
Abstract
Objective
The present study aims to investigate the cytokines interleukin (IL)-4, IL-6, IL-10, and IL-17 in the peripheral blood of patients with acute-on-chronic liver failure combined with sepsis, patients with acute-on-chronic liver failure, and patients with liver cirrhosis; to investigate the changes in the levels of inflammatory factors in cases of coagulation dysfunction in liver failure combined with sepsis; and to discover more typical inflammatory factors for further evaluation by functional experiments.
Methods
In the present study, 41 patients with acute-on-chronic liver failure and sepsis were enrolled as study subjects. These patients were compared with 20 patients with either acute-on-chronic liver failure and liver cirrhosis during the same period. The changes in IL-4, IL-6, IL-10, and IL-17 were detected in each group by enzyme-linked immunosorbent assay, and SPSS 17.0 software was adopted for data analysis.
Results
There were no significant changes in the levels of IL-4 in any of the groups. However, the levels of IL-6, IL-10, and IL-17 were significantly higher in the acute-on-chronic liver failure and sepsis group than in the acute-on-chronic liver failure and the liver cirrhosis groups.
Conclusion
The present study shows that when liver failure is accompanied by sepsis, the serum levels of inflammatory factors IL-6, IL-10, and IL-17 are significantly increased. This could be closely correlated with the occurrence and development of coagulation dysfunction and sepsis. These findings provide new ideas for delaying the deterioration of patients with liver failure in clinical practice.
Introduction
It has been reported in the literature that inflammatory storms occur during liver failure and sepsis, which is currently one of the most popular research topics.Citation1 Liver failure is associated with changes in the condition and prognosis of sepsis. Therefore, in patients with liver failure and sepsis, which is more common in the ICU than patients without sepsis, it is important to investigate the changes in the levels of the classic inflammatory factors and the role these changes play in the prognosis of these patients. The T helper (Th) 1/Th2 and Th17 cell dysregulation are the focus of current research and frontiers of infectious and immune diseases. Stopping excessive inflammatory response in a timely manner and restoring normal immune function has always been a topical and difficult research field. Previous studies have confirmed that the presence of Th17 is correlated with infectious bacterial diseases and involved in viral diseases and acute liver injury. We aim to detect changes in the levels of interleukin (IL)-4, IL-6, IL-10, and IL-17 in the peripheral blood of patients in different populations and disease states to investigate changes in the levels of these inflammatory factors in the case of liver failure, coagulation dysfunction, and sepsis, with the aim of finding more typical inflammatory factors for further evaluation by functional experiments.
Therefore, in the present study, patients with acute-on-chronic liver failure and sepsis (ACLF-SP) were selected as subjects. They were compared with patients with acute-on-chronic liver failure (ACLF) and those with liver cirrhosis (LC) during the same period. A comprehensive analysis was conducted to investigate the changes in the levels of IL-4, IL-6, IL-10, and IL-17 in patients with ACLF-SP.
Materials and Methods
The Pretreatment of the Experimental Material
All blood samples were anticoagulated with heparin and treated as follows: All specimens were centrifuged at 4°C for 10 minutes at 2000 g. The collected plasma was immediately stored at −80°C. The levels of cytokines (IL-4, IL-6, IL-10, and IL-17) were detected by enzyme-linked immunosorbent assay (ELISA) (Beijing Dakwei Biological Company). The sensitivities for the detection of the cytokines were as follows: 0.5 pg/mL for IL-4 (35–1.1 pg/mL), 2 pg/mL for IL-6 (200–6.25 pg/mL), 5 pg/mL for IL-10 (400–12.5 pg/mL), and 31.25 pg/mL for IL-17 (4000–62.5 pg/mL). The data were drawn using the ELISA Calc V 0.5 software to obtain a standard curve, and the cytokine contents from each sample were analyzed. The cytokine standard was a freeze-dried powder. The freeze-dried powder was dissolved in sterile distilled water, according to the label instructions, and the standard diluents were used for multiple dilutions. The concentration of the masterbatch for IL-4 was 113 pg/mL, and the concentration gradient of the standard diluents was 113 pg/mL, 56.5 pg/mL, 28.25 pg/mL, 14.125 pg/mL, and 7.06 pg/mL. The concentration of the masterbatch for IL-6 was 328 pg/mL, and the concentration gradient of the standard diluents was 328 pg/mL, 164 pg/mL, 82 pg/mL, 41 pg/mL, 20.5 pg/mL, and 10.25 pg/mL. The concentration of the masterbatch for IL-10 was 612 pg/mL, and the concentration gradient of the standard diluents was 612 pg/mL, 306 pg/mL, 153 pg/mL, 76.5 pg/mL, 38.25 pg/mL, and 19.125 pg/mL. The concentration of the masterbatch for IL-17 was 1000 pg/mL, and the concentration gradient of the standard was 1000 pg/mL, 500 pg/mL, 250 pg/mL, 125 pg/mL, 62.5 pg/mL, and 31.25 pg/mL.
Method
Before use, all reagents were thoroughly mixed to avoid foaming. We added 100 ul of the standard with multiple dilutions to the standard well, 100 ul of the sample to each sample well, and 100 ul of standard diluents to each blank control well. We added 50 ul of the diluted biotinylated antibody to each well. These were covered with sealing film and incubated at room temperature (18°C–25°C) for two hours. Washing the plate: The liquid in the well was discarded, 300 ul of washing solution was added to each well, and the liquid in the well was discarded after one minute. This was repeated three times. After the third time, it was dried on filter paper. We added 100 ul streptavidin–horseradish peroxidase to each well, covered them with sealing film, and incubated them at room temperature for 20 minutes. Washing the plate: The liquid in the well was discarded, 300 ul of washing solution was added to each well, and the liquid in the well was discarded after one minute. This was repeated three times. After the third time, it was dried on filter paper. We added 100 ul of TMB Chromogen Solution to each well and incubated these at room temperature for 10–15 minutes for a color reaction. After this, 100 ul of termination solution was quickly added to each well to terminate the reaction. The plate was read with a detection wavelength of 450 nm immediately after terminating the reaction. The analysis software ELISA Calc V 0.5 was used to draw a standard curve, and the cytokine concentrations in the samples were analyzed according to the optical density (OD) value. SPSS 17.0 software was used to test for normality of the experimental data. For data where this test resulted in P < 0.05, the experimental data were expressed as mean ± standard deviation. When it resulted in P ≥ 0.05, the experimental data were expressed as median and interquartile ranges. The t-test was adopted for comparisons between two groups, and the analysis of variance test was used for comparisons among multiple groups.
Results
The Establishment of the Standard Curve of Cytokines in Each Group
(1) The standard curve of IL-4 () R2 = 0.99276
Figure 1 (A) The standard curve of IL-4 detected in the plasma. (B) The standard curve of IL-6 detected in the plasma. (C) The standard curve of IL-10 detected in the plasma. (D) The standard curve of IL-17 detected in the plasma.
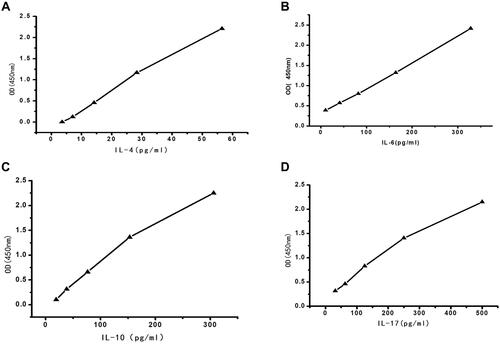
The equation: y = 18.9231 x −1.68121
The residual sum of squares: 2.02103
(2) The standard curve of IL-6 () R2 = 0.99897
The equation: y = 26.6124 x −9.01857
The residual sum of squares: 0.1685
(3) The standard curve of L-10 () R2 = 0.99796
The equation: y = 67.2789 x −4.41123
The residual sum of squares: 3.02141
(4) The standard curve of IL-17 () R2 = 0.99135
The equation: y = 257.99 x −61.9874
The residual sum of squares: 950.3211
The Comparison of the Levels of Cytokines IL4, IL6, IL10, and IL17 in the Control Group, The Liver Failure Group, and Liver Failure Combined with Sepsis Group
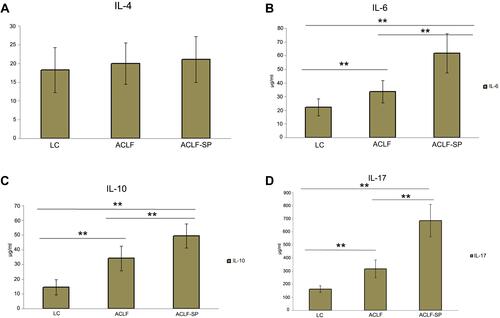
There was no statistical difference in the levels of IL-4 in the peripheral blood among each group (P > 0.05). The level of IL-6 in the ACLF-SP group (61.64 ± 14.38 pg/mL) was higher than that in the ACLF group (33.72 ± 8.18 pg/mL, P < 0.01) and that in the LC group (22.36 ± 6.21 pg/mL, P = 0.00, P < 0.01). The level of IL-6 in the ACLF group was higher than that in the LC group (P < 0.01). The level of IL-10 in the ACLF-SP group (49.43 ± 8.15 pg/mL) was significantly higher than that in the ACLF group (34.11 ± 8.20 pg/mL, P < 0.01) and that in the LC group (14.59 ± 5.13 pg/mL, P = 0.00, P < 0.01). The level of IL-10 in the ACLF group was higher than that in the LC group (P < 0.01). The level of IL-17 in the ACLF-SP group (685.27 ± 122.91 pg/mL) was significantly higher than that in the ACLF group (317.21 ± 68.13 pg/mL, P < 0.01) and that in the LC group (162.96 ± 25.19 pg/mL, P = 0.00, P < 0.01). The level of IL-17 in the ACLF group was higher than that in the LC group (P < 0.01) ().
Figure 2 The comparison of the levels of cytokines IL4, IL6, IL10, and IL17 in the control group, the liver failure group, and the liver failure combined with sepsis group. (A) The level of IL-4 not significantly different between the control group, the liver failure group, and the liver failure combined with sepsis group (P>0.05). (B) The level of IL-6 was highly increased in ACLF-SP than in ACLF group and LC group (**P<0.01, compared with ACLF and LC group, respectively), and the level of IL-6 was highly increased in ACLF group than LC group (**P<0.01, compared with LC group). (C) The level of IL-10 was obviously increased in ACLF-SP than in ACLF group and LC group (**P<0.01 compared with ACLF and LC group, respectively), and the level of IL-10 was highly increased in ACLF group than LC group (**P<0.01, compared with LC group). (D) The level of IL-17 was significantly increased in ACLF-SP than in ACLF group and LC group (**P<0.01 compared with ACLF and LC group, respectively), and the level of IL-17 was highly increased in ACLF group than LC group (**P<0.01, compared with LC group).
Discussion
Once there exists a co-infection in patients with liver failure, the liver injury will be further aggravated.Citation1 The Asian Pacific Liver Research Association updated the ACLF in 2019 and pointed out that inflammatory factors, including sepsis, play a key role in the development of ACLF. The mortality of patients with ACLF admitted to ICU reaches 21–87% within one month and 42–95% within three months.Citation2,Citation3 Among the 41 patients with co-infections in our study, 30 died, were voluntarily discharged, or received liver transplants. The fatality rate was 73.2%, which is consistent with the reported results. Co-infection can aggravate the condition of patients with liver failure. This is further confirmed by our study results, which show that the rate of death or inefficiency of the 30 patients with co-infection was much higher than the 20 patients without infection. A systematic review and meta-analysis of the impact of systemic inflammatory response syndrome (SIRS) and sepsis on mortality in alcoholic hepatitisCitation4 showed that both SIRS and sepsis were significantly correlated with mortality, and the risk ratios were 2.7 (95% CI, 1.74–4.14) and 2.8 (95% CI, 1.58–4.93), respectively. A variety of toxins and cytokines, such as infection-induced endotoxin, are involved in liver injury, and the subsequent response of the body to this immune response might be the main cause of liver injury.
IL-4 is mainly produced by Th2 cells. Its main functions are to promote the transformation of Th0 cells into Th2 cells; to reduce the formation of Th1 cells; and to downregulate the secretion of pro-inflammatory factors, such as tumor necrosis factor (TNF) 2α and IFN2γ, from monocytes by inhibiting the activity of NF2κB. This inhibits the inflammatory response at the level of cellular immunity and humoral immunity.Citation5 However, IL-4 can promote the proliferation of B cells and secrete IgA, IgE, and other antibodies while inhibiting inflammation and stimulating the production of acquired immunity by the body after the inflammation has dissipated.Citation6 In the present study, there was no significant difference in the expression of IL-4 between the LC, the ACLF-SP, and the ACLF-LC groups. This is inconsistent with the previously inferred mechanisms involved in the inflammatory response and is worthy of further investigation.
IL-6 is produced by Th2 cells, monocytes, vascular endothelial cells, fibroblasts, etc. It is one of the core cytokines that causes liver injury. It can promote the synthesis of acute-phase proteins in the liver, activate T lymphocytes, induce the differentiation of B lymphocytes, act on tissue cells through the modes of paracrine and autocrine, stimulate cell growth, promote the proliferation of the extracellular matrix, and participate in the process of inflammation.Citation7 IL-6 is both an immunomodulatory factor and an inflammatory mediator. When IL-6 levels are elevated, it causes tissue injury. In patients with hepatic disease, endotoxin may stimulate the monocytes to produce a large amount of IL-6, leading to massive necrosis of the hepatic cells as a result of infection.Citation8 Yao et alCitation9,Citation10 reported that IL-6 is highly active in patients with severe chronic hepatitis B, which was closely correlated with hepatic cell injury and the severity of liver disease. The results of our study showed that the level of IL-6 significantly increased in patients with liver failure and liver failure with sepsis, which is consistent with results reported in the literature.
IL-10 is produced by Th2 cells and is an anti-inflammatory cytokine and immunosuppressive factor.Citation11 It can inhibit the differentiation of monocytes into the antigen-presenting cells and the dendritic cells (DCs) and can broadly inhibit the synthesis and expression of inflammatory mediators secreted by monocytes and macrophages.Citation12 During the process of regulating the inflammatory response and limiting liver injury, IL-10 is mainly involved in reducing inflammatory liver injury, delaying liver regeneration, directly reducing collagen formation, increasing collagenase, and reducing the levels of TNFα to prevent hepatic fibrosis. As the degree of hepatic fibrosis changes in chronic hepatitis, the level of IL-10 decreases, and the magnitude of the decrease in IL-10 is consistent with the degree of liver injury.Citation9 The results of our study show that the levels of IL-10 in the peripheral blood of patients with ACLF and ACLF-SP were significantly higher than in the control group. Because the inflammation in ACLF and ACLF-SP was more serious, the level of IL-10 was increased to reduce inflammatory reactive liver injury.
IL-17 was cloned for the first time in 1995.Citation10 For more than ten years, IL-17 has proven to be a strong inflammatory factor. IL-17-mediated powerful effects on stromal cells can lead to the production of inflammatory cytokines and the recruitment of white blood cells, especially neutrophils, thereby creating a connection between innate and adaptive immunity.Citation13,Citation14 However, in 2005, Th17 was identified. This is a third T-cell subgroup that can produce IL-17. This changed the previous understanding of many diseases.Citation15,Citation16 Studies have shown that Th17 appears to be the main regulator of the pathogenesis of several autoimmune and inflammatory diseases.Citation17–Citation19 The discovery of Th17 cells opened up a new way to study the etiology and treatment of a broad spectrum of diseases.Citation20 Regarding the expression of IL-17 secreted by Th17 in liver failure, we observed the expression levels of IL-17 in the subjects in the present study and inferred that IL-17 might play an important role in both liver injury and sepsis.
IL-17 is the most important cytokine representing Th17. IL-17 has a pro-inflammatory effect and can induce pro-inflammatory cytokines and chemokines and cause tissue cell infiltration and tissue destruction.Citation21 IL-17 is also involved in the proliferation, maturation, and chemotaxis of neutrophils. It can promote the maturation of the DCs and has a co-stimulatory effect on the activation of T cells.Citation22 IL-22 can enhance the ability in anti-microbial infection and can cooperate with IL-17 to increase inflammation and cause tissue injury. IL-17 is also involved in the pathogenesis of and body response to many diseases.Citation23 A recent study has shown that the expression of IL-17, IL-23, IL-1b, IL-6, and TNFα is highest at sites with the most severe inflammation.Citation24 Researchers have shown that IL-6 has a very important role in regulating the balance between IL-17-producing Th17 cells and regulatory T cells (Treg). IL-6 induces the development of Th17 cells from naïve T cells together with transforming growth factor beta (TGF-beta). In contrast, IL-6 inhibits TGF-beta-induced Treg differentiation.Citation25 Pathogenic capabilities of Th17 cells can be restrained by stimulating IL-10 production and transdifferentiation into IL-10-producing Treg type 1 cells.Citation26 A recent study revealed an IL-17-dominated trait that is associated with periodontal disease and is inversely modified by the level of IL-10. In the study, IL-17 dominated an inflammatory network characteristic of periodontitis, and IL-10 dampened this excessive IL-17-mediated periodontitis trait.Citation27 Th17 cells are a group of cells that characteristically secrete IL-17. The detection of the concentration of IL-17 in plasma is the most important evidence of the functioning of Th17 cells. In our study, the levels of cytokines in the peripheral blood, including IL-4, IL-6, IL-10, and IL-17, were detected in the above-mentioned populations. The results indicate that the concentration of IL-17 in the peripheral blood of patients with ACLF is significantly higher than in both patients with LC and those with ACLF. The biological effects of IL-17 may further induce neutrophils, macrophages, etc. at the site of the inflammation, further aggravating liver injury. Follow-up research could consider conducting a comprehensive screening of protein chips to select more known or unknown markers with clinically significant research options.
One of the limitations of this study is the relatively small sample size, as liver failure combined with sepsis is relatively rare in clinical practice, making it difficult to collect a large number of cases. For future studies, we will continue to collect relevant cases to further confirm the conclusions of this study. Another limitation is that the study design was relatively simple and only compared groups at each level. No further correlation analysis was conducted. In the next step, we will perform further analysis to enrich the results.
Conclusion
The present experimental study confirms that when liver failure is complicated by sepsis, the serum levels of inflammatory factors, such as IL-6, IL-10, and IL-17, are significantly increased. This may be correlated with the occurrence and development of coagulation dysfunction and sepsis, which will provide new directions and ideas for clinically delaying and intervening in the deterioration of patients with liver failure.
Ethics Approval Statement
This study was conducted with approval from the Ethics Committee of Fifth Medical Center of Chinese PLA Hospital.
This study was conducted in accordance with the Declaration of Helsinki.
Written informed consent was obtained from all participants for this study.
Acknowledgment
Yuling Qin and Yuesu Zhou are co-corresponding authors.
Disclosure
The authors report no conflicts of interest in this work.
Additional information
Funding
References
- Woznica EA, Inglot M, Woznica RK, Lysenko L. Liver dysfunction in sepsis. Adv Clin Exp Med. 2018;27(4):547–551. doi:10.17219/acem/68363
- Hernaez R, Sola E, Moreau R, Gines P. Acute-on-chronic liver failure: an update. Gut. 2017;66(3):541–553. doi:10.1136/gutjnl-2016-312670
- Sarin SK, Choudhury A, Sharma MK, et al. Acute-on-chronic liver failure: consensus recommendations of the Asian Pacific association for the study of the liver (APASL): an update. Hepatol Int. 2019;13(4):353–390. doi:10.1007/s12072-019-09946-3
- Jaruvongvanich V, Sanguankeo A, Upala S. Effect of SIRS and sepsis on mortality in alcoholic hepatitis: a systematic review and meta-analysis. Turk J Gastroenterol. 2016;27(5):458–463. doi:10.5152/tjg.2016.16188
- Zhu J. T helper 2 (Th2) cell differentiation, type 2 innate lymphoid cell (ILC2) development and regulation of interleukin-4 (IL-4) and IL-13 production. Cytokine. 2015;75(1):14–24. doi:10.1016/j.cyto.2015.05.010
- Junttila IS. Tuning the cytokine responses: an update on Interleukin (IL)-4 and IL-13 receptor complexes. Front Immunol. 2018;9:888. doi:10.3389/fimmu.2018.00888
- Tanaka T, Narazaki M, Kishimoto T. Interleukin (IL-6) immunotherapy. Cold Spring Harb Perspect Biol. 2018;10(8):a028456. doi:10.1101/cshperspect.a028456
- Schmidt-Arras D, Rose-John S. IL-6 pathway in the liver: from physiopathology to therapy. J Hepatol. 2016;64(6):1403–1415. doi:10.1016/j.jhep.2016.02.004
- Choi JS, Jeong IS, Han JH, Cheon SH, Kim SW. IL-10-secreting human MSCs generated by TALEN gene editing ameliorate liver fibrosis through enhanced anti-fibrotic activity. Biomater Sci. 2019;7(3):1078–1087. doi:10.1039/C8BM01347K
- Yao Z, Painter SL, Fanslow WC, et al. Human IL-17: a novel cytokine derived from T cells. J Immunol. 1995;155(12):5483–5486.
- Ouyang W, O’Garra A. IL-10 family cytokines IL-10 and IL-22: from basic science to clinical translation. Immunity. 2019;50(4):871–891.
- Wang N, Wang J, Jiang R. Effects of IL-10 on OX62, MHC-II and CD86 in bone marrow DCs in rats with organophosphate poisoning. Exp Ther Med. 2018;15(2):1906–1909. doi:10.3892/etm.2017.5629
- Amatya N, Garg AV, Gaffen SL. IL-17 signaling: the Yin and the Yang. Trends Immunol. 2017;38(5):310–322. doi:10.1016/j.it.2017.01.006
- Lemmers A, Moreno C, Gustot T, et al. The interleukin-17 pathway is involved in human alcoholic liver disease. Hepatology. 2009;49(2):646–657. doi:10.1002/hep.22680
- Yasumi Y, Takikawa Y, Endo R, Suzuki K. Interleukin-17 as a new marker of severity of acute hepatic injury. Hepatol Res. 2007;37(4):248–254. doi:10.1111/j.1872-034X.2007.00040.x
- Zhang JP, Yan J, Xu J, et al. Increased intratumoral IL-17-producing cells correlate with poor survival in hepatocellular carcinoma patients. J Hepatol. 2009;50(5):980–989. doi:10.1016/j.jhep.2008.12.033
- Weaver CT, Harrington LE, Mangan PR, Gavrieli M, Murphy KM. Th17: an effector CD4 T cell lineage with regulatory T cell ties. Immunity. 2006;24(6):677–688. doi:10.1016/j.immuni.2006.06.002
- Yasuda K, Takeuchi Y, Hirota K. The pathogenicity of Th17 cells in autoimmune diseases. Semin Immunopathol. 2019;41(3):283–297. doi:10.1007/s00281-019-00733-8
- Bunte K, Beikler T. Th17 cells and the IL-23/IL-17 axis in the pathogenesis of periodontitis and immune-mediated inflammatory diseases. Int J Mol Sci. 2019;20(14):3394. doi:10.3390/ijms20143394
- Balanescu P, Ladaru A, Voiosu T, et al. Th17 and IL-17 immunity in chronic hepatitis C infection. Rom J Intern Med. 2012;50(1):13–18.
- McGeachy MJ, Cua DJ, Gaffen SL. The IL-17 family of cytokines in health and disease. Immunity. 2019;50(4):892–906. doi:10.1016/j.immuni.2019.03.021
- Miossec P, Kolls JK. Targeting IL-17 and TH17 cells in chronic inflammation. Nat Rev Drug Discov. 2012;11(10):763–776. doi:10.1038/nrd3794
- Eyerich K, Dimartino V, Cavani A. IL-17 and IL-22 in immunity: driving protection and pathology. Eur J Immunol. 2017;47(4):607–614. doi:10.1002/eji.201646723
- Weinstein JE, Pepple KL. Cytokines in uveitis[J]. Curr Opin Ophthalmol. 2018;29(3):267–274. doi:10.1097/ICU.0000000000000466
- Kimura A, Kishimoto T. IL-6: regulator of Treg/Th17 balance. Eur J Immunol. 2010;40(7):1830–1835. doi:10.1002/eji.201040391
- Stadhouders R, Lubberts E, Hendriks RW. A cellular and molecular view of T helper 17 cell plasticity in autoimmunity. J Autoimmun. 2018;87:1–15. doi:10.1016/j.jaut.2017.12.007
- Sun L, Girnary M, Wang L, et al. IL-10 dampens an IL-17-mediated periodontitis-associated inflammatory network. J Immunol. 2020;204(8):2177–2191. doi:10.4049/jimmunol.1900532