
Abstract
Purpose
This study aimed to evaluate the prognostic value of the lymphocyte-C-reactive protein ratio (LCR) score, a novel inflammation-based score based on lymphocytes and C-reactive protein, in hepatocellular carcinoma (HCC) patients treated with curative intent.
Patients and Methods
A total of 1158 HCC patients undergoing surgical resection or radiofrequency ablation with curative intent were recruited from 3 different centres and divided into a primary cohort (n=716) and a validation cohort (n=442). Univariate and multivariate analyses were performed to identify variables associated with overall survival (OS). The discriminatory accuracy of seven inflammation-based scores was compared by using the concordance index (C-index).
Results
The LCR score differentiated HCC patients into two groups with distinct prognoses (1-, 3-, and 5-year OS rates and median OS: 92.9%, 81.9%, 73.3% and 99.2 months and 79.8%, 56.6%, 49.7% and 69.1 months; P<0.001). Multivariate analysis showed that LCR score, AFP, ALBI score, tumour size, and TNM stage were independently associated with OS. When patients were stratified according to different disease states, the LCR score could still differentiate HCC patients into two groups with distinct prognoses (all P<0.005). The LCR score demonstrated a markedly superior C-index of 0.621 compared with the other inflammation-based scores (0.503–0.590). These findings were supported by the validation cohort.
Conclusion
The preoperative LCR score is a novel, stable, and clinically feasible prognostic marker for patients with HCC, independent of liver function, tumour characteristics, and treatment allocation and is superior to other inflammation-based scores in terms of its prognostic ability.
Introduction
Hepatocellular carcinoma (HCC) is a major health issue and is the third leading cause of death from cancer worldwide.Citation1 Because of the scarcity of donor organs, surgical resection and radiofrequency ablation (RFA) are the mainstay curative treatment options; globally, three-quarters of all new patients undergo these treatments.Citation2,Citation3 However, a serious disadvantage of local treatment with regard to achieving cure and long-term survival is the high rate of recurrence, which exceeds 60% at 5 years even in patients with small tumours.Citation4,Citation5 In addition, the reported long-term survival of these patients varies.Citation5–Citation7 There is obvious heterogeneity in patients who are classified by the commonly used staging systems as having early HCC. Therefore, it is reasonable to seek inexpensive, readily available, simplified, and objective approaches to inform clinical decision-making and stratify patients into different risk groups.
Systemic inflammation via host-tumour interactions is currently recognized as the seventh hallmark of cancerCitation8 and is intimately involved in tumour development and metastasis in various malignancies.Citation9–Citation12 Based on this knowledge, haematological components of the systemic inflammatory response have been combined to develop inflammation-based prognostic scores, including the Glasgow prognostic score (GPS),Citation13 the modified Glasgow prognostic score (mGPS),Citation14 the neutrophil-lymphocyte ratio (NLR),Citation15 the platelet-lymphocyte ratio (PLR),Citation16 the prognostic index (PI),Citation17 and the prognostic nutritional index (PNI).Citation18 Many studies have shown that these scores are associated with the survival of cancer patients, and they have been used clinically as useful prognostic indicators for cancers, including HCC.Citation19,Citation20 Recently, a novel prognostic score, the lymphocyte-C-reactive protein ratio (LCR), based on the preoperative lymphocyte count and C-reactive protein (CRP), was reported to be a powerful prognostic marker for colorectal cancer,Citation21 gastric cancer and cholangiocarcinoma.Citation22,Citation23 However, whether the LCR can predict the prognosis of HCC patients and its superiority to conventional inflammation-based scores remain unclear.
Therefore, this study aimed to evaluate the prognostic value of the LCR score in patients with HCC with various disease stages and liver functional statuses and to conduct a direct comparison of various inflammation-based scores in a large-scale multicentre cohort.
Patients and Methods
Patients
Consecutive patients who underwent curative hepatic resection (HR) or RFA at the Sun Yat-sen University Cancer Center between January 2010 and December 2015 were enrolled in this study. The diagnosis of HCC was confirmed pathologically or according to the European Association for the Study of the Liver (EASL) diagnostic criteria.Citation24 Only patients who met all of the following criteria were enrolled in the study: (a) age 18–75 years; (b) Child-Pugh class A or B cirrhosis; (c) absence of extrahepatic metastasis; (d) no evidence of hepatic decompensation including ascites refractory to diuretics, oesophageal or gastric variceal bleeding, or hepatic encephalopathy; and (e) no other anticancer treatments before surgical resection or RFA. Patients were excluded from the study if one or more of the following conditions were met: (a) patients were lost to follow-up; (b) patients had missing data for classification based on any of the seven inflammation-based scores; and (c) patients had other concurrent malignancies. Finally, 716 HCC patients were enrolled in the primary cohort of this study.
In addition, we evaluated the significance of the inflammation-based scores in an independent validation cohort of HCC patients treated with curative intent from Fudan University Shanghai Cancer Center and the First Affiliated Hospital of Traditional Chinese Medicine between January 2013 and December 2016 using the same inclusion and exclusion criteria. A total of 442 HCC patients were enrolled in the validation cohort.
This study was approved by the Institutional Review Board of Sun Yat-sen University Cancer Center, Fudan University Shanghai Cancer Center and the First Affiliated Hospital of Traditional Chinese Medicine, and complied with the standards of the Declaration of Helsinki and current ethical guidelines. Written informed consent was obtained from each participant.
Laboratory Measurements of Inflammation-Related Factors in Routine Blood Tests
All blood values recorded in this study, including CRP, bilirubin, albumin, aspartate aminotransferase (AST), alanine aminotransferase (ALT), and α-fetoprotein (AFP) levels and blood cell, neutrophil, lymphocyte, and platelet (PLT) counts, were determined within 5–7 days prior to treatment. Serum CRP levels were measured using latex-enhanced nephelometry (N-Latex CRP II; Siemens Healthcare Diagnostics, Tokyo, Japan). The LCR was calculated as follows: lymphocyte count (number/mL)/CRP level (mg/dL).Citation21 The GPS,Citation13 modified GPS,Citation14 NLR,Citation15 PLR,Citation16 PICitation17 and PNICitation18 were constructed as described in Supplementary Table 1. The albumin-bilirubin (ALBI) score was recorded to describe liver function. Tumour stage was recorded according to the 7th edition of The American Joint Committee on Cancer (AJCC)/International Union Against Cancer (UICC) tumour-node-metastasis (TNM) classification.
Treatment Protocols
Hepatic resection was performed using techniques as described previously.Citation25,Citation26 Resectable disease was defined according to previously reported criteria as the possibility to completely remove all tumours while retaining a sufficient liver remnant to maintain postoperative liver function, as assessed by the surgical team.Citation26 Pringle’s manoeuvre was routinely used with a clamp/unclamp time of 10 min/5 min. RFA was performed using a previously described technique under real-time ultrasound guidance.Citation27 For patients with multiple tumours, all lesions were treated in one single session. The evaluation of the complete ablation of lesions after RFA was performed by dynamic computed tomography (CT) at 4 weeks after treatment. Complete ablation was diagnosed when a low-density area in both the arterial and portal venous phases was observed and the size of the area was larger than the lesion before treatment.Citation28
Follow-Up
Patients were followed carefully after the initial treatment. Follow-up examinations included laboratory tests (including serum AFP, liver function, and blood tests), abdominal ultrasonography, and contrast-enhanced CT every 3 months for the first 2 years and every 6 months thereafter. All patients with HBV-related HCC who were prepared for treatment for their HCC were counselled by a hepatologist for antiviral therapy regardless of the serum HBV DNA result.Citation29 The follow-up start date was the date of the initial diagnosis of HCC. The end of follow-up was the time of the last follow-up (December 2020) or death.
Statistical Analysis
Overall survival (OS) was calculated from the date of the initial diagnosis of HCC until death or the end of the follow-up period. Disease-free survival (DFS) was defined as the interval between the operation and the date of diagnosis of the first recurrence or the last follow-up. Comparisons were made using unpaired Student’s t-test for continuous variables and the chi-square test for categorical variables. Survival was calculated using the Kaplan-Meier method, and comparisons between groups were made using the Log rank test. The Cox regression model was used to identify independent predictors of survival. The concordance index (C-index) method was used to rank the different inflammation-based scores based on their capacity to discriminate patients according to the outcome. To avoid overoptimistic results, the prognostic performance of all inflammation-based scores was further validated in an independent external validation cohort. The statistical analysis was performed using IBM SPSS v.24.0 (SPSS, Armonk, NY, USA) and R 2.13.2 (http://www.r-project.org/). All statistical tests were 2-tailed, and a p value less than 0.05 was considered significant.
Results
Patient Characteristics
In the primary cohort, a total of 533 (74.4%) patients underwent hepatic resection, and 183 (25.6%) patients underwent RFA. In the validation cohort, a total of 315 (71.3%) patients underwent hepatic resection, and 127 (28.7%) patients underwent RFA. For the primary cohort, 149 (20.8%) patients had an elevated CRP level (>10 mg/L), and 27 (3.8%) patients had hypoalbuminemia (<35g/L). A minority of patients were allocated to GPS 2 (5.9%), mGPS 2 (2.1%), NLR 1 (3.6%), PLR 2 (1.3%), PI 2 (1.8%), and PNI 1 (9.2%). A total of 409 (57.1%) patients were allocated to LCR 0, and 307 (42.9%) patients were allocated to LCR 1. The baseline characteristics of the primary cohort and the validation cohort are provided in . In addition, more surgery-related information for the primary cohort and the validation cohort are provided in Supplementary Table 2.
Table 1 Baseline Characteristics of the Patients in the Primary and Validation Cohorts
OS of the Primary and Validation Cohorts
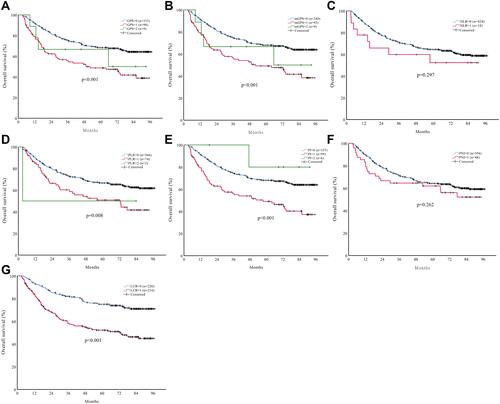
The median OS times for the primary and validation cohorts were 87.4 months (range, 3.2–128.2 months) and 68.9 months (range, 3.0–97.3 months), respectively. For the primary cohort, the 1-, 3-, and 5-year OS rates were 87.3%, 70.6%, and 63.5%, respectively. For the validation cohort, the 1-, 3- and 5-year OS rates were 89.1%, 71.1%, and 64.0%, respectively. The relationships between the inflammation-based scores and OS in the primary cohort are shown in . Elevated GPS, mGPS, PLR, PI, PNI, and LCR were associated with significantly reduced OS in the primary cohort (all P<0.05; except for NLR, P=0.244). However, some overlapping curves were still observed between GPS 1 and GPS 2, mGPS 1 and mGPS 2, PLR 1 and PLR 2, and PI 1 and PI 2 (). Interestingly, the LCR score identified two groups of patients with significantly different OS rates in the primary cohort (1-, 3- and 5-year OS rates and median OS: 92.9%, 81.9%, 73.3% and 99.2 months) for LCR score =0 (n=409) and (1-, 3- and 5-year OS rates and median OS: 79.8%, 56.6%, 49.7% and 69.1 months; P<0.001) for LCR score =1 (n=307; ). Importantly, these findings were supported by the validation cohort ().
Figure 1 The relationship between the inflammation-based scores and overall survival in HCC patients in the primary cohort: (A) GPS, (B) mGPS, (C) NLR, (D) PLR, (E) PI, (F) PNI and (G) LCR.
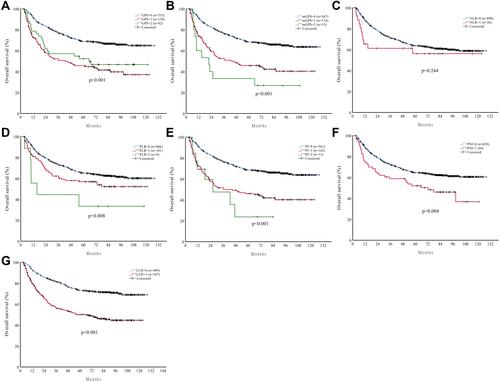
Figure 2 The relationship between the inflammation-based scores and overall survival in HCC patients in the validation cohort: (A) GPS, (B) mGPS, (C) NLR, (D) PLR, (E) PI, (F) PNI and (G) LCR.
Prognostic Factors in the Primary and Validation Cohorts
For the primary cohort, univariate analysis showed that white blood cell (WBC) count, albumin, CRP, AFP, ALBI score, tumour size, tumour number, macrovascular invasion, treatment, TNM stage, GPS, mGPS, PLR, PI, PNI, and LCR score were associated with OS (). Multivariate analysis showed that only AFP (hazard ratio (HR) 1.53, 95% confidence interval (CI): 1.19–1.96; P=0.001), ALBI score (HR 1.62, 95 CI: 1.24–2.10; P<0.001), tumour size (HR 1.36, 95% CI: 1.01–1.85; P=0.044), TNM stage (HR 2.42, 95% CI: 1.83–3.20; P<0.001), and LCR score (HR 1.63, 95% CI: 1.25–2.13; P<0.0001) were independently associated with OS (). For the validation cohort, the twelve factors correlated with survival in univariate analysis are reported in . The independent prognostic factors identified by multivariate analysis were AFP (HR 1.72, 95% CI: 1.25–2.37; P=0.001), tumour size (HR 1.56, 95% CI: 1.06–2.28; P=0.023), TNM stage (HR 1.98, 95% CI: 1.39–2.82; P<0.001), and LCR score (HR 1.89, 95% CI: 1.34–2.67; P<0.0001).
Table 2 Univariate and Multivariate Analyses of Prognostic Factors for OS in the Primary Cohort
Table 3 Univariate and Multivariate Analyses of Prognostic Factors for OS in the Validation Cohort
The LCR Score Predicts Prognosis in Subgroups of HCC Patients with Different Disease States
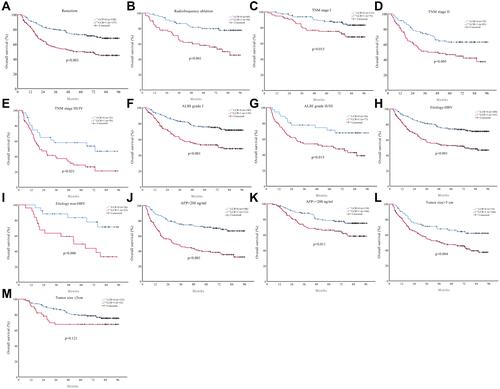
We further verified the predictive ability of the LCR score in HCC patients with different disease states. Kaplan–Meier curves were generated for the LCR score in the primary cohort for HCC patients with different treatment allocations (resection or RFA), TNM stages, ALBI grades, aetiologies (HBV/non-HBV), AFP levels (≤200 ng/mL/>200 ng/mL), and tumour sizes (≤5 cm/>5 cm) (). When the patients were stratified according to different disease states, the LCR score could still differentiate patients into two groups with distinct OS (all P<0.005, and ). In addition, these results were confirmed in the validation cohort ( and ). Next, we further verify the LCR score’s ability to predict DFS. The LCR score could still differentiate patients into two groups with distinct DFS in HCC patients with different disease states (Supplementary Figure 1). These results were also confirmed in the validation cohort (Supplementary Figure 2).
Table 4 LCR Score Predicts OS in Subgroups of HCC Patients with Different Disease States
Figure 3 The prognostic significance of the LCR score in HCC patients with different disease states in the primary cohort: (A) resection, (B) radiofrequency ablation, (C) TNM stage I, (D) TNM stage II, (E) TNM stage III/IV, (F) ALBI grade I, (G) ALBI grade II/III, (H) aetiology-HBV, (I) aetiology-non-HBV, (J) AFP>200 ng/mL, (K) AFP≤200 ng/mL, (L) tumour size≤5 cm, and (M) tumour size>5 cm.
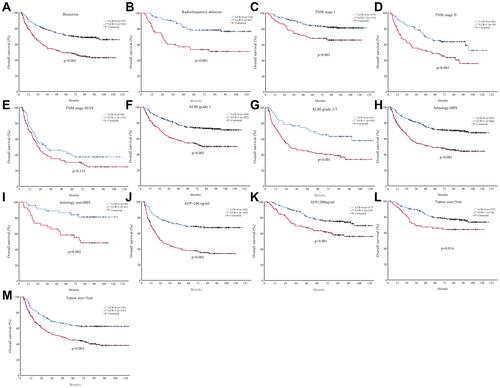
Figure 4 The prognostic significance of the LCR score in HCC patients with different disease states in the validation cohort: (A) resection, (B) radiofrequency ablation, (C) TNM stage I, (D) TNM stage II, (E) TNM stage III/IV, (F) ALBI grade I, (G) ALBI grade II/III, (H) aetiology-HBV, (I) aetiology-non-HBV, (J) AFP>200 ng/mL, (K) AFP≤200 ng/mL, (L) tumour size≤5 cm, and (M) tumour size>5 cm.
Comparison of the LCR Score with Other Commonly Used Inflammation-Based Scores
We next used the C-index to determine which inflammation-based scores performed best in predicting the survival of HCC patients treated with curative intent. The LCR scores consistently had higher C-index values (0.621) than the other scoring systems (0.503–0.590) for HCC in the primary cohort (). We found similar results in the validation cohort ().
Table 5 Concordance Index for the Comparison of Different Inflammation-Based Scores in the Primary and Validation Cohorts
Discussion
The identification of a simple and useful scoring system that is predictive of the prognosis of patients with HCC before treatment is an important objective. Our study is the first to report and validate that the preoperative LCR score was an independent prognostic risk factor for HCC patients treated with curative intent, independent of liver function, tumour characteristics, and treatment allocation. All findings were reproducible in a second independent validation cohort. These results will facilitate further clinical research on the importance of systemic inflammation for the prognosis of HCC patients.
HCC is biologically very heterogeneous.Citation30,Citation31 It has also been shown that even for patients in early stages, those who undergo radical treatment have different outcomes.Citation4–Citation6 To date, a few studies have used highly sophisticated gene expression analyses to analyse the complex molecular signatures of HCC to distinguish its heterogeneity and prognosis.Citation32,Citation33 However, these analyses are currently expensive and have unreliable repeatability; thus, they have not been widely used in clinical practice. Therefore, there is an urgent need for an easily determinable, simple, widely applicable, low-tech, and inexpensive marker from blood that can identify patients with very dismal prognostic features despite treatment.Citation34 In this study, subgroup analyses with respect to TNM stage, treatment allocation, and ALBI grade supported the prognostic relevance of LCR independent of the disease state. In fact, the present study showed that TNM stage II patients with low LCR scores had a similar median OS as TNM stage I patients with high LCR scores (). Similar results were found in comparing TNM stage III/IV patients with low LCR scores and TNM stage II patients with high LCR scores. Even more surprisingly, ALBI grade I/II patients who had low LCR scores virtually had better OS rates than patients with ALBI grade I who had high LCR scores (). These findings are of key clinical relevance since the LCR score identified subgroups with different prognoses within a defined TNM stage or ALBI grade and different treatment allocations. Moreover, lymphocyte and CRP determination are inexpensive, reproducible, objective, widely available, and routinely performed in clinical practice and does not rely on invasive tissue collection. The reproducibility of our results was verified in two independent data sets, further supporting the reliability of the LCR score as a prognostic marker for HCC patients. In addition, a recent meta-analysis data provided evidence that transarterial chemoembolization+RFA offer comparable oncologic outcomes in patients with HCC as compared with resection and with added benefit of lower morbidity.Citation35 Whether the LCR score have a predictive value in combination therapy needs further investigation.
Accumulating studies have demonstrated the potential of various types of systemic inflammatory factors as prognostic markers for determining oncological outcomes in human malignancies.Citation19,Citation20,Citation36 Notably, there is evidence that the inflammatory field effect, reflected by elevated CRP, may be directly involved in tumour progression, which could explain its prognostic significance in HCC.Citation37–Citation39 Several risk factors are currently known be associated with HCC recurrence, including inflammation-related factors.Citation7 However, the question of whether aggressive tumour behaviour prompts a prognostically detrimental inflammatory reaction or whether inflammation per se drives tumour progression remains to be elucidated.Citation9,Citation12 Our study revealed that high LCR score is significantly associated with aggressive and invasive factors (AFP, tumor size, tumor number, macrovascular invasion) and with high early recurrence of HCC patients as well (Supplementary Table 3). For all this, further preclinical studies in HCC are needed to elucidate the causal mechanisms of LCR in HCC progression.
There were a few potential limitations in this study. First, although we evaluated the preoperative LCR score in a large, multicentre cohort of patients with HCC, this was a retrospective study. Furthermore, another major limitation was that our three data sets included patients with HCC in an HBV-endemic area. It will certainly be necessary to validate the LCR score in other geographic regions to extend our results to patients with HCC of various aetiologies.
In conclusion, our study identified the LCR score as a novel, non-invasive, inexpensive, objective, available, and widely applicable prognostic marker for patients with HCC, irrespective of tumour stage, liver function and treatment allocation, and the LCR score was superior to other inflammation-based scores in terms of its prognostic ability. The LCR score may help surgeons determine surgical risk and oncological risk, thus facilitating the appropriate perioperative and postoperative management of patients with HCC.
Disclosure
The authors report no conflicts of interest in this work.
Additional information
Funding
References
- Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
- Forner A, Reig M, Bruix J. Hepatocellular carcinoma. Lancet. 2018;391(10127):1301–1314. doi:10.1016/S0140-6736(18)30010-2
- Heimbach JK, Kulik LM, Finn RS, et al. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology. 2018;67(1):358–380. doi:10.1002/hep.29086
- Poon RT, Fan ST, Lo CM, Liu CL, Wong J. Long-term survival and pattern of recurrence after resection of small hepatocellular carcinoma in patients with preserved liver function: implications for a strategy of salvage transplantation. Ann Surg. 2002;235(3):373–382. doi:10.1097/00000658-200203000-00009
- Shim JH, Jun MJ, Han S, et al. Prognostic nomograms for prediction of recurrence and survival after curative liver resection for hepatocellular carcinoma. Ann Surg. 2015;261(5):939–946. doi:10.1097/SLA.0000000000000747
- Chan AWH, Zhong J, Berhane S, et al. Development of pre and post-operative models to predict early recurrence of hepatocellular carcinoma after surgical resection. J Hepatol. 2018;69(6):1284–1293. doi:10.1016/j.jhep.2018.08.027
- Imamura H, Matsuyama Y, Tanaka E, et al. Risk factors contributing to early and late phase intrahepatic recurrence of hepatocellular carcinoma after hepatectomy. J Hepatol. 2003;38(2):200–207. doi:10.1016/S0168-8278(02)00360-4
- Hanahan D, Weinberg RA. Hallmarks of cancer: the next generation. Cell. 2011;144(5):646–674. doi:10.1016/j.cell.2011.02.013
- Mantovani A, Allavena P, Sica A, Balkwill F. Cancer-related inflammation. Nature. 2008;454(7203):436–444. doi:10.1038/nature07205
- Grivennikov SI, Greten FR, Karin M. Immunity, inflammation, and cancer. Cell. 2010;140(6):883–899. doi:10.1016/j.cell.2010.01.025
- Crusz SM, Balkwill FR. Inflammation and cancer: advances and new agents. Nat Rev Clin Oncol. 2015;12(10):584–596. doi:10.1038/nrclinonc.2015.105
- Greten FR, Grivennikov SI. Inflammation and cancer: triggers, mechanisms, and consequences. Immunity. 2019;51(1):27–41. doi:10.1016/j.immuni.2019.06.025
- Shedda S, Kosmider S, Faragher I, Jones I, Gibbs P. A critical review of the Glasgow prognostic score for colorectal cancer. Ann Surg. 2008;247(6):1087–1088; author reply 1088. doi:10.1097/SLA.0b013e3181758df1
- Hirashima K, Watanabe M, Shigaki H, et al. Prognostic significance of the modified Glasgow prognostic score in elderly patients with gastric cancer. J Gastroenterol. 2014;49(6):1040–1046. doi:10.1007/s00535-013-0855-5
- Halazun KJ, Hardy MA, Rana AA, et al. Negative impact of neutrophil-lymphocyte ratio on outcome after liver transplantation for hepatocellular carcinoma. Ann Surg. 2009;250(1):141–151. doi:10.1097/SLA.0b013e3181a77e59
- Koh CH, Bhoo-Pathy N, Ng KL, et al. Utility of pre-treatment neutrophil-lymphocyte ratio and platelet-lymphocyte ratio as prognostic factors in breast cancer. Br J Cancer. 2015;113(1):150–158. doi:10.1038/bjc.2015.183
- Kasymjanova G, MacDonald N, Agulnik JS, et al. The predictive value of pre-treatment inflammatory markers in advanced non-small-cell lung cancer. Curr Oncol. 2010;17(4):52–58. doi:10.3747/co.v17i4.567
- Pinato DJ, North BV, Sharma R. A novel, externally validated inflammation-based prognostic algorithm in hepatocellular carcinoma: the prognostic nutritional index (PNI). Br J Cancer. 2012;106(8):1439–1445. doi:10.1038/bjc.2012.92
- Proctor MJ, Morrison DS, Talwar D, et al. A comparison of inflammation-based prognostic scores in patients with cancer. A Glasgow Inflammation Outcome Study. Eur J Cancer. 2011;47(17):2633–2641. doi:10.1016/j.ejca.2011.03.028
- Kinoshita A, Onoda H, Imai N, et al. Comparison of the prognostic value of inflammation-based prognostic scores in patients with hepatocellular carcinoma. Br J Cancer. 2012;107(6):988–993. doi:10.1038/bjc.2012.354
- Okugawa Y, Toiyama Y, Yamamoto A, et al. Lymphocyte-C-reactive protein ratio as promising new marker for predicting surgical and oncological outcomes in colorectal cancer. Ann Surg. 2019.
- Lu LH, Zhong C, Wei W, et al. Lymphocyte-C-reactive protein ratio as a novel prognostic index in intrahepatic cholangiocarcinoma: a Multicentre Cohort Study. Liver Int. 2021;41(2):378–387. doi:10.1111/liv.14567
- Okugawa Y, Toiyama Y, Yamamoto A, et al. Lymphocyte-to-C-reactive protein ratio and score are clinically feasible nutrition-inflammation markers of outcome in patients with gastric cancer. Clin Nutr. 2019;39(4):1209–1217. doi:10.1016/j.clnu.2019.05.009
- European Association for the Study of the Liver. Electronic address EEE, European Association for the Study of the L. EASL clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol. 2018.
- Zhang YF, Zhou J, Wei W, et al. Intermediate-stage hepatocellular carcinoma treated with hepatic resection: the NSP score as an aid to decision-making. Br J Cancer. 2016;115(9):1039–1047. doi:10.1038/bjc.2016.301
- Shi M, Guo RP, Lin XJ, et al. Partial hepatectomy with wide versus narrow resection margin for solitary hepatocellular carcinoma: a prospective randomized trial. Ann Surg. 2007;245(1):36–43. doi:10.1097/01.sla.0000231758.07868.71
- Peng ZW, Zhang YJ, Chen MS, et al. Radiofrequency ablation with or without transcatheter arterial chemoembolization in the treatment of hepatocellular carcinoma: a prospective randomized trial. J Clin Oncol. 2013;31(4):426–432. doi:10.1200/JCO.2012.42.9936
- Lim HK, Choi D, Lee WJ, et al. Hepatocellular carcinoma treated with percutaneous radio-frequency ablation: evaluation with follow-up multiphase helical CT. Radiology. 2001;221(2):447–454. doi:10.1148/radiol.2212010446
- Wong JS, Wong GL, Tsoi KK, et al. Meta-analysis: the efficacy of anti-viral therapy in prevention of recurrence after curative treatment of chronic hepatitis B-related hepatocellular carcinoma. Aliment Pharmacol Ther. 2011;33(10):1104–1112. doi:10.1111/j.1365-2036.2011.04634.x
- Villanueva A, Llovet JM, Groszmann RJ, Iwakiri Y, Taddei TH. Impact of intra-individual molecular heterogeneity in personalized treatment of hepatocellular carcinoma. Hepatology. 2012;56(6):2416–2419. doi:10.1002/hep.26124
- Kim DY, Han KH. Staging for hepatocellular carcinoma in light of tumor heterogeneity: time to change or update? Hepatology. 2018;67(6):2076–2078. doi:10.1002/hep.29748
- Nault JC, De Reynies A, Villanueva A, et al. A hepatocellular carcinoma 5-gene score associated with survival of patients after liver resection. Gastroenterology. 2013;145(1):176–187. doi:10.1053/j.gastro.2013.03.051
- Utsunomiya T, Shimada M, Imura S, Morine Y, Ikemoto T, Mori M. Molecular signatures of noncancerous liver tissue can predict the risk for late recurrence of hepatocellular carcinoma. J Gastroenterol. 2010;45(2):146–152. doi:10.1007/s00535-009-0164-1
- Shelat VG. Role of inflammatory indices in management of hepatocellular carcinoma-neutrophil to lymphocyte ratio. Ann Transl Med. 2020;8(15):912. doi:10.21037/atm-2020-90
- Gui CH, Baey S, D’Cruz RT, Shelat VG. Trans-arterial chemoembolization + radiofrequency ablation versus surgical resection in hepatocellular carcinoma - A meta-analysis. Eur J Surg Oncol. 2020;46(5):763–771. doi:10.1016/j.ejso.2020.01.004
- Sieghart W, Pinter M, Hucke F, et al. Single determination of C-reactive protein at the time of diagnosis predicts long-term outcome of patients with hepatocellular carcinoma. Hepatology. 2013;57(6):2224–2234. doi:10.1002/hep.26057
- Hashimoto K, Ikeda Y, Korenaga D, et al. The impact of preoperative serum C-reactive protein on the prognosis of patients with hepatocellular carcinoma. Cancer. 2005;103(9):1856–1864. doi:10.1002/cncr.20976
- Yang J, Wezeman M, Zhang X, et al. Human C-reactive protein binds activating Fcgamma receptors and protects myeloma tumor cells from apoptosis. Cancer Cell. 2007;12(3):252–265. doi:10.1016/j.ccr.2007.08.008
- She S, Jiang L, Zhang Z, et al. Identification of the C-reactive protein interaction network using a bioinformatics approach provides insights into the molecular pathogenesis of hepatocellular carcinoma. Cell Physiol Biochem. 2018;48(2):741–752. doi:10.1159/000491903