
Abstract
Hepatocellular carcinoma (HCC) is the most common primary liver malignancy and is a leading cause of cancer-related death worldwide. In the United States, HCC is the ninth leading cause of cancer deaths. Despite advances in prevention techniques, screening, and new technologies in both diagnosis and treatment, incidence and mortality continue to rise. Cirrhosis remains the most important risk factor for the development of HCC regardless of etiology. Hepatitis B and C are independent risk factors for the development of cirrhosis. Alcohol consumption remains an important additional risk factor in the United States as alcohol abuse is five times higher than hepatitis C. Diagnosis is confirmed without pathologic confirmation. Screening includes both radiologic tests, such as ultrasound, computerized tomography, and magnetic resonance imaging, and serological markers such as α-fetoprotein at 6-month intervals. Multiple treatment modalities exist; however, only orthotopic liver transplantation (OLT) or surgical resection is curative. OLT is available for patients who meet or are downstaged into the Milan or University of San Francisco criteria. Additional treatment modalities include transarterial chemoembolization, radiofrequency ablation, microwave ablation, percutaneous ethanol injection, cryoablation, radiation therapy, systemic chemotherapy, and molecularly targeted therapies. Selection of a treatment modality is based on tumor size, location, extrahepatic spread, and underlying liver function. HCC is an aggressive cancer that occurs in the setting of cirrhosis and commonly presents in advanced stages. HCC can be prevented if there are appropriate measures taken, including hepatitis B virus vaccination, universal screening of blood products, use of safe injection practices, treatment and education of alcoholics and intravenous drug users, and initiation of antiviral therapy. Continued improvement in both surgical and nonsurgical approaches has demonstrated significant benefits in overall survival. While OLT remains the only curative surgical procedure, the shortage of available organs precludes this therapy for many patients with HCC.
Introduction
Hepatocellular carcinoma (HCC) is the most common primary liver malignancy and is a leading cause of cancer-related death worldwide. In the United States, HCC is the ninth leading cause of cancer deaths.Citation1 A total of 30,640 new liver and intrahepatic bile duct cancers were estimated to occur in 2013 in addition to 21,670 deaths.Citation2 HCC occurred more often in males than females (2.4:1), with a higher incidence in Eastern and Southern Asia, Middle and Western Africa, Melanesia, and Micronesia/Polynesia.Citation3 The age-adjusted incidence of liver cancer has risen from 1.6 per 100,000 individuals to 4.6 per 100,000 individuals among American Indians and Alaskan Natives followed by blacks, Whites, and Hispanics.Citation4 There are pockets in the United States where certain ethnic groups have significantly increased incidence of HCC. Importantly, the incidence of HCC will continue to escalate as hepatitis C reaches its maturity and as nonalcoholic steatohepatitis (NASH) and obesity become more prevalent in the United States.
Risk factors
Chronic liver disease and cirrhosis remain the most important risk factors for the development of HCC of which viral hepatitis and excessive alcohol intake are the leading risk factors worldwide.
Chronic viral hepatitis can lead to cirrhosis and/or HCC. Hepatitis B and C are the most common causes of chronic hepatitis in the world. Hepatitis B virus (HBV) is a double-stranded, circular DNA molecule with eight genotypes (A to H). Genotypes A and D are more common in Europe and the Middle East, while genotypes B and C are more common in Asia.Citation5 Hepatitis B is transmitted via contaminated blood transfusions, intravenous injections, and sexual contact. Vertical transmission from mother to fetus is the leading cause for HBV infection worldwide. Five percent of the world’s population is infected with hepatitis B.Citation6
Several epidemiological studies have demonstrated significant hepatocarcinogenicity with chronic HBV infection.Citation7 Hepatitis B carriers have a 10%–25% lifetime risk of developing HCC. Unlike other causes of chronic hepatitis, HBV is unique in that HCC can develop without evidence of cirrhosis.Citation2 Genotype C has been associated with a higher risk of HCC than genotypes A, B, and D.Citation8 Active infection with HBV carries an independent risk of HCC with HBV DNA levels >105/mL viral copies associated with a 2.5–3 times increased risk of developing HCC in 8–10 years follow-up.Citation9 Hepatitis B surface antigen (HBsAg) is not the only hematological marker that carries a significant risk for development of HCC. Patients with positive hepatitis B core antibody (anti-HBc) who are HBsAg-negative also remain at risk for development of HCC. The hepatocarcinogenicity of HBV can be significantly reduced with antiviral treatment for hepatitis B. Suppression of the virus can result in a significant 5-year reduction of the incidence of HCC from 13.7% (controls) to 3.7%, with the greatest reduction occurring in cirrhotic patients.Citation10 The use of HBV vaccination has resulted in significant declines in the incidence of HCC from HBV.Citation11 The East Asian neonatal vaccination program is estimated to result in a 70%–85% decrease in the incidence of hepatitis B-related HCC.Citation12 Despite perinatal immunization, 5%–10% of infants remain at risk of acquiring hepatitis B infection. The use of nucleoside analogs in treating chronic hepatitis B mothers in their third trimester of pregnancy has demonstrated superiority to vaccination alone in preventing neonatal transmission.Citation13,Citation14
Hepatitis C virus (HCV) is a small, single-stranded RNA virus, which exhibits high genetic variability.Citation15 There are six different genotypes of HCV isolated. Genotypes I, II, and III are predominant in the Western countries and the Far East, while type IV is predominant in the Middle East. The highest rates of chronic hepatitis C infection occur in Egypt (18%), with lower rates occur in Europe (0.5%–2.5%), the United States (1.8%), and Canada (0.8%).Citation16 Once infected with HCV, 80% of patients progress to chronic hepatitis, with ~20% developing cirrhosis.Citation17 In hepatitis C, the development of HCC occurs almost exclusively in the liver with established cirrhosis; however, in the HALT-C trial, 8% of HCC occurred in patients with only advanced fibrosis.Citation18 Dual infection with HBV and HCV in a cirrhotic patient increases the risk of HCC with an odds ratio (OR) of 165 compared to 17 for hepatitis C and 23 for hepatitis B alone.Citation2,Citation19 A synergistic effect with alcohol increases the incidence of HCC between 1.7- and 2.9-fold when compared to HCV–HCC alone.Citation20,Citation21 The risk of HCC is reduced significantly in patients who obtained a sustained viral response after treatment of HCV with a 54% reduction in all-cause mortality.Citation22 While advances in medications recently have made treating HCV easier, vaccinations against the virus remain elusive.
Alcohol consumption remains an important risk factor for the development of HCC.Citation23 The relationship between alcohol and liver disease correlates with the amount of alcohol consumed over a lifetime, with heavy alcohol use rather than social drinking being the main risk of HCC.Citation24 The prevalence rate of alcohol abuse in the United States is five times higher than that of hepatitis C.Citation25 Alcohol abuse accounts for 40%–50% of all HCC cases in Europe.Citation26 Studies in Europe reported an increase in the relative risk of developing liver disease above 7–13 drinks per week in women and 14–27 drinks per week in men.Citation25,Citation27 In the United States, studies showed that the risk of liver cancer is increased two-to fourfold among persons drinking more than 60 g/d of ethanol.Citation28 A meta-analysis of 19 prospective studies showed that consumption of three or more drinks per day resulted in a 16% increase risk of liver cancer and consumption of six or more drinks per day resulted in a 22% increase risk.Citation29
Diabetes and nonalcoholic fatty liver disease
Sixty percent of patients older than 50 years with diabetes or obesity are thought to have NASH with advanced fibrosis.Citation30 Chronic medical conditions such as diabetes mellitus and obesity increase the risk of HCC. Diabetes mellitus directly affects the liver because of the essential role the liver plays in glucose metabolism. It can lead to chronic hepatitis, fatty liver, liver failure, and cirrhosis. Diabetes is an independent risk factor for HCC.Citation19,Citation31 Patients with diabetes have between a 1.8- and 4-fold increased risk of HCC. When compared to HCV, NASH-related HCC liver transplants increased by nearly four times in the decade from 2002 to 2012.Citation32 In 2006, El-Serag et alCitation33 reviewed several cohort and case–control studies showing that diabetes mellitus is significantly associated with HCC. Hyperinsulinemia has been associated with a threefold increased risk of HCC. It is believed that the pleotropic effects of insulin that regulate the anti-inflammatory cascade and other pathways inducing cellular proliferation play a role in carcinogenesis. Insulin-like growth factor and insulin receptor substrate-1 promote cellular proliferation and inhibit apoptosis, respectively.Citation34,Citation35 It is well-known that obesity is associated with many hepatobiliary diseases, including nonalcoholic fatty liver disease (NAFLD), steatosis, and cryptogenic cirrhosis all of which can lead to the development of HCC.Citation36,Citation37 Obesity itself increases the risk of HCC to 1.5- to 4-fold. The relative risk of HCC is 117% for overweight subjects and 189% for obese patients.Citation38 The majority of HCC-NAFLD occurs in men. Compared to women, men developed HCC with less fibrosis and cirrhosis.Citation39 The mean age of presentation is 70 years. Up to 50% of cases of NAFLD-related HCC may occur in the absence of cirrhosis.Citation29 These tumors tend to have lower α-fetoprotein (AFP) synthesis but are more likely to have elevated des-γ-carboxy prothrombin (DCP) than HCV-related HCC.Citation40,Citation41
Other predisposing conditions
Sex may play a role in the development of HCC. HCC occurs more often in males, with a ratio of 2:1–4:1; however, this may not be due to sex alone.Citation42 Males are more likely to be infected with viral hepatitis, consume greater quantities of alcohol, smoke cigarettes, and have a higher body mass index than women. It may be the higher testosterone levels that account for the higher incidence in males. It is known that high testosterone levels have been linked to HCC in hepatitis B carriers and to advanced hepatic fibrosis in males with chronic hepatitis C infection.Citation43,Citation44 Elevated testosterone or intake of anabolic steroids has been associated with an increased incidence of HCC and liver adenomas.
Aflatoxin produced by Aspergillus species (molds) found on grains, corn, peanuts, or soybeans stored in warm humid conditions is a potent hepatocarcinogen. The risk of HCC with aflatoxin is dependent on the dose and duration of exposure. Aflatoxin exposure is more prevalent in rural United States. Aflatoxin exerts a synergistic effect on hepatitis B- and C-induced liver cancer, the risk being 30 times greater with chronic hepatitis B plus aflatoxin exposure than with aflatoxin exposure alone.Citation45 The most potent aflatoxin, AFB1, when removed from the environment has resulted in a reduction of the incidence of HCC.Citation46
Metabolic and genetic diseases associated with HCC include hemochromatosis, Wilson’s disease, α-1 antitrypsin disease, tyrosinemia, glycogen-storage disease types I and II, and porphyrias.
The risk of HCC with hereditary hemochromatosis is estimated to be between 100- and 200-fold.Citation47 Other iron overload states such as thalassemia have not only been associated with HCC but also have a high prevalence of HCV that may contribute to the increased risk of primary liver cancer. South African blacks who consume beer brewed in nongalvanized steel drums have increased iron stores leading to an increase in the risk of HCC 10 times that of people with normal iron stores.Citation48,Citation49
Other risk factors may include smoking. Cigarette smoking is associated with a significant increase in the development of HCC. A recent meta-analysis that reviewed the association between smoking and liver cancer demonstrated an OR of 1.6 (95% confidence interval [CI], 1.3–1.9) for current smokers and 1.5 (95% CI, 1.1–2.1) for former smokers. Studies investigating the use of oral contraceptive pills and the risk for development of HCC have previously been inconclusive; however, a recent review of six studies showed a significant increase in HCC risk with a longer duration (>5 years) of exposure to oral contraceptives.Citation50
Screening
Surveillance () for HCC should have the goal of decreasing mortality and improving patient outcomes. Studies have found a survival benefit for early screening of patients for HCC.Citation51,Citation52 Patients who are identified early consequently have multiple treatment options leading to improved outcomes. Defining the target population should be a priority in today’s rising health care costs, as surveillance for the general population is not recommended. An intervention (screening modality) is considered clinically effective if it provides at least 100 days increase in longevity. Cost-effectiveness would be defined as an intervention costing <$50,000/yr of life gained.Citation5 Screening intervals for HCC are based on the average tumor doubling time of 3–5 months and a cost-effective threshold of an expected annual incidence exceeding 1.5% in cirrhosis and 0.2% in noncirrhosis hepatitis B patients.Citation53 Given these criteria, any patient with cirrhosis should be screened for HCC, although screening in autoimmune hepatitis cirrhosis and primary biliary cirrhosis may be of less value. Another exception to this rule may be patients with advanced/decompensated cirrhosis who are not transplant candidates. Their life expectancy is too short to receive any survival benefit from surveillance.Citation54
Table 1 Screening guidelines for HCC
Persistent infection with HBV, in both noncirrhotic and cirrhotic patients, is a major risk factor for developing HCC. HBV carriers have a 223-fold higher risk of developing HCC than noncarriers.Citation55 The risk of HCC in Asian males exceeds the threshold for screening starting at the age of 40 years. HCC in Caucasians with hepatitis B is more related to virus inflammatory activity in noncirrhotic livers.Citation56 Active disease is defined as an elevated alanine transaminase (ALT) and/or a high viral load (>20,000 IU/mL). Screening for noncirrhotic HBV in Caucasian males with active disease should start at 40 years of age, while screening for Asian and Caucasian females should start at 50 years of age. African noncirrhotic hepatitis B carriers, in particular sub-Sahara Africans, have the highest incidence of HCC occurring particularly at a younger age.Citation57 Screening in these individuals should begin at the time of diagnosis or upon reaching the age of 20. Hepatitis B carriers with a family history of HCC are also at increased risk. The risk increases with age (23% with HCC at 70 years vs 8.9% without family history) and the number of family members affected (risk 5.6 times with >2 family members).Citation58 The age at which to start surveillance, however, has not been well-defined by guidelines. At our institution, we begin surveillance for males at age 40 and females at age 50 or 10 years before the index cancer developed in a family member.
Screening modalities
Modalities available for HCC screening include both radiographic tests and serological markers. Radiological tests commonly used for surveillance include ultrasonography (US), multiphase computerized tomography (CT), and magnetic resonance imaging (MRI) with contrast. US has historically been utilized to identify intrahepatic lesions since the early 1980s.Citation59 Sensitivity of US imaging is variable, ranging from 35% to 84%, and is operator and equipment dependent; however, studies have reported a specificity >90% when used for screening.Citation60,Citation61 Small HCC nodules ≤2 cm represented 85% of the lesions that failed to be detected by US.Citation62 Furthermore, central obesity hampers ultrasound’s ability to detect small lesions.Citation63 HCC lesions exhibit increased arterialization as well as decreased presence of contrast agents during the portal phase of imaging (washout) on both CT and MRI scans.Citation64 Tumors ≥2 cm are detected by CT and MRI at 90% sensitivity, while sensitivity detection of tumors between 1 and 2 cm is 65% and 80%–92% and that for tumors <1 cm is 10% and 34%–71%, respectively.Citation65 CT and MRI is preferred in patients who have equivocal results utilizing US as their initial modality.
AFP’s main function is the regulation of fatty acids in both fetal and proliferating adult liver cells.Citation55 Since 1968, AFP has been used as a serum marker for the detection of HCC.Citation32 Several studies have evaluated the sensitivity and specificity of utilizing AFP with ranges of 21%–64% and 82%–93%, respectively.Citation65–Citation69 One major disadvantage is that AFP levels can be falsely raised in patients who have active hepatitis but no evidence of HCC. The upper limit of normal that is often adopted is 20 ng/mL because AFP levels in healthy individuals rarely exceed this level. In chronic hepatitis C patients without HCC, AFP can be >20 ng/mL in 16% of patients.Citation70 Furthermore, the sensitivity of AFP >20 ng/mL may have racial differences, being found to be 42.9% among blacks and 60% among nonblacks.Citation71 AFP sensitivity is lower with small HCC lesions. It can be elevated in acute hepatitis, cirrhosis, colitis, germ cell tumors, and intrahepatic cholangiocarcinoma. AFP levels above 400 ng/mL can be considered definitive in diagnosing HCC, but sensitivity is lower at this higher cutoff value.Citation55 Lin et alCitation72 demonstrated that surveillance with AFP and ultrasound was cost-effective regardless of the incidence of HCC.
In 2011, American Association for the Study of Liver Diseases (AASLD) published updates to its guidelines for surveillance of HCC. Cost-effectiveness is achieved if the expected HCC risk exceeds 1.5% per year in patients with HCV and 0.2% per year in patients with HBV. Ultrasound is the most cost-effective modality when performed at 6-month intervals. Some studies show that 6-month ultrasound with AFP exceeds cost-effectiveness, while biannual AFP/annual contrast CT exceeds the threshold by $1,750.Citation72 AFP lacks adequate sensitivity and specificity for surveillance, and therefore surveillance has to be based on US examination every 6 months.Citation53
While standard AFP levels are of variable benefit in identifying patients with HCC, other assays are available. Lens culinaris agglutinin-reactive fraction of α-fetoprotein (AFP-L3) expressed as a percentage of AFP has been found to be elevated in patients with HCC. It is highly specific for HCC when AFP levels are >20 ng/mL. A level >10% may identify patients with increased risk of developing HCC. AFP-L3 is associated with a more aggressive tumor, shorter doubling time, infiltrative growth pattern, vascular invasion, and intrahepatic metastasis.Citation73
DCP is produced by malignant hepatocytes from an acquired posttranslational defect in vitamin K-dependent carboxylase system. The specificity of the DCP is 91% compared to 70% for AFP; however, sensitivity is low at 41%.Citation74 DCP normalizes with successful tumor resection. DCP levels >125 mAU/mL is sensitive and specific for differentiating HCC from chronic hepatitis and cirrhosis.Citation75 The highest accuracy for diagnosing HCC occurs when all three markers with appropriate cutoff values are used together. A DCP >40 mAU/mL + AFP >20 ng/mL and AFP-L3 >10% yield a sensitivity of 82.2% with a specificity of 82.4%.Citation76
Diagnosis
To obtain the best treatment result for HCC, early diagnosis is the key. Chronic hepatitis leads to the development of cirrhosis. Cirrhotic livers exhibit regenerative nodules, which result from increased proliferation of hepatocytes. Differentiation between these regenerative nodules and HCC can vary based on the size of the nodules. Nodules <1 cm () detected via US that cannot be defined should be followed up with a repeat US in 3–4 months. Nodules >1 cm detected via US should have further radiologic investigation including either contrast-enhanced triple or quadriphasic CT or MRI. The diagnosis of HCC is based on the contrast enhancement in the arterial phase (wash-in) followed by disappearance of the contrast in the venous phase (washout) ().Citation77 A recent meta-analysis of the diagnostic performance of CT and MRI for evaluating HCC has demonstrated that MRI has a higher per-lesion sensitivity than multidetector CT and should be the preferred imaging modality for the diagnosis of HCC in patients with chronic liver disease.Citation78 If the first radiologic test is equivocal, then confirmation with a different technique is recommended. If the diagnosis still remains uncertain, a serum AFP level >400 ng/mL has a high positive predictive value.Citation79 Percutaneous biopsy should be limited to those nodules that are radiologically nontypical on CT or MRI for HCC.Citation80
Figure 1 TACE.
Abbreviations: TACE, transarterial chemoembolization; MRI, magnetic resonance imaging.
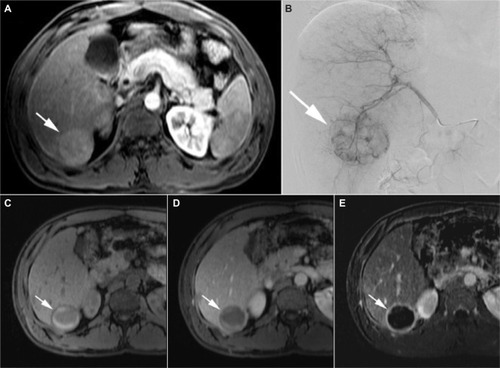
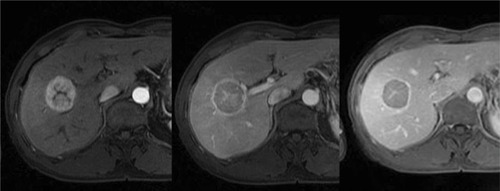
Figure 2 Typical HCC shows arterial phase hypervascularity with washout of contrast on portal venous and equilibrium phase.
Abbreviation: HCC, hepatocellular carcinoma.
Staging
Stratification of patients diagnosed with HCC into groups is the primary aim of staging systems. Staging systems will assist in organizing patients into groups based on prognosis and can guide clinicians in a choice of therapy, aid patient counseling, and facilitate patient selection and randomization for research protocols.Citation81 Currently, there are three clinical and four pathologic staging systems. Pathologic staging systems include the Liver Cancer Study Group of Japan, Japanese Integrated, Chinese University Prognostic Index, and American Joint Committee on Cancer/International Union Against Cancer Staging System. Clinical staging systems include the Okuda Staging System, Cancer of the Liver Italian Program score, and the Barcelona Clinic Liver Cancer Staging System (BCLC). The BCLC staging system is widely accepted in clinical practice and is also at the forefront of many clinical trials used to establish the effectiveness of new HCC drugs.Citation53 The BCLC staging system has become the de facto staging system that is used. In the United States, there are additional staging systems commonly used, including the Model for End-Stage Liver Disease (MELD) score, the tumor–node–metastasis (TNM) staging system, or the simplified TNM staging system.Citation82–Citation85 In 2010, the AASLD published their recommendations regarding staging systems for HCC. Staging systems should best assess the prognosis of HCC in that a staging system should take into account tumor stage, liver function, and physical status. BCLC is the only system that takes into account all of these factors.Citation5
CT scan of the chest, abdomen, and pelvis in addition to bone scan is vital to look for secondary disease and staging. Tumor characteristics such as size, maximum diameter, and number of lesions, location of tumors, vascular invasion, and any extrahepatic disease should be documented.
Treatment
Unfortunately, the diagnosis of HCC is too often made with advanced disease when patients have become symptomatic and have some degree of liver impairment. At this late stage, there is virtually no effective treatment that would improve survival. In addition, the morbidity associated with therapy is unacceptably high. The unfortunate truth is that many patients are not properly screened. In a study looking at Marketscan claims database, over 700,000 patients with at least one claim for NAFLD/NASH/HCV over one-quarter of those diagnosed with HCC had no knowledge of liver disease prior to their diagnosis.Citation86 HCC screening was regularly performed on 21.1% of NASH and 22.3% of hepatitis C patients in this study. Even when patients are followed by expert hepatologists at academic centers, up to one-third of the patients had inconsistent HCC surveillance.Citation87 With proper screening and vigilance, many patients can and should be diagnosed with early disease and preserved liver function. Currently, there are several treatment options, both surgical and nonsurgical, that can have a positive impact on survival.Citation88 The best outcomes are achieved when patients are carefully selected for each treatment option. Regardless of the treatment approach, patients with HCC require a multidisciplinary approach to care to ensure optimal outcome. The multidisciplinary team typically consists of a hepatologist, a radiologist, a pathologist, a medical oncologist, an interventional radiologist, a transplant surgeon, and a hepatobiliary surgeon. Each specialty will have unique contributions to ensure optimal long-term outcomes for patients with HCC.
Surgical approaches
Resection
Surgical resection is the accepted treatment of choice for noncirrhotic patients and offers the best curative rate with a 5-year survival of 41%–74%.Citation89 The resectability of the tumor is dependent on the tumor size, location, underlying liver function, and whether or not the remaining liver volume will allow for resection without drastically increasing postresection morbidity and mortality. Resection is considered the first-line treatment as long as R0 resection can be accomplished. The candidates for this therapy are patients with a solitary tumor confined to the liver, no radiologic evidence of vascular invasion, and well-maintained liver function.Citation90,Citation91 Optimum candidate selection is crucial to limit surgical morbidity and mortality. In patients with normal synthetic function, the size of the tumor does not necessarily affect the outcome when residual volume (volume of remaining liver) is adequate and technical aspects of the surgery are achievable.Citation92 Operative mortality is affected by the presence (10%) or absence (5%) of cirrhosis.Citation93 Over the previous decades, Child–Pugh classification has been utilized in the guidance of resection candidates. However, Child–Pugh classification is far from accurate in predicting postoperative liver failure and some authors argue that Child–Pugh A patients already have functional liver impairment, significant portal hypertension, and minor fluid retention necessitating diuretic use.Citation94 Utilizing the MELD, a score of ≤ 8 has been shown to have no mortality as compared to a perioperative mortality of 29% for a score of >9.Citation95 Many Japanese groups rely on the indocyanine green retention test to assess whether surgery is possible. The feasibility of surgery or degree of possible liver resection can be determined by the degree of indocyanine dye retention. In the United States and Europe, selection of ideal candidates for resection is usually based on the assessment of portal hypertension, which is assessed by cannulation of the hepatic vein and calculation of the hepatic portal venous gradient. Significant portal hypertension is evident when the portocaval gradient is >10 mmHg. A significant gradient can also be clinically surmised with evidence of gastroesophageal varices, splenomegaly, and a platelet count <1×1011/L that leads to an increase in postoperative morbidity and mortality.Citation96
Perioperative portal vein embolization (PVE) is a technique utilized to cause hypertrophy of the anticipated residual liver remnant, thus permitting a more extensive liver resection. When PVE is performed, an overall increase in the liver volume of 10%–12% can be achieved.Citation97 Perioperative PVE has less major complications (10% vs 36%) and 90-day mortality (0% vs 18%) compared to patients who have had major resection without PVE.Citation98
Postresection 5-year survival rates range from 41% to 74% for patients who have a solitary tumor confined to the liver without radiologic evidence of vascular invasion and preserved liver function.Citation17,Citation99,Citation100 In contrast, patients who exhibit significant portal hypertension will develop postoperative decompensation with a 5-year survival rate of <50%. Finally, survival in patients who exhibit both adverse predictors (portal hypertension and elevated bilirubin) and multifocal disease is <30% at 5 years.Citation101,Citation102 Cirrhotic patients have a perioperative mortality rate between 3% and 8% after resection, and a 5-year survival rate ranging from 30% to 50%.Citation96 Despite increasing overall survival in patients undergoing hepatic resection (HR) to treat HCC, the disease-free survival has not changed.Citation103 Recurrence rates may be as high as 70% after 5 years. Predictors of early recurrence include AFP levels >2,000 ng/dL, nonanatomic resection, micro- or macrovascular invasion, positive resection margins, and poorly differentiated tumors.Citation104 While de novo tumor development can occur after resection, the majority of HCC recurrences occurs within 1–2 years and is believed to be a result of dissemination or micrometastasis from the primary tumor and not inadequate surgical resection.Citation2 Contraindications to resection are the presence of extrahepatic metastasis or invasion of the main portal trunk by the tumor. Generally, neoplastic invasion of the portal vein leading to thrombosis is a poor prognostic indicator; however, in certain cases, hemihepatectomy can be feasible, especially when thrombosis of the main branch of the portal vein resulted in the hypertrophy of the contralateral hemiliver.Citation105
In comparison to traditional open surgery, laparoscopic liver resection is safeCitation106,Citation107 and effective in cirrhotic patients and now plays a key role in the treatment of HCC. Resection is also the primary treatment for advanced tumors and can be used as an alternative or a bridge to liver transplantation.Citation108–Citation111 Technical feasibility is the only limiting factor when offering laparoscopic vs open resection. Two criteria have been proposed to assist in the selection of appropriate candidates for surgery: size and location of the tumor and liver function.Citation112
Liver transplantation
Orthotopic liver transplantation (OLT) is the best curative option for patients with decompensated cirrhosis, and HCC is the only solid cancer that can be treated with transplantation. Mazzaferro et alCitation113 published a landmark study with <50 patients who were transplanted for HCC with specific criteria, which became known as the Milan criteria. These specific criteria included single HCC tumors <5 cm or three tumors all ≤3 cm each and demonstrated a 4-year survival rate of 75%. A recent systemic review of 90 studies that followed 17,780 patients over a 15-year period identified the Milan criteria as an independent prognostic factor of outcome after OLT.Citation114
Expansion of the Milan criteria, particularly by liberating the restrictions on tumor size, has also been studied. The University of California San Francisco (UCSF) criteria, which includes 1) a single lesion ≤6.5 cm, or 2) three or fewer nodules with the largest lesion ≤4.5 cm and with a total diameter ≤8 cm, have been studied both retrospectively and prospectively and have shown survival and recurrence rates equal to those patients using the Milan Criteria.Citation49 The 1- and 5-year survival rates were 90% and 75%, respectively.Citation115 Both the Milan and UCSF criteria consider the number and size of the tumor regardless of tumor biology. The University of Toronto developed a protocol for biopsying large tumors up to 10 cm, and poorly differentiated tumors were excluded. These patients were treated aggressively prior to transplantation with ablative therapies, with survival being similar in both the Milan criteria and expanded criteria patients.Citation116
Locoregional therapies have been used to downsize patients with HCC exceeding current transplant criteria with the goal to decrease the tumor burden in order to meet transplant criteria.Citation117–Citation119 Yao et alCitation119 published a downstaging protocol consisting of transarterial chemoembolization (TACE) and/or radiofrequency ablation (RFA) and demonstrated survival rates of 96.2% at 1 year and 92.1% at 4 years among patients who received transplantation. In compensated livers, locoregional therapy is utilized to downsize the tumor to an acceptable size and within standard criteria. Posttransplant survival data are comparable in patients who underwent downsizing with those within conventional criteria.Citation118 Ablative therapies can also be used as bridging therapies for transplantation, deceleration of tumor progression, minimization of dropout, and improvement of posttransplant survival.Citation8 Long waiting time, and a shortage in available organs, is one of the major disadvantages of OLT as a treatment option in HCC. Under the current United Network of Organ Sharing policy, patients who are diagnosed with HCC and are within the Milan criteria receive a MELD score of 22. This starting score increases in a stepwise fashion every 3 months after the results of repeated imaging (CT or MRI) reconfirm that criteria is still met.Citation120 This can result in a waiting time of >2 years in certain areas of the country. An alternative to deceased donor liver transplantation is living donor liver transplantation; however, the mortality to the donor is approximately 0.3% and life-threatening morbidity is 2%. Because of the risk to the donor, living donor liver transplantation should be restricted to centers of excellence.Citation121
Nonsurgical approaches
Transarterial chemoembolization
The most commonly used initial treatment for locoregional HCC as well as for downstaging tumors that exceed criteria is TACE.Citation122 TACE can also be considered prior to HR and RFA as neoadjuvant therapy to either reduce tumor volume or even target micrometastasis.Citation123 The rationale for using TACE is the neoangiogenic properties of HCC and its mechanism of action on the hepatic arterial supply of the tumor. During its initial development, the tumor derives its blood flow from the portal system. As the tumor increases in size, the blood supply becomes arterialized, so even a well-differentiated HCC is mostly dependent on hepatic arterial supply. This tumor characteristic provides the pathologic basis for the radiologic features used to diagnose HCC. Embolization of the hepatic artery branch leads to selective tumor hypoxia and eventually tumor necrosis. This is accomplished by a significant reduction in arterial blood flow through the use of image-guided catheter-based infusion of particles.Citation124 Potential agents including polyvinyl alcohol beads, alcohol, starch microspheres, metallic coils, autologous blood clots, and gelfoam have all been used for embolization.Citation5 Prior to arterial embolization, a chemotherapeutic agent is injected. Several chemotherapeutic agents have been historically used, including doxorubicin, cisplatin, mitomycin, and epirubicin.Citation2 In addition, doxorubicin-eluding beads have recently become an alternative to traditional TACE. Drug-eluding beads are considered an improvement in both treatment response rates and tumor necrosis compared to traditional TACE.Citation125 Contraindications for TACE are decompensating cirrhosis (Child–Pugh B), massive tumor with extensive replacement of both lobes, severely reduced portal flow (portal vein occlusion or hepatofugal blood flow), and a creatinine clearance of <30 mL/min.Citation126 Llovet et alCitation127 found that survival probabilities for TACE were 82% and 63% for 1 and 2 years, respectively, for unresectable HCC. The response to TACE is an independent predictor of survival. Additional studies have shown an improvement in survival in TACE-treated patients in the range of 20%–60% at 2 years.Citation128 Morbidity with embolization is relatively low (<5%), and common complications include abdominal pain, nausea, ileus, and fever, which are consistent with postembolization syndrome.Citation129 Historically, portal vein tumor thrombosis has been considered a contraindication to the performance of TACE therapy. This interruption of hepatic arterial blood flow which can lead to significant hepatic necrosis when combined with a portal vein occlusion from tumor thrombus which already compromised blood flow to the affected area of the liver. Several prospective and reactive retrospective studies have shown that TACE can improve overall survival in Child–Pugh’s A cirrhotic HCC patients with portal vein tumor thrombosis. Furthermore, the combination of TACE and sorafenib may have synergistic value.Citation130
Transartetial radiation
Transartetial radioembolization is a form of catheter-directed internal radiation that delivers small microspheres with radioisotopes directly into the tumor. Yttrium-90 (Y-90) microspheres or iodine-131-labeled lipiodolCitation127 are administered in a procedure similar to TACE. This procedure has been shown to be safe and effective in cirrhotic patients with HCC.Citation131,Citation132 One major advantage of Y-90 over TACE is that it is indicated in the case of portal vein neoplastic thrombosis, while TACE traditionally has been considered a contraindication.Citation133 The side effects are usually well tolerated.Citation134 The most common side effects include fatigue, nausea and vomiting, and abdominal pain. Postembolization syndrome (fever, unremitting nausea, general malaise, loss of appetite, and abdominal pain) is seen less frequently with TACE. A pretreatment evaluation that often includes an arteriogram, superior mesenteric angiogram, and celiac trunk angiogram is necessary to evaluate for the presence of arterioportal shunting. Coil embolization of these colateral vessels may be necessary to decrease unintended deposition of microspheres outside the targeted area. Vessels most often embolized include the inferior esophageal, left inferior phrenic, accessory left gastric, supraduodenal, and retroduodenal arteries. Y-90 is contraindicated in patients with hepatopulmonary shunting, which can lead to extremely high levels of pulmonary radiation exposure and the development of radiation pneumonitis. The reported rate of complete tumor necrosis in patients with tumors <3 cm was 90%.Citation91 The 2010 AASLD clinical practice guidelines stated that radioembolization with Y-90 glass beads has been shown to induce extensive tumor necrosis with an acceptable safety profile; however, no studies demonstrating an impact on survival have been established.Citation5
Percutaneous local ablation
Percutaneous local ablation, which includes both RFA and percutaneous ethanol injection, is the standard of care for BCLC stage 0-A HCC not suitable for surgery.Citation2 RFA is the treatment of choice for local destruction of liver tumors. RFA produces coagulative necrosis of the tumor while leaving a safety margin around the tumor, leading this to be the most common local ablative therapy. RFA can be performed both percutaneously under radiological guidance using CT or US or during surgery guided by intraoperative US. Complete ablation of tumors <2 cm is possible in >90% of cases.Citation135 There are several limitations of RFA:
for tumors >3 cm, complete necrosis is rarely observed;
there is difficulty in ablating tumors that are adjacent to major blood vessels;
it is difficult to reach certain segments of the liver (ie, Segment 1) percutaneously;
subcapsular lesions can rupture into peritoneum;
bladder injury can occur with ablation of segment IVb; and
in livers with multinodular cirrhosis, targeting lesions under ultrasound guidance can be difficult.Citation105
The treatment of HCC has been well demonstrated in multiple series with overall 5-year survival rates between 33% and 55%.Citation136 Ethanol injection requires multiple injections on separate days and rarely induces significant necrosis in tumors >3 cm largely because the injected ethanol rarely reaches the entire tumor volume. Tumor necrosis rates are 90%–100% for tumors <2 cm, 70% for 2- and 3-cm tumors, and 50% in HCC tumors between 3 and 5 cm.Citation5 In one prospective nonrandomized study, RFA achieved higher ablation rates on HCC tumors <3 cm than percutaneous ethanol injection (90% vs 80%) with fewer treatments.
Microwave ablation
Microwave ablation (MWA) can be utilized both percutaneously and intraoperatively and is a potentially curative ablative procedure.Citation137 It is a method very similar to RFA, except MWA utilizes electromagnetic waves with frequencies >900 kHz to irradiate and ablate tumor foci.Citation90 This leads to rapid elevation of temperatures within the MWA field to excess of 100°C without the damaging effects of tissue impedance, leading to a more rapid and uniform ablation.Citation53 This carries an increased risk of more severe injury to adjacent structures when compared to RFA. Earlier studies comparing MWA and RFA demonstrated no statistical difference in efficiency, and more recent studies using improved MWA modalities show potential.Citation90 Clinical advantage of MWA over RFA and its potential to demonstrate increased rates of tumor necrosis with a reduction in overall treatments need to be evaluated.
Systemic therapy
The majority of patients diagnosed with HCC present with advanced disease. Prior to 2008, no systemic therapy was available that demonstrated an improvement in survival. With the publication of two randomized placebo-controlled Phase III trials, the oral multitargeted tyrosine kinase inhibitor sorafenib has become the new standard of treatment for advanced HCC with an increased median survival from 7.9 months in the placebo group to 10.7 months in the treatment group.Citation138,Citation139 Sorafenib blocks the activity of Raf serine/threonine kinase isoforms, as well as the receptor tyrosine kinases vascular endothelial growth factor receptor 2 and 3, platelet-derived growth factors receptor β, c-KIT, FLT-3, and RET, to inhibit tumor angiogenesis and tumor cell proliferation.Citation140 Currently, sorafenib is recommended in patients with advanced HCC and preserved liver function who are not candidates for either resection or liver transplantation and have failed to respond to locoregional therapies.Citation141 The main side effects include anorexia, nausea, vomiting, weight loss, hoarseness of voice, esthesia, and hypertension.Citation142 Sorafenib can be difficult to tolerate because of the side effect profile, dose reduction (54%) or treatment interruption (40%) is often needed.Citation143 Despite the side effects, treatment is recommended to be continued until progression of the tumor is demonstrated. Currently, studies are continuing in an attempt to identify the best responders to sorafenib; c-Jun N-terminal kinase activity was positively correlated with the CD133 expression level and inversely correlated with the therapeutic response to sorafenib.Citation105 Consequently, c-Jun N-terminal kinase activity may be considered as a new predictive biomarker for response to sorafenib.Citation101
Conclusion
HCC is an aggressive cancer that occurs in the setting of chronic liver disease and cirrhosis that frequently presents in advanced stages. Concomitant liver dysfunction with advanced tumor stages further impedes curative therapies. HCC as well as other cancers, can be prevented if appropriate measures, including HBV vaccination, universal screening of blood products, use of safe injection practices, treatment and education of alcoholics and intravenous drug users, and initiation of antiviral therapy, have shown to be effective.Citation102,Citation144
Continued improvement in both surgical and nonsurgical approaches has demonstrated significant benefits in overall survival. While OLT remains the only curative surgical procedure, the shortage of available organs precludes this therapy for many patients with HCC. Sorafenib has shown to be a unique neoantigenic targeting agent with encouraging results. Studies need to further investigate other biomarkers both alone and in conjunction with other modalities to assess survival and tumor regression.
Disclosure
The authors report no conflicts of interest in this work.
References
- Center for Disease Control and Prevention (CDC)Hepatocellular carcinoma-United States 2001–2006MMWR Morb Mortal Wkly Rep2010591751752020448528
- CrissienAMFrenetteCCurrent Management of hepatocellular carcinomaGastroenterol Hepatol2014103153161
- FerlayJShinHRBrayFFormanDMathersCParkinDMEstimates of worldwide burden of cancer in 2008: GLOBOCAN 2008Int J Cancer2010127122893297121351269
- AltekruseSFMcGlynnKAReichmanMEHepatocellular carcinoma incidence, mortality and survival trends in the United States from 1975 to 2005J Clin Oncol2009271485149119224838
- BruixJShermanMAASLD Practice Guidelines: management of hepatocellular carcinoma: an updateHepatology2010135
- OttJJStevensGAGroegerJWiersmaSTGlobal epidemiology of hepatitis B virus infection: new estimates of age-specific HBsAg seroprevalence and endemicityVaccine201230122212221922273662
- International Agency for Research on Cancer (IARC)Monographs on the evaluation of carcinogenic risks to humansHepatitis Viruses199459182221
- McMahonBJThe natural history of chronic hepatitis B virus infectionHepatology2009495S45S5519399792
- ChenGLinWShenFIloejeUHLondonWTEvansAAPast HBV viral load as predictor of mortality and morbidity from HCC and chronic liver disease in a prospective studyAm J Gastroenterol200610181797180316817842
- HosakaTSuzukiFKobayashiMLong-term entecavir treatment reduces hepatocellular carcinoma incidence in patients with hepatitis B virus infectionHepatology20135819810723213040
- ChiangC-JYangY-WYouS-LLaiM-SChenC-JThirty-year outcomes of the national hepatitis B immunization program in TaiwanJAMA2013310997497624002285
- GoldsteinSTZhouFHadlerSCBellBPMastEEMargolisHSA mathematical model to estimate global hepatitis B disease burden and vaccination impactInt J Epidemiol20053461329133916249217
- DengMZhouXGaoSThe effects of telbivudine in late pregnancy to prevent intrauterine transmission of the hepatitis B virus: a systematic review and meta-analysisVirol J2012918522947333
- WuQHuangHSunXTelbivudine prevents vertical transmission of hepatitis B virus from women with high viral loads: a prospective long-term studyClin Gastroenterol Hepatol20151361170117625251571
- ChooQLRichmanKHHanJHGenetic organization and diversity of the hepatitis C virusProc Natl Acad Sci U S A1991886245124551848704
- BostanNMahmoodTAn overview about hepatitis C: a devastating virusCrit Rev Microbiol20103629113320345213
- AshamEHKasebAGhobrialRMManagement of hepatocellular carcinomaSurg Clin North Am201391423145024206860
- LokASSeeffLBMorganTRIncidence of hepatocellular carcinoma and associated risk factors in hepatitis C-related advanced liver diseaseGastroenterology2009136113814818848939
- GaoCFangLZhaoHCLiJTYaoSKPotential role of diabetes mellitus in the progression of cirrhosis to hepatocellular carcinoma: a cross-sectional case-control study from Chinese patients with HBV infectionHepatobiliary Pancreat Dis Int201312438539323924496
- PuotiMBrunoRSorianoVHepatocellular carcinoma in HIV-infected patients: epidemiological features, clinical presentation and outcomeAIDS200418172285229315577541
- SingalAKAnandBSMechanisms of synergy between alcohol and hepatitis C virusJ Clin Gastroenterol200741876177217700425
- MorganRLBaackBSmithBDYartelAPitasiMFalck-YtterYEradication of hepatitis C virus infection and the development of hepatocellular carcinoma: a meta-analysis of observational studiesAnn Intern Med2013158532933723460056
- International Agency for Research on Cancer (IARC)Monographs on the evaluation of carcinogenic risks to humansAlcohol Drinking19984444207215
- BateyRGBurnsTBensonRJBythKAlcohol consumption and the risk of cirrhosisMed J Aust19921564134161545749
- MorganTRMandayamSJamalMMAlcohol and hepatocellular carcinomaGastroenterology20041275S87S9615508108
- JewellJSheronNTrends in European liver death rates: implications for alcohol policyClin Med2010103259263
- BrechotCNalpasBFeitelsonMAInteractions between alcohol and hepatitis viruses in the liverClin Lab Med1996162732878792072
- HassanMMHwangLYHattenCJRisk factors for hepatocellular carcinoma: synergism of alcohol with viral hepatitis and diabetes mellitusHepatology20023651206121312395331
- TuratiFGaleoneCRotaMAlcohol and liver cancer: a systematic review and meta-analysis of prospective studiesAnn Oncol20142581526153524631946
- RinellaMENonalcoholic fatty liver disease: a systematic reviewJAMA2015313222263227326057287
- WangCWangXGongGIncreased risk of hepatocellular carcinoma in patients with diabetes mellitus: a systematic review and meta-analysis of cohort studiesInt J Cancer201213071639164821544812
- WongRJCheungRAhmedANonalcoholic steatohepatitis is the most rapidly growing indication for liver transplantation in patients with hepatocellular carcinoma in the U.SHepatology20145962188219524375711
- El-SeragHBHampelHJavadiFThe association between diabetes and hepatocellular carcinoma: a systemic review of epidemiologic evidenceClin Gastroenterol Hepatol2006436938016527702
- MooreMAParkCBTsudaHImplications of the hyperinsulinaemia-diabetes-cancer link for preventive effortsEur J Cancer Prev199872891079818771
- BalkauBKahnHCourbonDEschwegeEDucimetierePParis Prospective StudyHyperinsulinemia predicts fatal liver cancer but is inversely associated with fatal cancer at some other sites: the Paris Prospective StudyDiabetes Care200124584384911347741
- CalleeEERodriguezCWalker-ThurmondKThunMJOverweight, obesity and mortality from cancer in a prospective studied cohort of US adultsN Engl J Med20033481625163812711737
- ReddyJKRaoMSLipid metabolism and liver inflammationAm J Physiol Gastrointest Liver Physiol2006290G852G85816603729
- LarsonSCWolkAOverweight, obesity and risk of liver cancer: a meta-analysis of cohort studiesBr J Cancer2007971005100817700568
- MonsourHPAshamEMcFaddenRSVictorDWMuthuswamyBZaheerIHepatocellular carcinoma: the rising tide from east to west – a review of epidemiology, screening and tumor markersTransl Cancer Res201326492506
- WakaiTShiraiYSakataJKoritaPVAjiokaYHatakeyamaKSurgical outcomes for hepatocellular carcinoma in nonalcoholic fatty liver diseaseJ Gastrointest Surg20111581450145821512848
- TokushigeKHashimotoEYatsujiSProspective study of hepatocellular carcinoma in nonalcoholic steatohepatitis in comparison with hepatocellular carcinoma caused by chronic hepatitis CJ Gastroenterol201045996096720376504
- WhiteDLEpidemiology of hepatocellular carcinomaCarrBIHepatocelluar CarcinomaNew York, NYHumana Press2010125
- YuanJ-MRossRStanczykFZA cohort study of serum testosterone and hepatocellular carcinoma in Shanghai, ChinaInt J Cancer19956344914937591255
- WhiteDLTavakoli-TabasiSKuzniarekJPascuaRRamseyDJEl-SeragHBHigher serum testosterone is associated with increased risk of advanced hepatitis C-related liver disease in malesHepatology201255375976821858849
- LiuYWuFGlobal burden of aflatoxin-induced hepatocellular carcinoma: a risk assessmentEnviron Health Perspect2010118681882420172840
- ChenJGEgnerPANgDReduced aflatoxin exposure presages decline in liver cancer mortality in an endemic region of ChinaCancer Prev Res201361010381045
- KoCSiddaiahNBergerJPrevalence of hepatic iron overload and association with hepatocellular cancer in end-stage liver disease: results from the National Hemochromatosis Transplant RegistryLiver Int200727101394140117927713
- DeugnierYTurlinBIron and hepatocellular carcinomaJ Gastroenterol Hepatol200116549149411350542
- GandiniSBotteriEIodiceSBoniolMLowenfelsARMaisonneuvePTobacco smoking and cancer: a meta-analysisInt J Cancer200812215516417893872
- MaheshwariSSarrajAKramerJEl-SeragHBOral contraception and the risk of hepatocellular carcinomaJ Hepatol20074750651317462781
- van MeerSde ManRACoenraadMJSurveillance for hepatocellular carcinoma is associated with increased survival: results from a large cohort in the NetherlandsJ Hepatol20156351156116326100498
- ZhangBHYangBHTangZYRandomized controlled trial of screening for hepatocellular carcinomaJ Cancer Res Clin Oncol2004130741742215042359
- BruixJShermanMAmerican Association for the Study of Liver DiseasesAASLD Practice Guideline: management of hepatocellular carcinoma: an updateHepatology20115321020102221374666
- TrevisaniFSantiVGramenziASurveillance for early diagnosis of hepatocellular carcinoma: is it effective in intermediate/advanced cirrhosis?Am J Gastroenterol20071021122482257
- MasuzakiROmataMScreening program in high-risk populationsHepatocellular Carcinoma20115568
- LokASHeathcoteEJHoofnagleJHManagement of hepatitis B: 2000 – summary of a workshopGastroenterology200112071828185311375963
- KewMCMacerolloPEffect of age on the etiologic role of the hepatitis B virus in hepatocellular carcinoma in blacksGastroenterology19889424394422446950
- YuMWChangHCLiawYFFamilial risk of hepatocellular carcinoma among chronic hepatitis B carriers and their relativesJ Natl Cancer Inst200092141159116410904089
- TakashimaTMatsuiOSuzukiMIdaMDiagnosis and screening of small hepatocellular carcinomas. Comparison of radionuclide imaging, ultrasound, computed tomography, hepatic angiography, and α1-fetoprotein assayRadiology19821456356386183708
- PetersonMSBaronRLRadiologica diagnosis of hepatocellular carcinomaClin Liver Dis20015112314411218911
- BolondiLSofiaSSiringoSSurveillance programme of cirrhotic patients for early diagnosis and treatment of hepatocellular carcinoma: a cost effectiveness analysisGut200148225125911156649
- AchkarJPArayaVBaronRLMarshJWDvorchikIRakelaJUndetected hepatocellular carcinoma: clinical features and outcomes after liver transplantationLiver Transpl Surg199844774829791158
- BraheeDDOgedegbeCHasslerCBody mass index and abdominal ultrasound image quality: a pilot survey of sonographersJ Diagn Med Sonogr20132926672
- WaldCRussoMWHeimbachJKHussainHKPomfretEABruixJNew OPTN/UNOS policy for liver transplant allocation: standardization of imaging, diagnosis, classification, and reporting of hepatocellular carcinomaRadiology2013266237638223362092
- ColliAFraquelliMCasazzaGAccuracy of ultrasonography, spiral CT, magnetic resonance, and alpha-fetoprotein in diagnosing hepatocellular carcinoma: a systematic reviewAm J Gastroenterol2006101351352316542288
- CollierJShermanMScreening for hepatocellular carcinomaHepatology1998272732789425947
- ShermanMPeltekianKMLeeCScreening for hepatocellular carcinoma in chronic carriers of hepatitis B virus: incidence and prevelance of hepatocellular carcinoma in a North American urban populationHepatology1995224324387543434
- TrevisaniFD’IntinoPEMorselli-LabateAMSerum α-fetoprotein for diagnosis of hepatocellular carcinoma in patients with chronic liver disease: influence of HBsAg and anti-HCV statusJ Hepatol200134457057511394657
- Gambarin-GelwanMWolfDCShapiroRSchwartzMEMinADSensitivity of commonly available screening tests in detecting hepatocellular carcinoma in hepatitis C virus cirrhosisHepatology20009515351538
- Di BisceglieAMSterlingRKChungRTSerum α-fetoprotein levels in patients with advanced hepatitis C: results from the HALT-C TrialJ Hepat2005433434441
- NguyenMHGarciaRTSimpsonPWWrightTLKeeffeEBRacial differences in effectiveness of alpha-fetoprotein for diagnosis of hepatocellular carcinoma in hepatitis C virus cirrhosisHepatology200236241041712143050
- LinOSKeeffeEBSandersGDOwensDKCost-effectiveness of screening for hepatocellular carcinoma in patients with cirrhosis due to chronic hepatitis CAliment Pharmacol Ther200419111159117215153169
- KhienVVMaoHVChinhTTClinical evaluation of lentil lectin-reactive alpha-fetoprotein-L3 in histology-proven hepatocellular carcinomaInt J Biol Markers200116210511111471892
- IshiiMGamaHChidaNSimultaneous measurements of serum α-fetoprotein and protein induced by vitamin K absence for detecting hepatocellular carcinoma. South Tohoku District Study GroupAm J Gastroenterol20009541036104010763956
- MarreroJASuGLWeiWDes-γ carboxyprothrombin can differentiate hepatocellular carcinoma from nonmalignant chronic liver disease in American patientsHepatology20033751114112112717392
- SinghalAJayaramanMDhanasekaranDNKohliVMolecular and serum markers in hepatocellular carcinoma: predictive tools for prognosis and recurrenceCrit Rev Oncol Hematol201282211614021680198
- SangiovanniAManiniMAIavaroneMThe diagnostic and economic impact of contrast imaging techniques in the diagnosis of small hepatocellular carcinoma in cirrhosisGut20105963864419951909
- LeeYJLeeJMLeeJSHepatocellular carcinoma: diagnostic performance of multidetector CT and MR imaging – a systematic review and meta-analysisRadiology20152759710925559230
- El-SeragHBHepatocellular carcinomaN Engl J Med20113651118112721992124
- VerslypeCRosmorducORougierPESMO Guidelines Working GroupHepatocellular carcinoma: ESMO-ESDO Clinical Practice Guidelines for diagnosis, treatment and follow-upAnn Oncol2012237vii42vii48
- NathanHPawlikTMStaging of hepatocellular carcinomaMastersKMVautheyJ-NHepatocellular CarcinomaBerlin, GermanySpringer6980
- HuoTILinHCHsiaCYThe model for end-stage liver disease based cancer staging systems are better prognostic models for hepatocellular carcinoma: a prospective sequential surveyAm J Gastroenterol20071021920193017573792
- KamathPSWiesnerRHMalinchocMA model to predict survival in patients with end-stage liver diseaseHepatology200133246447011172350
- VautheyJNLauwersGYEsnaolaNFSimplified staging for hepatocellular carcinomaJ Clin Oncol20022061527153611896101
- FlemingIDAJCC/TNM cancer staging for hepatocellular carcinomaJ Surg Oncol20017723323611473370
- SanyalAPoklepovicAMoyneurEBargoutV(2010). Population-based risk factors and resource utilization for HCC: US perspectiveCurr Med Res Opin20102692183219120666689
- SingalAGNehraMAdams-HuetB(2013). Detection of hepatocellular carcinoma at advanced stages among patients in the HALT-C trial: where did surveillance fail?Am J Gastroenterol2013108342543223337478
- FornerRMRodriguez de LopeCBruixJCurrent strategy for staging and treatment: the BCLC update and future prospectsSemin Liver Dis201030617420175034
- AllemannPDemartinesNBouzoureneHTempiaAHalkicNLong-term outcome after liver resection for hepatocellular carcinoma larger than 10 cmWorld J Surg201337245245823188527
- WongRFrenetteCUpdates in the management of hepatocellular carcinomaGastroenterol Hepatol2011711624
- IshizawaTHasegawaAAokiTNeither multiple tumors nor portal hypertension are surgical contraindications for hepatocellular carcinomaGastroenterology200813471908191618549877
- RoayaieSHaimMBEmreSComparison of surgical outcomes for hepatocellular carcinoma in patients with hepatitis B versus hepatitis C: a western experienceAnn Surg Oncol200071076477011129425
- ColleoniMAudisioRADe BraudFFazioNMartinelliGGoldhirshAPractical considerations in treatment of hepatocellular carcinomaDrugs19985533673829530543
- D’AmicoGGarcia-TsaoGPagliaroLNatural history and prognostic indicators of survival in cirrhosis: a systemic review of 118 studiesJ Hepatol20064421723116298014
- TehSHChristeinJDonohueJHepatic resection of hepatocellular carcinoma in patients with cirrhosis: model of end-stage liver disease (MELD) score predicts perioperative mortalityJ Gastrointest Surg2005991207121516332475
- BelghitiJKianmaneshRSurgical treatment of hepatocellular carcinomaHPB20057424918333160
- AbulkhirALimongelliPHealeyAJPreoperative portal vein embolization for major liver resection: a meta-analysisAnn Surg20082471495718156923
- PalavecinoMChunYSMadoffDCMajor hepatic resection for hepatocellular carcinoma with or without portal vein embolization: perioperative outcome and survivalSurgery2009145439940519303988
- PoonRTFanSTLoCMLiuCIWongJLong-term survival and pattern of recurrence after resection of small hepatocellular carcinoma in patients with preserved liver function: implications for a strategy of salvage transplantationAnn Surg200223537338211882759
- TosoCTrotterJWeiATotal tumor volume predicts risk of recurrence following liver transplantation in patients with hepatocellular carcinomaLiver Transpl2007711071115
- RimassaLSantoroASorafenib therapy in advanced hepatocellular carcinoma: the SHARP trialExpert Rev Anticancer Ther20099673974519496710
- HagiwaraSKudoMNagaiTActivation of JNK and high expression level of CD133 predict a poor response to sorafenib in hepatocellular carcinomaBr J Cancer20121061997200322596232
- AuJSFrenetteCT(2015). Management of hepatocellular carcinoma: current status and future directionsGut Liver20159443744826087860
- ImamuraHMatsuyamaYTanakaERisk factors contributing to early and late phase intrahepatic recurrence of hepatocellular carcinoma after hepatectomyJ Hepatol20033820020712547409
- VivarelliMMontaltiRRisalitiAMultimodal treatment of hepatocellular carcinoma on cirrhois: an updateWorld J Gastroenterol201319427316732624259963
- TorzilliGMakuuchiMInoueKNo-mortality liver resection for hepatocellular carcinoma in cirrhotic and noncirrhotic patients: is there a way? A prospective analysis of our approachArch Surg1999134998499210487594
- FanSTLoCMLiuCLHepatectomy for hepatocellular carcinoma: toward zero hospital deathsAnn Surg199922932233010077043
- AbdallaEKDenysAHasegawaKTreatment of large and advanced hepatocellular carcinomaAnn Surg Oncol200815497998518236115
- CapussottiLFerreroAViganoLPolastriRTaboneMLiver resection for HCC with cirrhosis: surgical perspectives out of EASL/AASLD guidelinesEur J Surg Oncol200935111517689043
- CherquiDLaurentAMocellinNLiver resection for transplantable hepatocellular carcinoma: long-term survival and role of secondary liver transplantationAnn Surg2009250573874619801927
- ChaCHRuoLFongYResection of hepatocellular carcinoma in patients otherwise eligible for transplantationAnn Surg2003238231532314501497
- ViganoLCherquiDLaparoscopic liver resection for HCC: a European perspectiveHepatocellular CarcinomaBerlin, GermanySpringer2011185206
- MazzaferroVRegaliaEDociRLiver transplantation for the treatment of small hepatocellular carcinoma in patients with cirrhosisN Engl J Med1996334116936998594428
- MazzaferroVBhooriSSpositoCMilan criteria in liver transplantation for hepatocellular carcinoma: an evidence-based analysis of 15 years of experienceLiver Transpl2011172S44S5721695773
- YaoFYFerrellLBassNMLiver transplantation for hepatocellular carcinoma: expansion of tumor size limits does not adversly impact survivalHepatology2001331394140311391528
- DuBayDSandroussiCSandhuLLiver transplantation for advanced hepatocellular carcinoma using poor tumor differentiation on biopsy as an exclusion criteriaAnn Surg201125316617221294289
- YaoFYExpanded criteria for hepatocellular carcinoma: down-staging with a view to liver transplantation – yesSemin Liver Dis200626323924716850373
- YaoFYHiroseRLaBergeJMA prospective study on downstaging of hepatocellular carcinoma prior to liver transplantationLiver Transpl200511121505151416315294
- YaoFYKerlanRKHiroseR(2008). Excellent outcomes following down-staging of hepatocellular carcinoma prior to liver transplantation: an intention-to-treat analysisHepatology200848381982718688876
- US Department of Health and Human Services, Health Resources and Services Administration, Organ Procurement and Transplantation Network (n.d.). Retrieved January 1, 2015. Available from: http://optn.transplant.hrsa.gov/policiesAndBylaws/policies.aspAccessed May 19, 2016
- MancusoAManagement of hepatocellular carcinoma: enlightening the gray zonesWorld J Hepatol20135630231023805354
- TakayasuKAriiSIkaiIProspective cohort study of transarterial chemoembolization for unresectable hepatocellular carcinoma in 8,510 patientsGastroenterology200613146146916890600
- SchwartzMRoayaieSKonstadoulakisMStrategies for the management of hepatocellular carcinomaNat Clin Pract Oncol2007442443217597707
- LewandowskiRJGeschwindJFLiapiESalemRTranscatheter intraarterial therapies: rationale and overviewRadiology2011259364165721602502
- LammerJMalagariKVoglTProspective randomized study of doxorubicin-eluting-bead embolization in the treatment of hepatocellular carcinoma: results of PRECISION V studyCardiovasc Intervent Radiol2010331415219908093
- RaoulJLSangroBFornerAEvolving strategies for the management of intermediate-stage hepatocellular carcinoma: available evidence and expert opinion on the use of transarterial chemoembolizationCancer Treat Rev201137321222020724077
- LlovetJMRealMIMontanaXArterial embolization or chemoembolisation versus symptomatic treatment in patients with unresectable hepatocellular carcinoma: a randomized controlled trialLancet200235993191734173912049862
- LlovetJMBruixJSystematic review of randomized trials for unresectable hepatocellular carcinomaHepatology200337242944212540794
- TinkleCLHaas-KoganDHepatocellular carcinoma:natural history, current management, and emerging toolsBiologics2012620721922904613
- YuSJKimYJEffective treatment strategies other than sorafenib for the patients with advanced hepatocellular carcinoma invading portal veinWorld J Hepatol20157111553156126085914
- RaoulJLGuyaderDBretagneJFProspective randomized trial of chemoembolization versus intra-arterial injection of 131I-labeled-iodized oil in the treatment of hepatocellular carcinomaHepatology199726115611619362356
- SangroBCarpaneseLCianniRSurvival after yttrium-90 resin microsphere radioembolization of hepatocellular carcinoma across Barcelona liver cancer stages: a European evaluationHepatology201154386887821618574
- VenteMAWondergamMvan der TweelIYttrium-90 micro-sphere radioembolization for the treatment of liver malignancies: a structured meta-analysisEur Radiol20091995195918989675
- KulikLMCarrBIMulcahyMFSafety and efficacy of 90Y radiotherapy for hepatocellular carcinoma with and without portal vein thrombosisHepatology2008471718118027884
- RiazAKulikLLewandowskiRJRadiologic-pathologic correlation of hepatocellular carcinoma treated with internal radiation using yttirum-90 microspheresHepatology2009491185119319133645
- LivraghiTMeloniFDi StasiMSustained complete response and complications rates after radiofrequncy ablation of very early hepatocellular carcinoma in cirrhosis: is resection still the treatment of choice?Hepatology200847828918008357
- LencioniRCioniDCrocettiLEarly-stage hepatocellular carcinoma in patients with cirrhosis: long-term results of percutaneous image-guided radiofrequency ablationRadiology200523496196715665226
- BertotLCSatoMTateishiRYoshidaHKoikeKMortality and complication rates of percutaneous ablative techniques for the treatment of liver tumors: a systemic reviewEur Radiol2011212584259621858539
- LlovetJMRicciSMazzaferroVSorefenib in advanced hepatocellular carcinomaN Engl J Med2008359437839018650514
- ChengALKangYKChenZEfficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: a phase III randomized, double-blind, placebo controlled trialLancet Oncol2009101253419095497
- BruixJRaoulJ-LShermanMEfficiancy and safety of sorafenib in patients with advanced hepatocellular carcinoma: subanalysis of a phase III trialJ Hepatol20125782182922727733
- European Association For The Study Of The Liver, European Organisation For Research And Treatment Of CancerEASL-EORTC clinical practice guidelines: management of hepatocellular carcinomaJ Hepatol20125690894322424438
- IavaroneMCabibboGPiscagliaFField-practice study of sorafenib therapy for hepatocellular carcinoma: a prospective multicenter study in ItalyHepatology20115462055206321898496
- SohalDPSunWHepatocellular carcinoma: prevention and therapyCurr Oncol Rep201113318619421409527
- Cochrane MillerJBridging procedures prior to liver transplantationRadiology Rounds2015131