
Abstract
Introduction
Assessing COVID-19 risk in asthma patients is challenging due to disease heterogeneity and complexity. We hypothesized that potential risk factors for COVID-19 may differ among asthma age groups, hindering important insights when studied together.
Methods
We included a population-based cohort of asthma patients from the Swedish National Airway Register (SNAR) and linked to data from several national health registers. COVID-19 outcomes included infection, hospitalization, and death from Jan 2020 until Feb 2021. Asthma patients were grouped by ages 12–17, 18–39, 40–64, and ≥65 years. Characteristics of asthma patients with different COVID-19 outcomes were compared with those in their age-corresponding respective source population.
Results
Among 201,140 asthma patients studied, 11.2% were aged 12–17 years, 26.4% 18–39, 37.6% 40–64, and 24.9% ≥65 years. We observed 18,048 (9.0%) COVID-19 infections, 2172 (1.1%) hospitalizations, and 336 (0.2%) COVID-19 deaths. Deaths occurred only among patients aged ≥40. When comparing COVID-19 cases to source asthma populations by age, large differences in potential risk factors emerged, mostly for COVID-19 hospitalizations and deaths. For ages 12–17, these included education, employment, autoimmune, psychiatric, and depressive conditions, and use of short-acting β-agonists (SABA) and inhaled corticosteroids (ICS). In the 18–39 age group, largest differences were for age, marital status, respiratory failure, anxiety, and body mass index. Ages 40–64 displayed notable differences for sex, birth region, cancer, oral corticosteroids, antihistamines, and smoking. For those aged ≥65, largest differences were observed for cardiovascular comorbidities, type 1 diabetes, chronic obstructive pulmonary disease, allergic conditions, and specific asthma treatments (ICS-SABA, ICS-long-acting bronchodilators (LABA)). Asthma control and lung function were important across all age groups.
Conclusion
We identify distinct differences in COVID-19-related risk factors among asthma patients of different ages. This information is essential for assessing COVID-19 risk in asthma patients and for tailoring patient care and public health strategies accordingly.
Plain language summary
Why was the study done?
Asthma patients may be more susceptible to COVID-19 outcomes. Asthma affects all ages, and COVID-19-related risk factors may vary with age. Investigating factors that contribute to COVID-19 infection, hospitalization, and mortality within distinct age groups of asthma patients can yield a more comprehensive understanding of the age-specific nuances of COVID-19 risk.
What did the researchers do and find?
We analyzed sociodemographic characteristics, comorbidities, prescribed medications, and clinical characteristics of asthma patients with COVID-19 in different age groups and compared them with their age-corresponding source asthma populations.
Potential risk factors for COVID-19 and its outcomes differed by age group For ages 12-17, these included education, employment, autoimmune, psychiatric, and depressive conditions, and use of short-acting β-agonists (SABA) and inhaled corticosteroids (ICS). In the 18-39 age group, largest differences were for age, marital status, respiratory failure, anxiety, and body mass index. Ages 40-64 displayed notable differences for sex, birth region, cancer, oral corticosteroids, antihistamines, and smoking. For those aged ≥65, largest differences were observed for cardiovascular comorbidities, type 1 diabetes, chronic obstructive pulmonary disease, allergic asthma, and specific asthma treatments (ICS-SABA, ICS-long-acting bronchodilators (LABA)). Asthma control and lung function were important across all age groups.
What do these results mean?
These results emphasize the importance of recognizing age-specific patterns contributing to COVID-19 risk for consideration in causal analyses. The findings also highlight the necessity for age-specific approaches in both clinical and public health interventions in managing COVID-19 in asthma patients.
Introduction
Numerous risk factors, including advanced age, obesity, male sex, and comorbidities such as cardiovascular diseases, diabetes, chronic obstructive pulmonary disease (COPD), immunodeficiency, and malignancies, have been associated with poorer medical prognosis and outcomes in COVID-19.Citation1,Citation2 However, decreased or increased risk of COVID-19 in patients with asthma and the factors that might drive it are not entirely clear.Citation3–7
Early in the pandemic, COVID-19 risk varied among studies for asthma patients, with some indicating a reduced risk,Citation3 others finding an increased,Citation2,Citation8,Citation9 and othersCitation10,Citation11 reporting no discernible risk. More recent studies have provided valuable insights into the complex nature of COVID-19 risk among asthmatic patients, that may depend on several factors, including underlying comorbidities,Citation12 the type and severity of asthma,Citation1,Citation13–16 level of asthma control,Citation17 and concurrent medications, particularly inhaled corticosteroids (ICS)Citation13,Citation18,Citation19 and oral corticosteroids (OCS).Citation20 Notably, the use of medium to high-dose ICS or OCS, possibly as markers of severe asthma, has shown associations with increased COVID-19 mortality.Citation20,Citation21 Furthermore, there is evidence indicating favorable outcomes for asthma patients receiving anti-type 2 inflammation biologics during COVID-19,Citation22 but this hypothesis lacks robust support from observational studies.Citation23–25
Asthma is a heterogenous disease, affecting a diverse patient population with varied characteristics. The Global Initiative for Asthma (GINA) guidelinesCitation26 underscore the importance of age-specific treatments, emphasizing the need to tailor interventions to suit the requirements of different age groups with different asthma phenotypes. Considering the known very strong age-related risk of severe COVID-19,Citation27 investigating the impact of COVID-19 only across all ages could thus oversimplify findings, potentially overlooking crucial patterns that age-specific analyses might reveal. Our hypothesis was that age-specific analyses would uncover nuanced relationships between asthma and COVID-19, shedding light on distinct risk factors in different age groups. Therefore, we conducted a descriptive analysis to identify age-specific patterns and differences by comparing demographics, comorbidities, medications, and clinical factors of asthma patients with COVID-19 with the frequencies of such characteristics in the corresponding age-specific source asthma populations.
Methods
Study Design and Population
We performed a descriptive cohort study based on data from the SCIFI-PEARL (Swedish COVID-19 Investigation for Future Insights - Population Epidemiology Approach using Register Linkage) project.Citation28 The study population included asthma patients ≥12 years old registered in the Swedish National Airway Register (SNAR)Citation29 on 1 Jan 2020 (index date) with a prior asthma diagnosis (International Classification of Diseases version 10, (ICD-10) code J45) in primary or specialist care and linked with other data using pseudonymized personal identifiers. We categorized asthma patients in alignment with GINA treatment guidelines, distinguishing between adults and children. We grouped adults into three age groups to reflect the onset of COPD around age 40 and the increased prevalence of chronic conditions from age 65. The main analysis focused on age 12 and above due to very few outcomes observed in younger children. Ethical approval was granted by the Swedish Ethical Review Authority (2020–01800 and subsequent amendments). Data access complied with relevant data protection and privacy regulations.
Outcomes and Follow-Up
COVID-19 outcome data was obtained during follow-up from 1 Jan 2020 until 28 Feb 2021 (cutoff before widespread vaccination) from SmiNet (the national database of notifiable diseases),Citation30 the National Patient Register (NPR)Citation31 and the Cause-of-Death Register (CDR).Citation32 Three COVID-19 outcomes were identified: COVID-19 infection as positive polymerase chain reaction test for SARS-CoV-2 in SmiNet, or COVID-19 (ICD-10 U07.1 or U07.2) as primary or secondary diagnosis from inpatient or specialist outpatient care in the NPR, or COVID-19 as underlying or contributing cause of death in the CDR; hospitalization as inpatient care with primary or secondary diagnosis of COVID-19 from NPR; and death records with COVID-19 as underlying or contributing cause of in the CDR. ICU admissions were also identified from the Swedish Intensive Care register but were not further analyzed.
Baseline Characteristics
Sociodemographic data from the Register of Total Population (RTB)Citation33 and the Longitudinal Integrated Database for Health Insurance and Labor Market Studies (LISA)Citation34 at Statistics Sweden included education, employment status, marital status, and region of birth (for detailed definitions see e-Table 1).
Comorbidities were defined based on ICD codes in the National Patient Register during five years prior to 1 Jan 2020, including overall cardiovascular disease, hypertension, heart failure, type 1 and 2 diabetes, respiratory failure, COPD, allergy, cancer, chronic kidney disease, autoimmune disease, sleep apnea, depression, anxiety, and psychiatric disorders (e-Table 1).
Relevant prescribed medications, defined using anatomical therapeutic classification (ATC) codes from the National Prescribed Drug Register (NPDR),Citation35 were included for dispensed prescriptions for 2019 (e-Table 1). Medical treatments were categorized in accordance with the Global Initiative for Asthma (GINA) treatment guidelines into the following groups: inhalation treatments, including short-acting β-agonists (SABA), inhaled corticosteroids (ICS); and inhalation combinations, such as ICS-SABA, ICS with long-acting β-agonists (ICS-LABA); and triple therapy of ICS with LABA and long-acting muscarinic antagonists (ICS-LABA-LAMA). ICS-LABA and ICS-LABA-LAMA regimens may include an add-on SABA. Other medications included were leukotriene receptor antagonists (LTRA), biologics, and oral corticosteroids (OCS) (e-Table 1).
Clinical characteristics obtained from SNAR (e-Table 1) included: asthma control as measured by asthma control test (ACT, categorized as uncontrolled asthma (score ≤19) and controlled asthma (>19)); lung function as measured by spirometry (post-bronchodilator Forced Expiratory Volume in one second percent of predicted (FEV1% predicted), based on the Swedish Hedenström reference valuesCitation36); body mass index (BMI), classified as underweight (<18.5), normal (18.5–24.9), overweight (25.0–29.9) and obese (≥30.0 kg/m2). We defined two asthma phenotypes: (1) allergic asthma, based on present or absent concurrent allergy diagnosis as reported in SNAR, and (2) asthma with obesity, based on BMI≥30. Smoking history from SNAR (never, former, and current smoking) was included as a lifestyle factor. Since spirometry, BMI, ACT, and smoking were not measured on every visit, we relied on the most recently recorded measurement in the period 2015–2019 to mitigate missingness.
Statistical Analysis
We performed descriptive analyses. Categorical variables were reported as frequencies and proportions, and continuous variables as means with standard deviation, or as medians and interquartile ranges (IQR). For the main analysis, characteristics of asthma patients with COVID-19 infection, hospitalization and death were compared to their respective age-specific asthma source population, which includes all asthma patients in the specific age group. Relative differences between groups were evaluated using standardized mean differences (SMDs),Citation37 which were also visualized graphically. SMDs were calculated using the TableOne package in R,Citation38 which compares variables between two groups. A standardized difference can be obtained for each variable. For continuous variables, means are compared and standardized and for binary variables, proportions are compared and standardized.Citation39,Citation40 For multinomial variables, a multivariate Mahalanobis distance is used.Citation40 The SMD in principle compares the difference in means in units of the pooled standard deviation,Citation41 for different variable types. Thus it is not influenced by sample size and can be used to compare balance between groups in measured variables, facilitating comparison of the relative balance of variables measured in different units.Citation42 SMDs greater than 0.1 were considered indicators of substantial differences.Citation39,Citation42 Data management was performed in Stata 17.1, while statistical analysis and visualization were conducted in R 4.2.2.
Results
Cohort Characteristics
We studied a cohort of 201,140, asthma patients, comprised of 11.2% aged 12–17 years, 26.4% aged 18–40 years, 37.6% aged 40–64 years and 24.9% aged 65 and over (). Among them, 18,048 (9.0%) contracted COVID-19, whereof 2172 (1.1%) were hospitalized, and 336 (0.2%) died from COVID-19 by end of follow-up ().
Table 1 Socio-Demographic Characteristics of a Population-Based Cohort of Asthma Patients in Sweden on 1 Jan 2020, Overall and for Patients with Three Different COVID-19 Outcomes from 1 Jan 2020 to 28 Feb 2021 (n (%) or Mean (SD))
Severe COVID-19 leading to hospitalization and death was more common among adults than the 12–17 age group, with deaths only in patients aged 40 and above, especially 65 and older (). Across all outcomes, COVID-19 impacted more women (58.3% to 60.6%) (), although males dominated in the age group 12–17 (52.3%) (e-Table 2a) and for deaths in ages 40–64 (51.3%) (e-Table 2b). In age groups below 40, proportion of women was higher in asthma patients with COVID-19 outcomes than the respective source population. Conversely, for those aged 40 and older, the proportion of men with COVID-19 outcomes surpassed that of men in the respective source population (e-Table 2a and e-Table 2b).
Salient Characteristics in Asthma Patients with COVID-19
Results are presented separately for each COVID-19 outcome. shows the absolute value of the standardized differences in frequency of characteristics among patients with different COVID-19 outcomes from the expected based on the respective source population, with substantial differences (SMD > 0.1) in bold. present, the side-by-side, absolute frequencies for some characteristics, namely comorbidities and prescribed medications, respectively, to illustrate the same differences.
Figure 1 Standardized mean differences (SMD)* between characteristics of asthma patients with COVID-19 infections, hospitalizations, and deaths in Sweden during the period 1 Jan 2020 to 28 Feb 2021, compared to expected characteristics of the source asthma population of the same age group. COPD, chronic obstructive pulmonary disease; ICS, inhaled corticosteroids; OCS, oral corticosteroids; ACE, angiotensin converting enzyme inhibitors; ARB, angiotensin receptor blockers; SABA, short-acting bronchodilator agonists; LABA, long-acting bronchodilator agonists; SAMA, short-acting muscarinic antagonists; LAMA, long-acting muscarinic antagonists; LTRA, leukotriene receptor antagonists; COVID-19, Coronavirus disease 2019; ICU, intensive care unit. ACT, Asthma Control Test; FEV1, Forced Expiratory Volume in 1 second, percent of predicted.

Figure 2 Prevalence of comorbidity among asthma patients of different age groups in Sweden during the 5 years up to 1 January 2020, among those who had COVID-19 outcomes between 1 Jan 2020 and 28 Feb 2021, and patients in the source asthma population of the same age group. Comorbidities and outcomes meeting each group’s minimum count required (5 individuals) are shown. COVID-19, Coronavirus 2019; COPD, chronic obstructive pulmonary disease.
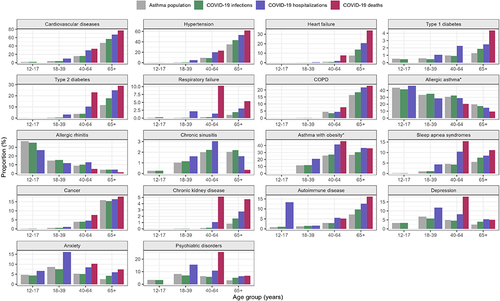
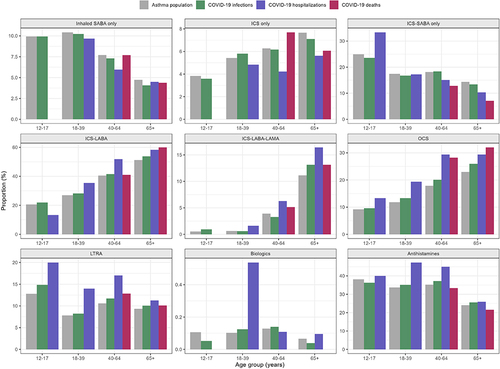
Figure 3 Prevalence of prescribed medications among asthma patients of different age groups in Sweden during the one year up to 1 January 2020, among those who had COVID-19 outcomes between 1 Jan 2020 and 28 Feb 2021, and asthma patients in the source asthma population within the specific age group. Prescribed medication only included those of respiratory indications, the other studied medications were excluded and outcomes meeting the minimum count required (5 individuals) in each group are shown. ICS, inhaled corticosteroids; LABA, long-acting beta-agonists; SABA, short-acting beta-agonists; LTRA, leukotriene receptor antagonists; OCS = oral corticosteroids.
COVID-19 Infection
Compared to the same-age asthma source population, large differences were evident only in age and employment status for asthma patients aged 12–17, and only in employment for those aged 18–39 among asthma patients aged <40 years with COVID-19 infection (, e-Table 3). Older age groups (≥40) also displayed larger than expected differences in age, marital status, and region of birth, with the 65 and older cohorts exhibiting particularly pronounced differences, and the 40–64 group showing the largest difference for employment (, e-Table 3). Notably, the 65 and older group showed larger than expected differences in prior cardiovascular diseases, type 2 diabetes, asthma control, and BMI, while the 40–64 group exhibited substantially larger than expected difference in smoking (, e-Table 3, , e-Table 4a and e-Table b).
COVID-19 Hospitalization
There were many substantial differences between hospitalized asthma patients with COVID-19 and respective asthma source populations (, e-Table 3). Notably, the most pronounced differences in characteristics were specific to distinct age groups. Specifically, patients aged 12–17 exhibited largest differences in education, employment, autoimmune disease, depression, psychiatric disorders, inhaled SABA, ICS, ICS-SABA, allergic rhinitis, asthma control and lung function (, e-Table 3, e-Tables 4a and e-Table 4b, e-Tables 5a and e-Table 5b). Patients aged 18–39 showed largest differences were in age, marital status, respiratory failure, BMI and anxiety. Those aged 40–64 displayed the largest differences in sex, region of birth, ICS-LABA, OCS and asthma with obesity. For those aged 65 and older, the most pronounced differences were in cardiovascular diseases, type 1 diabetes, COPD, chronic kidney disease, ICS-LABA-LAMA and allergic asthma (, e-Table 3).
COVID-19 Death
Asthma patients who died from COVID-19 were most obviously different from the respective source populations across many characteristics (, e-Table 3, e-Figure 1). In the 40–64 age group, more pronounced differences were observed for sex, employment status, region of birth, type 2 diabetes, respiratory failure, cancer, chronic kidney disease, depression, psychiatric disorders, sleep apnea and chronic sinusitis. The ≥65 age group showed larger differences from expected in age, education level, marital status, cardiovascular comorbidities, type 1 diabetes, autoimmune disease, anxiety, COPD and allergic asthma (, e-Table 3). For medication usage, particularly OCS and antihistamines differed the most from expected in the 40–64 age group, while ICS-SABA, ICS-LABA and OCS usage differed notably among those aged 65 and older (, e-Table 3, e-Table 5b). Asthma control and lung function also differed substantially from expected in individuals aged 40 and above, particularly in the 40–64 age group, with smoking differing only within this age group (, e-Tables 3, e-Table 6a, e-Table 6b).
ICU admissions and pediatrics
We observed 254 ICU admissions across age groups: 3 in ages 12–17 (<1%), 13 (5.12%) in 18–39, 144 (56.7%) in 40–64, and 94 (37.0%) in those ≥65 years (e-Table 7). Similarly, among pediatric asthma patients under 12 (totaling 12,700), 580 (4.5%) were infected with COVID-19, with only 8 (<1%) requiring hospitalization (e-Table 8). Due to limited numbers, these data were not further analyzed.
Discussion
In our comprehensive real-world asthma register study, we observed substantial age-related differences in COVID-19 outcomes (being infected, hospitalized, or dying) among asthma patients. The findings suggest potential risk factors specific to different age groups. In the age 12–17 factors related with COVID-19 hospitalization were education, employment, autoimmune disease, depression, psychiatric disorders, and SABA and ICS treatment. In the 18–39 age group, age, marital status, respiratory failure, anxiety, sleep apnea and obesity were of importance. For those aged 40–64, important factors include sex, cancer, chronic kidney disease, ICS-LABA combinations, OCS, antihistamines, BMI, and smoking status. In those age 65 and above, cardiovascular comorbidities, type 1 diabetes, autoimmune disease, anxiety, heart failure, COPD, and allergic asthma, ICS-SABA, ICS-LABA, and OCS emerged as most notable Uncontrolled asthma and lower lung function were important across all age groups and for the two severe outcomes of COVID-19 hospitalization and death.
Demographic Factors
Our results align with previous findings of asthma COVID-19 cohorts from various countries, including France,Citation43 the USA,Citation11,Citation44–46 South Korea,Citation9,Citation47 BelgiumCitation10 and the UK,Citation48 showing a higher proportion of COVID-19 outcomes in women than men. However, we observed variations across age groups, where more women appeared susceptible to outcomes in younger populations, and more men in older age groups. This underscores the importance of considering age in understanding asthma patients’ COVID-19 susceptibility. Moreover, large differences from expected in respective source populations for education, employment status, and country of birth, within the different age groups, underscores the role of these factors in shaping COVID-19 risk in different ways for different age strata of asthma patients. For instance, we observed that COVID-19 deaths were more common among unemployed individuals aged 65 and above, possibly due to an increased risk of transmission associated with factors linked to lower socioeconomic status, in this case unemployment, as supported by prior research.Citation49
Comorbidities
Inherent to younger age, our findings indicate fewer comorbidities in the young asthma patients. Yet, large differences in autoimmune diseases, depression, and psychiatric conditions were observed in the 12–17 age group hospitalized for COVID-19 compared to expected in the same-age asthma source population. In general populations, autoimmune diseases potentially increase susceptibility to infectious agents, particularly when regular immunosuppressants are used.Citation50 Depression, anxiety, and psychiatric diagnoses have been identified as significant risk factors for COVID-19 hospitalization in both young and older adults, highlighting the intricate relationship between mental and somatic health.Citation51,Citation52 Our current results for asthma patients of all age groups expands on this knowledge. This is particularly important during pandemics and restrictions when psychological issues may worsen, and access to medical, psychiatric, and psychological services could be disrupted.
The higher than expected prevalence of comorbidities such as hypertension, diabetes, obesity, and heart failure in asthma patients aged 40 and above with COVID-19 who were hospitalized and died aligns with existing literature on respiratory diseases, reporting higher rates of these risk factor comorbidities in COVID-19 hospitalizationsCitation8 and deaths.Citation9,Citation48 This study highlights specific, risk factors for COVID-19 relevant for different age groups with asthma, including potential cardiovascular risk in individuals under 40, cancer, smoking, and BMI for those aged 40–64, and heart failure, allergies, type 1 diabetes and COPD for individuals aged 65 and above. Our results show that older asthma patients (≥40 years) who died from COVID-19 had lower-than-expected prevalence of asthma with concurrent allergic conditions. This finding aligns with existing evidence that indicates atopic conditions are less common in severe COVID-19 cases,Citation53,Citation54 possibly due to a type 2 immune responseCitation55,Citation56 or the downregulation of ACE-2 receptor in allergic asthma patients.Citation57 The present study suggests that it is not appropriate to extrapolate explanations regarding atopic status and allergies to older adults, as this relationship appears to vary with age groups. In our study’s classification of asthma as “allergic vs non-allergic”, with a rather broad categorization of allergic conditions as reported in SNAR (allergy yes/no), there may be some misclassification between the groups. However, the spectrum of allergic diseases in the allergic asthma group is as expected and the misclassification between these groups would likely be limited and non-differential. Further research is needed to explore the role of allergic asthma as a potential risk factor in different age strata, especially in the elderly, where it appears to hold particular importance.
Medications
We consistently observed age- specific deviations from the expected in asthma medication use among asthma patients with COVID-19. For instance, in the 12–17 age group, large differences in the use of SABA, ICS and ICS-SABA were evident in the hospitalized group, although based on low numbers. In older age groups (≥40 years), we observed a higher than expected use of ICS-LABA or ICS-LAMA combinations and use of OCS. SABA is often still used as monotreatment in mild asthma. A Swedish study has highlighted the association between high childhood SABA use and asthma exacerbations, potentially due to undertreatment of underlying inflammation.Citation58 This association may, in part, relate to our finding that children who relied on ICS-SABA only were overrepresented among those hospitalized due to COVID-19. Recent asthma treatment guidelines emphasize regular controller treatment and recommend a transition toward the use of ICS-LABA or ICS-containing treatment, even in mild asthma.Citation26 Our findings suggest that this new treatment approach might also help to safeguard children against COVID-19 hospitalization and possibly future viral infections. Furthermore, as OCS is often prescribed for asthma exacerbations,Citation26 our findings suggest that previous asthma exacerbations could be a risk factor for hospitalization and death in COVID-19, especially among older age groups. Notably, previous studies have used OCS prescriptions to define severe asthma, and severe asthma has been associated with COVID-19-related mortality.Citation20,Citation23 Biologic therapies, also employed in severe asthma management, are hypothesized to potentially impact asthma and COVID-19 outcomes.Citation54 However, their influence could not be assessed in our dataset due to infrequent usage. Drawing conclusions about the relationship between medication use and COVID-19 is complex and requires careful consideration of various factors such as dosage, timing, confounding variables, and selection of comparison groups. Our study strongly suggests age-stratified analyses will be most informative, promoting increased homogeneity in treatment groups and enabling more meaningful comparisons.
Aside from the treatment-related findings, our study also underscores the importance of asthma severity, as measured by eg, the asthma control test and lung function - in alignment with earlier studies.Citation15,Citation21,Citation59 We further highlight BMI and smoking as potentially important risk factors for asthma patients, as previously reported,Citation11,Citation44,Citation60 particularly in those aged 40 and above.
Strengths and Limitations
Strengths of this study include using a large real-world population-representative cohort from a clinical register of asthma patients in Sweden, with sufficient power to illustrate the inherent variability of patient characteristics across different age groups, spanning adolescents to several adult age groups, and for different COVID-19 outcomes. An important feature of our analysis is the focus on the pre-vaccination phase of the pandemic, allowing a view of the potential age-specific risk factor patterns related to COVID-19 natural disease progression. However, one limitation is its descriptive nature, precluding formal causal inferences. Yet the age-stratified approach intentionally aims to illustrate large age-specific differences likely related at least partly to the age-related heterogeneity of asthma and of asthma therapy – thus providing important information on potentially relevant risk factors and confounders for different age groups that could be useful in future studies. However, our approach may not fully capture the heterogeneity within each age group and alternative categorization strategies could be explored in future studies.
Conclusion
This study identified age group specific risk factors for COVID-19 in asthma patients, highlighting variability across different age groups. These findings suggest that research on asthma and COVID-19 should consider age stratification as a fundamental element in study design. Moreover, our findings underscore the importance of tailoring COVID-19 risk assessment in asthma patients based on their age group, rather than across all patients uniformly. Healthcare practitioners and policymakers should consider these age-specific risk factors to develop more precise strategies for managing and supporting asthma patients.
Author Contributions
All authors contributed significantly to the reported work, whether in conception, study design, execution, data acquisition, analysis and interpretation, or across all these domains; participated in drafting, revising, or critically reviewing the article; provided final approval for publication; selected the journal for submission; and commit to being accountable for all aspects of the project.
Disclosure
CS has received personal and institutional fees from AstraZeneca, Boehringer-Ingelheim, Chiesi, TEVA and Novartis. LEGWV has received grants and personal fees from AstraZeneca and personal fees from GSK, Novartis, Boehringer-Ingelheim, Menarini, Resmed, Chiesi, AGA Linde, Zambon and Pulmonx. FN was an employee of AstraZeneca until 2019 and holds some AstraZeneca shares. The authors report no other conflicts of interest in this work.
Acknowledgments
We thank the SCIFI-PEARL team members, who provided insight, help and guidance that greatly assisted the research. Further acknowledgments are given to all the patients and healthcare professionals who contribute with registrations in SNAR, and to the SNAR steering committee and register coordinators.
Additional information
Funding
References
- Gao Y, Ding M, Dong X. et al. Risk factors for severe and critically ill COVID‐19 patients: a review. Allergy. 2021;76(2):428–455. doi:10.1111/all.14657
- Williamson EJ, Walker AJ, Bhaskaran K, et al. Factors associated with COVID-19-related death using openSAFELY. Nature. 2020;584(7821):430–436. doi:10.1038/s41586-020-2521-4
- Sunjaya AP, Allida SM, Di Tanna GL, Jenkins CR. Asthma and COVID-19 risk: a systematic review and meta-analysis. Eur Respir J. 2022;59(3):2101209. doi:10.1183/13993003.01209-2021
- Ubah CS, Kearney GD, Pokhrel LR. Asthma may not be a potential risk factor for severe COVID-19 illness: a scoping review. Environ Health Ins. 2024;18:11786302231221925. doi:10.1177/11786302231221925
- Otunla A, Rees K, Dennison P, et al. Risks of infection, hospital and ICU admission, and death from COVID-19 in people with asthma: systematic review and meta-analyses. BMJ EBM. 2022;27(5):263–273. doi:10.1136/bmjebm-2021-111788
- Bloom C. Covid‐19 pandemic and asthma: what did we learn? Respirology. 2023;28(7):603–614. doi:10.1111/resp.14515
- Assaf S, Stenberg H, Jeseňák M, Tarasevych S, Hanania N, Diamant Z. Asthma in the era of COVID-19. Respir Med. 2023;null:107373. doi:10.1016/j.rmed.2023.107373
- Izquierdo JL, Almonacid C, González Y, et al. The impact of COVID-19 on patients with asthma. Eur Respir J. doi:10.1183/13993003.03142-2020
- Lee SC, Son KJ, Han CH, Jung JY, Park SC. Impact of comorbid asthma on severity of coronavirus disease (COVID-19). Sci Rep. 2020;10(1):21805. doi:10.1038/s41598-020-77791-8
- Calmes D, Graff S, Maes N, et al. Asthma and COPD are not risk factors for ICU stay and death in case of SARS-CoV2 Infection. J Allergy Clin Immunol Pract. 2020;(1):160–169. doi:10.1016/j.jaip.2020.09.044
- Chhiba KD, Patel GB, THT V, et al. Prevalence and characterization of asthma in hospitalized and nonhospitalized patients with COVID-19. J Allergy Clin Immunol. 2020;146(2):307–314.e4. doi:10.1016/j.jaci.2020.06.010
- Skevaki C, Chinthrajah RS, Fomina D, et al. Comorbidity defines asthmatic patients’ risk of COVID-19 hospitalization: a global perspective. J Allergy Clin Immunol. 2023;151(1):110–117. doi:10.1016/j.jaci.2022.09.039
- Bloom CI, Cullinan P, Wedzicha JA. Asthma phenotypes and COVID-19 risk: a population-based observational study. Am J Respir Crit Care Med. 2022;205(1):36–45. doi:10.1164/rccm.202107-1704OC
- Karlsson Sundbaum J, Vanfleteren LEGW, Konradsen JR, Nyberg F, Ekberg-Jansson A, Stridsman C. Severe COVID-19 among patients with asthma and COPD: a report from the Swedish national airway register. Ther Adv Respir Dis. 2021;15:175346662110497. doi:10.1177/17534666211049738
- Selberg S, Karlsson Sundbaum J, Konradsen JR, et al. Multiple manifestations of uncontrolled asthma increase the risk of severe COVID-19. Respir Med. 2023;216:107308. doi:10.1016/j.rmed.2023.107308
- Zein JG, Mitri J, Bell JM, Lopez D, Strauss R, Attaway AH. The relationship of asthma severity to COVID-19 outcomes. J Aller Clini Immun in Prac. 2022;10(1):318–321.e2. doi:10.1016/j.jaip.2021.10.041
- Dolby T, Nafilyan V, Morgan A, Kallis C, Sheikh A, Quint JK. Relationship between asthma and severe COVID-19: a national cohort study. Thorax. 2023;78(2):120–127. doi:10.1136/thoraxjnl-2021-218629
- Furci F, Caminati M, Senna G, Gangemi S. The potential protective role of corticosteroid therapy in patients with asthma and COPD against COVID-19. Clin Mol Allergy. 2021;19(1):19. doi:10.1186/s12948-021-00159-4
- Schultze A, Walker AJ, MacKenna B, et al. Risk of COVID-19-related death among patients with chronic obstructive pulmonary disease or asthma prescribed inhaled corticosteroids: an observational cohort study using the OpenSAFELY platform. Lancet Respir Med. 2020;8(11):1106–1120. doi:10.1016/S2213-2600(20)30415-X
- Shi T, Pan J, Vasileiou E, Robertson C, Sheikh A. Risk of serious COVID-19 outcomes among adults with asthma in Scotland: a national incident cohort study. Lancet Respir Med. 2022;10(4):347–354. doi:10.1016/S2213-2600(21)00543-9
- Karlsson Sundbaum J, Konradsen JR, LEGW V, et al. Uncontrolled asthma predicts severe COVID-19: a report from the Swedish national airway register. Ther Adv Respir Dis. 2022;16:175346662210911. doi:10.1177/17534666221091183
- Poddighe D, Kovzel E. Impact of anti-type 2 inflammation biologic therapy on COVID-19 clinical course and outcome. JIR. 2021;Volume 14:6845–6853. doi:10.2147/JIR.S345665
- Adir Y, Humbert M, Saliba W. COVID-19 risk and outcomes in adult asthmatic patients treated with biologics or systemic corticosteroids: nationwide real-world evidence. J Allergy Clin Immunol. 2021;148(2):361–367.e13. doi:10.1016/j.jaci.2021.06.006
- Rial MJ, Valverde M, Del Pozo V, et al. Clinical characteristics in 545 patients with severe asthma on biological treatment during the COVID-19 outbreak. J Aller Clini Immun in Prac. 2021;9(1):487–489.e1. doi:10.1016/j.jaip.2020.09.050
- Papaioannou AI, Fouka E, Tzanakis N, et al. SARS-Cov-2 infection in severe asthma patients treated with biologics. J Aller Clini Immun in Prac. 2022;10(10):2588–2595. doi:10.1016/j.jaip.2022.05.041
- 2023 GINA Main Report. Global Initiative for Asthma - GINA. https://ginasthma.org/2023-gina-main-report/.
- Romero Starke K, Petereit-Haack G, Schubert M, et al. The age-related risk of severe outcomes due to COVID-19 infection: a rapid review, meta-analysis, and meta-regression. IJERPH. 2020;17(16):5974. doi:10.3390/ijerph17165974
- Nyberg F, Franzén S, Lindh M, et al. Swedish covid-19 investigation for future insights – a population epidemiology approach using register Linkage (SCIFI-PEARL). CLEP. 2021;Volume 13:649–659. doi:10.2147/CLEP.S312742
- Stridsman C, Konradsen J, Vanfleteren L, et al. The Swedish National Airway Register (SNAR): development, design and utility to date. European Clinic Respira Jour. 2020;7(1):1833412. doi:10.1080/20018525.2020.1833412
- Rolfhamre P, Jansson A, Arneborn M, Ekdahl K. SmiNet-2: description of an internet-based surveillance system for communicable diseases in Sweden. Euro Surveill. 2006;11(5):103–107. doi:10.2807/esm.11.05.00626-en
- Ludvigsson JF, Andersson E, Ekbom A, et al. External review and validation of the Swedish national inpatient register. BMC Public Health. 2011;11(1):450. doi:10.1186/1471-2458-11-450
- Brooke HL, Talbäck M, Hörnblad J, et al. The Swedish cause of death register. Eur J Epidemiol. 2017;32(9):765–773. doi:10.1007/s10654-017-0316-1
- Ludvigsson JF, Almqvist C, Bonamy AKE, et al. Registers of the Swedish total population and their use in medical research. Eur J Epidemiol. 2016;31(2):125–136. doi:10.1007/s10654-016-0117-y
- Ludvigsson JF, Svedberg P, Olén O, Bruze G, Neovius M. The longitudinal integrated database for health insurance and labour market studies (LISA) and its use in medical research. Eur J Epidemiol. 2019;34(4):423–437. doi:10.1007/s10654-019-00511-8
- Wettermark B, Hammar N, MichaelFored C, et al. The new Swedish prescribed drug register—opportunities for pharmacoepidemiological research and experience from the first six months. Pharmacoepidem Drug Safe. 2007;16(7):726–735. doi:10.1002/pds.1294
- Hedenström H, Malmberg P, Agarwal K. Reference values for lung function tests in females. Regression equations with smoking variables. Bull Eur Physiopathol Respir. 1985;21(6):551–557.
- Sullivan GM, Feinn R. Using effect size—or why the P value Is Not Enough. J Grad Med Educa. 2012;4(3):279–282. doi:10.4300/JGME-D-12-00156.1
- Yoshida K, Bartel A, Chipman JJ, et al. tableone: Create “Table 1” to Describe Baseline Characteristics. Available from: https://CRAN.R-project.org/package=tableone. Accessed June 13, 2024.
- Austin PC. Using the standardized difference to compare the prevalence of a binary variable between two groups in observational research. Commun Statis Simula Compu. 2009;38(6):1228–1234. doi:10.1080/03610910902859574
- Yang D, Dalton JE. A unified approach to measuring the effect size between two groups using SAS. 2012. Available from: https://api.semanticscholar.org/CorpusID:9425733. Accessed June 13.
- Flury BK, Riedwyl H. Standard Distance in Univariate and Multivariate Analysis. The American Statistician. 1986;40(3):249–251. doi:10.1080/00031305.1986.10475403
- Austin PC. Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity-score matched samples. Statist Med. 2009;28(25):3083–3107. doi:10.1002/sim.3697
- Beurnier A, Jutant EM, Jevnikar M, et al. Characteristics and outcomes of asthmatic patients with COVID-19 pneumonia who require hospitalisation. Eur Respir J. 2020;56(5). doi:10.1183/13993003.01875-2020
- Wang L, Foer D, Bates DW, Boyce JA, Zhou L. Risk factors for hospitalization, intensive care, and mortality among patients with asthma and COVID-19. J Allergy Clin Immunol. 2020;146(4):808–812. doi:10.1016/j.jaci.2020.07.018
- Lieberman-Cribbin W, Rapp J, Alpert N, Tuminello S, Taioli E. The impact of asthma on mortality in patients with COVID-19. Chest. 2020;158(6):2290–2291. doi:10.1016/j.chest.2020.05.575
- Robinson LB, Wang L, Fu X, et al. COVID-19 severity in asthma patients: a multi-center matched cohort study. J Asthma Pub Online Mar. 2(2021):1–14. doi:10.1080/02770903.2020.1857396
- Choi YJ, Park JY, Lee HS, et al. Effect of Asthma and asthma medication on the prognosis of patients with COVID-19. Eur Respir J. 2020. doi:10.1183/13993003.02226-2020
- Bloom CI, Drake TM, Docherty AB, et al. Risk of adverse outcomes in patients with underlying respiratory conditions admitted to hospital with COVID-19: a national, multicentre prospective cohort study using the ISARIC WHO clinical characterisation protocol UK. Lancet Respir Med. 2021;9(7):699–711. doi:10.1016/S2213-2600(21)00013-8
- Nwaru CA, Santosa A, Franzén S, Nyberg F. Occupation and COVID-19 diagnosis, hospitalisation and ICU admission among foreign-born and Swedish-born employees: a register-based study. J Epidemiol Community Health. 2022;76(5):440–447. doi:10.1136/jech-2021-218278
- Anaya JM, Shoenfeld Y, Rojas-Villarraga A, Levy RA, Cervera R. Autoimmunity: From Bench to Bedside. First edition ed. Center for Autoimmune Diseases Research, School of Medicine and Health Sciences, El Rosario University; 2013.
- Smith ML, Gradus JL. Psychiatric disorders and risk of infections: early lessons from COVID-19. Lancet Healthy Longe. 2020;1(2):e51–e52. doi:10.1016/S2666-7568(20)30020-9
- Yang H, Chen W, Hu Y, et al. Pre-pandemic psychiatric disorders and risk of COVID-19: a UK Biobank cohort analysis. Lancet Healthy Longe. 2020;1(2):e69–e79. doi:10.1016/S2666-7568(20)30013-1
- Scala E, Abeni D, Tedeschi A, et al. Atopic status protects from severe complications of COVID‐19. Allergy. 2021;76(3):899–902. doi:10.1111/all.14551
- Chen C, Song X, Murdock DJ, et al. Association between allergic conditions and COVID-19 susceptibility and outcomes. Ann Allergy Asthma Immunol. 2024;132(5):637–645.e7. doi:10.1016/j.anai.2024.01.011
- Kimura H, Francisco D, Conway M, et al. Type 2 inflammation modulates ACE2 and TMPRSS2 in airway epithelial cells. J Allergy Clin Immunol. 2020;146(1):80–88.e8. doi:10.1016/j.jaci.2020.05.004
- Liuzzo Scorpo M, Ferrante G, La Grutta S. An overview of asthma and COVID-19: protective factors against SARS-COV-2 in pediatric patients. Front Pediatr. 2021;9:661206. doi:10.3389/fped.2021.661206
- Jackson DJ, Busse WW, Bacharier LB, et al. Association of respiratory allergy, asthma, and expression of the SARS-CoV-2 receptor ACE2. J Allergy Clin Immunol. 2020;146(1):203–206.e3. doi:10.1016/j.jaci.2020.04.009
- Melén E, Nwaru BI, Wiklund F, et al. Short-acting β2 </sub> -agonist use and asthma exacerbations in Swedish children: a SABINA Junior study., Pediatric Allergy Immunology, 2022;3311:e13885. 10.1111/pai.13885. Pediatric Allergy and Immunology: Official Publication of the European Society of Pediatric Allergy and Immunology
- Nassoro DD, Mujwahuzi L, Mwakyula IH, Possi MK, Lyantagaye SL. 2021. Asthma and COVID-19: emphasis on adequate asthma control. In: Radovanovic D, editor. Canadian Respiratory Journal. 2021;1–12. doi:10.1155/2021/9621572
- Lovinsky-Desir S, Deshpande DR, De A, et al. Asthma among hospitalized patients with COVID-19 and related outcomes. J Allergy Clin Immunol. 2020;146(5):1027–1034.e4. doi:10.1016/j.jaci.2020.07.026