultsmokinghabitsingreatbritain/2016Accessed April 1, 2017
- WHOMalawi National STEPS Survey for Chronic Non-Communicable Diseases and their Risk Factors2010 Available from. http://www.who.int/ncds/surveillance/steps/Malawi_2009_STEPS_Report.pdfAccessed May 30, 2018
- LindhorstJAlexanderNBlignautJRaynerBDifferences in hypertension between blacks and whites: an overviewCardiovasc J Afr200718424124717940670
- OpieLHSeedatYKHypertension in sub-Saharan African populationsCirculation2005112233562356816330697
- NCD Risk Factor Collaboration (NCD-RisC)Data Downloads: Diabetes Available from: http://ncdrisc.org/data-downloads-diabetes.htmlAccessed June 14, 2018
- O’DonnellMJXavierDLiuLINTERSTROKE investigatorsRisk factors for ischaemic and intracerebral haemorrhagic stroke in 22 countries (the INTERSTROKE study): a case-control studyLancet2010376973511212320561675
- SolimanEZJumaHCardiac disease patterns in northern Malawi: epidemiologic transition perspectiveJ Epidemiol200818520420818753734
- Centers for Disease Control and PreventionGlobal Health – Malawi Available from: https://www.cdc.gov/globalhealth/countries/malawi/Accessed April 1, 2017
- SliwaKWilkinsonDHansenCSpectrum of heart disease and risk factors in a black urban population in South Africa (the Heart of Soweto Study): a cohort studyLancet2008371961691592218342686
- EdwardsRUnwinNMugusiFHypertension prevalence and care in an urban and rural area of TanzaniaJ Hypertens200018214515210694181
- PampelFTobacco use in sub-Sahara Africa: estimates from the demographic health surveysSoc Sci Med20086681772178318249479
- StrazzulloPD’EliaLKandalaNBCappuccioFPSalt intake, stroke, and cardiovascular disease: meta-analysis of prospective studiesBMJ2009339b456719934192
- ReddyKSYusufSEmerging epidemic of cardiovascular disease in developing countriesCirculation19989765966019494031
- OyebodeOOtiSChenYFLilfordRJSalt intakes in sub-Saharan Africa: a systematic review and meta-regressionPopul Health Metr201614126759530
- DauchetLAmouyelPHercbergSDallongevilleJFruit and vegetable consumption and risk of coronary heart disease: a meta-analysis of cohort studiesJ Nutr2006136102588259316988131
- WangXOuyangYLiuJFruit and vegetable consumption and mortality from all causes, cardiovascular disease, and cancer: systematic review and dose-response meta-analysis of prospective cohort studiesBMJ2014349g449025073782
- PoirierPGilesTDBrayGAObesity and cardiovascular disease: pathophysiology, evaluation, and effect of weight lossArterioscler Thromb Vasc Biol200626596897616627822
- GordonSGrahamSEpidemiology of respiratory disease in MalawiMalawi Med J200618313414627529007
- WHOAnalytical summary – non-communicable diseases and conditions2016 Available from: http://www.aho.afro.who.int/profiles_information/index.php/Malawi:Analytical_summary_-_Noncommunicable_diseases_and_conditionsAccessed April 1, 2017
- British Lung FoundationAsthma statistics2017 Available from: https://statistics.blf.org.uk/asthmaAccessed April 1, 2017
- MallolJCraneJvon MutiusEOdhiamboJKeilUStewartAISAAC Phase Three Study GroupThe International Study of Asthma and Allergies in Childhood (ISAAC) Phase Three: a global synthesisAllergol Immunopathol (Madr)2013412738522771150
- EriksenMMackayJSchlugerNGomeshtapehFDropeJThe Tobacco Atlas, 5thAtlanta, GAAmerican Cancer Society2015 Available from: http://www.tobaccoatlas.org/country-data/malawi/Accessed April 1, 2017
- HuTWLeeAHTobacco control and tobacco farming in African CountriesJ Public Health Policy2015361415125428192
- SaloojeeYDagliETobacco industry tactics for resisting public policy on healthBull World Health Organ200078790291010994263
- BoseleySThreats, bullying, lawsuits: tobacco industry’s dirty war for the African marketThe Guardian2017 Available from: https://www.theguardian.com/world/2017/jul/12/big-tobacco-dirty-war-africa-marketAccessed November 1, 2017
- CrosbieESosaPGlantzSADefending strong tobacco packaging and labelling regulations in Uruguay: transnational tobacco control network versus Philip Morris InternationalTob Control201827218519428336521
- WjstMBoakyeDAsthma in AfricaPLoS Med200742e7217326712
- van den BiggelaarAHvan ReeRRodriguesLCDecreased atopy in children infected with Schistosoma haematobium: a role for parasite-induced interleukin-10Lancet200035692431723172711095260
- IsmailTMcSharryCBoydGExtrinsic allergic alveolitisRespirology200611326226816635083
- TainioMde NazelleAJGotschiTCan air pollution negate the health benefits of cycling and walking?Prev Med20168723323627156248
- FullertonDGSempleSKalamboFBiomass fuel use and indoor air pollution in homes in MalawiOccup Environ Med2009661177778319671533
- SalviSBarnesPJIs exposure to biomass smoke the biggest risk factor for COPD globally?Chest201013813620605806
- HuGZhouYTianJRisk of COPD from exposure to biomass smoke: a metaanalysisChest20101381203120139228
- van GemertFKirengaBChavannesNPrevalence of chronic obstructive pulmonary disease and associated risk factors in Uganda (FRESH AIR Uganda): a prospective cross-sectional observational studyLancet Glob Health201531e44e5125539969
- SalviSThe silent epidemic of COPD in AfricaLancet Glob Health201531e6e725539971
- MsyambozaKPDzamalalaCMdokweCBurden of cancer in Malawi; common types, incidence and trends: national population-based cancer registryBMC Res Notes2012514922424105
- National Statistical Office of MalawiMalawi Demographic and Health Survey 2010 Available from: https://dhsprogram.com/pubs/pdf/FR247/FR247.pdfAccessed April 1, 2017
- FerlayJSoerjomataramIErvikMGLOBOCAN 2012 v1.0, Cancer Incidence and Mortality Worldwide: IARC CancerBase No. 11Lyon, FranceInternational Agency for Research on Cancer2013 Available from: http://globocan.iarc.frAccessed April 1, 2017
- MlombeYDzamalalaCChisiJOthieno-AbinyaNOesophageal cancer and Kaposi’s Sarcoma in Malawi: a comparative analysisMalawi Med J2009212666820345007
- McGlashanNDOesophageal cancer and alcoholic spirits in central AfricaGut19691086436505810975
- MakaulaPSadalakiJRMuulaASKayuniSJemuSBlochPSchistosomiasis in Malawi: a systematic reviewParasit Vectors2014757025490938
- ZaghloulMSBladder cancer and schistosomiasisJ Egypt Natl Cancer Inst2012244151159
- MsyambozaKPMandaGTemboBCancer survival in Malawi: a retrospective cohort studyPan Afr Med J20141923425838862
- MsyambozaKPPhiriTSichaliWKwendaWKachaleFCervical cancer screening uptake and challenges in Malawi from 2011 to 2015: retrospective cohort studyBMC Public Health201616180627535359
- FerenczyACoutléeFFrancoEHankinsCHuman papillomavirus and HIV coinfection and the risk of neoplasias of the lower genital tract: a review of recent developmentsCMAJ2003169543143412952805
- OremJMbiddeEKLambertBde SanjoseSWeiderpassEBurkitt’s lymphoma in Africa, a review of the epidemiology and etiologyAfr Health Sci20077316617518052871
- MutalimaNMolyneuxEJaffeHAssociations between Burkitt lymphoma among children in Malawi and infection with HIV, EBV and malaria: results from a case-control studyPLoS One200836e250518560562
- van den BoschCGriffinBEKazembePDziweniCKadzamiraLAre plant factors a missing link in the evolution of endemic Burkitt’s lymphoma?Br J Cancer1993686123212358260378
- GroggKLMillerRFDoganAHIV infection and lymphomaJ Clin Pathol200760121365137218042692
- WHOGlobal Report on Diabetes2016 Available from http://www.who.int/diabetes/global-report/en/Accessed May 30, 2018
- NCD Risk Factor Collaboration (NCD-RisC)Data Downloads: Blood Pressure Available from: http://ncdrisc.org/data-downloads-blood-pressure.htmlAccessed June 14, 2018
- International Diabetes FederationIDF Diabetes Atlas8th editionBrussels, BelgiumInternational Diabetes Federation2017 Available from http://www.diabetesatlas.orgAccessed May 30, 2018
- MbanyaJCRamiayaKDiabetes mellitusJamisonDTFeachemRGMakgobaMWDisease and Mortality in Sub-Saharan Africa2nd edWashington, DCThe International Bank for Reconstruction and Development/The World Bank2006 Chapter 19. Available from: https://www.ncbi.nlm.nih.gov/books/NBK2291/Accessed April 1, 2017
- MbanyaJCMotalaAASobngwiEAssahFKEnoruSTDiabetes in sub-Saharan AfricaLancet201037597332254226620609971
- MbanyaJCAssahFKSajiJAtangaENObesity and type 2 diabetes in Sub-Sahara AfricaCurr Diab Rep201414750124800746
- FrankLKHeraclidesADanquahIBedu-AddoGMockenhauptFPSchulzeMBMeasures of general and central obesity and risk of type 2 diabetes in a Ghanaian populationTrop Med Int Health201318214115123190041
- GaillardTConsequences of abdominal adiposity within the metabolic syndrome paradigm in black people of African ancestryJ Clin Med20143389791226237484
- GowshallMA Registry-Based Approach to Diabetes Risk Scores in Malawi [dissertation]LondonImperial College London2016
- OkosunISLiaoYRotimiCNPrewittTECooperRSAbdominal adiposity and clustering of multiple metabolic syndrome in White, Black and Hispanic AmericansAnn Epidemiol200010526327010942873
- JasperUSDiabetes and exercise in sub-Saharan Africa: challenges and way forwardInt J Diabetes Metabol20145413
- SobngwiEMbanyaJCUnwinNCPhysical activity and its relationship with obesity, hypertension and diabetes in urban and rural CameroonInt J Obes Relat Metab Disord20022671009101612080456
- ColbergSRSigalRJFernhallBAmerican College of Sports MedicineAmerican Diabetes AssociationExercise and type 2 diabetes: the American College of Sports Medicine and the American Diabetes Association: joint position statementDiabetes Care20103312e147e16721115758
- Ardisson KoratAVWillettWCHuFBDiet, lifestyle, and genetic risk factors for type 2 diabetes: a review from the Nurses’ Health Study, Nurses’ Health Study 2, and Health Professionals’ Follow-up StudyCurr Nutr Rep20143434535425599007
- MlothaVMwangwelaAMKasapilaWSiyameEWMasambaKGlycemic responses to maize flour stiff porridges prepared using local recipes in MalawiFood Sci Nutr20154232232827004122
- SinghGMMichaRKhatibzadehSGlobal Burden of Diseases Nutrition and Chronic Diseases Expert Group (NutriCoDE)Global, Regional, and National Consumption of Sugar-Sweetened Beverages, Fruit Juices, and Milk: a systematic assessment of beverage intake in 187 countriesPLoS One2015108e012484526244332
- KalimbiraAGondweEConsumption of sweetened beverages among school-going children in a densely populated township in Lilongwe, MalawiMalawi Med J2015272555926405513
- MalikVSPopkinBMBrayGADespresJPWillettWCHuFBSugar-sweetened beverages and risk of metabolic syndrome and type 2 diabetes: a meta-analysisDiabetes Care201033112477248320693348
- MsyambozaKPKathyolaDDzowelaTBowieCThe burden of hypertension and its risk factors in Malawi: nationwide population-based STEPS surveyInt Health20124424625224029670
- CarterBLErnstMEThiazide-induced hyperglycemia: can it be prevented?Am J Hypertens200922547319387432
- IslamFMWuJJanssonJWilsonDPRelative risk of cardiovascular disease among people living with HIV: a systematic review and meta-analysisHIV Med201213845346822413967
- HarriesADKumarAMSatyanarayanaSAddressing diabetes mellitus as part of the strategy for ending TBTrans R Soc Trop Med Hyg2016110317317926884497
- DooleyKEChaissonRETuberculosis and diabetes mellitus: convergence of two epidemicsLancet Infect Dis200991273774619926034
- ManyemaMVeermanJLCholaLTugendhaftALabadariosDHofmanKDecreasing the burden of type 2 diabetes in South Africa: the impact of taxing sugar-sweetened beveragesPLoS One20151011e014305026575644
- Malawi Ministry of HealthHealth Education Services: What We Do Available from: http://www.healthpromotion.gov.mw/index.php/what-we-doAccessed April 1, 2017
- CrawfordJLarsen-CooperEJezmanZCunninghamSCBancroftESMS versus voice messaging to deliver MNCH communication in rural Malawi: assessment of delivery success and user experienceGlob Health Sci Pract201421354625276561