
Abstract
Purpose
Combining transarterial chemoembolization (TACE) with systemic therapy has shown significant efficacy for intermediate-stage hepatocellular carcinoma (HCC) patients. This study aimed to validate the therapeutic efficacy of TACE combined with atezolizumab and bevacizumab (TACE + Atez/Bev) compared to TACE alone.
Methods
A retrospective study was conducted across three centers in China, encompassing 155 patients at the intermediate-stage of HCC. Propensity Score Matching (PSM) was used to minimize selection bias, with a ratio of 1:1. Primary outcomes were TACE-specific Progression-Free Survival (PFS) and Overall Survival (OS). Objective Response Rate (ORR) and Disease Control Rate (DCR) were assessed based on the modified Response Evaluation Criteria in Solid Tumors (mRECIST). Adverse events (AEs) related to treatment were analyzed to evaluate safety.
Results
Before PSM, the TACE + Atez/Bev group demonstrated extended median OS (not reached vs 20.3 months, P = 0.004) and PFS (20.0 months vs 9.8 months, P = 0.029) compared to the TACE-alone group. The TACE + Atez/Bev group also had a higher ORR (60.9% vs 41.3%, P = 0.026) and DCR (89.1% vs 58.7%, P < 0.001) than the TACE-alone group. After applying the PSM, the study included 42 pairs of patients. Compared to the TACE-alone group, the combination therapy group also showed significantly longer median OS (not reached vs 21.4 months, P = 0.008) and PFS (21.7 vs 9.7 months, P = 0.009). The combination therapy group also had a higher ORR (66.7% vs 38.1%, P = 0.009) and DCR (92.9% vs 57.1%, P < 0.001). AEs in the combination therapy group were mostly manageable, with the most common being elevated liver transaminase.
Conclusion
In treating intermediate-stage HCC, the survival benefit of combining TACE with atezolizumab and bevacizumab was significantly higher than TACE alone, and the treatment was well-tolerated.
Introduction
Hepatocellular carcinoma (HCC) ranks as the sixth most prevalent cancer and the third highest contributor to cancer-related fatalities globally.Citation1 The early stages of HCC often exhibit no symptoms, leading to over half of the patients being diagnosed at intermediate to advanced stages, hence missing the opportunity for radical resection.Citation2,Citation3
Patients with intermediate-stage HCC fall under the category of Barcelona Clinic Liver Cancer (BCLC) stage B.Citation1 Transarterial chemoembolization (TACE) is the recommended standard treatment for these patients according to multiple guidelines.Citation4–7 However, the effectiveness of TACE alone is often limited due to the high heterogeneity of intermediate-stage liver cancer.Citation8,Citation9 The latest BCLC guidelines have been revised to recommend systemic therapy for some patients in stage B, in addition to TACE.Citation10 The TACTICS trial has successfully demonstrated that the combined or sequential use of sorafenib and TACE can provide significant clinical benefits in TACE-specific Progression-Free Survival (PFS),Citation11 and an increasing number of studies have found that TACE combined with other systemic therapies can improve the prognosis of HCC patients.Citation12–15 TACE induces tumor necrosis by embolizing the tumor-supplying arteries, leading to an elevated expression of the vascular endothelial growth factor (VEGF).Citation16 Furthermore, TACE triggers an increase in the release of tumor neoantigens, thereby boosting immune activation and recognition.Citation17 Atezolizumab and bevacizumab, respectively a PD-L1 inhibitor and an anti-angiogenic drug, are recommended as the first-line systemic treatment for patients with intermediate to advanced liver cancer when used in combination.Citation10,Citation18 Thus, combining TACE with atezolizumab plus bevacizumab (Atez/Bev) is promising as a treatment approach. However, there is currently limited data available on this treatment regimen.
Therefore, we embarked on a multicenter retrospective cohort study to compare the effectiveness of TACE plus Atez/Bev (TACE + Atez/Bev) versus TACE alone in treating patients with intermediate-stage HCC.
Patients and Methods
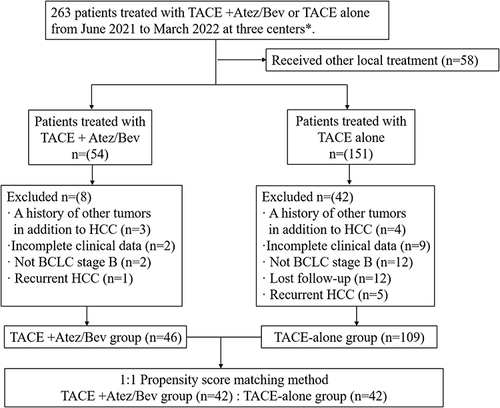
We retrospectively reviewed patients at the intermediate-stage of HCC who received either TACE alone or TACE + Atez/Bev as their first-line therapy at Ningbo No.2 Hospital, Eastern Hepatobiliary Hospital, and the First Affiliated Hospital of Wenzhou Medical University from June 2021 to Mar 2022. The inclusion criteria encompassed patients: (1) diagnosed with HCC at BCLC B stage (multinodular, without macrovascular invasion and extrahepatic metastasis, showcasing preserved liver function and devoid of cancer-related symptoms); (2) treated with either TACE alone or TACE + Atez/Bev; (3) demonstrating adequate liver function (Child-Pugh A or B7); (4) with at least one measurable lesion on Computed Tomography (CT) and Magnetic Resonance Imaging (MRI) as per the modified Response Evaluation Criteria in Solid Tumors (mRECIST) criteria.Citation19 Patients were excluded if they had: (1) a history of other tumors besides HCC; (2) undergone other local treatments, such as ablation, radiotherapy and Hepatic arterial infusion chemotherapy (HAIC); (3) recurrent HCC; (4) incomplete clinical data; (5) lost to follow-up; (6) staging other than BCLC B.
This study received approval from the Institutional Ethics Committee at the Ningbo No.2 Hospital, Eastern Hepatobiliary Hospital and the First Affiliated Hospital of Wenzhou Medical University. Given the retrospective nature of this study and the anonymity maintained for all patients, all three ethics committees waived the requirement for informed consent.
Tace
TACE procedures were carried out employing the Seldinger technique. A femoral artery puncture was performed under local anesthesia. Guided by Digital Subtraction Angiography (DSA), the puncture catheter was introduced into the tumor-feeding artery. This catheter administered either doxorubicin hydrochloride, pirarubicin, or epirubicin and iodized oil. The dosage of iodized oil and doxorubicin was modulated based on the patient’s liver function and body surface area. This was followed by an injection of gelatin sponge particles to embolize the tumor-feeding vessels. In instances where follow-up CT or MRI scans revealed considerable residual viable tumor tissue, and the patient’s liver function was deemed satisfactory, TACE could be administered repeatedly every 4 to 6 weeks.
Atezolizumab and Bevacizumab
Within 7 days post-TACE, treatments with atezolizumab and bevacizumab were initiated. The doses of atezolizumab and bevacizumab were respectively set at 1200mg and 15mg per kilogram of body weight and administered intravenously every 3 weeks.Citation20 In the event of severe toxic side effects during the treatment, the clinician may opt to halt one or both medications. Medication can be resumed after the resolution of adverse reactions based on the clinician’s assessment.
Follow-Up and Safety Analyses
All patients were put on follow-up every 6–8 weeks. Every routine follow-up session involved a physical examination, lab blood tests, and enhanced CT/MRI scans. The latest follow-up was conducted on June 1st, 2023. The primary endpoint of this study was Overall survival (OS), defined as the duration from the initial treatment until death from any cause or the most recent follow-up. The secondary outcome was TACE-specific PFS,Citation21 and the definition is as follows: from the initiation of the first TACE session until TACE can no longer be performed or the patient no longer benefits from TACE treatment. This includes: 1) intrahepatic tumor progression (an increase of 25% compared to baseline), 2) rapid deterioration of liver function following TACE, with a decline to Child-Pugh class C, and 3) the occurrence of macrovascular invasion or extrahepatic metastasis. Another secondary outcome was tumor progression, which was assessed based on mRECIST criteria. Adverse events (AEs) were extracted from outpatient visit records or medical histories, and were evaluated based on the Common Terminology Criteria for Adverse Events (CTCAE, version 5.0).
Statistical Analysis
A comprehensive statistical analysis was conducted on all clinical data using the IBM SPSS Statistics 23 or R 4.3.1 software (http://www.r-project.org/). We employ propensity score matching (PSM) at a ratio of 1:1 to balance the characteristics of patients in the TACE + Atez/Bev group and the TACE-alone group, aiming to minimize the impact of potential confounding factors. The matched data includes sex, age, hepatitis B surface antigen, Child-Pugh grade, alpha‐fetoprotein concentration, Protein Induced by Vitamin K Absence or Antagonist II, alanine aminotransferase (ALT), aspartate aminotransferase (AST), albumin (ALB), total bilirubin levels, as well as Albumin-bilirubin grade, number of nodules, tumor size, and up-to-7 criteria. Additionally, we employed the Inverse Probability of Treatment Weighting (IPTW) approach to further calibrate the baseline characteristics between the two groups, while also conducting post-matching survival analysis. Continuous variables were compared using t-tests, while categorical variables were assessed using χ2 tests or Fisher’s exact tests. The “cobalt” package in R software was used to compare the baseline differences between the matched groups. We employed the Kaplan-Meier method to calculate survival curves, and Log rank tests were utilized for their comparison. To pinpoint potential risk factors linked to PFS and OS, we carried out a Univariate COX regression analysis. Factors that demonstrated P < 0.20 in the univariate COX regression results were advanced to the multivariate regression analysis (Enter regression, P < 0.05). We designated P < 0.05 as the threshold for marking significant differences.
Results
Study Population
As depicted in , the study encompassed 46 TACE + Atez/Bev patients and 109 separate TACE treatment patients. We have illustrated the baseline characteristics of both patient groups in before and after PSM. There was no statistical difference at baseline between the two groups after PSM. The median follow-up duration for the entire cohort was 18.8 months (95% CI: 18.0–19.6 months), including 20.6 months (95% CI: 18.2–22.9 months) in TACE+Atez/Bev group and 18.3 months (95% CI: 17.5–19.2 months) in TACE-alone group. In the whole cohort, a total of 66 patients passed away during the study period, with 13 from the TACE + Atez/Bev group and 53 from the TACE-alone group. Both groups’ median number of TACE procedures was recorded twice, with the TACE + Atez/Bev group having a range of 1–4 and the TACE-alone group having a range of 1–6. The median number of Atez/Bev treatments applied in the TACE + Atez/Bev group stood at 6 (range, 1–20).
Table 1 Baseline Characteristics of the Patients
Figure 1 Diagram of patient screening.
Survival
and present the Kaplan-Meier curves of OS and PFS before and after PSM for the two treatment groups. Before PSM, the median OS for the TACE+Atez/Bev group was not reached, with a 1-year OS rate of 84.8%, while the median OS for the TACE-alone group was 20.3 months (95% CI = 15.8-NA months), with a 1-year OS rate of 63.3%. The median PFS for the TACE+Atez/Bev group and the TACE-alone group were 20.0 months (95% CI = 11.4-NA months) and 9.8 months (95% CI = 7.3–15.4 months), respectively, with 1-year PFS rates of 58.7% and 45.0%. Before PSM, the TACE+Atez/Bev treatment significantly improved patients’ OS (not reached vs 20.3 months, P = 0.004) and PFS (20.0 months vs 9.8 months, P = 0.029) compared to TACE alone treatment.
Figure 2 Kaplan-Meier curves for OS in patients with intermediate-stage HCC treated with TACE + Atez/Bev or TACE-alone before and after PSM. (2A) before PSM; (2B) after PSM.
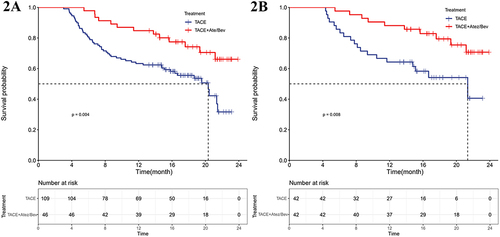
Figure 3 Kaplan-Meier curves for PFS in patients with intermediate-stage HCC treated with TACE + Atez/Bev or TACE-alone before and after PSM. (3A) before PSM; (3B) after PSM.
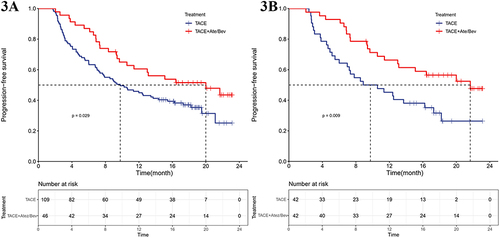
After PSM, the median OS of the TACE + Atez/Bev group was not reached, and the median PFS was 21.7 months (95% CI = 13.1-NA months), with 1-year OS and PFS rates of 88.1% and 64.3%, respectively. In contrast, the TACE-alone group had median OS and PFS durations of 21.4 months (95% CI = 14.8-NA months) and 9.7 months (95% CI = 7.0–18.2 months), with 1-year OS and PFS rates of 64.3% and 45.2%, respectively. Therefore, after PSM, the combined treatment also demonstrated a significant improvement in patients’ OS (not reached vs 21.4 months, P = 0.008) and PFS (21.7 months vs 9.7 months, P = 0.009) compared to TACE alone treatment.
Prognostic Factors for OS and PFS
As depicted in Supplementary Table S1, we utilized univariate and multivariate Cox regression analyses to identify factors associated with OS and PFS before PSM. Within the ambit of multivariate Cox regression analyses, combined therapy emerged as a protective factor influencing OS (HR = 0.44, 95% CI: 0.24–0.82, P = 0.010) and PFS (HR = 0.60, 95% CI: 0.38–0.97, P = 0.036). Conversely, beyond up-to-7 criteria identified as a risk factor affecting OS and PFS, with HRs of 4.47 (95% CI: 1.61–12.37, P = 0.004) and 3.13 (95% CI: 1.46–6.69, P = 0.003) respectively. As depicted in , after the application of PSM, beyond up-to-7 criteria persisted as an independent risk factor detrimentally impacting OS and PFS, with HRs of 7.55 (95% CI: 1.53–37.34, P = 0.013) and 3.01 (95% CI: 1.11–8.19, P = 0.031) in the multivariate Cox regression analyses.
Table 2 Univariate and Multivariate Cox Proportional Hazards Regression Model Analysis of OS and PFS After PSM
Tumor Response
As shown in Supplementary Table S2, before PSM, the ORR for the TACE + Atez/Bev group and the TACE-alone group were 60.9% and 41.3%, respectively (P = 0.026), and the DCR was 89.1% and 58.7% respectively (P < 0.001). After PSM, As depicted in , the ORR for the combination therapy group and the monotherapy group were 66.7% and 38.1%, respectively (P = 0.009), and the DCR was 92.9% and 57.1%, respectively (P < 0.001). Therefore, before and after PSM, the ORR and DCR in the combination therapy group were higher than in the monotherapy group.
Table 3 Best Tumor Response According to mRECIST After PSM
Subgroup Analysis
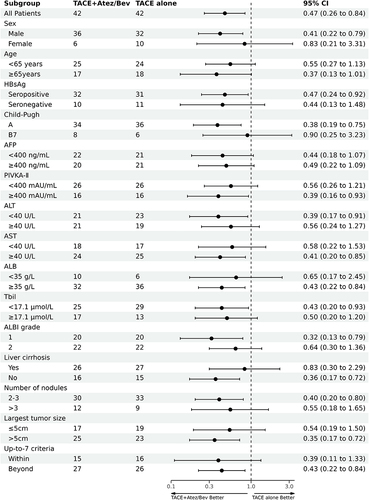
and present the forest plot of the subgroup analysis for OS and PFS in both the TACE + Atze/Bev and TACE-alone groups after PSM, respectively. The subgroup analysis reveals that, in comparison to TACE alone, TACE + Atez/Bev is associated with improved OS and PFS in most patient subgroups, notably in those with the largest tumor size ≥ 5cm and beyond the up-to-7 criteria, both of which are prognostically significant. Moreover, we executed subgroup analyses of OS and PFS on patients before PSM, as illustrated in Supplementary Figures S1 and S2. The results procured from these analyses were fundamentally congruent with those obtained post-PSM.
Figure 4 Forest plot of OS in subgroup analysis after PSM.
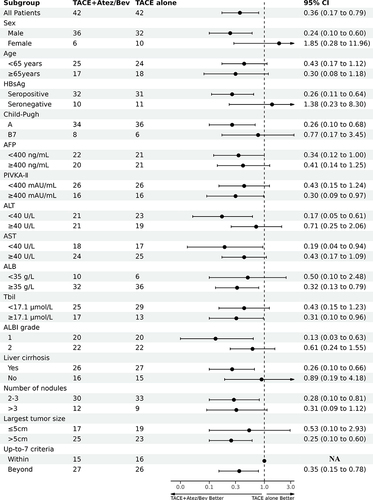
Figure 5 Forest plot of PFS in subgroup analysis after PSM.
Safety Outcomes
According to CTCAE version 5.0, treatment-related AEs were assessed based on frequency and severity. As depicted in , the common adverse reactions in the TACE + Atez/Bev group were elevated ALT (43.5%) and AST (41.3%), decreased ALB (37.0%), and hypertension (34.8%), with elevated ALT (10.9%) and hypertension (10.9%) being the most common grade 3/4 adverse reaction. Atez/Bev therapy was discontinued in two patients because of gastrointestinal hemorrhage. In the TACE-alone group, the common adverse reactions included elevated ALT (30.3%) and AST (27.5%), along with hypertension (29.4%), with the most common grade 3/4 adverse reaction being elevated ALT (10.1%). The combined treatment group is more susceptible to developing hypoalbuminemia (any grade and grade ≥3) and a reduction in platelet count (any grade). In the cohort undergoing combination therapy, six patients exhibited severe hepatic injury: two patients presented with concurrent elevations in ALT and AST levels (exceeding quintuple their baseline values), coupled with significant hypoalbuminemia (<20g/L); one patient exhibited isolated elevations in ALT and AST (exceeding septuple his baseline values); two patients experienced exclusive elevations in ALT levels (exceeding quintuple their baseline values), with concomitant AST elevation (Grade 2); and one patient developed hypoalbuminemia (<20g/L) with associated increases in ALT and AST (Grade 2). The temporal onset of hepatic injury in these six patients was as follows: one patient developed liver injury on day 18 following the initial administration of Atez/Bev treatment; another on day 14 after the second Atez/Bev treatment; three within one week post the third Atez/Bev treatment; and one on day 70. Four patients were administered intravenous methylprednisolone at a dose of 0.5 mg/kg/day as a standard intervention, and those with hypoalbuminemia were treated with intravenous infusion of human albumin. All six above patients exhibited clinical improvement post-treatment, and no fatalities were attributed to adverse reactions. After the onset of liver injury, four patients discontinued Atez/Bev therapy and altered their subsequent systemic treatment regimens; two resumed Atez/Bev therapy after albumin supplementation.
Table 4 Treatment Emergent Adverse Events
Subsequent Treatments
illustrates the alternative treatment approaches adopted by two groups of patients after disease progression. In the TACE + Atez/Bev group, 24 patients switched treatments, compared to 69 patients in the TACE-alone group. Most patients in the TACE + Atez/Bev group shifted to either atezolizumab + lenvatinib or lenvatinib monotherapy. Meanwhile, in the TACE-alone group, most patients received treatment with tyrosine kinase inhibitors, including Lenvatinib, Sorafenib, and Regorafenib. Most patients underwent repeated TACE treatments after progression until they were untraceable in both groups.
Table 5 Alternative Treatment Approaches Adopted by Patients After Disease Progression
Analysis Results After IPTW
As demonstrated in Supplementary Table S3, following IPTW adjustment, the number of patients in both groups increased compared to prior counts, with no significant baseline differences between the groups. Post-IPTW, the TACE + Atez/Bev group exhibited superior outcomes in OS (median OS, not reached vs 20.3 months, P = 0.004) and PFS (median PFS, 16.4 vs 10.2 months, P = 0.029) relative to the TACE-alone group (Supplementary Figure S3). Furthermore, beyond the up-to-7 criteria, it emerged as an independent risk factor affecting both OS and PFS in the multivariate Cox regression analysis (Supplementary Table S4), maintaining consistency with the results analyzed before and after PSM.
Discussion
This study compared the efficacy and safety of TACE + Atez/Bev versus TACE alone for patients with intermediate-stage HCC. The results indicated that the combination therapy significantly extended both OS and PFS compared to TACE alone. Moreover, the combination therapy demonstrated superior ORR and DCR. In a multivariate Cox regression analysis, TACE + Atez/Bev was identified as an independent predictive factor for improved prognosis, while beyond the up-to-7 criteria was an independent risk factor for prognosis. The safety of the combination therapy was acceptable, with no unexpected adverse or toxic reactions observed. In conclusion, we believe TACE + Atez/Bev therapy may be one of the best treatment options for HCC patients in BCLC B.
The latest 2022 revision of the BCLC staging system has split stage B into three subgroups. Both TACE and systemic therapy are recommended for patients in stage B, particularly for those with diffuse, infiltrative, and extensive involvement of both lobes of the liver, where systemic treatment is more strongly advised.Citation10 More recently, the multiparametric therapeutic hierarchy concept, introduced by Alessandro Vitale et alCitation22 has emphasized personalized treatment approaches for HCC. This has led to a more diverse array of treatment options for patients with BCLC stage B. In recent years, an escalating number of clinicians have commenced trials of TACE in conjunction with systemic therapy, as opposed to the solitary application of TACE. The EMERALD-1 trialCitation23 reported that the combination treatment of TACE with durvalumab and bevacizumab, as opposed to placebo plus TACE, demonstrated a benefit in PFS. However, the combination of TACE with durvalumab, when compared to placebo plus TACE, did not exhibit a PFS advantage. A potential reason could be that TACE induces tumor necrosis and subsequently activates tumor-specific T cells.Citation24–26 However, the immune activation brought about by TACE might not be sufficient to control tumor growth and prevent the recurrence of HCC. Studies have found that TACE can increase the expression of PD-1 and PD-L1 related mRNA and VEGF.Citation27,Citation28 The binding of PD-L1 ligands on tumor cells with PD-1 receptors on T cells can inhibit the immune toxic effects of T cells, thus leading to immune evasion of tumor cells.Citation29 In addition to promoting angiogenesis, VEGF can increase the intratumoural number of regulatory T cells and myeloid-derived suppressor cells,Citation30,Citation31 and inhibit the maturation of dendritic cells from influencing immune responses.Citation32,Citation33 Furthermore, VEGF has been found to impede the development and function of T cells,Citation34,Citation35 and promote T-cell exhaustion by upregulating immune checkpoints.Citation36 These studies also provide a theoretical basis for the superiority of combined TACE treatment with Atez/Bev over TACE alone.
Lenvatinib, a classic tyrosine kinase inhibitor, has been recommended as the first-line systemic therapy for HCC over the past several years.Citation37 FU’s research teamCitation2 has discovered that the combination of Lenvatinib with TACE yields better clinical benefits than TACE alone in both OS and PFS. Atezolizumab, a PD-L1 inhibitor, and bevacizumab, an anti-angiogenesis drug, are now recommended as the first-line treatment plan for advanced liver cancer when used together. The CHANCE001Citation38 trial revealed that combining TACE with PD-(L)1 inhibitors plus molecular targeted therapies could improve PFS, OS, and ORR in patients with advanced liver cancer compared to TACE alone. The single-arm study performed by Wang’s research,Citation39 on patients beyond the up-to-7 criteria for HCC, who underwent TACE + Atez/Bev treatment, found that this combined therapy has good clinical benefits and acceptable safety. However, there have not been any reports on comparing TACE combined with Atez/Bev versus TACE alone, which has prompted us to conduct this study.
Given the significant heterogeneity in tumor burden and liver function among patients with HCC, more researchers are exploring novel clinical endpoints such as time to treatment failure and time to unTACEable progression (TTUP) to assess the efficacy of TACE.Citation40–42 Kudo’s analysisCitation43 suggests that the relative success of the TACTICS trial was primarily due to intrahepatic de novo lesions not being considered as tumor progression, along with the incorporation of TTUP as a trial endpoint. In light of these studies, we have employed TACE-specific PFS as a metric to evaluate the therapeutic effectiveness of TACE.
In our study, the median PFS for the TACE + Atez/Bev group (20.0 months before PSM and 21.7 months after PSM) matching closely with the triple therapy regimen (TACE + Lenvatinib + PD-1 inhibitors) of Xiang’s studyCitation44 and the dual therapy regimen (Sorafenib + TACE) of Kudo’s teamCitation11 in their phase B subgroups – both at 22.5 months and 22 months respectively. Regarding the tumor response assessment, before PSM, the TACE + Atez/Bev group experienced an ORR and DCR of 60.9% and 89.1%, respectively. After PSM, these rates elevated to 66.7% and 92.9%, respectively. These figures align closely with the observational results of Wang’s single-arm studyCitation39 (TACE + Atez/Bev regimen, ORR = 61.9%, DCR = 100%) and Xiang’s triple therapy group (TACE + Lenvatinib + PD-1 inhibitors, ORR = 64.3%, DCR = 85.7%). The median PFS for the TACE-alone group was 9.8 months before PSM, and 9.7 months after. These durations are shorter than the median PFS for BCLC B patients in the TAITICs trial who underwent TACE treatment alone (median PFS = 11 months). Furthermore, the median OS was 20.3 months before PSM, and 21.4 months after PSM, shorter than patients only receiving treatment in the TACTICS trial during BCLC B (median OS = 29.3 months). These might be due to a higher number of patients in our study beyond the up-to-7 criteria associated with HCC prognosis.
We also assessed the safety of combination therapy. The adverse reactions in the combination therapy were generally consistent with monotherapy,Citation18 and no unexpected adverse reactions occurred. We have found that hypoalbuminemia is more apt to occur in the combined therapy group, likely due to the repeated episodes of proteinuria caused by multiple courses of Atez/Bev treatment,Citation18 consequently leading to hypoalbuminemia in patients. TACE + Atez/Bev therapy is more likely to cause liver injury compared to TACE monotherapy, which may be associated with immune-related liver injury (irLI) induced by the Atez/Bev treatment. Celsa C et alCitation45 have reported that, compared to patients with other solid tumors, those with HCC undergoing immunotherapy are more susceptible to irLI, and the occurrence of irLI does not necessarily indicate a poorer survival outcome. Joycelyn et alCitation46 have found that patients who experience irLI have better OS (16.2 months vs 4.6 months), PFS (5.5 months vs 1.3 months), ORR (27.8% vs 11.3%), and DCR (67.0% vs 28.2%). Furthermore, in patients with irLI, those treated with systemic steroids showed a trend towards longer PFS compared to those not receiving systemic steroid treatment. In our combination therapy group, a total of 42 patients experienced hepatic injury, of whom four received intravenous methylprednisolone treatment. The prognosis for these patients will necessitate extended follow-up for further clarification.
Our study has some limitations. Firstly, it is retrospective, inherently susceptible to selection and confounding biases. Although we employed PSM to mitigate some known biases, the potential for unknown biases remains. Furthermore, despite our radiological follow-up interval being 6–8 weeks, variations in actual patient follow-up times may still exist, potentially impacting the accuracy of the measured PFS. Secondly, the patient sample size included in the study is relatively small, which could potentially reduce statistical power. Thirdly, the follow-up period is short, requiring a longer follow-up to improve the PFS and OS. Therefore, future prospective studies are needed to further validate the combined treatment’s efficacy.
In conclusion, our findings suggest that the combined treatment of TACE + Atez/Bev demonstrates superior efficacy compared to using TACE alone in managing intermediate-stage liver cancer patients. Moreover, the safety profile of this combined treatment is deemed acceptable, with no significant increase in adverse events reported. This provides a new approach for the combined treatment of intermediate-stage HCC patients.
Abbreviations
AEs, adverse events; BCLC, Barcelona Clinic Liver Cancer; CT, Computed Tomography; CTCAE, Common Terminology Criteria for Adverse Events; DSA, digital subtraction angiography; HAIC, hepatic arterial infusion chemotherapy; HCC, hepatocellular carcinoma; irLI, immune-related liver injury; IPTW, Inverse Probability of Treatment Weighting; mRECIST, modified Response Evaluation Criteria in Solid Tumors; MRI, Magnetic Resonance Imaging; ORR, objective response rate; OS, overall survival; PFS, progression‐free survival; PSM, propensity score matching; TACE, transarterial chemoembolization; TTUP, time to unTACEable progression; VEGF, vascular endothelial growth factor.
Ethical Consideration
The study was approved by the Medical Ethics Committee of the Ningbo No.2 hospital, Eastern Hepatobiliary Hospital, and the First Affiliated Hospital of Wenzhou Medical University (No.: YJ-NBEY-KY-2023-122-01). All procedures were in accordance with the ethical standards of the above three Clinical Research Committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. As patient identities were anonymized, the ethics committees of Ningbo No.2 Hospital, Eastern Hepatobiliary Hospital, and the First Affiliated Hospital of Wenzhou Medical University all waived the requirement of informed consent.
Disclosure
The authors report no conflicts of interest in this work.
Acknowledgments
We would like to thank Professor Su for the English language editing of this manuscript. We also thank Jingna Hu for her contribution to the statistical analysis of the article.
Data Sharing Statement
Data for this study can be reasonably obtained by contacting the corresponding authors.
Additional information
Funding
References
- Forner A, Reig M, Bruix J. Hepatocellular carcinoma. Lancet. 2018;391(10127):1301–1314. doi:10.1016/S0140-6736(18)30010-2
- Fu Z, Li X, Zhong J, et al. Lenvatinib in combination with transarterial chemoembolization for treatment of unresectable hepatocellular carcinoma (uHCC): a retrospective controlled study. Hepatol Int. 2021;15(3):663–675. doi:10.1007/s12072-021-10184-9
- Leowattana W, Leowattana T, Leowattana P. Systemic treatment for unresectable hepatocellular carcinoma. World J Gastroenterol. 2023;29(10):1551–1568. doi:10.3748/wjg.v29.i10.1551
- Galle PR, Forner A, Llovet JM, et al. EASL clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol. 2018;69(1):182–236. doi:10.1016/j.jhep.2018.03.019
- Marrero JA, Kulik LM, Sirlin CB, et al. Diagnosis, staging, and management of Hepatocellular carcinoma: 2018 practice guidance by the American association for the study of liver diseases. Hepatology. 2018;68(2):723–750. doi:10.1002/hep.29913
- Vogel A, Cervantes A, Chau I, et al. Hepatocellular carcinoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2018;29(Suppl 4):iv238–iv255. doi:10.1093/annonc/mdy308
- Omata M, Cheng AL, Kokudo N, et al. Asia-Pacific clinical practice guidelines on the management of hepatocellular carcinoma: a 2017 update. Hepatol Int. 2017;11(4):317–370. doi:10.1007/s12072-017-9799-9
- Bolondi L, Burroughs A, Dufour JF, et al. Heterogeneity of patients with intermediate (BCLC B) hepatocellular carcinoma: proposal for a subclassification to facilitate treatment decisions. Semin Liver Dis. 2012;32(4):348–359. doi:10.1055/s-0032-1329906
- Dufour JF, Bargellini I, De Maria N, De Simone P, Goulis I, Marinho RT. Intermediate hepatocellular carcinoma: current treatments and future perspectives. Ann Oncol. 2013;24(Suppl 2):ii24–29. doi:10.1093/annonc/mdt054
- Reig M, Forner A, Rimola J, et al. BCLC strategy for prognosis prediction and treatment recommendation: the 2022 update. J Hepatol. 2022;76(3):681–693. doi:10.1016/j.jhep.2021.11.018
- Kudo M, Ueshima K, Ikeda M, et al. Final results of TACTICS: a randomized, prospective trial comparing transarterial chemoembolization plus sorafenib to transarterial chemoembolization alone in patients with unresectable hepatocellular carcinoma. Liver Cancer. 2022;11(4):354–367. doi:10.1159/000522547
- Ju S, Zhou C, Hu J, et al. Late combination of transarterial chemoembolization with apatinib and camrelizumab for unresectable hepatocellular carcinoma is superior to early combination. BMC Cancer. 2022;22(1):335. doi:10.1186/s12885-022-09451-1
- Liu J, Li Z, Zhang W, et al. Comprehensive treatment of Trans-Arterial chemoembolization plus lenvatinib followed by camrelizumab for advanced hepatocellular carcinoma patients. Front Pharmacol. 2021;12:709060. doi:10.3389/fphar.2021.709060
- Cai M, Huang W, Huang J, et al. Transarterial chemoembolization combined with Lenvatinib plus PD-1 inhibitor for advanced hepatocellular carcinoma: a retrospective cohort study. Front Immunol. 2022;13:848387. doi:10.3389/fimmu.2022.848387
- Chen S, Wu Z, Shi F, et al. Lenvatinib plus TACE with or without pembrolizumab for the treatment of initially unresectable hepatocellular carcinoma harbouring PD-L1 expression: a retrospective study. J Cancer Res Clin Oncol. 2022;148(8):2115–2125. doi:10.1007/s00432-021-03767-4
- Carmeliet P, Jain RK. Angiogenesis in cancer and other diseases. Nature. 2000;407(6801):249–257. doi:10.1038/35025220
- Llovet JM, De Baere T, Kulik L, et al. Locoregional therapies in the era of molecular and immune treatments for hepatocellular carcinoma. Nat Rev Gastroenterol Hepatol. 2021;18(5):293–313. doi:10.1038/s41575-020-00395-0
- Cheng AL, Qin S, Ikeda M, et al. Updated efficacy and safety data from IMbrave150: atezolizumab plus bevacizumab vs. sorafenib for unresectable hepatocellular carcinoma. J Hepatol. 2022;76(4):862–873. doi:10.1016/j.jhep.2021.11.030
- Lencioni R, Llovet JM. Modified RECIST (mRECIST) assessment for hepatocellular carcinoma. Semin Liver Dis. 2010;30(1):52–60. doi:10.1055/s-0030-1247132
- Finn RS, Qin S, Ikeda M, et al. Atezolizumab plus bevacizumab in unresectable hepatocellular carcinoma. N Engl J Med. 2020;382(20):1894–1905. doi:10.1056/NEJMoa1915745
- Kudo M, Ueshima K, Ikeda M, et al. Randomised, multicentre prospective trial of transarterial chemoembolisation (TACE) plus sorafenib as compared with TACE alone in patients with hepatocellular carcinoma: TACTICS trial. Gut. 2020;69(8):1492–1501. doi:10.1136/gutjnl-2019-318934
- Vitale A, Cabibbo G, Iavarone M, et al. Personalised management of patients with hepatocellular carcinoma: a multiparametric therapeutic hierarchy concept. Lancet Oncol. 2023;24(7):e312–e322. doi:10.1016/S1470-2045(23)00186-9
- Riccardo L, Masatoshi K, Joseph E, et al. EMERALD-1: a Phase 3, randomized, placebo-controlled study of transarterial chemoembolization combined with durvalumab with or without bevacizumab in participants with unresectable hepatocellular carcinoma eligible for embolization. J Clin Oncol. 2024;42(3_suppl):LBA432–LBA432.
- Mizukoshi E, Nakamoto Y, Arai K, et al. Comparative analysis of various tumor-associated antigen-specific t-cell responses in patients with hepatocellular carcinoma. Hepatology. 2011;53(4):1206–1216. doi:10.1002/hep.24149
- Wissniowski TT, Hänsler J, Neureiter D, et al. Activation of tumor-specific T lymphocytes by radio-frequency ablation of the VX2 hepatoma in rabbits. Cancer Res. 2003;63(19):6496–6500.
- Dromi SA, Walsh MP, Herby S, et al. Radiofrequency ablation induces antigen-presenting cell infiltration and amplification of weak tumor-induced immunity. Radiology. 2009;251(1):58–66. doi:10.1148/radiol.2511072175
- Guo J, Wang S, Han Y, Jia Z, Wang R. Effects of transarterial chemoembolization on the immunological function of patients with hepatocellular carcinoma. Oncol Lett. 2021;22(1):554. doi:10.3892/ol.2021.12815
- Petrillo M, Patella F, Pesapane F, et al. Hypoxia and tumor angiogenesis in the era of hepatocellular carcinoma transarterial loco-regional treatments. Future Oncol. 2018;14(28):2957–2967. doi:10.2217/fon-2017-0739
- Abril-Rodriguez G, Ribas A. SnapShot: immune Checkpoint Inhibitors. Cancer Cell. 2017;31(6):848–848.e841. doi:10.1016/j.ccell.2017.05.010
- Wada J, Suzuki H, Fuchino R, et al. The contribution of vascular endothelial growth factor to the induction of regulatory T-cells in malignant effusions. Anticancer Res. 2009;29(3):881–888.
- Terme M, Pernot S, Marcheteau E, et al. VEGFA-VEGFR pathway blockade inhibits tumor-induced regulatory T-cell proliferation in colorectal cancer. Cancer Res. 2013;73(2):539–549. doi:10.1158/0008-5472.CAN-12-2325
- Gabrilovich DI, Chen HL, Girgis KR, et al. Production of vascular endothelial growth factor by human tumors inhibits the functional maturation of dendritic cells. Nature Med. 1996;2(10):1096–1103. doi:10.1038/nm1096-1096
- Huinen ZR, Huijbers EJM, van Beijnum JR, Nowak-Sliwinska P, Griffioen AW. Anti-angiogenic agents - overcoming tumour endothelial cell anergy and improving immunotherapy outcomes. Nat Rev Clin Oncol. 2021;18(8):527–540. doi:10.1038/s41571-021-00496-y
- Gavalas NG, Tsiatas M, Tsitsilonis O, et al. VEGF directly suppresses activation of T cells from ascites secondary to ovarian cancer via VEGF receptor type 2. Br. J. Cancer. 2012;107(11):1869–1875. doi:10.1038/bjc.2012.468
- Ohm JE, Gabrilovich DI, Sempowski GD, et al. VEGF inhibits T-cell development and may contribute to tumor-induced immune suppression. Blood. 2003;101(12):4878–4886. doi:10.1182/blood-2002-07-1956
- Voron T, Colussi O, Marcheteau E, et al. VEGF-A modulates expression of inhibitory checkpoints on CD8+ T cells in tumors. J Exp Med. 2015;212(2):139–148. doi:10.1084/jem.20140559
- Llovet JM, Kelley RK, Villanueva A, et al. Hepatocellular carcinoma. Nat Rev Dis Primers. 2021;7(1):6. doi:10.1038/s41572-020-00240-3
- Zhu H-D, H-L L, Huang M-S, et al. Transarterial chemoembolization with PD-(L)1 inhibitors plus molecular targeted therapies for hepatocellular carcinoma (CHANCE001). Signal Transduct Target Ther. 2023;8(1):58. doi:10.1038/s41392-022-01235-0
- Wang K, Zhu H, Yu H, et al. Early experience of TACE combined with Atezolizumab plus Bevacizumab for patients with intermediate-stage Hepatocellular carcinoma beyond up-to-seven criteria: a multicenter, single-arm study. J Oncol. 2023;2023:6353047. doi:10.1155/2023/6353047
- Lencioni R, Llovet JM, Han G, et al. Sorafenib or placebo plus TACE with doxorubicin-eluting beads for intermediate stage HCC: the SPACE trial. J Hepatol. 2016;64(5):1090–1098. doi:10.1016/j.jhep.2016.01.012
- Hidaka H, Izumi N, Aramaki T, et al. Subgroup analysis of efficacy and safety of orantinib in combination with TACE in Japanese HCC patients in a randomized Phase III trial (ORIENTAL). Med Oncol. 2019;36(6):52. doi:10.1007/s12032-019-1272-2
- Labeur TA, Takkenberg RB, Klumpen HJ, van Delden OM. Reason of discontinuation after transarterial chemoembolization influences survival in patients with hepatocellular carcinoma. Cardiovasc Intervent Radiol. 2019;42(2):230–238. doi:10.1007/s00270-018-2118-6
- Kudo M. Proposal of primary endpoints for TACE combination trials with systemic therapy: lessons learned from 5 negative trials and the positive TACTICS trial. Liver Cancer. 2018;7(3):225–234. doi:10.1159/000492535
- Xiang YJ, Wang K, Yu HM, et al. Transarterial chemoembolization plus a PD‐1 inhibitor with or without lenvatinib for intermediate‐stage hepatocellular carcinoma. Hepatol Res. 2022;52(8):721–729. doi:10.1111/hepr.13773
- Celsa C, Cabibbo G, Enea M, et al. Are radiological endpoints surrogate outcomes of overall survival in hepatocellular carcinoma treated with transarterial chemoembolization? Liver Int. 2021;41(5):1105–1116. doi:10.1111/liv.14822
- Kyy N, Tan SH, Tan JJE, et al. Impact of immune-related adverse events on efficacy of immune checkpoint inhibitors in patients with advanced hepatocellular carcinoma. Liver Cancer. 2022;11(1):9–21. doi:10.1159/000518619