
Abstract
Purpose
To evaluate the efficacy and safety of chemoembolization with drug-eluting microspheres (DEM-TACE) combined with intra-arterial infusion of bevacizumab in patients with unresectable hepatocellular carcinoma (uHCC) and to identify possible prognostic factors.
Patients and Methods
Between November 2014 and December 2020, 34 patients underwent DEM-TACE combined with intra-arterial infusion of bevacizumab for Barcelona Clinic Liver Cancer (BCLC) stage B hepatocellular carcinoma (HCC) beyond the Up-to-seven criteria or BCLC stage C HCC. Patients with extrahepatic metastasis or inferior vena cava invasion were excluded. The primary endpoint was overall survival (OS). The secondary endpoints were safety (assessed using Common Terminology Criteria for Adverse Events v5.0), the response rate at 1 month, and the identification of prognostic factors. The median OS was calculated using the Kaplan–Meier method. The response rate was evaluated according to the modified Response Evaluation Criteria in Solid Tumors. Prognostic factors were investigated by univariate and multivariable analysis using the Cox proportional hazards model.
Results
The median OS was 13 months. BCLC stage and presence of portal vein invasion were not significantly associated with OS. There were no grade ≥3 adverse events. The Child–Pugh class did not decline after treatment in 31 of 34 patients. The overall response rate was 14.2% and the disease control rate was 100%. Significant prognostic factors were alcoholic liver disease, Child–Pugh score of ≥8, and microsphere size of 50–100 μm.
Conclusion
DEM-TACE combined with intra-arterial infusion of bevacizumab is safe and effective, and it could be a treatment option for unresectable HCCs.
Introduction
Transcatheter arterial chemoembolization (TACE) was first performed in Japan in 1978 by Yamada et al. Following the first publication of the outcomes of TACE in 1983, this procedure was rapidly adopted worldwide.Citation1 Currently, TACE is mainly indicated for patients with hypervascular hepatocellular carcinoma (HCC) classified as Child–Pugh class A or B, with 1–3 tumors of ≥3 cm in diameter or ≥4 tumors.Citation2 According to the Barcelona Clinic Liver Cancer (BCLC) staging system, TACE is only indicated for Stage B HCC (intermediate stage).Citation3 In fact, this intermediate stage includes patients with a wide variety of tumor factors and liver function, and several subcategories have been proposed.Citation4–7
In recent years, the advent of molecular-targeted drugs and immune checkpoint drugs has led to dramatic changes in the treatment of HCC, especially in the intermediate stage.Citation8,Citation9 Furthermore, the concepts of TACE failure and TACE refractoriness were recently introduced,Citation10,Citation11 and systemic therapy is now recommended as first-line treatment for some cases in the intermediate stage.Citation2,Citation12 This is because, in addition to the effectiveness of novel systemic therapies,Citation8,Citation9 it is important to avoid deterioration of liver function due to repeated TACE.Citation13–16 However, advances in equipment and technology have enabled selective TACE, which can help preserve liver function. Therefore, TACE has a significant role in patients who are refractory to systemic therapy or patients who experience severe adverse events that make it difficult to continue systemic therapy.
Because chemoembolization with drug-eluting microspheres (DEM-TACE) is believed to have milder effects on liver function than conventional TACE (cTACE),Citation17,Citation18 we hypothesized that DEM-TACE could be used to continue treatment while preserving liver function in patients otherwise deemed unsuitable for TACE due to intermediate or advanced HCC. It has been reported that serum vascular endothelial growth factor (VEGF) levels are significantly greater in patients with hepatocellular carcinoma (HCC) than in healthy subjects,Citation19 and that transarterial chemoembolization (TACE) increases VEGF production in the residual surviving cancerous tissue.Citation20 This increase in VEGF is thought to contribute to the recurrence of HCC after TACE.Citation21 Therefore, we hypothesized that intra-arterial infusion of bevacizumab, an anti-VEGF monoclonal antibody, could suppress the increase in VEGF within residual HCC tissue, and enhance the effect of TACE by normalizing the tumor vasculature.Citation22
Therefore, the purpose of this study was to evaluate the efficacy and safety of DEM-TACE combined with intra-arterial infusion of bevacizumab in patients with unresectable HCC, and to identify possible prognostic factors. This is the first report to describe intra-arterial infusion of bevacizumab for uHCC.
Materials and Methods
DEM-TACE combined with intra-arterial infusion of bevacizumab was approved by the institutional review board of the Institute of Image Guided Therapy (protocol code no. 001) based on the ethical principles of the Declaration of Helsinki. All patients provided written informed consent to undergo the procedures described. This study was performed retrospectively, and all of the data were included in the patients’ medical records. Informed consent was obtained in the form of an opt-out option on the institution’s website, and the need for written informed consent was waived. This study was approved by the institutional review board of the Institute of Image Guided Therapy (protocol code no. 14).
Patients
Between November 2014 and December 2020, 45 consecutive patients underwent DEM-TACE combined with intra-arterial infusion of bevacizumab for BCLC stage B HCC beyond the Up-to-seven criteriaCitation23 or BCLC stage C HCC. Patients with extrahepatic metastasis (n = 5) or inferior vena cava invasion (n = 4), and patients who could not be followed up for more than 3 months (n = 2) were excluded. However, patients who died within 3 months were included. Thus, 34 patients were included in this retrospective study. HCC was diagnosed according to the guidelines of the Japanese Society of Hepatology.Citation2 The final follow-up date for this study was September 30, 2021.
Dem-Tace
A 4-Fr long sheath (Radifocus® Introducer IIH, Terumo, Tokyo, Japan) was inserted into the femoral artery under local anesthesia. A 4-Fr guiding catheter (RC2, Medikit, Tokyo, Japan) was placed in the celiac artery and/or superior mesenteric artery. Using a 0.014 microguidewire (LABYRINTH, Piolax Medical Device, Kanagawa, Japan), a 2.0-Fr microcatheter (Estream 2.0 IGT type, Toray Medical, Tokyo, Japan) was advanced to the target hepatic artery. Digital subtraction angiography and computed tomography angiography (Toshiba Medical Systems, Tochigi, Japan) were performed to confirm the distribution of the drug in the target lesions. After confirming the blood supply to tumors, 1–3 anticancer drugs including doxorubicin (10–20 mg), epirubicin (10–20 mg), cisplatin (10–50 mg), or fluorouracil (250–500 mg) were selectively infused into the feeding arteries. The anticancer drugs were selected after considering the patient’s treatment history and known allergies. Then bevacizumab (50–200 mg) was infused into feeding arteries. Each anticancer drug was diluted in saline to a total of volume 20 mL and infused over several minutes. Immediately after drug infusion, embolization was performed with 25–50 or 50–100 μm superabsorbent polymer microspheres (SAP-MS) loaded with an anticancer drug (usually epirubicin 20 mg or doxorubicin 20 mg). This embolic material is self-preparing and has the same composition and properties as Hepasphere (Merit Medical Systems, Inc, South Jordan, Utah).Citation24 The anticancer drug to be loaded into the SAP-MS was dissolved in 1 mL of 10% sodium chloride and 4 mL of nonionic iodine contrast medium. This method reduced the expansion rate of SAP-MS by about twice.Citation25 The endpoint of embolization was defined as the disappearance of tumor staining, although a decrease in tumor staining was acceptable in patients with severe hepatic dysfunction. If a vascular lake appeared, embolization was performed using gelatin sponges. Generally, DEM-TACE with bevacizumab was repeated on demand if the tumor had progressed. Patients were followed up without additional treatment if the tumor had shrunk or remained unchanged. Occasionally, treatment was divided into several sessions, taking into account the distribution and number of tumors and liver function.
Post-TACE Assessments
The primary endpoints were overall survival (OS) and safety. OS was defined as the interval from the date of first treatment of DEM-TACE combined with intra-arterial infusion of bevacizumab to the date of death or, in the case of survivors, to the date of the last follow-up. Secondary endpoints were the response rate at 1 month and prognostic factors. Adverse events were assessed using the Common Terminology Criteria for Adverse Events v5.0 (CTCAE v5.0). Post-embolization syndrome (fever, pain, general fatigue, anorexia, nausea, and vomiting) was assessed during hospitalization and after discharge. Blood tests were performed before, the day after, and 1 month after treatment to evaluate changes in liver function. Liver function was assessed in terms of the changes in aspartate transaminase (AST), alanine transaminase (ALT), alkaline phosphatase (ALP), Child–Pugh gradeCitation26 and mALBI (modified albumin–bilirubin) grade.Citation27 The ALBI score was calculated from serum albumin (ALB) and total-bilirubin (T-Bil) values using the following formula: (log10 T-Bil [µmol/L] × 0.66) + (ALB [g/L] × −0.085), and categorized into three grades as follows: ≤ −2.60 = Grade 1; > −2.60 to ≤ −1.39 = Grade 2; > −1.39 = Grade 3.Citation28 The mALBI grade was also divided into two subgrades, ALBI grade 2a and 2b, based on the cutoff value of −2.270.Citation29 Tumor responses were evaluated by two radiologists according to the modified Response Evaluation Criteria in Solid Tumors (mRECIST)Citation30 using contrast-enhanced computed tomography (CE-CT) performed 1 month after the procedure. The objective response rate (ORR) was defined as (complete response [CR] + partial response [PR])/(CR + PR + stable disease [SD] + progressive disease [PD]) × 100(%). The disease control rate (DCR) was defined as (CR + PR + SD)/(CR + PR + SD + PD) × 100(%).
Statistical Analysis
OS was calculated using the Kaplan–Meier method and differences among subgroups of patients were determined using the Log rank test. Prognostic factors were investigated by univariate and multivariable analysis using the Cox proportional hazards model. Factors with a P-value of <0.05 in univariate analyses were included in multivariable models. Variables were selected using the backwards stepwise method with the Bayesian information criterion (BIC). P-values of <0.05 were considered statistically significant. Statistical analyses were performed using JMP Pro 14.1.0 (SAS Institute Inc., Cary, NC, USA) and R software version 4.1.1(R Foundation for Statistical Computing, Vienna, Austria).
Results
Patient Characteristics
The patient characteristics are shown in . There were 25 males and 9 females, with a median age of 68 years (range 49–85 years). The Child–Pugh class was A in 27 patients and B in 7 patients. There were 16 patients with BCLC stage B HCC beyond the Up-to-seven criteria and 18 with BCLC stage C HCC. Fifteen patients had portal vein invasion and 11 patients were classified as high risk based on tumor invasion of the main portal vein (Vp4) and/or bile duct, and/or tumor occupancy of ≥50% of the liver.Citation31 The median treatment interval was 2.2 months (95% confidence interval [CI] 0.7–42.2 months).
Table 1 Patient Characteristics (N = 34)
OS
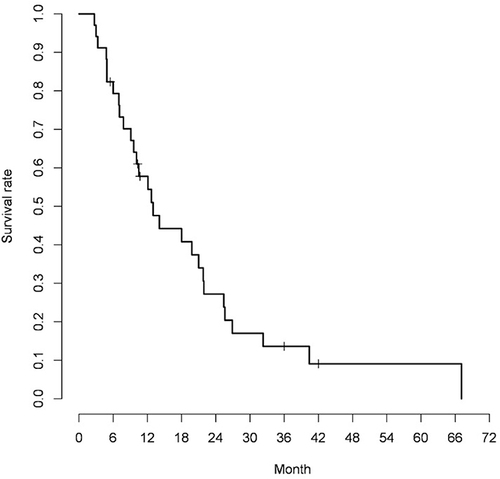
The median OS was 13 months (95% CI 9.1–21.8 months; ). The median OS was 10.1 months (95% CI 7.0–25.6 months) in patients with BCLC stage B HCC beyond the Up-to-seven criteria and 13 months (95% CI 7.1–21.8 months) in patients with BCLC stage C HCC, without a significant difference (p=0.724). The median OS was not significantly different between patients without portal vein invasion (14.1 months, 95% CI 7.1–21.8 months) and patients with portal vein invasion (10.1 months, 95% CI 3.3–40.4 months)(p=0.865). The median OS in patients with high-risk HCC was 7 months (95% CI 3.0–25.4 months), which was not significantly different to that of 18 months (95% CI 9.6–21.9 months) in non-high-risk patients(p=0.201). The median OS in patients using 25–50 μm SAP-MS was 18 months (95% CI 10.5–25.4 months), which was significantly different from that of 6.0 months (95% CI 2.7–14.1 months) in patients using 50–100 μm SAP-MS (p=0.011).
Figure 1 Kaplan-Meier curve for overall survival in all patients (median overall survival 13 months, 95% confidence interval 9.1–21.8).
Safety
There were no procedure-related complications during treatment, treatment-related deaths, adverse events associated with intra-arterial infusion of bevacizumab, or grade ≥3 adverse events. Grade 2 adverse events occurred in one patient during hospitalization and in another patient after discharge. Grade 1 adverse events were infrequent (). The Child–Pugh class did not change after treatment in 30 of 34 patients, worsened in three patients, and improved in one patient. None of the patients experienced grade ≥2 increases in AST, ALT, or ALP. The ALBI score increased temporarily on the day after treatment but improved at 1 month after treatment (). The mean hospital stay after treatment was 1.7 ± 0.7 days.
Table 2 Post-Embolization Syndrome
Table 3 Biochemistry, Hematology, and ALBI Score
Tumor Responses
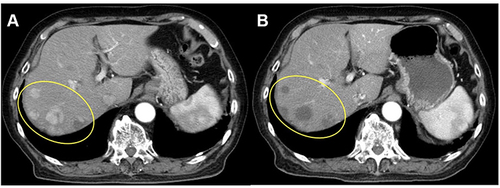
Tumor responses were evaluated in 21 patients with measurable lesions. There were three patients with PR and 18 with SD (). Therefore, the ORR was 14.2% (3/21) and the DCR was 100% (21/21). CE-CT images before and 1 month after treatment are shown in for one patient with PR.
Figure 2 Tumor responses at 1 month in individual patients with measurable lesions (N = 21).
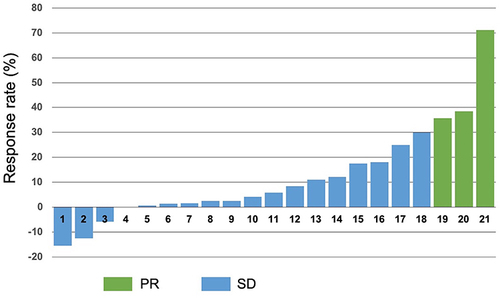
Figure 3 Arterial phase contrast-enhanced computed tomography images in a patient with a partial response. (A) Image obtained before treatment showing five viable lesions within the yellow oval. (B) Image obtained 1 month after treatment showing complete necrosis of three lesions and partial necrosis of two lesions.
Prognostic Factors
Significant prognostic factors were alcoholic liver disease, Child–Pugh score of ≥8, and microsphere size of 50–100 μm ().
Table 4 Prognostic Factors
Discussion
In this analysis of patients who underwent DEM-TACE combined with intra-arterial infusion of bevacizumab for treating uHCC, the median OS was 13 months (95% CI 9.1–21.8 months), which is comparable to the median OS (8.5–19.2 months) for currently approved systemic therapies.Citation8,Citation9,Citation32–35 Regarding the safety of the treatment, adverse events were infrequent and of low severity. This may represent a valuable advantage compared with current treatments for uHCC. Although most of the patients (85.7%) had SD, the ability to repeat treatment at the time of disease progression without a marked deterioration of liver function may have contributed to long-term disease control and prolonged prognosis. Using sorafenib, achieving SD for a long period of time is considered one of the most important goals for improving survival.Citation36 This concept also applies to the treatment used in this study. The majority of patients in this study were not indicated for cTACE and about half of the patients had portal vein invasion. Portal vein invasion is associated with worst prognosis,Citation37 with an OS of 2–4 months in untreated patients.Citation38 In our study, we found no significant difference in OS between patients with or without portal vein invasion. In our experience, two patients with portal vein tumor thrombosis extending into the main trunk of the portal vein survived for more than 2 years with DEM-TACE combined with intra-arterial infusion of bevacizumab.Citation39 This treatment method is expected to be effective regardless of the presence or absence of portal vein invasion. In this study, most of the patients with BCLC stage C HCC had portal vein invasion. We consider that there was no significant difference in OS between patients with BCLC stage B HCC beyond the Up-to-seven criteria and patients with BCLC stage C HCC because this treatment had similar results in patients with and without portal vein invasion. Recently, it was reported that hepatic arterial infusion chemotherapy (HAIC) is more effective than sorafenib in patients with portal vein invasion.Citation40,Citation41 However, considering the technical difficulty, length of hospital stay, complications and side effects, the treatment used here is technically simple and was associated with few side effects and short hospital stay, which may preserve the patient’s quality of life. In an updated analysis of the IMbrave150 study, a global, multicenter, open-label Phase 3 trial, the median OS was 7.6 months (95% CI 6.6–12.8 months) in the high-risk group.Citation31 In a multicenter analysis of the efficacy of lenvatinib in patients with highly advanced HCC, the median OS was 201 days in patients with a tumor thrombus in the main trunk of the portal vein (VP4) and 229 days in patients whose tumor occupied more than 50% of the liver.Citation42 In our study, the median OS in the high-risk group was 7.0 months (95% CI 3.0–25.4 months), similar to the values reported in those earlier studies. Therefore, if systemic therapy is not effective in patients with high-risk HCC, the treatment used here could be considered before selecting best supportive care.
The key benefits of the treatment used here, including the preservation of liver function, and the low frequency and low severity of adverse events, may be attributed to the use of microspheres and the fact that we did intend to completely halt blood flow during embolization. The use of microspheres may also contribute to the successful outcomes of TACE in patients with portal vein invasion without hepatic failure or hepatic infarction. Because microspheres do not reach the portal vein or sinusoids, their use can preserve portal vein blood flow and reduce the risk of hepatic infarction.Citation43 The PRECISION V multicenter Phase 2 study, which compared chemoembolization with drug-eluting beads (DEB-TACE) and cTACE, showed that the anticancer drug-related side effects and liver dysfunction were significantly milder with DEB-TACE, and that DEB-TACE was associated with a higher response rate in the Child–Pugh B, multiple tumors in both lobes, recurrence after TACE, and poor performance status subgroups.Citation17 In a recent prospective randomized controlled trial that compared DEB-TACE and cTACE, the frequency of post-embolization syndrome and the increases in T-Bil and ALT were significantly lower in the DEB-TACE group.Citation44 DEB-TACE was also reported to be a safe and effective treatment for intermediate and advanced HCC, and it can be repeated in patients with cirrhosis and decreased liver function.Citation18,Citation45 Because maintaining liver function is the most important aspect of treating HCC, the current data suggest that DEB-TACE is more suitable than cTACE in patients similar to those included in our study. The low frequency and low severity of adverse events may also contribute to shorter hospital stay after TACE. Such factors may also lead to an improvement in the patient’s quality of life.
Bevacizumab has recently become first-line therapy for uHCC in combination with atezolizumab,Citation8 and the clinical effects of bevacizumab are attracting increasing attention. Bevacizumab is a humanized monoclonal antibody that targets VEGF-A, an isoform of VEGF that stimulates the proliferation and migration of endothelial cells. Bevacizumab specifically binds to VEGF-A, and thereby inhibits angiogenesis.Citation46 TACE increases VEGF production in the residual surviving cancerous tissue.Citation20 Jia et al reported that the serum hypoxia-inducible factor (HIF-1α) and VEGF levels in patients with HCC were significantly higher than those in healthy volunteers.Citation19 The serum HIF-1α and VEGF levels reached peak values at 1 day after TACE. Although the levels decreased 1 week after TACE, they were still significantly greater than the levels measured before TACE. At 1 month after TACE, the serum HIF-1α and VEGF levels were significantly lower in patients with CR than in the group of patients with PR, SD, or PD.Citation19 This increase in VEGF is thought to contribute to disease recurrence after TACE.Citation19,Citation47 Bevacizumab also normalizes tumor vasculature and improves the tumor uptake of coadministered anticancer drugs.Citation22
In recent years, researchers have also become more interested in the effects of bevacizumab on the immune system. Bevacizumab is thought to reduce myeloid derived suppressor cells and regulatory T cells, thereby releasing immunosuppression of the tumor microenvironment.Citation48,Citation49 Therefore, TACE combined with intra-arterial infusion of bevacizumab may suppress hypoxia-induced VEGF secretion, inhibit invasion and metastasis, and normalize the tumor vasculature to enhance the effect of TACE. Prior studies have reported the safety and antitumor efficacy of concurrent TACE and intravenous bevacizumab.Citation47 It was reported that TACE plus intravenous bevacizumab diminished neovessel formation, detected by angiography, compared with TACE alone.Citation50 A systematic review of Phase 2 trials of bevacizumab for advanced HCC suggested that it may be a relatively effective and tolerable treatment. In that review, the trials had median PFS and OS of 5.3–9.0 and 5.9–13.7 months, respectively, with disease control rates ranging from 51.1% to 76.9% and response rates ranging from 0% to 23.7%.Citation51
Regarding intra-arterial infusion of bevacizumab, animal experiments have confirmed the antitumor effects of hepatic arterial infusion of bevacizumab for treating liver metastases from colorectal cancer.Citation52 In addition, for brain tumors, bevacizumab has been injected into the cerebral artery, and no side effects due to intra-arterial infusion were reported.Citation53 We also observed no adverse events associated with intra-arterial infusion of bevacizumab. In ophthalmology, bevacizumab is locally administered, and it has been reported that higher concentrations are more effective.Citation54 Intra-arterial infusion of bevacizumab can reduce the total dose required because this administration method increases the local concentration without greatly increasing systemic exposure. In our study, the dose was limited to 200 mg per procedure. Therefore, administering a low dose of bevacizumab can help to reduce side effects and cost.
We found that patients treated with 50–100 μm SAP-MS had a worse prognosis than patients treated with 25–50 μm SAP-MS. This might be due to selection bias because no clear criteria were established for selecting the size of SAP-MS. Malagary et al reported that the use of smaller microspheres was associated with greater local efficacy and better survival in patients with intermediate or advanced HCC,Citation18 which is compatible with our results. It is important to consider that SAP-MS show significant swelling (by about four times) in serum.Citation55 Thus, 50–100 µm SAP-MS swell to about 200–400 μm, which exceeds the standard size of 100–300 μm for other spherical embolic materials. So far, Hepasphere with a size of 30–60 μm has been marketed, and several studies have examined the efficacy and safety.Citation56,Citation57 The Child–Pugh score is a well-known prognostic factor for HCC,Citation58,Citation59 and we found that OS was significantly shorter in patients with a Child–Pugh score of ≥8 than in patients with a score of 5–7. This suggests that patients with a Child–Pugh score of ≤7 may experience a greater benefit of this treatment strategy. We also note that, in the intermediate stage subclassification, patients with Child–Pugh scores of 7 and 8 are classified into different groups.Citation36 Prior reports have also shown differences in prognosis and frequency of complications between patients with scores of 7 and 8 among those with Child–Pugh class B.Citation60–62 We also found that alcoholic liver disease was a poor prognostic factor. Although this finding is not common, several European studies have shown that alcohol-related HCC has a worse prognosis than non-alcohol-related HCC, not because alcohol-related HCC is more aggressive or shows worse treatment outcomes, but instead because delayed diagnosis appeared to affect prognosis.Citation63,Citation64 Because of the small number of patients with alcoholic liver disease in our study, it will be necessary to increase the number of patients for future studies.
This study has three limitations to discuss. First, it was a single-arm, single-center retrospective study with a small sample size. Second, we did not perform any comparisons with other treatment modalities such as cTACE or DEM-TACE without intra-arterial infusion of bevacizumab. Finally, the dose of bevacizumab, the types and doses of anticancer drugs, the size of SAP-MS, and the treatment methods varied among the patients.
Conclusion
This is the first report to describe the efficacy and safety of DEM-TACE combined with intra-arterial infusion of bevacizumab in patients with uHCC. The results show acceptable safety and efficacy of this treatment; therefore, we believe it will become a new treatment option for uHCC. In the future, we hope to increase the number of patients and further evaluate the efficacy and safety of this treatment, as well as determine the optimal dose of bevacizumab for intra-arterial infusion.
Data Sharing Statement
Due to the use of patient medical records, the data generated in this study are not publicly available.
Ethics Approval and Informed Consent
Chemoembolization with drug-eluting microspheres combined with intra-arterial infusion of bevacizumab was approved by the institutional review board of the Institute of Image Guided Therapy (protocol code no. 001). All patients provided written informed consent to undergo the procedures described. The institutional review board at the Institute of Image Guided Therapy approved this retrospective study (protocol code no. 14). Informed consent was obtained in the form of an opt-out option on the institution’s website and the need for written informed consent was waived, in compliance with the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no conflicts of interest in this work.
Additional information
Funding
References
- Yamada R, Sato M, Kawabata M, Nakatsuka H, Nakamura K, Takashima S. Hepatic artery embolization in 120 patients with unresectable hepatoma. Radiology. 1983;148(2):397–401. doi:10.1148/radiology.148.2.6306721
- Kudo M, Kawamura Y, Hasegawa K, et al. Management of Hepatocellular Carcinoma in Japan: JSH Consensus Statements and Recommendations 2021 Update. Liver Cancer. 2021;10(3):181–223. doi:10.1159/000514174
- European Association for the Study of the Liver. Corrigendum to “EASL Clinical Practice Guidelines: management of hepatocellular carcinoma” [J Hepatol 69 (2018) 182–236]. J Hepatol. 2019;70(4):817. doi:10.1016/j.jhep.2019.01.020.
- Bolondi L, Burroughs A, Dufour JF, et al. Heterogeneity of patients with intermediate (BCLC B) hepatocellular carcinoma: proposal for a subclassification to facilitate treatment decisions. Semin Liver Dis. 2013;32(04):348–359.
- Kudo M, Arizumi T, Ueshima K, Sakurai T, Kitano M, Nishida N. Subclassification of BCLC B stage hepatocellular carcinoma and treatment strategies: proposal of modified Bolondi’s subclassification (Kinki Criteria). Dig Dis. 2015;33(6):751–758. doi:10.1159/000439290
- Yamakado K, Miyayama S, Hirota S, et al. Subgrouping of intermediate-stage (BCLC stage B) hepatocellular carcinoma based on tumor number and size and Child–Pugh grade correlated with prognosis after transarterial chemoembolization. Jpn J Radiol. 2014;32(5):260–265. doi:10.1007/s11604-014-0298-9
- Kim JH, Shim JH, Lee HC, et al. New intermediate-stage subclassification for patients with hepatocellular carcinoma treated with transarterial chemoembolization. Liver Int. 2017;37(12):1861–1868. doi:10.1111/liv.13487
- Finn RS, Qin S, Ikeda M, et al. Atezolizumab plus bevacizumab in unresectable hepatocellular carcinoma. N Engl J Med. 2020;382(20):1894–1905. doi:10.1056/NEJMoa1915745
- Kudo M, Finn RS, Qin S, et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: a randomised phase 3 non-inferiority trial. The Lancet. 2018;391(10126):1163–1173. doi:10.1016/S0140-6736(18)30207-1
- Kudo M, Matsui O, Izumi N, et al. JSH consensus-based clinical practice guidelines for the management of hepatocellular carcinoma: 2014 update by the Liver Cancer Study Group of Japan. Liver Cancer. 2014;3(3–4):458–468. doi:10.1159/000343875
- Kudo M, Han K-H, Ye S-L, et al. A changing paradigm for the treatment of intermediate-stage hepatocellular carcinoma: Asia-Pacific primary liver cancer expert consensus statements. Liver Cancer. 2020;9(3):245–260. doi:10.1159/000507370
- Llovet JM, Villanueva A, Marrero JA, et al. trial design and endpoints in hepatocellular carcinoma: AASLD consensus conference. Hepatology. 2021;73(S1):158–191. doi:10.1002/hep.31327
- Hiraoka A, Kumada T, Kudo M, et al. Hepatic function during repeated TACE procedures and prognosis after introducing sorafenib in patients with unresectable hepatocellular carcinoma: multicenter analysis. Dig Dis. 2017;35(6):602–610. doi:10.1159/000480256
- Arizumi T, Ueshima K, Minami T, et al. Effectiveness of sorafenib in patients with transcatheter arterial chemoembolization (TACE) refractory and intermediate-stage hepatocellular carcinoma. Liver Cancer. 2015;4(4):253–262. doi:10.1159/000367743
- Peck-Radosavljevic M, Raoul J-L, Lee HC, Kudo M, Nakajima K, Cheng A-L. OPTIMIS: an international observational study to assess the use of sorafenib after transarterial chemoembolization (TACE) in patients with hepatocellular carcinoma (HCC).. J Clin Oncol. 2014;32(15_suppl):TPS4155. doi:10.1200/jco.2014.32.15_suppl.tps4155
- Ogasawara S, Chiba T, Ooka Y, et al. Efficacy of sorafenib in intermediate-stage hepatocellular carcinoma patients refractory to transarterial chemoembolization. Oncology. 2014;87(6):330–341. doi:10.1159/000365993
- Lammer J, Malagari K, Vogl T, et al. Prospective randomized study of doxorubicin-eluting-bead embolization in the treatment of hepatocellular carcinoma: results of the PRECISION V study. Cardiovasc Intervent Radiol. 2010;33(1):41–52. doi:10.1007/s00270-009-9711-7
- Malagari K, Pomoni A, Filippiadis D, Kelekis D. Chemoembolization of hepatocellular carcinoma with HepaSphereTM. Hepatic Oncol. 2015;2(2):147–157. doi:10.2217/hep.15.2
- Jia ZZ, Jiang GM, Feng YL. Serum HIF-1α and VEGF levels pre-and post-TACE in patients with primary liver cancer. Chin Med Sci J. 2011;26(3):158–162. doi:10.1016/s1001-9294(11)60041-2
- Wang B, Xu H, Gao ZQ, Ning HF, Sun YQ, Cao GW. Increased expression of vascular endothelial growth factor in hepatocellular carcinoma after transcatheter arterial chemoembolization. Acta Radiol. 2008;49(5):523–529. doi:10.1080/02841850801958890
- Liu K, Min XL, Peng J, Yang K, Yang L, Zhang XM. The changes of HIF-1α and VEGF expression after TACE in patients with hepatocellular carcinoma. J Clin Med Res. 2016;8(4):297–302. doi:10.14740/jocmr2496w
- Jain RK. Normalization of tumor vasculature: an emerging concept in antiangiogenic therapy. Science. 2005;307(5706):58–62. doi:10.1126/science.1104819
- Mazzaferro V, Llovet JM, Miceli R, et al. Predicting survival after liver transplantation in patients with hepatocellular carcinoma beyond the Milan criteria: a retrospective, exploratory analysis. Lancet Oncol. 2009;10(1):35–43. doi:10.1016/S1470-2045(08)
- Osuga K, Hori S, Hiraishi K, et al. Bland embolization of hepatocellular carcinoma using superabsorbent polymer microspheres. Cardiovasc Intervent Radiol. 2008;31(6):1108–1116. doi:10.1007/s00270-008-9369-6
- Sato T, Tanaka T, Nishiofuku H, et al. Superabsorbent polymer microspheres prepared with hypertonic saline to reduce microsphere expansion. Cardiovasc Intervent Radiol. 2018;41(9):1412–1418. doi:10.1007/s00270-018-1990-4
- Pugh RNH, Murray-Lyon IM, Dawson JL, Pietroni MC, Williams R. Transection of the oesophagus for bleeding oesophageal varices. BJS Br J Surg. 1973;60(8):646–649. doi:10.1002/bjs.1800600817
- Hiraoka A, Kumada T, Tsuji K, et al. Validation of modified ALBI Grade for more detailed assessment of hepatic function in hepatocellular carcinoma patients: a multicenter analysis. Liver Cancer. 2019;8(2):121–129. doi:10.1159/000488778
- Johnson PJ, Berhane S, Kagebayashi C, et al. Assessment of liver function in patients with hepatocellular carcinoma: a new evidence-based approach—the ALBI grade. J Clin Oncol. 2015;33(6):550–558. doi:10.1200/JCO.2014.57.9151
- Hiraoka A, Michitaka K, Kumada T, et al. Validation and potential of albumin-bilirubin grade and prognostication in a nationwide survey of 46,681 hepatocellular carcinoma patients in Japan: the need for a more detailed evaluation of hepatic function. Liver Cancer. 2017;6(4):325–336. doi:10.1159/000479984
- Lencioni R, Llovet JM. Modified RECIST (mRECIST) Assessment for Hepatocellular Carcinoma. Semin Liver Dis. 2010;30(1):052–060.
- Finn RS, Qin S, Ikeda M, et al. Abstract CT009: iMbrave150: updated efficacy and safety by risk status in patients (pts) receiving atezolizumab (atezo) + bevacizumab (bev) vs sorafenib (sor) as first-line treatment for unresectable hepatocellular carcinoma (HCC). Cancer Res. 2021;81(13_Supplement):CT009. doi:10.1158/1538-7445.AM2021-CT009
- Llovet JM, Ricci S, Mazzaferro V, et al. Sorafenib in advanced hepatocellular carcinoma. N Engl J Med. 2008;359(4):378–390. doi:10.1056/NEJMoa0708857
- Bruix J, Qin S, Merle P, et al. Regorafenib for patients with hepatocellular carcinoma who progressed on sorafenib treatment (RESORCE): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2017;389(10064):56–66. doi:10.1016/S0140-6736(16)32453-9
- Abou-Alfa GK, Meyer T, Cheng AL, et al. Cabozantinib in patients with advanced and progressing hepatocellular carcinoma. N Engl J Med. 2018;379(1):54–63. doi:10.1056/NEJMoa1717002
- Zhu AX, Kang YK, Yen CJ, et al. Ramucirumab after sorafenib in patients with advanced hepatocellular carcinoma and increased α-fetoprotein concentrations (REACH-2): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2019;20(2):282–296. doi:10.1016/S1470-2045(18)30937-9
- Arizumi T, Ueshima K, Chishina H, et al. Duration of stable disease is associated with overall survival in patients with advanced hepatocellular carcinoma treated with sorafenib. Dig Dis. 2014;32(6):705–710. doi:10.1159/000368006
- Ikai I, Arii S, Kojiro M, et al. Reevaluation of prognostic factors for survival after liver resection in patients with hepatocellular carcinoma in a Japanese nationwide survey. Cancer. 2004;101(4):796–802. doi:10.1002/cncr.20426
- Han K. Treatment of hepatocellular carcinoma with portal venous tumor thrombosis: a comprehensive review. World J Gastroenterol. 2016;22(1):407. doi:10.3748/wjg.v22.i1.407
- Hori A, Ueda S, Hori S, et al. [Microsphere TACE with arterial infusion of bevacizumab for portal vein tumor thrombus by hepatocellular carcinoma]. Gan Kagaku Ryoho. 2021;48(11):1389–1392. Japanese
- Ueshima K, Ogasawara S, Ikeda M, et al. Hepatic arterial infusion chemotherapy versus sorafenib in patients with advanced hepatocellular carcinoma. Liver Cancer. 2020;9(5):583–595. doi:10.1159/000508724
- Iwamoto H, Niizeki T, Nagamatsu H, et al. Survival benefit of hepatic arterial infusion chemotherapy over sorafenib in the treatment of locally progressed hepatocellular carcinoma. Cancers. 2021;13(4):646. doi:10.3390/cancers13040646
- Chuma M, Uojima H, Hiraoka A, et al. Analysis of efficacy of lenvatinib treatment in highly advanced hepatocellular carcinoma with tumor thrombus in the main trunk of the portal vein or tumor with more than 50% liver occupation: a multicenter analysis. Hepatol Res. 2021;51(2):201–215. doi:10.1111/hepr.13592
- Osuga K, Khankan AA, Hori S, et al. Transarterial embolization for large hepatocellular carcinoma with use of superabsorbent polymer microspheres: initial experience. J Vasc Interv Radiol. 2002;13(9):929–934. doi:10.1016/s1051-0443(07)
- Ikeda M, Inaba Y, Tanaka T, et al. A prospective randomized controlled trial of selective transarterial chemoembolization using drug-eluting beads loaded with epirubicin versus selective conventional transarterial chemoembolization using epirubicin-lipiodol for hepatocellular carcinoma: the JIVROSG-1302 PRESIDENT study. J Clin Oncol. 2020;38(15_suppl):4518. doi:10.1200/JCO.2020.38.15_suppl.4518
- Prajapati HJ, Dhanasekaran R, El-Rayes BF, et al. Safety and efficacy of doxorubicin drug-eluting bead transarterial chemoembolization in patients with advanced hepatocellular carcinoma. J Vasc Interv Radiol. 2013;24(3):307–315. doi:10.1016/j.jvir.2012.11.026
- Mukherji SK. Bevacizumab (Avastin). Am J Neuroradiol. 2010;31(2):235–236. doi:10.3174/ajnr.A1987
- Buijs M, Reyes DK, Pawlik TM, et al. Phase 2 trial of concurrent bevacizumab and transhepatic arterial chemoembolization in patients with unresectable hepatocellular carcinoma. Cancer. 2013;119(5):1042–1049. doi:10.1002/cncr.27859
- Voron T, Colussi O, Marcheteau E, et al. VEGF-A modulates expression of inhibitory checkpoints on CD8+ T cells in tumors. J Exp Med. 2015;212(2):139–148. doi:10.1084/jem.20140559
- Hegde PS, Wallin JJ, Mancao C. Predictive markers of anti-VEGF and emerging role of angiogenesis inhibitors as immunotherapeutics. Immuno-Oncol Biomark. 2018;52:117–124. doi:10.1016/j.semcancer.2017.12.002
- Britten CD, Gomes AS, Wainberg ZA, et al. Transarterial chemoembolization plus or minus intravenous bevacizumab in the treatment of hepatocellular cancer: a pilot study. BMC Cancer. 2012;12(1):16. doi:10.1186/1471-2407-12-16
- Fang P, Hu JH, Cheng ZG, Liu ZF, Wang JL, Jiao SC. Efficacy and safety of bevacizumab for the treatment of advanced hepatocellular carcinoma: a systematic review of Phase II trials. PLoS One. 2012;7(12):e49717. doi:10.1371/journal.pone.0049717
- Sperling J, Schäfer T, Ziemann C, et al. Hepatic arterial infusion of bevacizumab in combination with oxaliplatin reduces tumor growth in a rat model of colorectal liver metastases. Clin Exp Metastasis. 2012;29(2):91–99. doi:10.1007/s10585-011-9432-6
- Boockvar JA, Tsiouris AJ, Hofstetter CP, et al. Safety and maximum tolerated dose of superselective intraarterial cerebral infusion of bevacizumab after osmotic blood-brain barrier disruption for recurrent malignant glioma: clinical article. J Neurosurg. 2011;114(3):624–632. doi:10.3171/2010.9.JNS101223
- Habot-Wilner Z, Barequet IS, Ivanir Y, Moisseiev J, Rosner M. The inhibitory effect of different concentrations of topical bevacizumab on corneal neovascularization. Acta Ophthalmol. 2010;88(8):862–867. doi:10.1111/j.1755-3768.2009.01571.x
- Jiaqi Y, Hori S, Minamitani K, et al. A new embolic material: super absorbent polymer (SAP) microsphere and its embolic effects. Nihon Igaku Hoshasen Gakkai Zasshi Nippon Acta Radiol. 1996;56(1):19–24.
- Malagari K, Pomoni M, Moschouris H, et al. Chemoembolization of hepatocellular carcinoma with HepaSphere 30–60 μm. Safety and efficacy study. Cardiovasc Intervent Radiol. 2014;37(1):165–175. doi:10.1007/s00270-013-0777-x
- Bishay VL, Maglione K, Khanna R, et al. Chemoembolization with drug-eluting microspheres (DEM-TACE) for hepatocellular carcinoma: single-center review of safety and efficacy. J Hepatocell Carcinoma. 2014;1:187–193. doi:10.2147/JHC.S71602
- Brown DB, Fundakowski CE, Lisker-Melman M, et al. Comparison of MELD and Child-Pugh scores to predict survival after chemoembolization for hepatocellular carcinoma. J Vasc Interv Radiol. 2004;15(11):1209–1218. doi:10.1097/01.RVI.0000128123.04554.C1
- Yamakado K, Miyayama S, Hirota S, et al. Prognosis of patients with intermediate-stage hepatocellular carcinomas based on the Child-Pugh score: subclassifying the intermediate stage (Barcelona Clinic Liver Cancer stage B). Jpn J Radiol. 2014;32(11):644–649. doi:10.1007/s11604-014-0358-1
- Piscaglia F, Terzi E, Cucchetti A, et al. Treatment of hepatocellular carcinoma in Child-Pugh B patients. Dig Liver Dis. 2013;45(10):852–858. doi:10.1016/j.dld.2013.03.002
- Kim JE, Ryoo BY, Ryu MH, et al. Sorafenib for hepatocellular carcinoma according to Child-Pugh class of liver function. Cancer Chemother Pharmacol. 2011;68(5):1285–1290. doi:10.1007/s00280-011-1616-x
- Ogasawara S, Chiba T, Ooka Y, et al. Sorafenib treatment in Child–Pugh A and B patients with advanced hepatocellular carcinoma: safety, efficacy and prognostic factors. Invest New Drugs. 2015;33(3):729–739. doi:10.1007/s10637-015-0237-3
- Bucci L, Garuti F, Camelli V, et al. Comparison between alcohol‐and hepatitis C virus‐related hepatocellular carcinoma: clinical presentation, treatment and outcome. Aliment Pharmacol Ther. 2016;43(3):385–399. doi:10.1111/apt.13485
- Costentin CE, Mourad A, Lahmek P, et al. Hepatocellular carcinoma is diagnosed at a later stage in alcoholic patients: results of a prospective, nationwide study. Cancer. 2018;124(9):1964–1972. doi:10.1002/cncr.31215