
Abstract
Purpose
The aim of this review was to assess the efficacy of cannabis preparations for relieving pain in patients with malignant diseases, through a systematic review of randomized controlled trials (RCTs), which were predominantly double-blind trials that compared cannabis preparation to a placebo.
Methods
An electronic search of all literature published until June 2017 was made in MEDLINE/PubMed, Embase, The Cochrane Controlled Trials Register and specific web pages devoted to cannabis.
Results
Fifteen of the 18 trials demonstrated a significant analgesic effect of cannabinoids as compared to placebo. The most commonly reported adverse effects were generally well tolerated, mild to moderate. The main side effects were drowsiness, nausea, vomiting and dry mouth. There is evidence that cannabinoids are safe and modestly effective in neuropathic pain and also for relieving pain in patients with malignant diseases. The proportion of “responders” (patients who at the end of 2 weeks of treatment reported ≥30% reduction in pain intensity on a scale of 0–10, which is considered to be clinically important) was 43% in comparison with placebo (21%).
Conclusion
The target dose for relieving pain in patients with malignant diseases is most likely about 10 actuations per day, which is about 27 mg tetrahydrocannabinol (THC) and 25 mg cannabidiol (CBD), and the highest approved recommended dose is 12 actuations per day (32 mg THC/30 mg CBD). Further large studies of cannabinoids in homogeneous populations are required.
Introduction
Pain is a disagreeable sensorial and emotional experience that subjects associate with tissue damage and impairs quality of life.Citation1 Effective therapeutic options for patients living with different forms of pain are limited. Opioids and anti-inflammatory drugs as first-line medications for the treatment of pain in patients with malignant diseases do not always give satisfactory results.
In traditional medicine, cannabis preparations have been used for thousands of years to treat disease or alleviate symptoms, but their efficacy for specific indications is not clear. Clinical use of cannabinoid substances is restricted, due to legal and ethical reasons, as well as limited evidence showing benefits. The medical use of cannabis is attractive to patients suffering from malignant diseases. However, scientific justification or positive experience of the use of cannabis in patients with malignant diseases has only been found for the following indications: alleviation of sickness, nausea and vomiting associated with the use of cytotoxic therapy, pain relief and stimulation of appetite (treatment of cachexia). Pain relief is the most commonly cited reason for the medical use of cannabis.Citation2–Citation5
Mechanism of action of cannabinoids
Cannabinoids bind to cannabinoid receptors and act as agonists. Cannabinoid receptors are cell membrane receptors, members of the G protein-coupled receptors. They are activated by three major groups of ligands: endocannabinoids, plant cannabinoids and synthetic cannabinoids. Four subtypes of these receptors have been identified. Two have been cloned (CB1 and CB2 cannabinoid receptors),Citation6,Citation7 while the other two, WIN and abnormal-cannabidiol (abn-CBD) receptors, have been characterized pharmacologically.Citation8–Citation11
The analgesic effect of cannabinoids as a result of binding of cannabinoids to cannabinoid receptors has been confirmed, and the role of the endocannabinoid system in pain relief has been verified in various types of pain: somatic, visceral and neuropathy.Citation12 Classical analgesics, nonsteroidal anti-inflammatory drugs or opioids, paracetamol and antidepressants (with an analytical effect in some conditions) increase the activity of the endocannabinoid system.Citation12
The discovery of the endocannabinoid system and the development of animal models with different forms of pain have recently demonstrated the synergism between the opiate and cannabinoid systems.Citation12 There is a large amount of preclinical data in animal models on the analgesic effect of cannabinoids, predominantly Δ9-tetrahydrocannabinol (THC), nabilone and dronabinol, or combinations of THC and cannabidiol (CBD) and some other synthetic cannabinoids; and analgesic effects in the treatment of cancer-related pain without serious side effects have been shown.Citation13–Citation15
In humans, pharmacodynamic studies have demonstrated the effect of cannabinoids on provoked somatic pain (e.g., thermal stimulation), capsaicin-induced hyperalgesia, painful spasms in patients with multiple sclerosis (MS), and neuropathic pain in HIV/AIDS patients.Citation12,Citation26–Citation28,Citation30
Available cannabinoid analgesic agents
Two finished drug products – nabilone (Cesamet) and dronabinol (Marinol) – have been approved in many countries for the “prevention/treatment of chemotherapy induced nausea and vomiting”.Citation15 The only pharmaceutical industry drug product carrying the cannabinoid therapeutic principle with regulatory approval (in some countries) for pain relief in patients with malignant diseases is nabiximols (Sativex spray). Sativex® (GW Pharmaceuticals, Cambridge, UK) is an oromucosal cannabis-based spray combining a CB1 partial agonist (THC) with a cannabinoid system modulator (CBD).Citation16,Citation17 It was approved by Health Canada in June 2005 for prescription for central neuropathic pain in MS, and in August 2007, it was additionally approved for the treatment of cancer pain, as an adjuvant analgesic in adults with advanced malignancy, who, despite the highest tolerated opioid dose, still feel moderate to severe chronic pain.Citation18
In randomized controlled trials (RCTs), Sativex was adjunctively added to optimal drug regimens in patients with intractable symptoms, those often termed “untreatable”. The recommended maximum is 12 daily doses (32.4 mg THC and 30 mg CBD).Citation12 Data on the analgesic effect of nabiximols in malignant patients are shown primarily as an illustration of the effects of different ratios of THC/CBD.
Approved ongoing clinical trials
An investigational new drug (IND) application to study Sativex in advanced clinical trials in the USA was approved by the FDA in January 2006 in patients with intractable cancer pain.Citation15
Recently, the European Medicine Agency (EMEA) approved two double-blind, placebo-controlled safety and efficacy studies of Sativex as adjunctive therapy to opiates: the first one in pediatric patients from 8 to less than 18 years of age with cancer-related pain and the second one in pediatric patients from birth to less than 8 years of age with cancer-related pain (decision number P/0298/2014, PIP number EMEA-000181-PIP02-13). The completion date of the pediatric investigation plan is by July 2026.Citation19
On February 17, 2016, orphan designation (EU/3/16/1621) was granted by the European Commission to GW Pharmaceuticals, for THC and CBD from extracts of Cannabis sativa for the treatment of glioma.Citation20
Methods
An electronic search of all literature published until June 2017 was made in MEDLINE/PubMed, Embase, The Cochrane Controlled Trials Register and specific web pages devoted to cannabis. A systematic review of literature identified RCTs, evaluating the efficacy of cannabinoids in various chronic pain conditions that are not related to malignant diseases (including MS and HIV/AIDS neuropathies), compared with placebo and sometimes other active treatments.Citation21–Citation38 They demonstrated an analgesic effect of dronabinol, nabilone and natural THC and CBD in comparison with smoking marijuana. A detailed overview of preclinical and clinical data on the analgesic efficacy of cannabinoids is found in the document Health CanadaCitation2 and Ethnopharmacology.Citation39 Only three RTCs evaluated the efficacy of cannabinoids compard to placebo in various pain conditions that are related to malignant diseases.Citation40-Citation42 The studies selected were double-blind RTCs with a crossover or parallel design.
Selection criteria
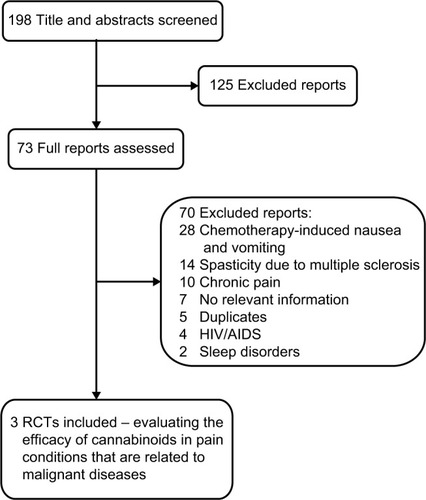
A systematic review of literature using the keywords cannabinoids, pain, malignant diseases, THC and RCTs identified 198 reports, of which 73 were potentially relevant RCTs, based on title and abstract screening. Seven of them had no relevant information obtained as full-text studies, five reports were duplicates (they contained data that had previously been published), 60 were in other clinical examinations (chemotherapy-induced nausea and vomiting, spasticity due to MS, sleep disorders and HIV/AIDS) and ten compared efficacy of cannabis for the treatment of chronic pain. Only three RCTs evaluated the efficacy of cannabinoids in pain conditions that are related to malignant diseases compared with synthetic THC and placebo ().Citation40–Citation42
Figure 1 Flow of studies through the review process.
Review of relevant research
In the intervention group, subjects were required to have received cannabis preparation, which at minimum contained the cannabinoids THC and CBD, applied by oral administration. Synthetic derivates of THC, such as dronabinol, nabilone or benzopyranoperidine, were likewise included. In the control group, subjects were required to have received a placebo treatment.Citation40–Citation42
The measure of efficacy chosen was the variable “intensity of pain” as scored by numeric analog scales. Patients at the end of 2 weeks of treatment reported ≥30% reduction in pain intensity on a scale of 0–10, which was considered as clinically important.
Double-blind, 2-week, multicenter RCT, placebo-controlled study
Respondents to the double-blind, 2-week, multicenter RCT, placebo-controlled studyCitation40 were adult patients with malignant diseases in terminal stage, who for at least a week used high (the most tolerated) doses of strong opiates, and despite this showed an intensity of pain ≥4 on a scale of 0–10.
For the treatment, patients were randomized into three groups. The first group received Sativex oral spray (nabixi-mols, 2.7 mg THC, 2.5 mg CBD per actuation) (n=60), the second group received THC as oral spray (2.7 mg THC per actuation) (n=58) and the third group received placebo spray (n=59). During the first week, the dose was titrated in patients based on tolerability and analgesia. The maximum permissible dose was 8 actuations in 3 hours (in intervals of at least 15 minutes between two doses) or at most 48 actuations for 24 hours (130 mg THC and 120 mg CBD).
The proportion of “responders” (patients who at the end of 2 weeks of treatment reported ≥ 30% reduction in pain intensity on a scale of 0–10, which is considered to be clinically important) in the Sativex group was 43% (statistically significantly compared with placebo; an improvement of −1.37 vs −0.69); in the THC group 23% (non-significant change compared with placebo; an improvement of −1.01 vs −0.69) and in the placebo group 21%.
Regarding side effects, in the Sativex group, 10/60 patients dropped out of treatment because of the side effects; in the second group where THC was orally administrated as spray, 7/58 patients dropped out of treatment because of the side effects and in the placebo group, 3/59 patients dropped out of treatment because of the side effects. The main side effects were drowsiness, nausea, vomiting and dry mouth.
Extension of the main double-blind, 2-week, multicenter RCT, placebo-controlled study
In 2013, an extension of the main study was opened.Citation28 A total of 39 patients with chronic pain due to malignant disease, who had been treated with opioids in a previous study but with an inadequate analgesic response, were involved in a new extended open, randomized, controlled, multicenter study for 2 weeks in which patients continued treatment with Sativex.Citation41 Doses remained unchanged. Of the 39 patients, 15 were treated for less than 2 weeks; others gradually withdrew from treatment during 1 year due to side effects (23/39), loss of efficacy (3/39) and a number of other reasons.
The study showed that the long-term use of THC/CBD spray is generally well tolerated without any loss of effect for pain relief because of long-term use. Moreover, patients who continued to use spray did not seek to increase the dose of spray or other medications for pain relief, suggesting that the adjuvant use of cannabinoids in cancer-related pain could be useful.
Multicenter, double-blind, placebo-controlled RCT, three different doses of Sativex
Respondents to this multicenter, double-blind, placebo-controlled RCT, with three different doses of Sativex,Citation42 were adult patients with malignant diseases in terminal stage, who for at least a week used high (the most tolerated) doses of strong opiates, and despite this showed an intensity of pain ≥4 on a scale of 0–10.
For treatment, patients were randomized to receive three different doses of Sativex: group 1 received 4 actuations per day (10.8 mg THC, 10 mg CBD) (n=91), group 2 received 10 actuations per day (27 mg THC, 25 mg CBD) (n=88) and group 3 received 16 actuations per day (43 mg THC, 40 mg CBD) (n=90). A group receiving THC as oral spray and placebo spray (n=90) was also included. During the first 7 days, the dose was gradually increased (from 1 to 4, 10 or 16) and then adjusted for the next 2 weeks. From the 21st to the 35th day, there was a 14-day evaluation period.
Patients who at the end of 2 weeks of treatment reported ≥30% reduction in pain intensity on a scale of 0–10 were considered clinically important.
The results showed that with increasing doses, several patients dropped out of treatment because of side effects: 3/91 placebo, 5/91 lowest dose, 6/88 medium dose and 20/90 highest dose. Overall, the share of those with ≥30% reduction in pain did not differ for Sativex vs placebo. However, in an analysis that evaluated the average daily pain score during 14 days, the lowest and midpoint doses were better than placebo.
There is no RTC for relief of pain in malignant diseases that evaluates “smoking marijuana” or some other herbal preparation consisting of natural THC and CBD, except Sativex.
Discussion
The natural and synthetic agonists of the cannabinoid receptors have shown positive therapeutic results in the treatment of various pathological conditions, including pain as an inevitable symptom of tissue damage. The antinociceptive and anti-hyperalgesic effect of cannabinoids at the peripheral and central levels has been demonstrated and confirmed in various models of acute and chronic pain.Citation43,Citation44
The adverse effects (AEs) of cannabinoids on the central nervous system (CNS) are associated with abnormal psychomotor behavior, short-term memory impairment and intoxication.Citation45
This review is prepared according to recommendations for systematic reviews.Citation46,Citation47 A systemic literature review identified more RCTs evaluating the efficacy of cannabinoids/cannabis in pain conditions, but only three double-blind controlled RTCs comparing the effectiveness of cannabinoids with synthetic THC and placebo in a variety of painful conditions that are associated with malignant disease.
In the first double-blind, 2-week multicenter RCT, placebo-controlled study,Citation40 the proportion of responders in the Sativex group was 43%, in the THC group was 23% and in the placebo group was 21%. Extension of the main double-blind, 2-week, multicenter RCT, placebo-controlled studyCitation41 in 2013 showed that long-term use of THC/CBD spray is generally well tolerated without any loss of effect for pain relief because of long-term use. A multicenter double-blind, placebo-controlled RCT, in which three different doses of Sativex were used,Citation42 showed that with increasing doses of THC/CBD, several patients dropped out of treatment because of side effects and those with ≥30% reduction in pain did not differ for Sativex vs placebo.
Thus, in two high-quality studies, the primary outcome of one can be regarded as positive and the other negative; however, both can be considered as evidence of the effectiveness of Sativex in specific painful conditions.
The inefficacy of the THC oral spray in one study, and variable results with relatively high doses of dronabinol, indicate that THC alone may not be sufficient for a good analgesic effect. This means that THC should be combined with CBD in order to achieve desire results.
Medicines that contain active ingredients that act as agonists of cannabinoid receptors are a promising therapeutic approach for treatment of various types of pain: neuropathic, inflammatory and oncological. This primarily refers to preparations containing exactly known similar amounts of THC and CBD, intended for the treatment of patients who do not respond to conventional therapy.Citation11,Citation41,Citation42
In the studies of Sativex in patients with malignant diseases and pain despite opioid therapy, the target dose is most likely about 10 actuations per day (the average number of actuations in one RCT was 9; in the second, the “successful” dose was 6–10 actuations per day), which is about 27 mg THC and 25 mg CBD, and the highest approved recommended dose is 12 actuations per day (32 mg THC/30 mg CBD). The dose is introduced gradually, from 1 to 4–6 actuations during the day, for 5–7 days.Citation12,Citation37
Conclusion
There is evidence, although limited, to support the use of cannabis pharmacotherapy in the treatment of different forms of pain in patients. If a patient with chronic pain and their healthcare provider work together through first- and second-line treatment modalities without success, a trial of cannabis or a cannabinoid may be a reasonable next step. With increased use of medical cannabis as pharmacotherapy for pain comes a need for comprehensive risk–benefit discussions that take into account the significant possible AEs of cannabis.
Numerous randomized clinical trials have demonstrated the safety and efficacy of Sativex in central and peripheral neuropathic pain, rheumatoid arthritis and cancer pain. Common AEs included dizziness, dry mouth, nausea, fatigue, somnolence, euphoria and vomiting.
The recommended daily dose for the treatment of pain is a maximum of 32.4 mg THC and 30 mg CBD. Data on the analgesic effect of nabiximols in patients with malignant diseases are shown primarily as an illustration of the effects of different ratios of the THC/CBD combination. The degree to which cannabinoid analgesics will be adopted in adjunctive pain management practices remains to be determined.
Further large studies of cannabinoids in homogeneous populations are required.
Author contributions
All authors contributed toward data analysis, drafting and critically revising the paper and agreed to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
- Classification of Chronic PainDescriptions of chronic pain syndromes and definitions of pain terms. Prepared by the International Association for the Study of Pain, Subcommittee on TaxonomyPain Suppl19863S1226 Available from: https://s3.amazonaws.com/rdcms-iasp/files/production/public/Content/ContentFolders/Publications2/Free-Books/Classification-of-Chronic-Pain.pdfAccessed March, 24, 20183461421
- BestrashniyJWintersKCVariability in medical marijuana laws in the United StatesPsychol Addict Behav20152963964226415061
- LightMKOrensALewandowskiBMarket size and demand for marijuana in ColoradoThe Marijuana Policy Group2014 Available from: http://www.cannabisconsumer.org/uploads/9/7/9/6/97962014/market_size_and_demand_study_july_9_2014%5B1%5D.pdfAccessed November 17, 2016
- IlgenMABohnertKKleinbergFCharacteristics of adults seeking medical marijuana certificationDrug Alcohol Depen2013132654659
- HillKPPalastroMDJohnsonBDitreJWCannabis and pain: a clinical reviewCannabis Cannabinoid Res2017219610428861509
- MatsudaLALolaitSJBrownsteinMJYoungACBonnerTIStructure of a cannabinoid receptor and functional expression of the cloned cDNANature19903465615642165569
- MunroSThomasKLAbu-ShaarMMolecular characterization of a peripheral receptor for cannabinoidsNature199336561657689702
- BreivogelCSGriffinGDi MarzoVMartinBREvidence for a new G-protein-coupled cannabinoid receptor in mouse brainMol Pharmacol20016015516311408610
- Di MarzoVBreivogelCSTaoQLevels, metabolism, and pharmacological activity of anandamide in CB1 cannabinoid receptor knockout mice, evidence for non-CB1, non-CB2 receptor-mediated actions of anandamide in mouse brainJ Neurochem2000752434244411080195
- HájosNLedentCFreundTFNovel cannabinoid sensitive receptor mediates inhibition of glutamatergic synaptic transmission in the hippocampusNeuroscience200110614
- ManzanaresJJulianMDCarrascosaARole of the cannabinoid system in pain control and therapeutic implications for the management of acute and chronic pain episodesCurr Neuropharmacol20064323925718615144
- Health Canada [webpage on the Internet]Information for health care professionalsCannabis (marihuana, marijuana) and the cannabinoidsHealth Canada2013 Available from: https://www.canada.ca/en/health-canada/services/drugs-health-products/medical-use-marijuana/information-medical-practitioners/information-health-care-professionals-cannabis-marihuana-marijuana-cannabinoids.htmlAccessed March, 24, 2018
- CridgeBJRosengrenRJCritical appraisal of the potential use of cannabinoids in cancer managementCancer Management Res20135301315
- McAllisterSDSoroceanuLDesperzPYThe antitumor activity of plant-derived non-psychoactive cannabinoidsJ Neuroimmune Pharmacol201510225526725916739
- AbramsDIGuzmanMCannabis in cancer careClin Pharmacol Ther20159757558625777363
- McPartlandJMRussoEBCannabis and cannabis extracts: greater than the sum of their parts?J Cannabis Therapeut20011103132
- RussoEBGuyGWA tale of two cannabinoids: the therapeutic rationale for combining tetrahydrocannabinol and cannabidiolMed Hypotheses2006662344616209908
- RussoEBCannabinoids in the management of difficult to treat painTher Clin Risk Manag20084124525918728714
- European Medicines Agency [webpage on the Internet]EMEA-001902-PIP01-15-M01 Available from: http://www.ema.europa.eu/ema/index.jsp?curl=pages/medicines/pips/EMEA-000181-PIP02-13/pip_001257.jsp&mid=WC0b01ac058001d129Accessed March, 24, 2018
- European Medicines Agency [webpage on the Internet]EU/3/16/1621 Available from: http://www.ema.europa.eu/ema/index.jsp?curl=pages/medicines/human/orphans/2016/04/human_orphan_001722.jsp&mid=WC0b01ac058001d12bAccessed March, 24, 2018
- WadeDTCollinCStottCDuncombePMeta-analysis of the efficacy and safety of Sativex (nabiximols) on spasticity in people with multiple sclerosisMult Scler20101670771420558502
- ZajicekJBallSWrightDEffect of dronabinol on progression in progressive multiple sclerosis (CUPID): a randomized, placebo-controlled trialLancet Neurol20131285786523856559
- BallSVickeryJHobartJThe cannabinoid use in progressive inflammatory brain disese (CUPID) trial: a randomized dobule-blind placebo-controlled parallel-group multicenter trial and economic evaluation of cannabinoids to slow progression in multiple sclerosisHealth Technol Assess20151912viiviiixxvxxxi1187
- CollinCDaviesPMutibokoIKRatcliffeSSativex Spasticity in MS Study GroupRandomized controlled trial of cannabis-based medicine in spasticity caused by multiple sclerosisEur J Neurol20071429029617355549
- CollinCEhlerEWaberzinekGA double-blind, randomized, placebo-controlled, parallel group study of Sativex in subjects with symptoms of spasticity due to multiple sclerosisNeurol Res20103245145920307378
- NotcuttWLangfordRDaviesPRatcliffeSPottsRA placebo-controlled, parallel-group randomized withdrawal study of subjects with symptoms of spasticity due to multiple sclerosis who are receiving long-term Sativex (nabiximols)Mult Scler20121821922821878454
- NovotnaAMaresJRatcliffeSA randomized, double-blind, placebo-controlled, parallel-group enriched-design study of nabiximols (Sativex) as add-on therapy in subjects with refractory spasticity caused by multiple sclerosisEur J Neurol2011181122113121362108
- WadeDTMakelaPRobsonPHouseHBatemanCDo cannabis-based medicinal extracts have general or specific effects on symptoms in multiple sclerosis? A double-blind, randomized, placebo-controlled study of 160 patientsMult Scler20041043444115327042
- ZajicekJFoxPSandersHCannabinoids for treatment of spasticity and other symptoms related to multiple sclerosis (CAMS study): multicenter randomized placebo-controlled trialLancet20033621517152614615106
- Corey-BloomJWolfsonTGamstASmoked cannabis for spasticity in multiple sclerosis: a randomized, placebo-controlled trialCMAJ20121841143115022586334
- RogDJNurmikkoTJFriedeTYoungCARandomized controlled trial of cannabis-based medicine in central pain in multiple sclerosisNeurology20056581281916186518
- PhillipsTJCCherryCLCoxSMarshallSJRiceASPharmacological treatment of painful HIV-associated sensory neuropathy: a systematic review and meta-analysis of randomized controlled trialsPlos One2010512e1443321203440
- AbramsDIHiltonJFLeiserRJShort-term effects of cannabinoids in patients with HIV-1 infection: a randomized placebo-controlled clinical trialAnn Intern Med200313925826612965981
- AbramsDIJayCAShadeSBCannabis in painful HIV-associated sensory neuropathyNeurology20076851552117296917
- EllisRJToperoffWVaidaFvan den BrandeGSmoked medicinal cannabis for neuropathic pain in HIV: a randomized, crossover clinical trialNeuropsychopharmacology20093467268018688212
- AshtonJCEmerging treatment options for spasticity in multiple sclerosis – clinical utility of cannabinoidsDeg Neurol Neuromusc Dis201111523
- LynchMECampbellFCannabinoids for treatment of chronic non-cancer pain; a systematic review of randomized trialsBr J Clin Phar-macol201172735744
- Martín-SánchezEFurukawaTATaylorJMartinJLSystematic review and meta-analysis of cannabis treatment for chronic painPain Med2009101353136819732371
- Ben AmarMCannabinoids in medicine: a review of their therapeutic potentialJ Ethnopharmacol200610512516540272
- JohnsonJRBurnell-NugentMLossignolDGanae-MotanEDPottsRFallonMTMulticenter, double-blind, randomized, placebo-controlled, parallel-group study of the efficacy, safety and tolerability of THC:CBD extract and THC extract in patients with intractable cancer-related painJ Pain Symptom Manage20103916717919896326
- JohnsonJRLossignolDBurnell-NugentMFallonMTAn open-label extension study to investigate the long-term safety and tolerability of THC/CBD oromucosal spray and oromucosal THC spray in patients with terminal cancer-related pain refractory to strong opioid analgesicsJ Pain Symptom Manage20134620721823141881
- PortenoyRKBanae-MotanEDAllendeSNabiximols for opioid-treated cancer patients with poorly-controlled chronic pain: a randomized placebo-controlled dose-graded trialJ Pain20121343844922483680
- IversenLChapmanVCannabinoids, a real prospect for pain relief?Curr Opin Pharmacol20022505511786308
- PertweeRGCannabinoid receptors and painProg Neurobiol20016356961111164622
- IversenLCannabis and the brainBrain20031261252127012764049
- HigginsJPTGreenSCochrane Handbook for Systematic Reviews of Interventions [webpage on the Internet]. Version 5.1.O (updated March 2011) Available from: http://handbook.cochrane.org/Accessed June 23, 2017
- Centre for Reviews and DisseminationSystematic Reviews: CRD’s Guidance for Undertaking Reviews in Health CareYork, UKUniversity of York2009 Available from: https://www.york.ac.uk/media/crd/Systematic_Reviews.pdfAccessed June 23, 2017