
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Iron overload causes iron deposition and accumulation in the liver, heart, skin, and other tissues resulting in serious tissue damages. Significant blood clearance from iron and ferritin using wet cupping therapy (WCT) has been reported. WCT is an excretory form of treatment that needs more research efforts. WCT is an available, safe, simple, economic, and time-saving outpatient modality of treatment that has no serious side effects. There are no serious limitations or precautions to discontinue WCT. Interestingly, WCT has solid scientific and medical bases (Taibah mechanism) that explain its effectiveness in treating many disease conditions differing in etiology and pathogenesis. WCT utilizes an excretory physiological principle (pressure-dependent excretion) that resembles excretion through renal glomerular filtration and abscess evacuation. WCT exhibits a percutaneous excretory function that clears blood (through fenestrated skin capillaries) and interstitial fluids from pathological substances without adding a metabolic or detoxification burden on the liver and the kidneys. Interestingly, WCT was reported to decrease serum ferritin (circulating iron stores) significantly by about 22.25% in healthy subjects (in one session) and to decrease serum iron significantly to the level of causing iron deficiency (in multiple sessions). WCT was reported to clear blood significantly of triglycerides, low-density lipoprotein (LDL) cholesterol, total cholesterol, uric acid, inflammatory mediators, and immunoglobulin antibodies (rheumatoid factor). Moreover, WCT was reported to enhance the natural immunity, potentiate pharmacological treatments, and to treat many different disease conditions. There are two distinct methods of WCT: traditional WCT and Al-hijamah (WCT of prophetic medicine). Both start and end with skin sterilization. In traditional WCT, there are two steps, skin scarification followed by suction using plastic cups (double S technique); Al-hijamah is a three-step procedure that includes skin suction using cups, scarification (shartat mihjam in Arabic), and second skin suction (triple S technique). Al-hijamah is a more comprehensive technique and does better than traditional WCT, as Al-hijamah includes two pressure-dependent filtration steps versus one step in traditional WCT. Whenever blood plasma is to be cleared of an excess pathological substance, Al-hijamah is indicated. We will discuss here some reported hematological and therapeutic benefits of Al-hijamah, its medical bases, methodologies, precautions, side effects, contraindications, quantitative evaluation, malpractice, combination with oral honey treatment, and to what extent it may be helpful when treating thalassemia and other conditions of iron overload and hyperferremia.
Video abstract
Point your SmartPhone at the code above. If you have a QR code reader the video abstract will appear. Or use:
Introduction
Cupping therapy is the term given to treatment modalities using sucking cups that are applied to the skin surface at different anatomical points. It includes both dry cupping therapy (DCT) and wet cupping therapy (WCT). WCT is an excretory form of treatment that needs more research as a safe, economic, time-saving technique without serious side effects.Citation1 WCT does not require sophisticated equipment, expensive disposables, or extensive effort to practice.Citation1 There are no serious limitations, precautions, or side effects to discontinue WCT. Interestingly, WCT has solid scientific and medical bases that explain its effectiveness in treating many disease conditions differing in etiology and pathogenesis according to the evidence-based Taibah mechanism (Taibah theory)Citation1 (). WCT includes both the traditional WCT (skin scarification and suction method), and the more comprehensive WCT of prophetic medicine, Al-hijamah (skin suction, scarification, and suction method). We will discuss here some reported hematological and therapeutic benefits of WCT, its medical basis, methodologies, WCT-induced reduction in serum iron and ferritin, combination with oral honey, and to what extent this may be helpful when treating thalassemia, hemochromatosis, sideroblastic anemia, and other conditions of iron overload and hyperferremia.
Important reported therapeutic and hematological benefits of WCT
A single session of WCT (blood cupping therapy, Al-hijamah) was reported to decrease serum ferritin (circulating iron stores) significantly by about 22.25% in healthy subjects (from 129±59.2 to 100.6±45.8 ng/mL).Citation2 The same session of WCT cleared blood significantly of triglycerides, low-density lipoprotein (LDL) cholesterol, total cholesterol, and uric acid.Citation2 In rheumatoid arthritis, WCT cleared patients’ blood of immunoglobulin antibodies (rheumatoid factor) in a time-dependent manner,Citation3 which may increase the therapeutic benefits of WCT. In another report, frequent WCT was reported to decrease serum iron, causing iron deficiency that brought about iron deficiency anemia.Citation4
Potentiation of the natural immunity in the form of physiological leukocytosis and an increased number of natural killer cells were reported after applying WCT.Citation3 That was confirmed by the study of Zhang et al, who reported that traditional WCT decreased serum levels of the immune inhibitory cytokines (eg, immunoglobin E [IgE], interleukin-4 [IL-4], IL-10) and decreased the number of T cytotoxic cells (CD8+) cells. In the same subjects, WCT increased the production of endogenous immunostimulatory cytokines (eg, interferon-gamma, IL-2, complement-3, complement-4, immunoglobulins [IgA, IgG, and IgM]) and activated cells of the immune system (eg, T helper cells), causing an increased ratio of T helper/T cytotoxic cells,Citation5 which may help in treating hepatitis viral infections that may complicate frequent blood transfusions.
Being a mechanical modality of treatment, WCT has no chemical or pharmacological antagonism with pharmacological treatments such as iron chelation therapeutics. As mentioned before, WCT was reported to clear blood significantly of excess pathological substances, which may facilitate and potentiate the related pharmacological and therapeutic effects of coadministered pharmacotherapy.Citation1 Moreover, WCT was reported to significantly decrease the blood pressure, and improve the lipid profile and treat different diseases, such as hypertension and hyperlipidemia.Citation1,Citation2 WCT was reported to exert pharmacological potentiation when treating different diseases and to alleviate drug-induced side effects;Citation1,Citation3 for example, WCT-induced leukocytosis counteracted methotrexate-induced leucopenia when treating rheumatoid patients with Al-hijamah combined with methotrexate.Citation1,Citation3 Interestingly, skin wounding (eg, the minor skin scarifications done during WCT) was reported to enhance the production of endogenous nitric oxide through upregulating the expression of nitric oxide synthase (NOS).Citation1,Citation6 Neuronal NOS messenger ribonucleic acid (mRNA) is upregulated and neuronal NOS protein expression peaks at the late stages of skin wound healing.Citation7 Moreover, inducible NOS mRNA was reported to increase by about tenfold,Citation8 peak 24 hours after wounding, and persist for a few days.Citation9 Nitric oxide exerts many important roles, including antioxidant effects,Citation10 vasodilator functions, and antimicrobial effects,Citation11 among others.Citation1 Recently, Al-hijamah was reported to exert multiple therapeutic health benefits; for example, nonspecific biochemical clearance of serum and interstitial fluids, excretory benefits, antinociceptive (analgesic) effects, anti-inflammatory effects, hemodynamic effects, antiviral effects, anticancer effects, antiallergic effects, respiratory benefits, and neurological health benefits. Moreover, Al-hijamah was reported to exert nonspecific-tissue protective benefits, cardioprotective effects, hepatoprotective benefits, nephroprotective effects, and neuroprotective effects, among others. Therefore, the reported antihypertensive and antihyperlipidemic effects of Al-hijamah may be beneficial in guarding against the development and progression of premature atherosclerosis that is encountered in some diseases, such as thalassemia. We reported Al-hijamah as a promising suggested treatment for hematological conditions characterized by iron overload; eg, hemochromatosis, thalassemia, sideroblastic anemia, and others.Citation11
Indices for evaluating therapeutic effects of Al-hijamah
Recently, we reported the novel therapeutic indices of Al-hijamah for evaluating the health benefits gained from practicing Al-hijamah for treating different disease conditions.Citation11 Such indices included excretion index, purification index, immunological potentiation index, pharmacological potentiation index, and clinical therapeutic index (CTI).
Excretion index (excretion value, EV) is the quantity of noxious substances excreted after the end of the session of Al-hijamah in quantity units/volume units. EV can be calculated by determining the difference in levels of noxious substances before and after Al-hijamah (in quantity units/volume units). An example for that was the decrease in serum ferritin from 129.4 ng/mL (before Al-hijamah) to 100.6 ng/mL (after Al-hijamah):
(1)
Plasma clearance index, or purification index (PI), is the percentage of purification of plasma from any noxious substance or component estimated at different time points after Al-hijamah. PI can be calculated by estimating the difference in the concentration of a noxious substance before and after Al-hijamah divided by its initial plasma concentration level. Using the abovementioned example, PI for plasma from serum ferritin equals
(2)
This means that Al-hijamah induced clearance of more than one-fifth of initial serum ferritin in a single session, which may be promising when treating conditions of iron overload.
Pharmacological potentiation index measures the degree of pharmacological potentiation gained when conventional pharmacological treatments are administered concomitantly with practicing Al-hijamah. It also compares the gained therapeutic benefits versus using conventional pharmacological treatment as a sole treatment. When treating rheumatoid arthritis patients using conventional pharmacological treatment, the initial serum rheumatoid factor was 129.75 to 131.47 IU/mL, which decreased to 122 IU/mL when conventional pharmacological treatment was used as a sole treatment.Citation3 A combination of conventional pharmacological treatment plus Al-hijamah caused serum rheumatoid factor to decrease to 51.46 IU/mL. Pharmacological potentiation index for decreasing serum rheumatoid factor:
(3)
Thus, combining Al-hijamah with pharmacological treatment increased the gained therapeutic effects more than ten times.
Immunological index measures the degree of immunological potentiation gained after Al-hijamah; eg, natural killer cell lymphocytosis. It can be calculated by measuring the number of natural killer cells before and after Al-hijamah. A percentage count of natural killer cells before Al-hijamah was 8.5% and increased to 11.33% after Al-hijamah. II for the increase in the count of natural killer cells can be calculated as
(4)
Thus, natural immunity using natural killer (NK) cells increased by about 133% after Al-hijamah.
CTI is the improvement percentage of an investigated clinical parameter (eg, diastolic blood pressure value, systolic blood pressure value, pain intensity value, disease activity value, and others) after Al-hijamah (as a sole treatment or as a combined treatment) was measured at different time points versus the same value before Al-hijamah. Diastolic blood pressure was 81.1 mmHg before Al-hijamah and significantly decreased to 75 mmHg after Al-hijamah.Citation2 The improvement in diastolic blood pressure equals
(5)
When calculating the percentage improvement versus the initial value of systolic blood pressure, CTI can be derived from the formula:
(6)
Thus, diastolic blood pressure decreased by 7.5% in healthy subjects after Al-hijamah.
Scientific principles of WCT and Al-hijamah
Making use of simple scientific facts in physiology and histology may improve treatment outcomes. For example, human skin has a superficial network of fenestrated dermal capillariesCitation13 () that may help percutaneous pressure-dependent and size-dependent filtration and blood clearance upon application of external suction pressure; WCT utilizes a physiological filtration and an excretory principle for inducing blood clearance. Capillary pores and fenestrations are 6–12 nm (and may reach up to 100 nm in diameter) (),Citation12,Citation14 which cannot filter intact blood cells (having diameters in microns).Citation14 This may carry a lot of similarities with renal glomerular filtration. This confirms the fact that Al-hijamah utilizes a physiological principle for inducing blood clearance (pressure-dependent filtration followed by excretion) that is better than the chemical methods of blood clearance; eg, dialysis (concentration-dependent excretion). All this constituted the basis for Taibah mechanism (Taibah theory) for scientific basis of Al-hijamah and cupping therapy.Citation1
Figure 1 Skin histology is ideal for practicing wet cupping therapy.
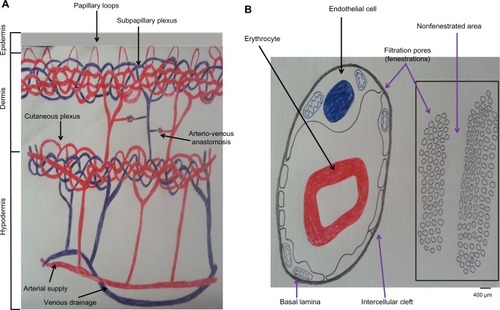
Moreover, skin comprises three layers: epidermis, dermis, and hypodermis. Epidermis is the most superficial layer, and does not contain blood capillaries. The most superficial layer of the epidermis is the horny cell layer that is the keratinized epithelium layer (stratum corneum). This keratinized cell layer constitutes the skin barrier (10–20 μm) that provides the function of protecting the skin and the underlying structure through preventing the entry and exit of substances through the skin. Immediately below the stratum corneum, there are the viable epidermal cell layers (50–100 μm thick), which are responsible for generating the stratum corneum.Citation15
The dermis (1–2 mm thick) is the second layer of the skin that lies immediately beneath the epidermis. The dermis constitutes the mechanical support for the skin. Unlike the epidermis, the dermis contains fenestrated skin capillaries that are suitable for pressure-dependent filtration upon application of negative suction pressure, as that done during Al-hijamah.Citation15 Interestingly, the ultrastructure of the skin vasculature confirms that the arterial blood supply of the skin comes through the cutaneous arteries that run in the hypodermis, then give rise to branches that anastomose to form the cutaneous capillary plexus of capillary networks at the dermis–hypodermis junction. That cutaneous capillary plexus gives rise to the subpapillary plexus of fenestrated capillaries that lie at the dermoepidermal junction.Citation16 The subpapillary plexus gives rise to capillary loops in each dermal papilla. Venous drainage of the skin is arranged in plexuses corresponding to the arterial supply.Citation16 Based on that, skin scarification done during Al-hijamah should be so superficial as to just open the skin barrier and reach the superficial dermal capillaries.
Scarifying the skin deeply during Al-hijamah is a malpractice that may cause damage to the fenestrated dermal capillaries and impair the filtration function exerted during Al-hijamah, as we will discuss in the side effects and malpractice of Al-hijamah. Huber et alCitation17 reported that many different methods for creating suction pressure can be utilized for sucking skin inside sucking cups during cupping therapy. However, some variable differences in pressure may occur and govern the proper choice of the most suitable method to exert such suction pressure. Huber et al studied the mean suction pressure produced during mechanical suction, lighter flame 2 cm suction, lighter flame 4 cm suction, and alcohol flame, and found that large differences in suction magnitude were produced. Negative suction was −200±30 hecta Pascal (hPa) (=−150±23 mmHg) when using 2 cm flame, −310±30 hPa (−232.5±23 mmHg) with 4 cm flame, −560±30 hPa (−420±23 mmHg) with burning an alcohol-soaked cotton swab, and −270±16 hPa (−202±12 mmHg) with rubber balloon mechanical suction. The pressure produced through the rubber balloon was the easiest technically, moderate in intensity, maximal in safety (not harmful), and was the most reproducible when repeating cupping therapy.Citation17
Methods of practicing WCT
DCT is a one-step therapeutic modality that involves skin suction only and is done mainly for the purpose of pain relief or to stimulate blood flow at a given anatomical area of the human body.Citation11 WCT includes both cupping and bloodletting. There are two reported methodologies of WCT: traditional WCT and Al-hijamah (WCT of prophetic medicine). In both, sterilization using alcohol or povidone iodine in a strict aseptic environment is necessary. Traditional WCT has two steps: skin scarification (puncturing) followed by skin suction (cupping); ie, the double S method or puncturing and cupping method of WCT.Citation18 Al-hijamah has three main steps: skin suction (cupping step using sucking cups) (), skin scarification (puncturing skin) (), and second skin suction (cupping) (); ie, the triple S method or cupping, puncturing, and cupping method of WCT.Citation1,Citation18 The methodology of using traditional WCT for treating many different disease conditions was reported in many published research studies from Germany,Citation19 Korea,Citation20 and the People’s Republic of China.Citation21–Citation24 The methodology of traditional WCT described in those published studies is different from Al-hijamah, which was described in reports from Saudi ArabiaCitation25 and other countries.Citation26,Citation27
Figure 2 First step of Al-hijamah (first suction step).
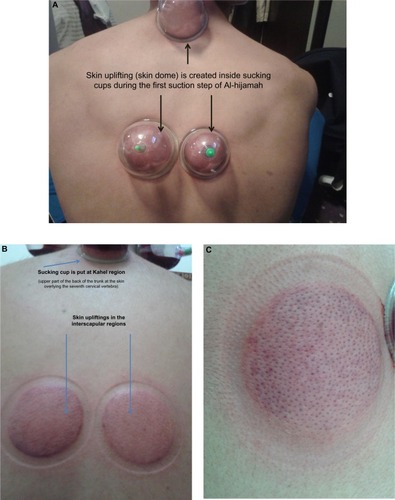
Figure 3 Second step of Al-hijamah (skin scarification, shartat mihjam in Arabic).
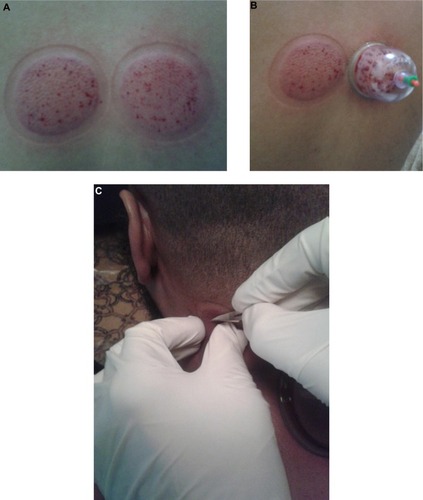
Figure 4 Third step of Al-hijamah (second suction step).
Abbreviation: RBC, red blood cell.
Each suction step during WCT is a pressure-dependent filtration step; ie, Al-hijamah has two filtration steps versus one filtration step for traditional WCT, which allows also a longer duration of pressure-dependent filtration during Al-hijamah than during traditional WCT.Citation1,Citation18 Based on this, Al-hijamah was reported to provide better filtration, better excretory functions, and less blood loss than traditional WCT.Citation18
Traditional WCT is a partial form of Al-hijamah; ie, all diseases treated by traditional WCT can be treated by Al-hijamah.Citation1,Citation11 Indications for practicing Al-hijamah were previously reported.Citation11 Al-hijamah is indicated whenever an excess noxious substance or fluid is to be removed from plasma and interstitial fluids. Those excess harmful substances may be causative substances for the disease process or pathogenesis; eg, excess uric acid in gout (causing gouty arthritis) and excess iron in thalassemia and iron overload conditions. Both can be referred to as disease-causing substances. When the excess noxious substances are formed during disease pathogenesis; eg, oxidized LDL in thalassemia patients (induced by excess iron), which can be referred to as disease-related substances. Both disease-causing substances and disease-related substances can be referred to as causative pathological substances. Al-hijamah is indicated when the serum level of any causative pathological substances increases in blood or interstitial fluids enough to require clearance.Citation11 Moreover, other therapeutic benefits of Al-hijamahCitation11 may help in treating different disease conditions, such as musculoskeletal pain conditions and neuropsychiatric conditions.Citation11
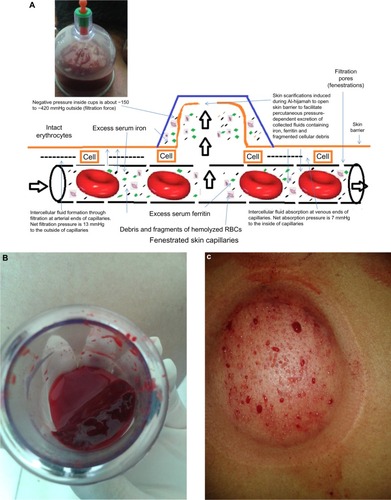
Skin scarification during Al-hijamah (shartat mihjam in Arabic) () is a vital step, as it opens the skin barrier and transmits the suction pressure to the fenestrated dermal skin capillaries to favor the excretion of local intercellular fluids and capillary filtration, causing excretion of small-sized particlesCitation1,Citation18 (serum iron, serum ferritin, liberated hemoglobin and fragments of hemolyzed cells excluding intact blood cells) from skin capillary blood (). Shartat mihjam refers to the superficial skin scarifications (0.1 mm–0.2 mm in depth) that open the skin barrier to transmit the suction pressure around skin dermal capillaries to facilitate the suction-induced, pressure-dependent filtration process of blood circulating in the fenestrated skin capillaries during Al-hijamah. The superficial nature of skin scarifications ensures that no damage will occur to the fenestrated skin capillaries, which ensures preservation of the pressure-dependent filtration function. To ensure the superficial nature of the skin scarifications, skin incisions done during shartat mihjam should be short (1–2 mm) in length, vertical, in parallel rows, multiple, evenly distributed, confined to the skin uplifting (skin dome), and preceded and followed by a suction step. All that may guarantee the superficial nature of skin scarification and the best conditions for transmitting the negative suction pressure to the fenestrated dermal skin capillaries. Skin scarifications done during traditional WCT cannot be described as shartat mihjam, as those scarifications are not preceded by a suction step.Citation11 Filtered fluids (plasma-like fluids) may come out through shartat mihjam with repeated suctions using sucking cups (). Al-hijamah has been reported to exert a percutaneous nonspecific clearance of blood and interstitial spaces.Citation1,Citation2,Citation11,Citation18 Increasing the number of Al-hijamah sessions or sucking cups at many anatomical sites may increase blood clearance.
Al-hijamah, also called bloodletting cupping therapyCitation3 or blood cupping therapy in Arabic countries,Citation2 is a simple therapeutic modality of WCT that is practiced for treating many diseases. Health professionals practicing Al-hijamah should receive adequate medical education and evaluation. Unfortunately, few research studies have focused on Al-hijamah. Detailed scientific bases of Al-hijamah were reported in the evidence-based Taibah theory (Taibah mechanism).Citation1,Citation18
Al-hijamah is more comprehensive than the worldwide traditional WCT.Citation1,Citation18 Detailed differences between Al-hijamah and traditional WCT were previously reported.Citation11,Citation18 In traditional WCT, skin scarifications are done on the surface of the intact skin (not uplifted skin), which may produce pain during the procedure (due to lack of the hypothetic or anaesthetic effect gained during the first suction step). Moreover, lack of the first suction step in traditional WCT (present in Al-hijamah) prevents the formation of a fluid barrier that creates a mechanical barrier between the superficial skin layers and the dermal capillaries. That fluid barrier created during the first step of Al-hijamah separates the fenestrated dermal capillaries from the skin surface () and protects the dermal capillaries from damage or injury during the superficial skin scarifications. Based on this, the possibility of injuring the fenestrated dermal capillaries using superficial scarifications during traditional WCT is greater than the possibility of injuring dermal capillaries with superficial scarifications during Al-hijamah. It is important to decide which type of WCT (Al-hijamah or traditional WCT) was done when writing or reading research articles about WCT. Some authors may write WCT when Al-hijamah is meant in the methodology section,Citation27 which may confuse the reader.
Proper practice, precautions, contraindications, and side effects of Al-hijamah
Al-hijamah is a safe therapeutic procedure when practiced properly by a qualified, well-trained, and licensed practitioner. It is rare to face side effects when the criteria for proper practice of Al-hijamah are fulfilled. Strict sterilization is a must in the beginning, throughout the whole procedure, and at the end of Al-hijamah. The most important precaution is to take care regarding selecting the best anatomical sites for cup application.Citation28 It is essential to practice Al-hijamah in specialized clinics in hospitals. In addition, moderate suction pressure inside cups (less than −300 mmHg) for 5 minutes is the best. It is better if Al-hijamah is not practiced near the course of superficial veins or nerves to guard against injury to those structures. It is not advisable to practice Al-hijamah in patients with high-risk pregnancy, recent burns (inflamed tissues), or attacks of severe bleeding. Circulatory shock, uncontrolled bleeding disorders, uncontrolled coagulation disturbances, conditions of severe anemia, and conditions of active bleeding are relative contraindications for performing Al-hijamah. Once the abovementioned conditions are corrected and the patient’s condition improves, Al-hijamah can be practiced when there is a strong therapeutic indication, taking into account the risk/benefit ratio. When Al-hijamah is highly indicated at some special anatomical sites (near the course of superficial veins or nerves), risk/benefit ratio should be applied and Al-hijamah should be done using Salah’s techniqueCitation28 () for safe practice of Al-hijamah where a skin fold of the skin uplifting is pinched out between the thumb and index fingers of the left hand to make sure that it is away from the underlying anatomical structures while the right hand makes superficial scarifications in the pinched-out skin fold. The suction step should be manual using a handheld pumpCitation11 and should not be done using cotton or alcohol ignition to avoid skin burns or fire accidents. Suction time should be about 5 minutes, and suction pressure should be moderate (three to four maximal suction times using the handheld pump).
Shartat mihjam ( and ) is an Arabic term that means superficial skin scarifications (0.1 mm in depth to preserve the structure of the superficial fenestrated dermal capillaries) that are confined to the skin dome (skin uplifting created after the first suction step). Skin scarifications of Al-hijamah denote the hand skills that differentiate one skillful practitioner from another. Skin scarifications should be multiple, longitudinal (1–2 mm in length; ie, not pinpoint pricks), in parallel rows, equally distributed, and productive. Malpractice of Al-hijamah is caused by any violation of those criteria and may carry side effects. Practitioner skill is required to do shartat mihjam properly for better blood clearance benefits that can be evaluated and quantitated using the previously mentioned indices of Al-hijamah. Frequency of performing Al-hijamah varies according to disease condition and response to treatment. It can be done every other week, monthly, twice per year, or yearly. Every case should be individualized according to the patient’s condition and follow-up in light of current treatment.
There are no absolute contraindications for practicing Al-hijamah. Proper practice of Al-hijamah necessitates the presence of an experienced practitioner to perform Al-hijamah and an eligible patient having a disease condition that will benefit from treatment using Al-hijamah. Al-hijamah can be done for both preventive and therapeutic health purposes.Citation11,Citation28 Al-hijamah should be done in a sterile, well-equipped environment (hospital or specialized clinic) using the triple S steps (suction, scarification, and suction) of Al-hijamah. In the vast majority of cases, Al-hijamah is done by applying sucking cups on points on the back of the trunk.Citation28 This carries the advantages of a simpler technique (the flat surface of the back is easier for large cup application for better blood clearance) and cosmetic benefit (the back is a hidden area covered by clothes).
The most important points of malpractice causing possible side effects include deep skin scarifications (>0.5 mm in depth) causing damage of the superficial fenestrated capillaries (causing disturbed Al-hijamah-induced filtration function), long skin incisions causing bleeding, large skin incisions causing postcupping scars, strong suction pressure (≥300 mmHg) may cause skin ecchymosis and Taibah sign,Citation11 suction using cotton ignition may burn the skin, prolonged suction time causing skin ecchymosis, and pinpoint pricks causing inefficient clearance function. However, after the acute condition improves, re-evaluation of the patient’s general condition is needed before practicing Al-hijamah where the risk/benefit ratio should be applied. In the literature, side effects of cupping therapy were mainly related to malpractice of traditional DCT and traditional WCT, but not Al-hijamah. As the methodology is similar in all three, reported side effects should be considered and should be divided into common and rare side effects.
Common side effects include skin bruises, Taibah signCitation11 (due to excessive suction pressure or prolonged suction duration causing dermal capillary rupture), bleeding (due to deep or long skin scarification), keloid scarring, and burns (when using cotton or alcohol ignition). Rare serious side effects may include acquired hemophilia A,Citation29 hemorrhagic stroke,Citation30 factitious panniculitis,Citation31 reversible cardiac hypertrophy, and iron deficiency anemia (due to too frequent sessions of traditional WCT with extensive bleeding caused by an unqualified practitioner).Citation32,Citation33
Pathophysiology of iron overload and hyperferremia
Iron overload is a major health problem in thalassemia, hemochromatosis, sickle cell anemia, sideroblastic anemia, and others that may cause tissue damage (involving the heart, liver, skin, pancreas, and endocrine glands, among others) and serious complications in children and adults. Mean iron level in the skin of thalassemia patients increased by more than 200%.Citation13 Treatment of iron overload using iron chelation therapy is vital. Long-term treatment using deferoxamine, deferiprone, and deferasirox (at full doses) may carry intolerable side effects (eg, decreased immunity due to neutropenia, agranulocytosis, renal disturbances, and gastrointestinal disturbances) requiring drug discontinuation in 30% of patients.Citation34 Unfortunately, iron overload persists as a cause of morbidity even after curing thalassemia with bone marrow transplantation.Citation35 The blood clearance percentage of iron and ferritin is a good parameter for treating iron overload, taking into account other health and economic burdens of treatment.
Mechanisms of hemolysis in thalassemia
Mechanisms of hemolysis in thalassemia (an example of iron overload) need careful understanding, medical education, and evaluation, being the source of iron (from liberated hemoglobin of hemolyzed cells) in addition to the increased intestinal absorption of iron. Hemolysis in thalassemia is multifactorial in origin; eg, due to precipitation of globin chains in the erythrocytes, erythrocyte membrane skeletal protein defects,Citation36 presence of natural antigalactosyl IgG antibodies on thalassemic erythrocytes,Citation37 alloimmunization (or erythrocyte autoimmunization due to autoantibodies) in transfusion-dependent thalassemic patients,Citation37 sensitivity of thalassemic erythrocytes to oxidative stress (due to increased oxidants as malondialdehyde and decreased antioxidants as polyunsaturated fatty acids),Citation36 and excessive oxidation of the unstable globin chains with subsequent release of oxygen-free radicals.Citation36 Red blood cell destruction by human monocytes may be related to changes in the intracellular iron and ferritin concentrations and phenotype.Citation38
Complications of excessive frequent blood transfusions and excessive hemolysis may aggravate the iron overload condition and may cause blood-borne infections such as viral hepatitis (C or B). Unfortunately, iron chelation therapy does not treat the abovementioned causes of hemolysis.
Iron is high in the interstitial fluids and in the serum of iron overload patients. This may be explained by the fact that interstitial fluid is formed by filtration of capillary blood at the arterial ends of capillaries and is absorbed later at the venous ends of capillaries.Citation1,Citation18 Moreover, the pathophysiology of pulmonary hypertension in beta-thalassemia may be mediated through iron overload, reduced bioavailability of nitric oxide, hemolysis, and hypercoagulopathy.Citation39 As skin iron deposition is high in iron overload, treatment modalities using percutaneous iron excretion may be promising.
Oxidative and pathological roles exerted by excess serum iron and ferritin
Iron is a major oxidant in vivo.Citation40 Iron-induced generation of reactive oxygen species is responsible for the damaging effects induced by iron released by isoferritins (containing iron) on lymphocyte functions.Citation41 Iron overload causes oxidative stress, depletion of endogenous antioxidants, and lipid peroxidative damage.Citation42 Iron may induce the formation of the major atherogenic factor (oxidized LDL), causing atherosclerosis (). Serum cholesterol was reported to increase iron deposits that could be identified in the arterial walls in conditions of experimental hypercholesterolemia and in iron-overloaded hypercholesterolemia. Lipoperoxides in liver and spleen homogenates were high in conditions of iron overload.Citation40
Table 1 Reported pathological roles of ferritin in iron overload conditions; eg, thalassemia
Moreover, young thalassemic patients showed an atherogenic lipid profile where serum triglycerides, total cholesterol, apolipoprotein A, and carotid intima-media thickness (CIMT) were significantly elevated. Serum high-density lipoprotein (HDL) was significantly lowered. In thalassemic patients, CIMT was positively correlated with age, hemoglobin F (Hb F), ferritin, and cholesterol levels.Citation40,Citation43 Interestingly, both serum iron and triglycerides may be involved in the pathogenesis of LDL oxidation, as evidenced by the report that high levels of oxidized LDL antibodies promoted atherosclerosis in patients with beta-thalassemia.Citation44 That was confirmed by another report in which iron was a potent catalyst of oxidative reactions and macrophage-mediated LDL oxidation in atherogenesis.Citation45 In addition, released heme may have injurious effects that result from its potent catalysis of LDL oxidation.Citation46 Moreover, circulating iron stores (serum ferritin) were reported to be associated with vascular damage in patients with nonalcoholic fatty liver disease.Citation47
Iron overload suppresses patients’ immunity
Iron overload is usually associated with hyperferremia in conditions of beta-thalassemia major, dyserythropoiesis, hereditary hemochromatosis, and chronic diffuse liver diseases; eg, cirrhosis and chronic hepatitis. This may cause the formation of antiferritin antibodies and circulating immune complexes. Increased body stores of iron may affect the immunoregulatory balance, resulting in increased growth rates of cancer cells, infectious organisms, and opportunistic pathogens. Iron overload may complicate the clinical management of pre-existing acute and chronic diseases.Citation48 Iron and ferritin impaired a variety of immunological functions. Ferritin-associated iron induced neutrophil dysfunction in hemosiderosis.Citation49 Iron overload, especially with hyperferremia, may exert an immune-suppressing effect through altering the distribution of T lymphocytes in various compartments of the immune system,Citation50 suppressing the immunological functions of the complement system (classic and alternative pathways), decreasing the T helper (CD4) proliferative capability, decreasing T helper numbers, decreasing T helper activity, increasing the CD8/CD4 ratios, impairing the generation of cytotoxic T cells, enhancing the suppressor T cell numbers and activity, suppressing the antibody-mediated and mitogen-stimulated phagocytosis (by monocytes and macrophages), inducing alterations in the T lymphocyte subsets, inducing modification of lymphocyte distribution in different immunological locations, and altering immunoglobulin secretion.Citation48–Citation54
There is a reported progressive dysfunction of monocytes associated with iron overload in patients with thalassemia major.Citation51 Moreover, there is an impaired neutrophil defense against Yersinia enterocolitica in patients with iron overload who are undergoing dialysis.Citation52–Citation54
Negative correlations between T helper/T cytotoxic ratio and malondialdehyde levels were obtained in the blood and spleen tissues during experimental iron overload, indicating that lipid peroxidation may play a role in the immunological abnormalities observed in experimental hemosiderosis.Citation53 Secondary hemosiderosis may be accompanied by a decrease in the phagocytic functions of neutrophils, as evidenced by the report that neutrophils from patients with secondary hemosiderosis contain excessive amounts of autotoxic iron and have increased cellular iron and ferritin content.Citation49 Iron concentrations were four to five times more elevated in secondary hemosiderosis than in healthy subjects. This iron accumulation may be toxic for neutrophils and may explain the three-fold higher risk of bacteremia reported in those patients.Citation51–Citation54
Infections with virulent pathogens are commonly encountered in patients having iron overload; eg, Listeria monocytogenes meningitis.Citation55 Although iron-binding proteins such as transferrin and lactoferrin are bacteriostatic in vitro,Citation56–Citation58 iron overload may disturb the bacteriostatic functions of these proteins and decrease their antimicrobial activity, resulting in increased incidence of infections.Citation56,Citation59–Citation61 Subclinical atherosclerosis in children with major beta-thalassemia begins early in life and these children are at risk of developing premature atherosclerosis.Citation62
Phlebotomy versus Al-hijamah for treating iron overload
After successful marrow transplantation, iron overload is still an important cause of morbidity in thalassemia. Phlebotomy is a safe, efficient, and widely accepted method where mobilization of iron from overloaded tissues occurs, causing a decrease in iron overload in ex-thalassemic patients. Phlebotomy was reported to decrease serum ferritin and liver iron concentration maximally and significantly. It also improved the histological grading for chronic hepatitis in ex-thalassemic patients.Citation63 Phlebotomy (versus iron chelation therapy) is still practiced as the therapeutic procedure aiming at getting rid of a portion of blood to excrete an abnormally increased offending blood component. Phlebotomy is the initial treatment of choice in hemochromatosis, while iron chelation therapy is the treatment of choice for transfusional siderosis encountered in thalassemia.Citation64 A phlebotomy program was reported to be beneficial for two-thirds of patients who underwent allogeneic hematopoietic stem cell transplantation for treating thalassemia.Citation65 Thalassemia patients (who received bone marrow transplant) with subclinical left ventricular diastolic dysfunction and impaired left ventricular contractility may reverse these processes with an effective regimen of iron reduction using phlebotomy.Citation66 Interestingly, cure of thalassemia in some hepatic cirrhosis patients with allogeneic bone marrow transplantation resulted in reversibility of liver cirrhosis after iron removal treatment where serum aminotransferase levels decreased, histologic inflammatory activity decreased, and histological biopsies showed regression of incomplete or definite cirrhosis.Citation67 Phlebotomy may treat iron overload but it may cause significant blood loss, causing aggravation of the anemic status in patients having thalassemia or sickle cell anemia. Blood shed out during phlebotomy may benefit patients by decreasing the level of serum ferritin, iron, antibodies, and hemolyzed cells, but the necessity for a second blood transfusion consequently increases. Elevated erythrocyte ferritin during phlebotomy therapy in iron overload depends on the body iron stores that can be regulated by the activity of erythropoiesis.Citation68
However, phlebotomy was not reported to treat the above-mentioned causes of hemolysis in thalassemic patients. As for Al-hijamah, it may treat some causes of hemolysis; eg, through excretion of immunoglobulin antibodies and noxious substances. Al-hijamah-induced percutaneous excretion of iron and ferritinCitation2 may improve the therapeutic outcomes in iron overload patients (). Al-hijamah may induce pharmacological potentiationCitation3 (decreasing the needed dose and frequency of iron chelation drug administration and causing decreased drug-induced side effects). Al-hijamah may enhance the natural immunityCitation3 and enhance the removal of cellular fragments of hemolyzed cells. Reported WCT-induced blood clearance of antibodiesCitation3 may treat some causes of hemolysis and benefit iron overload patients. Al-hijamah may decrease the needed frequency (and amount) of blood transfusions. Al-hijamah-induced reduction in blood pressure and blood clearance of triglycerides, LDL cholesterol, and total cholesterolCitation2 may prevent and treat disease conditions associated with thalassemia, such as premature atherosclerosis, and improve the general status in hepatitis patients.
Table 2 Al-hijamah versus phlebotomy for treating iron overload
Interestingly, Al-hijamah efficiently treated other diseases, including rheumatoid arthritis,Citation3 headache,Citation26 hypertension,Citation1 and bronchial asthmaCitation5 ( and ). Reported therapeutic benefits of production of endogenous nitric oxide (antioxidant, antimicrobial, and vasodilator)Citation1,Citation6 may benefit thalassemia patients. Serum iron, serum ferritin, necessity, and frequency of repeated blood transfusions should be compared before and after Al-hijamah. Al-hijamah was reported to improve the oxygen saturation and respiratory functions better than phlebotomy in cigarette-smoking patients having chronic obstructive pulmonary disease.Citation27
Table 3 Al-hijamah versus iron chelation therapy for treating iron overload
Table 4 Safety issue of iron chelation therapy versus Al-hijamah
Interestingly, Al-hijamah did not induce anemia or significant blood loss, as evidenced by the normal hematological indices after practicing Al-hijamah.Citation27 Al-hijamah (suction, scarification, and suction method) was reported to significantly decrease the level of serum C-reactive protein better than phlebotomy in patients having urticaria and angioedema;Citation69 Al-hijamah decreased serum CRP from 11.95 to 1.1 mg/L, while phlebotomy decreased it to a much lower extent.Citation69
Reported therapeutic benefits of Al-hijamah during treatment of iron overload
There are a lot of reported hematological health benefits that can be gained when treating patients having different diseases with Al-hijamah. However, the most attractive reported side effect of repeated traditional WCT is iron deficiency anemia, which can be utilized for treating iron overload conditions. Practicing Al-hijamah was not reported to cause massive blood loss or anemia. Instead, Al-hijamah was reported to reduce serum ferritin significantly.Citation1 Although there are no published reported studies about the use of Al-hijamah for treating thalassemia or conditions of iron overload, the safety of practicing Al-hijamah and the reported health benefits associated with itCitation11 may be an attractive topic for hematologists and researchers to explore. The therapeutic benefits of Al-hijamah for treating different disease conditions have been previously reported.Citation11 Many of those health and therapeutic benefits are helpful when treating patients having iron overload with hemolysis; for example, thalassemia. Al-hijamah-induced immunological enhancement (eg, physiological leukocytosis and increased count of NK cellsCitation3,Citation11) is beneficial for improving the poor immunity status in thalassemia patients. Blood and interstitial fluid clearance from excess ferritin and iron is the single most important therapeutic benefit of Al-hijamah when treating thalassemia patients. Being a percutaneous excretory procedure, skin (a site for iron deposition) clearance of excessive iron can be gained through Al-hijamah. Moreover, nonspecific blood clearance gained during Al-hijamah, where patients’ serum can be cleared significantly of LDL cholesterol, total cholesterol, and triglycerides,Citation1 may protect thalassemia patients against the development of premature atherosclerosis. Pharmacological potentiation reported when combining Al-hijamah with different drug treatments may enhance the therapeutic effects and decrease the side effects of concomitantly administered drugs by iron overload patients, such as iron chelation therapy. Importantly, Al-hijamah was not reported to cause massive bleeding (red blood cell loss)Citation26,Citation27 or aggravate anemic status. Al-hijamah induces possible nonspecific blood clearance of liberated hemoglobin and fragments of hemolyzed cells (having small particle sizes that can be filtered through capillary pores).
Al-hijamah combined with oral honey for treating hyperferremia and its complications
Consumption of oral honey was reported to provide numerous beneficial effects that may expand the therapeutic effects of Al-hijamah when combined with Al-hijamah. Oral honey may benefit thalassemia and iron overload patients, especially thalassemia cases complicated with diabetes mellitus, poor immunity, and oxidative stress-induced effects; oral honey improved body weight and serum lipid profile of diabetic patientsCitation70 to the extent that it was recommended to be used as a sugar substitute in patients with type 1 diabetes mellitusCitation71 or impaired glucose tolerance.Citation72 Patients having impaired glucose tolerance exhibited significant lower plasma glucose concentrations after consumption of oral honey where the plasma glucose levels peaked at 30–60 minutes in response to oral honey and showed a rapid decline as compared to patients consuming glucose, which indicated a better control of the glycemic index with oral honey administration.Citation72 Oral honey consumption was reported to increase serum antioxidant capacity, vitamin C concentration, beta-carotene, and glutathione reductase. Interestingly, honey reduced plasma ferritin by 11%.Citation73 Moreover, oral honey was reported to enhance the natural immunological response through increasing the monocytes and lymphocytes percentage, decreasing serum immunoglobulin ECitation73 and stimulating antibody production during primary and secondary immune responses against thymus-dependent and thymus-independent antigens.Citation74
Interestingly, oral honey ingestion was reported to decrease prostaglandins levels, elevate nitric oxide production, and improve the hematological and biochemical tests in a patient with a long history of AIDS.Citation75 It might be concluded that combining Al-hijamah with oral honey may improve the therapeutic outcomes in thalassemia and iron overload patients. Interestingly, in prophetic medicine, both Al-hijamah and oral honey are curative remedies according to the prophetic teaching: “Cure is in three: in sharat mihjam, gulp of honey (oral honey), and cauterization. I do not recommend my nation to cauterize.”Citation76,Citation77
Conclusion
In conclusion, Al-hijamah is a beneficial, safe, economic, time-saving (about 30 minutes), and repeatable treatment modality. Al-hijamah may be a good combinatory treatment with iron chelation therapy, and can be a sole treatment when there is a limitation or contraindication to iron chelation therapy. Al-hijamah may be superior to phlebotomy, and it needs to be researched further for educational evaluation in treating iron overload. Oral honey also carries a lot of therapeutic health benefits when treating conditions of iron overload. This may strongly suggest Al-hijamah combined with oral honey as a novel treatment for thalassemia and iron overload conditions may potentiate therapeutic effects of iron chelation therapy.
Acknowledgments
We are so grateful to the helpful revision and grammatical corrections exerted by Professor Antar Abdellah, Associate Professor of English Language and Linguistics in the Faculty of Education at Taibah University, Al-Madinah Al-Munawwarah, Saudi Arabia.
Supplementary Video 1
Disclosure
The authors declare no conflict of interest in this work.
References
- El SayedSMMahmoudHSNaboMMHMedical and scientific bases of wet cupping therapy (Al-hijamah): in light of modern medicine and prophetic medicineAltern Integ Med201323116
- AlshowafiFKEffect of blood cupping on some biochemical parameterMed J Cairo Univ201078311315
- AhmedSMMadboulyNHMakladSSAbu-ShadyEAImmunomodulatory effects of blood letting cupping therapy in patients with rheumatoid arthritisEgypt J Immunol2005122395117977209
- YunGWYangYJSongICA prospective evaluation of adult men with iron-deficiency anemia in KoreaIntern Med201150131371137521720055
- ZhangCQLiangTJZhangWEffects of drug cupping therapy on immune function in chronic asthmatic bronchitis patients during protracted periodZhongguo Zhong Xi Yi Jie He Za Zhi20062611984987 Chinese17186726
- Cals-GriersonMMOrmerodADNitric oxide function in the skinNitric Oxide200410417919315275864
- BoisselJPOhlyDBrosMGödtel-ArmbrustUFörstermannUFrankSThe neuronal nitric oxide synthase is upregulated in mouse skin repair and in response to epidermal growth factor in human HaCaT keratinocytesJ Invest Dermatol2004123113213915191553
- RendellMSJohnsonMLSmithDSkin blood flow response in the rat model of wound healing: expression of vasoactive factorsJ Surg Res20021071182612384060
- LeeRHEfronDTantryUBarbulANitric oxide in the healing wound: a time-course studyJ Surg Res2001101110410811676563
- WinkDAMirandaKMEspeyMGMechanisms of the antioxidant effects of nitric oxideAntioxid Redox Signal2001320321311396476
- El SayedSMAl-qulitiAMahmoudHSTherapeutic benefits of Al-hijamah: in light of modern medicine and prophetic medicineAJMBR224671
- KanitakisJAnatomy, histology and immunohistochemistry of normal human skinEur J Dermatol20021239039912095893
- El SayedSMAbou-TalebAMahmoudHSPercutaneous excretion of iron and ferritin (through Al-hijamah) as a novel treatment for iron overload in beta-thalassemia major, hemochromatosis and sideroblastic anemiaMed Hypotheses201483223824624857772
- SaladinKSThe circulatory system: blood vessels and circulationAnatomy and Physiology: The Unity of Form and Function3rd edNew YorkMcGraw-Hill2003756781
- BouwstraJAHoneywell-NguyenPLGoorisGSPonecMStructure of the skin barrier and its modulation by vesicular formulationsProg Lipid Res200342113612467638
- YoungBHeathJWSkinWheater’s Functional Histology: A Text and Colour Atlas4th edLondonChurchill Livingstone2000164
- HuberREmerichMBraeunigMCupping – is it reproducible? Experiments about factors determining the vacuumComplement Ther Med2011192788321549258
- El SayedSMMahmoudHSNaboMMHMethods of Wet Cupping Therapy (Al-hijamah): In Light of Modern Medicine and Prophetic MedicineAltern Integ Med20132116
- MichalsenABockSLüdtkeREffects of traditional cupping therapy in patients with carpal tunnel syndrome: a randomized controlled trialJ Pain200910660160819380259
- KimJIKimTHLeeMSEvaluation of wet-cupping therapy for persistent non-specific low back pain: a randomised, waiting-list controlled, open-label, parallel-group pilot trialTrials20111214621663617
- XuJLinRWangJEffect of acupuncture anesthesia on acne vulgaris of pricking-bloodletting cupping: a single-blind randomized clinical trailJ Tradit Chin Med201333675275624660606
- ZhangSJLiuJPHeKQTreatment of acute gouty arthritis by blood-letting cupping plus herbal medicineJ Tradit Chin Med2010301182020397456
- ErqingDHaiyingLZhankaoZOne hundred and eighty-nine cases of acute articular soft tissue injury treated by blood-letting puncture with plum-blossom needle and cuppingJ Tradit Chin Med200525210410516136937
- PanHThirty-two cases of acne treated with blood-letting puncture, cupping and Chinese-drug facemaskJ Tradit Chin Med200525427027216447668
- HuangYLCupping-bloodletting therapy of Saudi Arabia and its clinical applicationZhongguo Zhen Jiu2008285375377 Chinese18652333
- AhmadiASchwebelDCRezaeiMThe efficacy of wet-cupping in the treatment of tension and migraine headacheAm J Chin Med2008361374418306448
- HekmatpouHMoeiniLHaji-NadaliSThe effectiveness of wet cupping vs venesection on arterial O2 saturation level of cigarette smokers: A randomized controlled clinical trialPak J Med Sci20132961349135324550951
- MahmoudHSAbou-El-NagaMOmarNAAEl-GhazzawyHAFathyYMNaboMMHAnatomical sites for practicing Wet Cupping Therapy (Al-Hijamah): In Light of Modern Medicine and Prophetic MedicineAltern Integ Med201328130
- WengYMHsiaoCTAcquired hemophilia A associated with therapeutic cuppingAm J Emerg Med2008268970. e1970. e218926376
- BluntSBLeeHPCan traditional “cupping” treatment cause a stroke?Med Hypotheses201074594594920031334
- MoonSHHanHHRhieJWFactitious panniculitis induced by cupping therapyJ Craniofac Surg20112262412241422134296
- KimKHKimTHHwangboMYangGYAnaemia and skin pigmentation after excessive cupping therapy by an unqualified therapist in Korea: a case reportAcupunct Med201230322722822738805
- LeeHJParkNHYunHJKimSJoDYCupping therapy-induced iron deficiency anemia in a healthy manAm J Med20081218e5e618691469
- GradyRWGalanelloRRandolphREKleinertDADessiCGiardinaPJToward optimizing the use of deferasirox: potential benefits of combined use with deferoxamineHaematologica201398112913522875626
- AngelucciEMurettoPLucarelliGPhlebotomy to reduce iron overload in patients cured of thalassemia by bone marrow transplantation. Italian Cooperative Group for Phlebotomy Treatment of Transplanted Thalassemia PatientsBlood19979039949989242528
- ShinarERachmilewitzEALuxSEDiffering erythrocyte membrane skeletal protein defects in alpha and beta thalassemiaJ Clin Invest19898324044102521488
- GaliliUKorkeshAKahaneIRachmilewitzEADemonstration of a natural antigalactosyl IgG antibody on thalassemic red blood cellsBlood1983616125812646839023
- Raha-ChowdhuryRWilliamsBJWorwoodMRed cell destruction by human monocytes – changes in intracellular ferritin concentration and phenotypeEur J Haematol199350126318436211
- AnthiAOrfanosSEArmaganidisAPulmonary hypertension in β thalassaemiaLancet Respir Med20131648849624429247
- AraujoJARomanoELBritoBEIron overload augments the development of atherosclerotic lesions in rabbitsArterioscler Thromb Vasc Biol1995158117211807542998
- CardierJRomanoESoyanoAEffect of hepatic isoferritins from iron overloaded rats on lymphocyte proliferative response: role of ferritin iron contentImmunopharmacol Immunotoxicol19951747197328537608
- GedikGKCağlarMUnalSGümrükFEvaluation of cardiovascular complications with 99mTc tetrofosmin gated myocardial perfusion scintigraphy in patients with thalassemia majorRev Esp Med Nucl208827319119818570861
- TantawyAAAdlyAAEl MaatyMGAminSASubclinical atherosclerosis in young beta-thalassemia major patientsHemoglobin200933646347419958191
- BrizziPIsajaTD’AgataAMalaguarneraLMalaguarneraMMusumeciSOxidized LDL antibodies (OLAB) in patients with beta-thalassemia majorJ Atheroscler Thromb20029313914412226555
- YuanXMBrunkUTIron and LDL-oxidation in atherogenesisAPMIS199810698258429808409
- JacobHSNewly recognized causes of atherosclerosis: the role of microorganisms and of vascular iron overloadJ Lab Clin Med199412368088168201257
- ValentiLSwinkelsDWBurdickLSerum ferritin levels are associated with vascular damage in patients with nonalcoholic fatty liver diseaseNutr Metab Cardiovasc Dis201121856857520392616
- WalkerEMJrWalkerSMEffects of iron overload on the immune systemAnn Clin Lab Sci200030435436511045759
- CantinieauxBBoelaertJRDe MeuleneireJKerrelsVFonduPNeutrophils from patients with secondary haemosiderosis contain excessive amounts of autotoxic ironEur J Haematol19935131611658405331
- CardierJERomanoESoyanoAT lymphocytes subsets in experimental iron overloadImmunopharmacol Immunotoxicol199719175879049660
- BallartIJEstevezMESenLProgressive dysfunction of monocytes associated with iron overload and age in patients with thalassemia majorBlood19866711051093940540
- CantinieauxBJanssensABoelaertJRFerritin-associated iron induces neutrophil dysfunction in hemosiderosisJ Lab Clin Med1999133435336110218766
- CardierJERomanoESoyanoALipid peroxidation and changes in T lymphocyte subsets and lymphocyte proliferative response in experimental iron overloadImmunopharmacol Immunotoxicol19951747057178537607
- CantinieauxBBoelaertJHarigaCFonduPImpaired neutrophil defense against Yersinia enterocolitica in patients with iron overload who are undergoing dialysisJ Lab Clin Med198811155245283361231
- van AsbeckBSVerbrughHAvan OostBAMarxJJImhofHWVerhoefJListeria monocytogenes meningitis and decreased phagocytosis associated with iron overloadBr Med J (Clin Res Ed)19822846315542544
- BullenJJSpaldingPBWardCGGutteridgeJMHemochromatosis, iron and septicemia caused by Vibrio vulnificusArch Intern Med19911518160616091872665
- ReiterBBrockJHSteelEDInhibition of Escherichia coli by bovine colostrum and post-colostral milk. II. The bacteriostatic effect of lactoferrin on a serum susceptible and serum resistant strain of E. coliImmunology197528183951090522
- LawrenceTHBiggersCJSimontonPRBacteriostatic inhibition of Klebsiella pneumoniae by three human transferrinsAnn Hum Biol197743281284332055
- AbbottMGallowayACunninghamJLHaemochromatosis presenting with a double Yersinia infectionJ Infect19861321431453531350
- CapronJPCapron-ChivracDTossouHDelamarreJEbFSpontaneous Yersinia enterocolitica peritonitis in idiopathic hemochromatosisGastroenterology1984876137213756489703
- BrennanROCrainBJProctorAMDurackDTCunninghamella: a newly recognized cause of rhinocerebral mucormycosisAm J Clin Pathol1983801981026858971
- GurselOKurekciAETascilarEPremature atherosclerosis in children with β-thalassemia majorJ Pediatr Hematol Oncol201234863063423108004
- AngelucciEMurettoPLucarelliGTreatment of iron overload in the “ex-thalassemic”. Report from the phlebotomy programAnn N Y Acad Sci19988502882939668550
- FlatenTPAasethJAndersenOKontoghiorghesGJIron mobilization using chelation and phlebotomyJ Trace Elem Med Biol2012262–312713022565013
- BuscaAFaldaMManziniPIron overload in patients receiving allogeneic hematopoietic stem cell transplantation: quantification of iron burden by a superconducting quantum interference device (SQUID) and therapeutic effectiveness of phlebotomyBiol Blood Marrow Transplant201016111512219766730
- MariottiEAngelucciEAgostiniABaroncianiDSgarbiELucarelliGEvaluation of cardiac status in iron-loaded thalassaemia patients following bone marrow transplantation: improvement in cardiac function during reduction in body iron burdenBr J Haematol199810349169219886301
- MurettoPAngelucciELucarelliGReversibility of cirrhosis in patients cured of thalassemia by bone marrow transplantationAnn Intern Med2002136966767211992302
- BodemannHHTanzi-FettaRFSchröter-UrbanHVolkBAKeulJLöhrGWFerritin in erythrocytes and plasma of patients with iron overloadBlut198551125313848335
- SharifiSMAfrasiabianHEvaluation of wet cupping treatment in patients with chronic urticaria and angioedemaOpen Conf Proc J2013315
- BahramiMAtaie-JafariAHosseiniSForuzanfarMHRahmaniMPajouhiMEffects of natural honey consumption in diabetic patients: an 8-week randomized clinical trialInt J Food Sci Nutr200960761862619817641
- AbdulrhmanMEl-HefnawyMHusseinREl-GoudAAThe glycemic and peak incremental indices of honey, sucrose and glucose in patients with type 1 diabetes mellitus: effects on C-peptide level-a pilot studyActa Diabetol2011482899419941014
- AgrawalOPPachauriAYadavHSubjects with impaired glucose tolerance exhibit a high degree of tolerance to honeyJ Med Food200710347347817887941
- Al-WailiNSEffects of daily consumption of honey solution on hematological indices and blood levels of minerals and enzymes in normal individualsJ Med Food20036213514012935325
- Al-WailiNSHaqAEffect of honey on antibody production against thymus-dependent and thymus-independent antigens in primary and secondary immune responsesJ Med Food20047449149415671696
- Al-WailiNSAl-WailiTNAl-WailiANSaloomKSInfluence of natural honey on biochemical and hematological variables in AIDS: a case studyScientificWorldJournal200661985198917369997
- LoukasMSaadYTubbsRSShojaMMThe heart and cardiovascular system in the Qur’an and HadeethInt J Cardiol20101401192319709769
- Al-BukhariMIThe English Translation of Sahih Al Bukhari. Book of medicine. Chapter of (Cure is in three). Hadeeth numbers 5680–5681Assryia librarySayda, Lebanon2002
- CazzolaMBorgna-PignattiCde StefanoPInternal distribution of excess iron and sources of serum ferritin in patients with thalassemiaScand J Haematol19833042892966857145
- Di MarcoVCapraMGagliardottoFLiver disease in chelated transfusion-dependent thalassemics: the role of iron overload and chronic hepatitis CHaematologica20089381243124618556410
- TriadouPRegnat-LusinchiAGirotRUse of the ferritin/alanine aspartate transaminase ratio as an iron overload marker independent of liver cell damageEur J Haematol19894354234272612615
- WonkeBHoffbrandAVBrownDDusheikoGAntibody to hepatitis C virus in multiply transfused patients with thalassaemia majorJ Clin Pathol19904386386402119395
- LaiMEOrigaRDanjouFNatural history of hepatitis C in thalassemia major: a long-term prospective studyEur J Haematol201390650150723414443
- AlavianSMMiriSMTabatabaeiSVLipid Profiles and Hepatitis C Viral Markers in HCV-Infected Thalassemic PatientsGut Liver20115334835521927665
- OmarNSalamaKAdolfSEl-SaeedGSAbdel GhaffarNEzzatNMajor risk of blood transfusion in hemolytic anemia patientsBlood Coagul Fibrinolysis201122428028421508832
- AmeliMBesharatiSNematiKZamaniFRelationship between elevated liver enzyme with iron overload and viral hepatitis in thalassemia major patients in Northern IranSaudi Med J200829111611161518998011
- RagabLHelalSZaghloulNClinicovirologic analysis of hepatitis C infection in transfusion-dependent beta-thalassemia major childrenInt J Lab Hematol201032218419019389113
- SartoriMAndornoSLa TerraGEvaluation of iron status in patients with chronic hepatitis CItal J Gastroenterol Hepatol19983043964019789136
- MazzaPGiuaRDe MarcoSIron overload in thalassemia: comparative analysis of magnetic resonance imaging, serum ferritin and iron content of the liverHaematologica19958053984048566878
- AgarwalMBMalkanGHBhaveAAAntibody to hepatitis-C virus in multi-transfused thalassaemics – Indian experienceJ Assoc Physicians India19934141951978270554
- AlavianSMMiriSMKeshvariMDistribution of hepatitis C virus genotype in Iranian multiply transfused patients with thalassemiaTransfusion200949102195219919538541
- HuYWAl-MoslihMIAl AliMTClinical outcome of frequent exposure to Torque Teno virus (TTV) through blood transfusion in thalassemia patients with or without hepatitis C virus (HCV) infectionJ Med Virol200880236537118098140
- ChuWCMetreweliCChikKWLamWWChanYLLiCKEnlargement of hepatoduodenal ligament lymph nodes in beta thalassemia children receiving multiple transfusions: a common observationHaematologica200287888288412161366
- TabatabaeiSVAlavianSMKeshvariMLow dose ribavirin for treatment of hepatitis C virus infected thalassemia major patients; new indications for combination therapyHepat Mon201212637238122879826
- SpiliopoulouIRepantiMKatinakisSKarana-GinopoulouAPapanastasiouDAResponse to interferon alfa-2b therapy in mutitransfused children with beta-thalassemia and chronic hepatitis CEur J Clin Microbiol Infect Dis1999181070971510584897
- TelferPTGarsonJAWhitbyKCombination therapy with interferon alpha and ribavirin for chronic hepatitis C virus infection in thalassaemic patientsBr J Haematol19979848508559326177
- ChoiEYKimECOhHMIron chelator triggers inflammatory signals in human intestinal epithelial cells: involvement of p38 and extracellular signal-regulated kinase signaling pathwaysJ Immunol2004172117069707715153529
- LeeHJLeeJLeeSKLeeSKKimECDifferential regulation of iron chelator-induced IL-8 synthesis via MAP kinase and NF-kappaB in immortalized and malignant oral keratinocytesBMC Cancer2007717617850672
- BrittenhamGMNathanDGOlivieriNFDeferiprone and hepatic fibrosisBlood2003101125089509012788794