
Abstract
Objective
To report a rare case of spontaneous fusion (SF) following cervical disc arthroplasty (CDA), to review the related literature, and to propose a new measure to prevent it.
Methods
The course of a patient with SF is described here. The potential causes, risk factors, and preventive measure of SF after CDA published in previous studies have also been reviewed and discussed.
Results
A 63-year-old man presented with a 6-month history of progressive neck pain and developed left C-7 radiculopathy 4 years ago. Magnetic resonance imaging revealed disc herniation at the C6–C7 levels resulting in compression of the left C-7 nerve root. The patient underwent CDA at the C6–C7 levels, during which a PRESTIGE cervical disc device was implanted. He failed to follow-up regularly as recommended postoperatively because he was completely free from the pain in his neck and left upper limb. Four years later, he was readmitted with a 2-month history of occasional neck stiffness. Plain radiographs indicated complete radiographic fusion of the C6–C7 levels with trabecular bone bridging surrounding the cervical disc prosthesis, and dynamic imaging showed no motion. He was seen at regular follow-up visits for up to 60 months without special treatment, as his symptoms of neck stiffness were minor and his symptom has not worsened since then.
Conclusion
SF after CDA is a rare condition that can be attributed to patient- or prosthesis-related causes, and its risk factors are diverse. SF after CDA did not affect the patient’s clinical outcome, and no special treatment was required for it. Practitioners should be aware of this rare complication and advise patients of the risks before performing CDA.
Introduction
Anterior cervical discectomy and fusion (ACDF) has become the gold standard for treating degenerative cervical disc disease for the past decades.Citation1 However, some studies have shown that fusions limit the movement and alter the cervical spine biomechanics in the fused segment, which can result in the occurrence of adjacent segment disease (ASD).Citation2,Citation3 As a result, cervical disc arthroplasty (CDA) has emerged as an alternative treatment that may decrease the incidence of ASD through motion preservation.Citation4,Citation5 However, spontaneous fusion (SF), may also occur at the surgical segment as a rare complication of CDA.Citation6 Herein, we describe a rare case of SF following CDA and review related literature to identify its courses, risk factors, and preventive measures.
Case Report
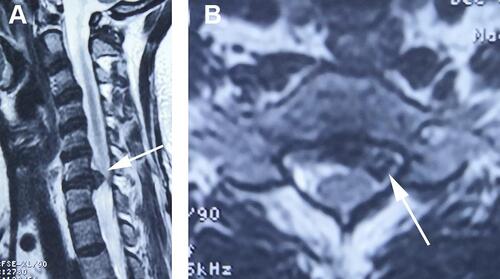
Four years ago, a 63-year-old man presented with a 6-month history of progressive neck pain and left C-7 radiculopathy. The physical examination revealed left upper limb hypesthesia and weakness (strength, 4/5). T2-weighted magnetic resonance imaging scans of the cervical spine revealed disc herniation at the C6–C7 levels resulting in compression of the left C-7 nerve root ().
Figure 1 Preoperative MRI. Sagittal (A) and axial (B) MRI scans revealed a C6–C7 disc herniation resulting in compression of the left C-7 nerve root (arrow).
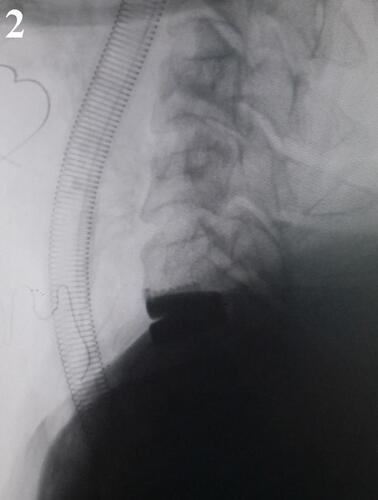
After conservative treatment failed, surgery was recommended for the patient. Cervical anterior discectomy at the C6–C7 levels was performed via a left-sided approach to avoid injury of the recurrent laryngeal nerve. After discectomy and amputation of the posterior longitudinal ligament, the C6–C7 intervertebral space was distracted and held by a Caspar distractor. An unambiguous and dissociative herniated disc penetrating the posterior longitudinal ligament was found and removed completely during the decompression process. A drill was used to drill and open the bone canals to prepare the endplates. Subsequently, a prosthesis cervical disc device (PRESTIGE disc prosthesis; Medtronic Sofamor Danek) was implanted at the C6–C7 level ().
Figure 2 Intraoperative fluoroscopy. A prosthesis cervical disc device was implanted at C6–C7.
Postoperatively, the patient failed to follow-up regularly as recommended, because he was completely free from pain in the neck and left upper limb, and the muscle strength of his left upper limb improved to normal immediately postoperatively. Four years later, he was readmitted with a 2-month history of occasional stiffness of the neck. Findings from the neurological examination were negative. Plain radiographs indicated complete osseous fusion of the C6–C7 levels with trabecular bone bridging surrounding the cervical disc prosthesis, and dynamic imaging showed no motion (), which was further confirmed by computed tomography (CT) (). We inferred that the patient had developed SF after CDA. He was seen at regular follow-up visits for up to 60 months without special treatment, as his symptoms of neck stiffness were minor and his symptom has not worsened since then. No specific radiological evidence of ASD in this patient was found at his last follow-up.
Figure 3 Plain radiographs obtained 4 years postoperatively. Lateral (A) imagings showed a complete radiographic fusion of the C6–C7 level with trabecular bone bridging surrounding the cervical disc prosthesis (arrows). No motion of C6–C7 was observed on flexion (B) and extension (C) imagings.
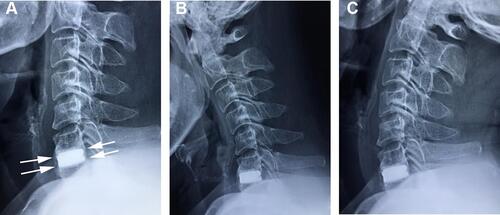
Figure 4 Computed tomography confirmed the cervical disc prosthesis was surrounded bone bridging (arrows).

Discussion
Considering the excellent surgical results, ACDF has become more popular over the past few decades for the treatment of degenerative cervical spondylosis.Citation1 However, during the long-term follow-up, it was found that ACDF increased the compensatory activity of adjacent segments due to lack of motion in the fused segments.Citation2 Excessive compensatory activity may result in ASD, which may require a second surgery.Citation3 As a result, CDA has emerged as an alternative that can not only achieve similar outcomes as that of ACDF but also reduce the incidence of ASD through motion preservation, which has been proved by many high-quality clinical studies.Citation5,Citation7,Citation8 Many biomechanical studies have shown that compared with ACDF, CDA can maintain normal range of motion, intradiscal pressure, and facet joint contact pressure.Citation9–Citation11
Heterotopic ossification (HO), the formation of bone outside the skeletal system, was first proposed and categorized in the field of hip or knee arthroplasty by McAfee et al in 2003,Citation12 and classification of HO after CDA was modified by Mehren et al in 2006.Citation13 Under this system, HO was divided into 5 classes (0-IV) according to the severity of ossification. Class IV indicates that bony fusion formation is present at the replacement segment and flexion and extension activities of the replaced segment are limited. SF is a complete bony ankylosis or fusion without movement of the CDA in active flexion and extension, and should be categorized as class IV HO. As a relatively rare complication of CDA, SF or class IV HO after CDA has been reported a few times since it was first reported in 2005.Citation14–Citation26
The exact incidence of SF after CDA is still unclear, and it varies greatly in the literature.Citation26 Oh et al reported that the incidence of SF after CDA was 3.3% (2/60).Citation27 However, Tu et al reported that its incidence was 1.9% (1/52).Citation26 This difference can be attributed to multiple factors. Some studies have identified a definite difference in the SF occurrence rate between different prosthetics types used in CDA.Citation21,Citation28 Moreover, detection tools may affect the incidence. Tu et al thought that CT was a more sensitive and accurate detector than plain radiography.Citation26 Some other researchers owed this difference to the dynamic progressive nature of HO partially, which means that it may increase over time.Citation29 Besides, the inter-observer error is also a factor that cannot be ignored.Citation28
The reasons for SF after CDA can be attribute to the result of patient- or prosthesis-related causes. With regard to the prosthesis-related causes, all cervical artificial discs can be divided into 3 categories according to its mechanism of motion: “constrained,” the device is within the physiological range of motion; “semiconstrained,” the device is outside of the normal range of motion; and “unconstrained,” the device has no mechanical stop.Citation21 Heary et al deemed that there was a strong association between the development of SF and degree of activity of the implanted prosthesis. If the motion of CDA is limited, then the artificial disc may behave like a cage and result in arthrodesis, so they thought that SF is more likely to occur with a constrained prosthesis.Citation14 Besides, mismatch between the prosthesis size and intervertebral space size is another prosthesis-related cause.Citation6 With respect to the patient-related causes, patients’ underlying diseases, such as diffuse idiopathic skeletal hyperostosis, may predispose them to bridging bone developing in a scenario in which progression to ossification would not have occurred in most individuals.Citation16
Several theories have been proposed to explain the risk factors of SF after CDA. Leung et al concluded that male sex and increased age were 2 possible risk factors for the development of SF.Citation19,Citation30 However, Yang et al showed that all factors including age, sex, body mass index, smoking, and alcohol were not associated with class IV HO.Citation31 Moreover, some surgical related factors are also considered as the risk factors, such as direct trauma to the longus colli, excessive drilling on the endplates and removal of bone, and bone dust and osteogenesis after endplate milling.Citation21,Citation23,Citation32 Among them, residual bone dust after endplate preparation was considered to be the most important factor by some researchers.Citation17
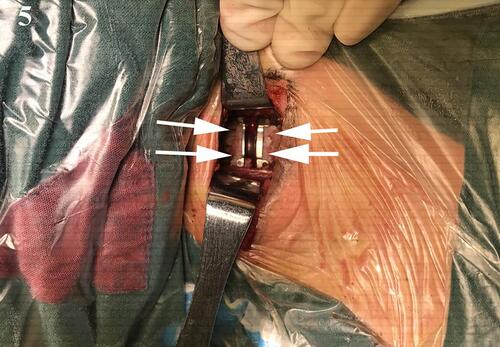
Lee et al thought that strict surgical indication for CDA was the first step to prevent HO formation and subsequent SF formation.Citation18 Osteophytes can usually be observed in patients with severe cervical degenerative disease, which may ultimately lead to arthrodesis between 2 adjacent vertebral bodies.Citation33 Thus, patients with osteophytes are not appropriate candidates for CDA. Leung et al recommended copious irrigation of the operative site with normal saline during milling and again before closure.Citation19 Additionally, it has been reported that radiation therapy and prophylactic use of non-steroidal anti-inflammatory drugs can decrease the incidence rates of HO after arthroplasty.Citation32 Moreover, Yang et al proposed that maximizing the implant-endplate interface can help to reduce high-grade HO and preserve motion.Citation23 We believe that residual bone and blood supply are the key factors in the formation of SF after CDA. In our case, we routinely irrigated the wound with copious saline to remove residual bone dust introduced during endplate milling, and used bone wax to seal the milled endplate stump and block the blood supply before closing the wound to prevent SF formation (). Before that, only 1 case of SF occurred, and after the routine protocol was in place, SF never happened again. This measure has never been reported before; we think it is a very effective way to prevent SF after CDA, and it should be used widely in the clinical setting.
Figure 5 The bone wax (arrows) was used to seal the milled endplate stump.
In our case, the occurrence of SF after CDA did not significantly affect the patient’s clinical outcome, except for limited range of motion at the index level, which was consistent with the conclusions of previously published literature.Citation14,Citation18,Citation31,Citation34 However, SF formation may increase the risk of ASD if fusion occurs at the surgical level.Citation23 A second surgery is only indicated when conservative treatment for cervical spondylosis due to ASD fails.Citation26 Our patient was satisfied with his clinical outcome, except for the occasional stiffness of his neck. So we just advised him to follow-up regularly. His symptom has not worsened since then, and no specific radiological evidence of ASD in this patient was found at his last follow-up.
Conclusion
SF after CDA is a rare condition that can be attributed to patient- or prosthesis-related causes, and its risk factors are diverse. In our case, SF after CDA did not affect the patient’s clinical outcome, and no special treatment was required for it. Practitioners should be aware of this rare complication and advise patients of the risks before performing CDA.
Abbreviations
CDA, cervical disc arthroplasty; ASD, adjacent segment disease; ACDF, anterior cervical discectomy and fusion; SF, spontaneous fusion; HO, heterotopic ossification.
Ethics and Consent Statement
This study was approved by the ethics committee of Xi’an Honghui Hospital and the patient has provided written informed consent for publication of the case details and accompanying images.
Acknowledgments
This work was supported by the National Natural Science Foundation of China (grant number 81830077). We would like to thank Yan-Sheng Huang for his help in writing the manuscript and Editage for English language editing.
Disclosure
The authors report no conflicts of interest in this work.
References
- Oliver JD, Goncalves S, Kerezoudis P, et al. Comparison of outcomes for anterior cervical discectomy and fusion with and without anterior plate fixation: a systematic review and meta-analysis. Spine. 2018;43(7):E413–E422. doi:10.1097/BRS.0000000000002441
- Donk RD, Verhagen WIM, Hosman AJF, Verbeek A, Bartels R. Symptomatic adjacent segment disease after anterior cervical discectomy for single-level degenerative disk disease. Clin spine Surg. 2018;31(1):E50–E54. doi:10.1097/BSD.0000000000000551
- Yan S-Z, Di J, Shen Y. Adjacent segment degeneration following anterior cervical discectomy and fusion versus the bryan cervical disc arthroplasty. Med Sci Monit. 2017;23:2692–2700. doi:10.12659/MSM.905178
- Lavelle WF, Riew KD, Levi AD, Florman JE. Ten-year outcomes of cervical disc replacement with the BRYAN cervical disc: results from a prospective, randomized, controlled clinical trial. Spine. 2019;44(9):601–608. doi:10.1097/BRS.0000000000002907
- Coric D, Guyer RD, Nunley PD, et al. Prospective, randomized multicenter study of cervical arthroplasty versus anterior cervical discectomy and fusion: 5-year results with a metal-on-metal artificial disc. J Neurol Neurosurg Spine. 2018;28(3):252–261. doi:10.3171/2017.5.SPINE16824
- Pointillart V, Castelain JE, Coudert P, Cawley DT, Gille O, Vital JM. Outcomes of the bryan cervical disc replacement: fifteen year follow-up. Int Orthop. 2018;42(4):851–857. doi:10.1007/s00264-017-3745-2
- Gornet MF, Lanman TH, Burkus JK, et al. Cervical disc arthroplasty with the Prestige LP disc versus anterior cervical discectomy and fusion, at 2 levels: results of a prospective, multicenter randomized controlled clinical trial at 24 months. J Neurol Neurosurg Spine. 2017;26(6):653–667. doi:10.3171/2016.10.SPINE16264
- Zou S, Gao J, Xu B, Lu X, Han Y, Meng H. Anterior cervical discectomy and fusion (ACDF) versus cervical disc arthroplasty (CDA) for two contiguous levels cervical disc degenerative disease: a meta-analysis of randomized controlled trials. Eur Spine J. 2017;26(4):985–997. doi:10.1007/s00586-016-4655-5
- Zhao X, Yuan W. Biomechanical analysis of cervical range of motion and facet contact force after a novel artificial cervical disc replacement. Am J Transl Res. 2019;11(5):3109–3115.
- Yu CC, Hao DJ, Huang DG, et al. Biomechanical analysis of a novel prosthesis based on the physiological curvature of endplate for cervical disc replacement. PLoS One. 2016;11(6):e0158234. doi:10.1371/journal.pone.0158234
- Yu CC, Liu P, Huang DG, Jiang YH, Feng H, Hao DJ. A new cervical artificial disc prosthesis based on physiological curvature of end plate: a finite element analysis. Spine J. 2016;16(11):1384–1391. doi:10.1016/j.spinee.2016.06.019
- McAfee PC, Cunningham BW, Devine J, Williams E, Yu-Yahiro J. Classification of heterotopic ossification (HO) in artificial disk replacement. J Spinal Disord Tech. 2003;16(4):384–389. doi:10.1097/00024720-200308000-00010
- Mehren C, Suchomel P, Grochulla F, et al. Heterotopic ossification in total cervical artificial disc replacement. Spine. 2006;31(24):2802–2806. doi:10.1097/01.brs.0000245852.70594.d5
- Heary RF, Goldstein IM, Getto KM, Agarwal N. Solid radiographic fusion with a nonconstrained device 5 years after cervical arthroplasty. J Neurol Neurosurg Spine. 2014;21(6):951–955. doi:10.3171/2014.8.SPINE14101
- Parkinson JF, Sekhon LH. Cervical arthroplasty complicated by delayed spontaneous fusion. Case report. J Neurol Neurosurg Spine. 2005;2(3):377–380. doi:10.3171/spi.2005.2.3.0377
- Bartels RH, Donk R. Fusion around cervical disc prosthesis: case report. Neurosurgery. 2005;57(1):E194; discussion E194. doi:10.1227/01.NEU.0000163419.59635.78
- Lee JH, Jung TG, Kim HS, Jang JS, Lee SH. Analysis of the incidence and clinical effect of the heterotopic ossification in a single-level cervical artificial disc replacement. Spine J. 2010;10(8):676–682. doi:10.1016/j.spinee.2010.04.017
- Lee SE, Chung CK, Jahng TA. Early development and progression of heterotopic ossification in cervical total disc replacement. J Neurol Neurosurg Spine. 2012;16(1):31–36. doi:10.3171/2011.8.SPINE11303
- Leung C, Casey AT, Goffin J, et al. Clinical significance of heterotopic ossification in cervical disc replacement: a prospective multicenter clinical trial. Neurosurgery. 2005;57(4):759–763. doi:10.1227/01.NEU.0000175856.31210.58
- Meisel HJ, Jurak L, Antinheimo J, et al. Four-year results of a prospective single-arm study on 200 semi-constrained total cervical disc prostheses: clinical and radiographic outcome. J Neurol Neurosurg Spine. 2016;25(5):556–565. doi:10.3171/2016.3.SPINE15810
- Mehren C, Wuertz-Kozak K, Sauer D, Hitzl W, Pehlivanoglu T, Heider F. Implant design and the anchoring mechanism influence the incidence of heterotopic ossification in cervical total disc replacement at 2-year follow-up. Spine. 2019;44(21):1471–1480. doi:10.1097/BRS.0000000000003098
- Chin KR, Pencle FJR, Mustafa LS, Mustafa MS, Quijada KA, Seale JA. Incidence of fusion across total disc replacement with heterotopic ossification: are ball and socket disk replacements fusing with and without radiographic evidence. Clin Spine Surg. 2019;32(10):E469–E473. doi:10.1097/BSD.0000000000000866
- Yang MMH, Ryu WHA, Casha S, DuPlessis S, Jacobs WB, Hurlbert RJ. Heterotopic ossification and radiographic adjacent-segment disease after cervical disc arthroplasty. J Neurol Neurosurg Spine. 2019;1:1–10.
- Dufour T, Beaurain J, Huppert J, Dam-Hieu P, Bernard P, Steib JP. Clinical and radiological evaluation of cervical disc arthroplasty with 5-year follow-up: a prospective study of 384 patients. Eur Spine J. 2019;28(10):2371–2379. doi:10.1007/s00586-019-06069-z
- Brenke C, Scharf J, Schmieder K, Barth M. High prevalence of heterotopic ossification after cervical disc arthroplasty: outcome and intraoperative findings following explantation of 22 cervical disc prostheses. J Neurol Neurosurg Spine. 2012;17(2):141–146. doi:10.3171/2012.4.SPINE12223
- Tu TH, Wu JC, Huang WC, et al. Heterotopic ossification after cervical total disc replacement: determination by CT and effects on clinical outcomes. J Neurol Neurosurg Spine. 2011;14(4):457–465. doi:10.3171/2010.11.SPINE10444
- Oh CH, Kim DY, Ji GY, et al. Cervical arthroplasty for moderate to severe disc degeneration: clinical and radiological assessments after a minimum follow-up of 18 months–Pfirrmann grade and cervical arthroplasty. Yonsei Med J. 2014;55(4):1072–1079. doi:10.3349/ymj.2014.55.4.1072
- Yi S, Kim KN, Yang MS, et al. Difference in occurrence of heterotopic ossification according to prosthesis type in the cervical artificial disc replacement. Spine. 2010;35(16):1556–1561. doi:10.1097/BRS.0b013e3181c6526b
- Yi S, Oh J, Choi G, et al. The fate of heterotopic ossification associated with cervical artificial disc replacement. Spine. 2014;39(25):2078–2083. doi:10.1097/BRS.0000000000000640
- Yi S, Shin DA, Kim KN, et al. The predisposing factors for the heterotopic ossification after cervical artificial disc replacement. Spine J. 2013;13(9):1048–1054. doi:10.1016/j.spinee.2013.02.036
- Yang X, Bartels R, Donk R, et al. Does heterotopic ossification in cervical arthroplasty affect clinical outcome? World Neurosurg. 2019;131:e408–e414. doi:10.1016/j.wneu.2019.07.187
- Li G, Wang Q, Liu H, Yang Y. Postoperative heterotopic ossification after cervical disc replacement is likely a reflection of the degeneration process. World Neurosurg. 2019;125:e1063–e1068. doi:10.1016/j.wneu.2019.01.244
- Park CK, Ryu KS. Are controversial issues in cervical total disc replacement resolved or unresolved?: A review of literature and recent updates. Asian Spine J. 2018;12(1):178–192. doi:10.4184/asj.2018.12.1.178
- Zhou HH, Qu Y, Dong RP, Kang MY, Zhao JW. Does heterotopic ossification affect the outcomes of cervical total disc replacement? A meta-analysis. Spine. 2015;40(6):E332–E340. doi:10.1097/BRS.0000000000000776