
Abstract
Objective
In current most observational studies, the prognosis of cervical adenocarcinoma is worse than that of cervical squamous cell carcinoma. However, most of the current studies are holistic and lack more detailed staging and grouping analysis of the prognosis of the two types of cervical tumors.
Patients and Methods
Inclusion from the SEER database of stage IIB-IVA cervical squamous cell carcinoma and cervical adenocarcinoma patients who did not undergo surgery from 2000 to 2019, underwent radiotherapy/chemotherapy/radiotherapy and chemotherapy/no treatment, and then propensity score matching (PSM) was performed to eliminate confounding factors between cervical squamous cell carcinoma and cervical adenocarcinoma patients with the same stage and treatment method. After matching the original data and propensity score, logarithmic rank test and chi square test were used to evaluate the survival benefits of different stages and treatment methods for patients using Kaplan Meier curve. The prognosis of two types of cervical tumors under the same treatment method was compared, and factors that may cause poor prognosis were analyzed, excluding confounding factors.
Results
A total of 10,057 patients were included in this study, and survival analysis showed a significant correlation between the treatment method used and patient prognosis (P<0.05). However, for patients who received radiotherapy or no special treatment, OS and CSS were only related to tumor stage and not to tumor type. In patients undergoing radiotherapy and chemotherapy, the OS and CSS of stage IIIA and IVA patients are not related to tumor pathological characteristics, while the OS of stage IIB patients is not related to tumor properties after PSM.
Conclusion
In patients undergoing radiotherapy and chemotherapy, the OS and CSS of stage IIIA and IVA patients were not related to histological type, while the OS of stage IIB patients was not related to histological type after PSM.
Introduction
Cervical cancer was once one of the most common malignant tumors in women. With the promotion of cytological screening programs and the vaccination of human papillomavirus (HPV) vaccine, the incidence rate and mortality of cervical cancer have significantly decreased.Citation1 Pathological diagnosis shows that most cervical cancer is squamous cell carcinoma of the cervix caused by HPV, but the true incidence rate and relative incidence rate of cervical adenocarcinoma with unclear relationship with HPV continue to rise.Citation2,Citation3
Cervical adenocarcinoma is considered a type of cervical cancer with different causes and clinical outcomes compared to cervical squamous cell carcinoma. In the 5th edition of the WHO classification of female reproductive organ tumors,Citation4 cervical adenocarcinoma is listed separately and Silva staging is recommended to evaluate patient prognosis.
In the current NCCN guidelines for cervical adenocarcinoma and squamous cell carcinoma, radical surgery is recommended for patients with stage I–IIA, and radiotherapy and chemotherapy are preferred for patients with stage IIB and above. However, previous guidelines have not separately distinguished cervical adenocarcinoma from cervical squamous cell carcinoma and the treatment plan was made according to FIGO staging. Current studies and comparisons on cervical adenocarcinoma and squamous cell carcinoma show that there are differences in treatment and survival rates between them,Citation5–7 and these studies mostly use conventional methods. In small sample studies, the prognosis of cervical adenocarcinoma is significantly worse than that of cervical squamous cell carcinoma.Citation5,Citation8 In large sample analysis, the incidence of AC is related to age and race.Citation3 These differences may lead to different patient outcomes under the same treatment method, and there are significant differences in the situation of advanced cervical cancer patients in stage IIB-IV. At present, there is a lack of large-scale statistics to demonstrate the prognostic differences between cervical squamous cell carcinoma and adenocarcinoma in different stages, and there is a lack of clinical basis for developing different treatment strategies for different stages. SEER database contains a lot of information, direct comparison results will inevitably be affected by related confounding factors. A study has shown that there are important age and ethnic differences in the diagnosis and treatment of cervical adenocarcinoma and squamous cell carcinoma.Citation3 In observational studies, there are a lot of data biases and confounding variables due to various reasons, and the Propensity Score Matching (PSM) is designed to reduce the impact of these biases and confounding variables, so that the experimental group and the control group can be compared more reasonably, and interference factors between the groups can be eliminated. PSM is widely used in other cancers.Citation9 Therefore, in order to balance the influence of confounding factors on the results, PSM was used in this study to study the influence of different stages and different treatment methods on the prognosis of patients with cervical adenocarcinoma and squamous cell carcinoma. This study used the SEER database to extract the required data, excluded confounding factors through propensity score matching analysis, and stratified analyzed the prognostic differences of cervical squamous cell carcinoma and cervical adenocarcinoma patients at different stages.
Patients and Method
Data Source and Screening
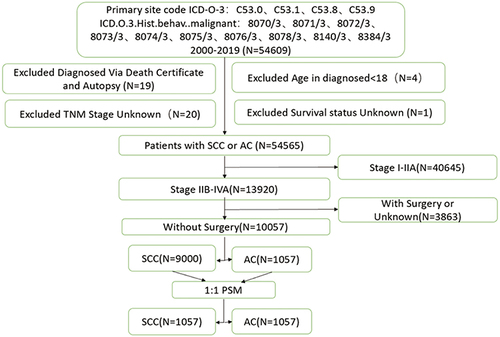
This article obtains data on cervical cancer patients through the SEER database (National Cancer Institute Monitoring, Epidemiology, and Final Results Database). Download data through SEER * Stat Software (version 8.4.0.1). Select individuals diagnosed with cervical adenocarcinoma and squamous cell carcinoma from 2000 to 2019, with primary sites of C53.0, C53.1, C53.8, and C53.9, and histological types of squamous cell carcinoma: 8070/3, 8071/3, 8072/3, 8073/3, 8074/3, 8075/3, 8076/3, 8078/3, as well as adenocarcinoma: 8140/3, 8384/3. Exclude individuals under the age of 18 years of diagnosis, confirmed through autopsy or death certificate, with unknown survival status, or TNM staging. Patients who did not undergo surgery were selected through surgical methods and classified as stage IIB-IVA. The process diagram for data exclusion and inclusion is shown in .
Figure 1 Schematic illustration of the study workflow.
Obtain the following clinical data from the database: diagnosis year, diagnosis age, insurance status, marital status, race, tumor differentiation grade, tumor size, T stage, N stage, M stage, surgical method, radiotherapy status, chemotherapy status, survival time, survival status, and cause of death. Overall survival (OS) is defined as the time from diagnosis to death from any cause, while Cancer Specific Survival (CSS) is defined as the time from diagnosis to death from cervical cancer. The last follow-up was on December 31, 2019.
Statistical Analysis
To eliminate the confounding factors between survival differences in adenocarcinoma and squamous cell carcinoma, this article adopts propensity score matching analysis to determine the data of adenocarcinoma and squamous cell carcinoma groups in a 1:1 ratio. Continuous variables were analyzed using unpaired t-tests and categorical variables were analyzed using chi square tests. Evaluate the survival benefits of patients using different treatment methods at different stages using Kaplan Meier curves. Bilateral P<0.05 has statistical significance. The data screening, statistical analysis, and image rendering in this article were all conducted using R software (1.1.463) Statistical Analysis.
A Propensity Score Matching (PSM) method was used to reduce the impact of confounding factors between cervical adenocarcinoma and squamous cell carcinoma to better and more convincingly study the differences between the two types of cervical cancer at different stages and in different treatment modalities. SM balanced variables included age, race, insurance, marital status, grade, tumor size, and T, N, and M stages. PSM was constructed in 1:1 within calipers (0.05). In order to ensure adequate matching, the nearest-neighbor matching was used, without replacement. The data were basically cleaned and processed before PSM, and all NA was deleted. Since this paper mainly studied the differences between different stages and different treatment methods of cervical adenocarcinoma and squamous cell carcinoma, data with unknown T, N, M stages or living status was deleted. After PSM, Kaplan-Meier curves were further used to evaluate the survival benefits of different treatment at different stages. The unpaired T-test was used to analyze the continuous variables, and the Chi-square test was used to analyze the categorical variables. Bilateral P<0.05 was statistically significant. In this paper, R software was used for data screening, statistical analysis and picture rendering (1.1.463). The R package used in this document includes survival3.2–7, tableone0.13.0, ggplot3.3.5, MatchIt4.3.4.
Result
In this study, we included data from a total of 10,057 patients, including 9000 patients with stage IIB-IVA cervical squamous cell carcinoma and 1057 patients with adenocarcinoma. There were significant differences in marital status (P<0.001), race (P<0.001), grade (P<0.001), tumor size (P<0.001), T stage (P<0.001), N stage (P,0.0075), and M stage (P<0.001) between squamous cell carcinoma and adenocarcinoma patients, as shown in . The distribution of cervical adenocarcinoma and squamous cell carcinoma patients with different stages and treatment methods is shown in .
Table 1 Baseline Characteristics Before Propensity Score Matching of AC and SCC Patients
Table 2 Treatment Before and After Propensity Score Matching of AC and SCC Patients
We analyzed the OS and CSS data of patients with different stages and treatment methods (), and the results showed that the selection of treatment methods had a significant impact on the OS and CSS of patients with stage IIB-IVA cervical squamous cell carcinoma and adenocarcinoma. In each stage, the OS of patients undergoing radiotherapy and chemotherapy is the longest among patients in the same stage (), and CSS can also obtain similar conclusions ().
Figure 2 OS and CSS data of patients with different stages and treatment. The time from randomization to death from any cause, is considered the best therapeutic endpoint in tumor clinical trials when the patient’s survival can be extended. It can intuitively determine whether the treatment method used benefits the patient. The time from randomization to death from the cancer. Reflect the effectiveness of targeted treatment methods on cancer.
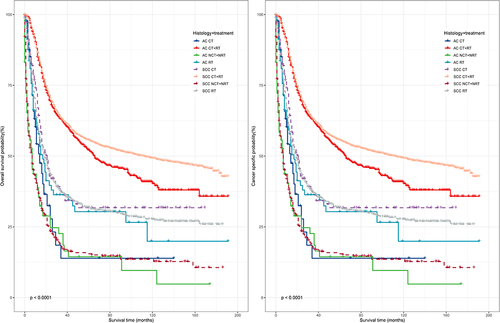
Figure 3 The impact of different treatment on OS in patients with different stages of cervical squamous cell carcinoma and cervical adenocarcinoma.
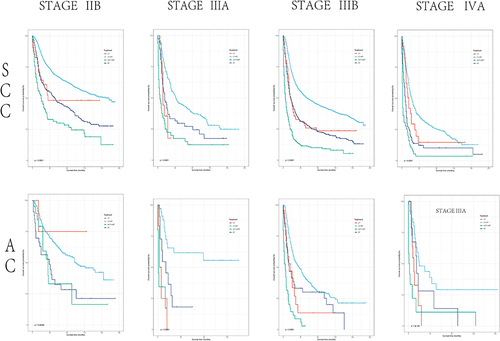
Figure 4 The impact of different treatment on CSS in patients with different stages of cervical squamous cell carcinoma and cervical adenocarcinoma.
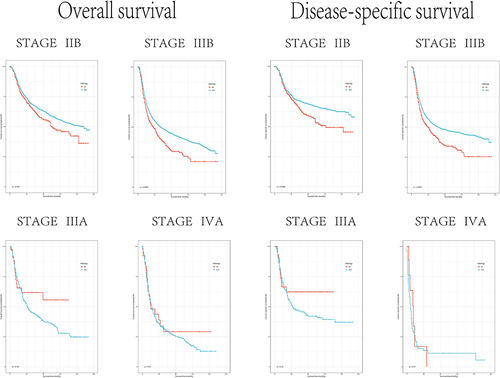
Due to the fact that the OS and CSS of patients with cervical squamous cell carcinoma and adenocarcinoma treated with radiotherapy and chemotherapy are the highest in each stage, we analyzed the treatment outcomes of cervical squamous cell carcinoma and adenocarcinoma patients at different stages after radiotherapy and chemotherapy to compare whether there is a difference in treatment efficacy between the two types of cervical tumors.
The results showed that patients with stage IIIA and IVA cervical squamous cell carcinoma and cervical adenocarcinoma did not show significant differences in OS and CSS after receiving radiotherapy and chemotherapy (stage IIIA: OS: P,0.18, CSS: P,0.24; stage IVA: P,0.61, CSS: P,0.51). There were significant differences in OS and CSS between patients in stage IIB and IIIB after receiving radiotherapy and chemotherapy (stage IIB: OS: P,0.024, CSS: P,0.0046; stage IIIB: P,<0.01, CSS: P<0.01) (). If radiotherapy and no treatment are chosen, there is no significant difference in OS and CSS between patients with cervical squamous cell carcinoma and cervical adenocarcinoma at any stage.
Figure 5 OS and CSS data of cervical squamous cell carcinoma and cervical adenocarcinoma in different stages after radiotherapy and chemotherapy.
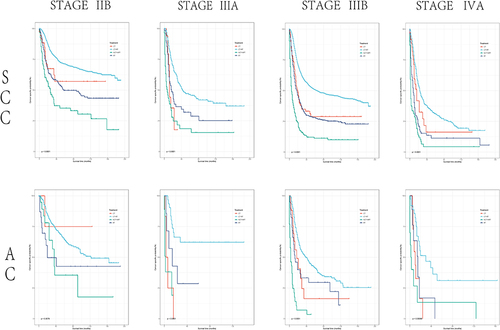
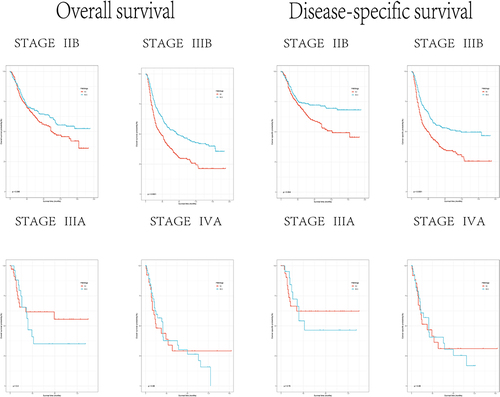
To exclude interfering factors beyond the tumor itself, we used propensity score matching analysis to organize the original data, and determined the adenocarcinoma and squamous cell carcinoma groups in a 1:1 ratio. After PSM, 1057 cases of cervical squamous cell carcinoma and cervical adenocarcinoma were included, and confounding factors and bias between the two groups were balanced, as shown in . The choice of treatment has a significant impact on OS and CSS in patients with cervical squamous cell carcinoma and cervical adenocarcinoma (). The OS and CSS of patients undergoing radiotherapy and chemotherapy after PSM were still significantly higher than other treatment methods (). After analyzing the OS and CSS data of patients with different stages of radiotherapy and chemotherapy, similar results were obtained. There was no significant difference in prognosis between stage IIIA and IVB cervical squamous cell carcinoma and adenocarcinoma patients (stage IIIA: OS: P,0.4, CSS: P,0.79; stage IVA: P,0.99, CSS: P,0.98), but there was a significant difference in prognosis between stage IIB and IIIB cervical squamous cell carcinoma and adenocarcinoma,(stage IIB: OS: P,0.0.066, CSS: P,0.004; stage IIIB: P,<0.01, CSS: P<0.01), as shown in .
Table 3 Baseline Characteristics After Propensity Score Matching of SCC Patients
Figure 6 OS and CSS data of patients with different stages and treatment methods after PSM.
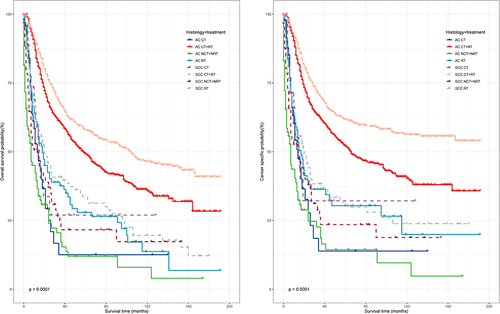
Figure 7 The impact of different treatment methods on OS in patients with different stages of cervical squamous cell carcinoma and cervical adenocarcinoma after PSM.
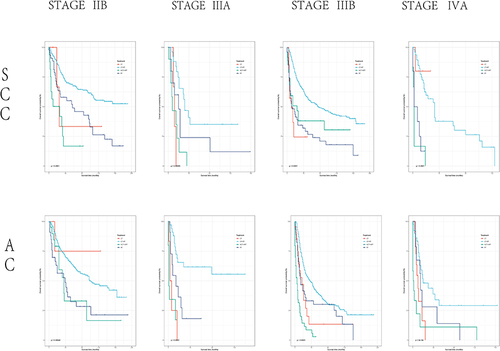
Figure 8 OS and CSS data of different stages of cervical squamous cell carcinoma and cervical adenocarcinoma after radiotherapy and chemotherapy after PSM.
Discussion
After 1970, due to the improvement of early diagnosis methods and the promotion of large-scale screening projects, the incidence rate of cervical cancer gradually decreased, but researchers gradually noticed that the incidence rate of cervical adenocarcinoma gradually increased.Citation10,Citation11 Currently, cervical squamous cell carcinoma and cervical adenocarcinoma are the top two pathological subtypes of cervical cancer, accounting for 80–85% and 15–20% of all cervical cancer cases, respectively.Citation12 There are significant differences in immunological behavior,Citation13–16 tumor suppressor gene expression,Citation17 and apoptosis related protein regulation,Citation18 Immunological characteristicsCitation19 between cervical squamous cell carcinoma and adenocarcinoma, which may further lead to different prognosis.
The basic situation of patients with cervical squamous cell carcinoma and cervical adenocarcinoma is different. The average age of patients with cervical adenocarcinoma is higher than that of patients with cervical squamous cell carcinoma.Citation20 The fitting age incidence rate curve indicates that cervical squamous cell carcinoma reaches its peak before the age of 40, and then decreases, but cervical adenocarcinoma continues to rise,Citation21 indicating that there is a significant difference between the age baseline of patients with cervical adenocarcinoma and squamous cell carcinoma, and age is considered to be one of the factors affecting the prognosis of cervical cancer. Women with race and public insurance are diagnosed with cervical adenocarcinoma at a later stage.Citation3 Further research suggests that living in rural areas and being trapped by economic factors may lead to lower rates of cervical cancer vaccination, screening, and treatment among patients compared to other patients,Citation1 which may lead to differences in the prognosis of evaluating cervical adenocarcinoma and cervical squamous cell carcinoma. In this experiment, there were significant differences in marital status, race, and other factors between cervical squamous cell carcinoma and adenocarcinoma patients. We paired cervical adenocarcinoma and cervical squamous cell carcinoma patients 1:1 using PSM to eliminate the impact of patient basic information and social factors on prognosis.
A small-scale study suggests that the treatment effect of cervical adenocarcinoma is worse than that of cervical squamous cell carcinoma under the same treatment method. Hu et alCitation22 suggested that in IIB-IVA patients, whether alone or in combination with radiotherapy and chemotherapy, the OS and DFS of cervical adenocarcinoma patients were worse than those of SCC patients. Researchers gradually refined the patient staging to Farley et alCitation23 proposed that there was no difference between AC and SCC in stage I cervical cancer patients, but the prognosis of AC was significantly worse than SCC in the median and overall survival analysis of stage II–IV patients. Xie et alCitation24 suggested that in stage IB-IIA cervical cancer patients undergoing surgical treatment, the prognosis of AC was significantly worse, There was no significant difference in the five-year survival rate between cervical squamous cell carcinoma patients and AC patients. In patients from stage IIA to stage IIB, Jung et al’s study showed that compared with CSS, the disease-free survival and overall survival of AC were significantly reduced, and the risk of distant recurrence was higher. Meng et alCitation25 suggested that the difference in prognosis between AC and SCC patients only occurred in stage II and III patients. In our study, we further investigated the OS and CSS of patients with different treatment methods in stage II–IVA patients. After excluding the basic information differences between adenocarcinoma and squamous cell carcinoma patients, the results showed that there were significant differences in prognosis between stage IIB and IIIB patients in radiotherapy and chemotherapy treatment. According to the FIGO staging, stage IIB refers to patients with parametrial metastasis but not reaching the pelvic wall, while stage IIIB refers to patients with cancer lesions affecting the lower third of the vagina and cervical cancer metastasis reaching the pelvic wall or presenting with hydronephrosis or renal dysfunction. The appearance of a certain range of parametrial metastasis is a clinical characteristic of the two stages being the same. This suggests that parametrial infiltration may be an important influencing factor for the difference in prognosis between cervical adenocarcinoma and cervical squamous cell carcinoma. The characteristics of tumor metastases may be completely different from the primary lesion, which may be due to the different effects of the tumor microenvironment on different tumor subtypes.Citation26 At present, there is no research on the specificity of pelvic metastases in cervical cancer. Further research is needed to investigate the changes that occur during metastasis in adenocarcinoma and squamous cell carcinoma. For cervical adenocarcinoma patients with parametrial metastasis, further treatment may be needed. Furthermore, different staging methods may be needed for different types of cervical cancer. It is possible to consider re grouping IIB-IIIB stage patients based on parametrial infiltration, Currently, there is a lack of large-scale clinical data support.
Abbreviations
AC, Adenocarcinoma of cervix; SCC, Squamous carcinoma of cervix; OS, Overall survival; CSS, Cancer Specific Survival; CT, Chemotherapy; RT, Radiotherapy; NCT, No Chemotherapy; NRT, No Radiotherapy; PSM, Propensity Score Matching.
Ethical Approval
Given that data in the SEER database have been de-identified and are publicly available after permission, written informed consent for participation was not required for this study. The requirement of ethical approval for this was waived by the Institutional Review Board of Beijing Obstetrics and Gynecology Hospital. We confirm that this study was performed in accordance with the Declaration of Helsinki.
Disclosure
All authors have no conflicts of interests to declare.
Acknowledgments
We are thankful for the contribution of the SEER database and the registries supplying cancer research information, and thank all colleagues and staff involved in the study for their contributions. Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Additional information
Funding
References
- Buskwofie A, David-West G, Clare CA. A review of cervical cancer: incidence and disparities. J Natl Med Assoc. 2020;112(2):229–232. doi:10.1016/j.jnma.2020.03.002
- Hodgson A, Park KJ. Cervical adenocarcinomas: a heterogeneous group of tumors with variable etiologies and clinical outcomes. Arch Pathol Lab Med. 2019;143(1):34–46. doi:10.5858/arpa.2018-0259-RA
- Smith A, Beavis AL, Rositch AF, Levinson K. Disparities in diagnosis and treatment of cervical adenocarcinoma compared with squamous cell carcinoma: an analysis of the national cancer database, 2004–2017. J Low Genit Tract Dis. 2023;27(1):29–34. doi:10.1097/LGT.0000000000000702
- Hohn AK, Brambs CE, Hiller G, May D, Schmoeckel E, Horn LC. 2020 WHO classification of female genital tumors. Geburtshilfe Frauenheilkd. 2021;81(10):1145–1153. doi:10.1055/a-1545-4279
- Lee J, Kim YT, Kim S, et al. Prognosis of cervical cancer in the era of concurrent chemoradiation from national database in Korea: a comparison between squamous cell carcinoma and adenocarcinoma. PLoS One. 2015;10(12):e144887. doi:10.1371/journal.pone.0144887
- Jung EJ, Byun JM, Kim YN, et al. Cervical adenocarcinoma has a poorer prognosis and a higher propensity for distant recurrence than squamous cell carcinoma. Int J Gynecol Cancer. 2017;27(6):1228–1236. doi:10.1097/IGC.0000000000001009
- Zhou J, Wu SG, Sun JY, et al. Comparison of clinical outcomes of squamous cell carcinoma, adenocarcinoma, and adenosquamous carcinoma of the uterine cervix after definitive radiotherapy: a population-based analysis. J Cancer Res Clin Oncol. 2017;143(1):115–122. doi:10.1007/s00432-016-2246-9
- Nakanishi T, Ishikawa H, Suzuki Y, Inoue T, Nakamura S, Kuzuya K. A comparison of prognoses of pathologic stage Ib adenocarcinoma and squamous cell carcinoma of the uterine cervix. Gynecol Oncol. 2000;79(2):289–293. doi:10.1006/gyno.2000.5935
- Pausch TM, Liu X, Cui J, et al. Survival benefit of resection surgery for pancreatic ductal adenocarcinoma with liver metastases: a propensity score-matched SEER database analysis. Cancers. 2021;14(1):57. doi:10.3390/cancers14010057
- Vesterinen E, Forss M, Nieminen U. Increase of cervical adenocarcinoma: a report of 520 cases of cervical carcinoma including 112 tumors with glandular elements. Gynecol Oncol. 1989;33(1):49–53. doi:10.1016/0090-8258(89)90602-1
- Smith HO, Tiffany MF, Qualls CR, Key CR. The rising incidence of adenocarcinoma relative to squamous cell carcinoma of the uterine cervix in the United States—a 24-Year Population-Based Study. Gynecol Oncol. 2000;78(2):97–105. doi:10.1006/gyno.2000.5826
- Xu Y, Luo H, Hu Q, Zhu H. Identification of potential driver genes based on multi-genomic data in cervical cancer. Front Genet. 2021;12:598304. doi:10.3389/fgene.2021.598304
- Li J, Xue X, Zhang Y, et al. The differences in immune features and genomic profiling between squamous cell carcinoma and adenocarcinoma – a multi-center study in Chinese patients with uterine cervical cancer. Gynecol Oncol. 2023;175:133–141. doi:10.1016/j.ygyno.2023.05.071
- Qiu J, Qu X, Wang Y, et al. Single‐cell landscape highlights heterogenous microenvironment, novel immune reaction patterns, potential biomarkers and unique therapeutic strategies of cervical squamous carcinoma, Human Papillomavirus‐Associated (HPVA) and Non‐HPVA Adenocarcinoma. Adv Sci. 2023;10(10). doi:10.1002/advs.202204951
- Sundfør K, Lyng H, Rofstad EK. Oxygen tension and vascular density in adenocarcinoma and squamous cell carcinoma of the uterine cervix. Acta Oncol. 1998;37(7–8):665–670. doi:10.1080/028418698430016
- Heeren AM, Punt S, Bleeker MC, et al. Prognostic effect of different PD-L1 expression patterns in squamous cell carcinoma and adenocarcinoma of the cervix. Mod Pathol. 2016;29(7):753–763. doi:10.1038/modpathol.2016.64
- Tornesello ML, Buonaguro L, Buonaguro FM. Mutations of the TP53 gene in adenocarcinoma and squamous cell carcinoma of the cervix: a systematic review. Gynecol Oncol. 2013;128(3):442–448. doi:10.1016/j.ygyno.2012.11.017
- Eduardo MGDP, Campaner AB, Silva MALG. Apoptosis phenomena in squamous cell carcinomas and adenocarcinomas of the uterine cervix. Pathol Oncol Res. 2015;21(4):887–892. doi:10.1007/s12253-015-9906-y
- Liu B, Xu Y, Hu B, et al. Immune landscape and heterogeneity of cervical squamous cell carcinoma and adenocarcinoma. Aging. 2024;16(1):568–592. doi:10.18632/aging.205397
- Yang S, Wu Y, Deng Y, et al. Identification of a prognostic immune signature for cervical cancer to predict survival and response to immune checkpoint inhibitors. Oncoimmunology. 2019;8(12):e1659094. doi:10.1080/2162402X.2019.1659094
- Reimers LL, Anderson WF, Rosenberg PS, Henson DE, Castle PE. Etiologic heterogeneity for cervical carcinoma by histopathologic type, using comparative age-period-cohort models. Cancer Epidemiol. 2009;18(3):792–800. doi:10.1158/1055-9965.EPI-08-0965
- Hu K, Wang W, Liu X, Meng Q, Zhang F. Comparison of treatment outcomes between squamous cell carcinoma and adenocarcinoma of cervix after definitive radiotherapy or concurrent chemoradiotherapy. Radiat Oncol. 2018;13(1). doi:10.1186/s13014-018-1197-5
- Farley JH, Hickey KW, Carlson JW, Rose GS, Kost ER, Harrison TA. Adenosquamous histology predicts a poor outcome for patients with advanced‐stage, but not early‐stage, cervical carcinoma. Cancer-Am Cancer Soc. 2003;97(9):2196–2202. doi:10.1002/cncr.11371
- Xie X, Song K, Cui B, Jiang J, Yang X, Kong B. A comparison of the prognosis between adenocarcinoma and squamous cell carcinoma in stage IB–IIA cervical cancer. Int J Clin Oncol. 2018;23(3):522–531. doi:10.1007/s10147-017-1225-8
- Meng Y, Chu T, Lin S, et al. Clinicopathological characteristics and prognosis of cervical cancer with different histological types: a population-based cohort study. Gynecol Oncol. 2021;163(3):545–551. doi:10.1016/j.ygyno.2021.10.007
- Fares J, Fares MY, Khachfe HH, Salhab HA, Fares Y. Molecular principles of metastasis: a hallmark of cancer revisited. Signal Transduct Target Ther. 2020;5(1):28. doi:10.1038/s41392-020-0134-x