Abstract
Objective
We aimed to evaluate whether preoperative chemotherapy provides benefits in the survival and prognosis of patients with non-small cell lung cancer (NSCLC) in resectable stages I to IIIA, except T1N0.
Methods
In this randomized, controlled trial, 356 patients with stage I (except for T1N0), II and IIIA NSCLC were assigned to either the preoperative chemotherapy plus surgery arm (179 patients) or the primary surgery arm (177 patients). Both treatments were followed by adjuvant chemotherapy. The end point of this study included overall survival (OS), progression-free survival (PFS), and survival rate associated with clinical remission.
Results
Statistical survival difference was found between the preoperative chemotherapy plus surgery arm and the surgery-alone arm. However, the median survival time (MST) in the preoperative chemotherapy arm was lower than that of surgery-alone arm (MST, 45.42 months vs 57.59 months) (P = 0.016). When comparing the effect of preoperative chemotherapy at each stage of NSCLC, a statistical survival difference was found in stage II NSCLC but not in stage I and IIIA (MST 40.86 months vs 80.81 months) (P = 0.044). However, no statistically significant difference in PFS was noticed between the two arms, except for stage I NSCLC (hazard radio [HR] = 0.87; 95% CI, 0.561–1.629; P = 0.027). The survival rate was higher for patients who had clinical remission after preoperative chemotherapy, but the differences did not reach statistical significance (MST 42.10 months vs 35.33 months) (P = 0.630).
Conclusion
Preoperative chemotherapy did not show benefits in OS and PFS for stage I–IIIA NSCLC patients.
Introduction
As one of the leading causes of mortality throughout the world, non-small cell lung cancer (NSCLC) accounts for approximately 80% of the 1.18 million deaths from lung cancer each year.Citation1,Citation2 For patients with IB–IIIA stages of NSCLC, surgery is well recognized as the most effective treatment. However, 30% to 70% of patients who had tumor completely resected still experience relapse.Citation3,Citation4 Surgery followed by adjuvant chemotherapy is thus generally recommended to most patients with NSCLC. A meta-analysis in 1995 showed there was a 5% increase in 5-year survival with surgery followed by adjuvant chemotherapy compared with surgery alone (hazard ratio [HR], 0.87; P = 0.08).Citation5 The International Adjuvant Lung Cancer Trial (IALT), which included 1867 patients, has reported a significant overall survival (OS) benefit for adjuvant chemotherapy.Citation6 Preoperative chemotherapy also provides many benefits to cancer patients and is offered to shrink tumors before surgical resection, to eliminate micrometastases, and to assess chemotherapy response to identify patients who will potentially benefit from adjuvant chemotherapy.Citation7,Citation8 However, given conflicting results in the efficacy of preoperative chemotherapy from past clinical trials, the benefits of preoperative chemotherapy in NSCLC remain controversial. The latest meta-analysis evaluating preoperative chemotherapy in NSCLC, which included 3615 patients from 14 randomized, controlled trials (RCTs), showed that patients with stage IIIA NSCLC benefited the most from preoperative chemotherapy (B = −0.18; t = −5.25; P = 0.006),Citation9 although several independent trials did not show benefits of preoperative chemotherapy for NSCLC patients.Citation10
In this study, we analyzed the long-term results of a multicenter RCT to compare preoperative chemotherapy plus surgery vs surgery alone for patients with stage I to IIIA (except for T1N0) NSCLC.
Patients and methods
Patient selection
A total of 356 patients were enrolled in this trial from the Shanghai Chest Hospital, the Shanghai Pulmonary Hospital, and the Shanghai Huadong Hospital between February 1995 and October 2001. Eligible patients were required to have stage I (except for T1N0), II, or IIIA histologically confirmed NSCLC, according to the tumor-node-metastasis (TNM) classification. They had to be 75 years old or younger, have a Karnofsky performance score of 80 or higher, and have had curative surgical resection. Previous chemotherapy or radiotherapy was not allowed. Patients with other organic diseases were ineligible. Preinclusion investigations consisted of history and physical evaluation, chest X-ray, computed tomographic (CT) scan of the chest and brain, upper abdomen CT scan or ultrasound, and isotope bone scan.
The institutional review boards of the participating centers approved the protocols used in this study. All patients provided written, informed consent.
Treatments
Patients were randomly assigned into either a preoperative chemotherapy plus surgery group or a surgery-alone group. Patients from both groups received adjuvant chemotherapy after surgery.
The chemotherapy consisted of mitomycin (6 mg/m2), cisplatin (80 mg/m2), and vindesine (2.5 mg/m2) on day 1, 8, and 15. For both study arms, chemotherapy was repeated every 28 days for 4 cycles. In the preoperative chemotherapy arm, 1–2 cycles of chemotherapy treatment had to be completed before surgery. For both arms, 4–6 cycles of chemotherapy were given to patients after surgery. A physical examination and blood analyses were performed at each cycle during chemotherapy. Responses to chemotherapy were assessed according to the WHO criteria.
Surgery had to start after randomization in the surgery-alone arm and after chemotherapy in the preoperative chemotherapy arm. Upon completion of the preoperative chemotherapy treatment, all patients were assessed for their physical conditions before surgery. If patients’ physical conditions did not meet the requirement of surgery, the surgery was delayed until all parameters return to an acceptable level. Surgical resections (lobectomy, bilobectomy, or pneumonectomy) were performed on the basis of the chest CT scan. Mediastinal involvement was assessed by CT. Mediastinal node dissection and sampling were performed by surgeons and pathologists. Patients with pN2 stage NSCLC at surgery received postoperative thoracic radiotherapy.
Patients were followed up every 3 months until death or until the cut-off date of this study (May 1, 2012). The median follow-up period for patients in this trial was 53.7998 ± 48.7049 months.
Statistical analysis
The primary end points of this study included OS and progression-free survival (PFS). OS was defined as the time from the date of randomization to the date of death or May 1, 2012. PFS was calculated from the date of randomization to the time of disease progression, death, or May 1, 2012. The secondary end point was the survival rate associated with clinical remission.
The OS and PFS were computed by the Kaplan-Meier methodCitation11 and compared by the log-rank testCitation12 and the Cox proportional hazards model.Citation13 The multivariate Cox modelCitation13 was used to study variation in the OS and PFS according to major baseline characteristics (age, sex, stage, histology, and treatment). Statistical analyses were conducted using SPSS software, version 13.0 (SPSS, Inc, Chicago, IL, USA).
Results
A total of 356 patients were enrolled in this trial. 179 Patients were then randomly assigned to the preoperative chemotherapy arm, while 177 patients were assigned to the surgery-alone arm (). Reasons for ineligibility included stage IIIB tumor (one patient), incomplete resection (eight patients), and missing follow-up (ten patients). Thus, 169 patients in the preoperative chemotherapy arm and 168 patients in the surgery-alone arm were included in the final analysis. The baseline patient characteristics were not statistically different between the two arms ().
Figure 1 Patient enrollment and outcomes.
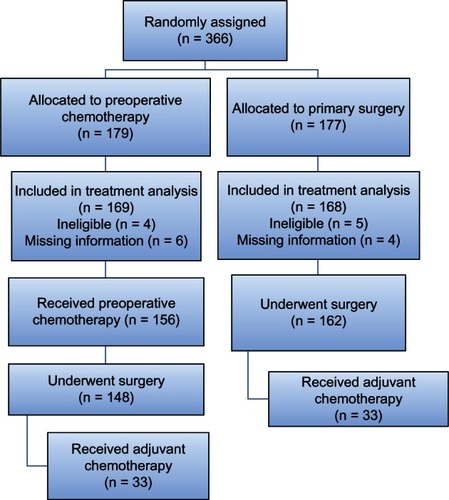
Table 1 Characteristics of the 337 patients, by treatment arm
Preoperative chemotherapy
In the preoperative chemotherapy arm, 156 patients completed all 4 cycles, and 13 patients were not evaluable, including six patients who refused to complete chemotherapy. Among the 169 patients who received chemotherapy, the overall chemotherapy response rate was 46.7% (79 patients), and progression of disease was observed in ten patients (5.9%). Chemotherapy-associated adverse events included grade 3 to 4 nausea and vomiting, grade 3 alopecia, grade 3 thrombocytopenia, and grade 3 to 4 neutropenia. After surgery, 83 patients from each arm received adjuvant chemotherapy.
Surgery
Surgery was performed in 310 patients (92%), including 148 patients (87.6%) in the preoperative chemotherapy arm and 162 patients (96.4%) in the surgery-alone arm. The proportions of patients who underwent lobectomy and pneumonectomy were not significantly different between the two arms (). A total of 19 patients (6.1%) died after surgery: eight patients (5.4%) in the preoperative chemotherapy arm and eleven patients (6.8%) in the surgery-alone arm. The postoperative deaths were mainly due to a complication from surgery or comorbidities. We did not observe any differences in term of postsurgery recovery between the preoperative chemotherapy and the control arms.
Table 2 Surgical procedures, by treatment arm
Overall survival
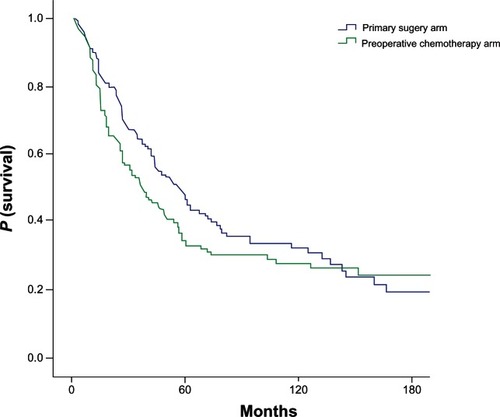
At the time that this trial ended on May 1, 2012, 261 patients had died, including 128 in the preoperative chemotherapy arm and 133 in the surgery-alone arm. Survival rates at 5, 10, and 15 years were 34%, 28%, and 24%, respectively in the preoperative chemotherapy arm and 48%, 33%, and 21%, respectively in the surgery-alone arm (). The median survival time (MST) was 45.42 months in the preoperative chemotherapy arm and 57.59 months in the surgery-alone arm (log-rank P = 0.016), with a HR of death of 1.67 (95% CI, 1.43–1.96). The influences of age, sex, stage, histology, and treatment were assessed by the Cox model. The only relevant factor was disease stage. When the log-rank test was stratified on stage, the survival rate of stage II NSCLC at 5, 10, and 15 years was 27%, 22%, and 22%, respectively in the preoperative chemotherapy arm and 48%, 33%, and 21%, respectively in the primary surgery arm. The MST of stage II NSCLC was 40.86 months in the preoperative chemotherapy arm and 80.81 months in the primary surgery arm (log-rank P = 0.044). There were not significant differences between the two arms in the survival rates of stage I and stage IIIA NSCLC (log-rank P = 0.734; log-rank P = 0.051, respectively).
Figure 2 Overall survival, by treatment arm.
Progression-free survival
No statistical difference in PFS was seen between the two arms, with a HR of progression of 1.135 (95% CI, 0.855–1.506). The median PFS time was 42.21 months in the preoperative chemotherapy arm and 45.67 months in the surgery-alone arm (log-rank P = 0.38). The HR of progression of stage I NSCLC was significantly lower in the preoperative chemotherapy arm when compared with the surgery-alone arm (HR = 0.87; 95% CI, 0.561–1.629; P = 0.027). The risks of progression or death of stage II and stage IIIA NSCLC were not significantly different between the two arms, with HR = 1.226 (95% CI, 0.687–2.186; P = 0.491) for stage II NSCLC and HR = 1.332 (95% CI, 0.877–2.023; P = 0.179) for stage IIIA NSCLC. After the multivariate Cox mode analysis, we found that the relevant factors of disease progression were age (HR = 1.012; 95% CI, 0.996–1.029; P = 0.012) and stage (HR = 1.241; 95% CI, 1.051–1.467; P = 0.011).
Survival associated with remission
Among the 169 patients in the preoperative chemotherapy arm, the clinical remission rate following preoperative chemotherapy was 40.8% (69 patients), including one patient with complete remission and 68 patients with partial remission. The 5-year survival rates were 38.48% and 35.03%, respectively in patients with clinical remission and without clinical remission. The MST was 42.10 months in patients with clinical remission and 35.33 months in patients without clinical remission (log-rank P = 0.630).
Survival associated with changes in clinical staging
Downstaging (clinical stage higher than the pathological stage) was found in 16 patients (9.5%), unchanged staging (clinical stage the same as the pathological stage) in 134 patients (79.3%), and upstaging (clinical stage lower than the pathological stage) in 19 patients (11.2%). There were significant beneficial effects of preoperative chemotherapy in the OS of patients who experienced clinical downstaging compared with the patients who did not experience clinical downstaging. In the downstaging vs unchanged vs upstaging groups, the 5-year survival rates were 44.14% vs 39.52% vs 14.04%, respectively, and the MST was 55.62 months vs 39.52 months vs 25.81 months, respectively (P = 0.03).
Discussion
This long-term follow-up trial demonstrated that preoperative chemotherapy did not produce benefits in the OS for stage I–IIIA NSCLC patients. There was no statistically significant difference in PFS between the two arms. A significant increase in PFS was demonstrated only in the stage I NSCLC patients in the preoperative chemotherapy arm.
Due to the inconsistent results from previous clinical trials, the benefit of preoperative chemotherapy in NSCLC has been long debated in the past decade. Similar to the result from our trial, several other trials have also shown that there are not benefits for NSCLC patients in having preoperative chemotherapy. Westeel et alCitation14 reported the long-term results of a French randomized trial that compared preoperative chemotherapy followed by surgery versus surgery alone in resectable (stage I to IIIA) NSCLC (n = 355). After a median 13.8 years of follow-up study, these authors concluded that preoperative chemotherapy did not produce a significant survival benefit, by univariate analysis, but did produce an improved survival in stage I and II, using multivariate analysis.Citation15 The randomized phase III trial reported by Pisters et alCitation16 compared preoperative chemotherapy using paclitaxel and carboplatin followed by surgery, with surgery alone in early-stage NSCLC patients. Although the OS and PFS were higher with preoperative chemotherapy treatment, the differences did not reach statistical significance.Citation16 In the European Organisation for Research and Treatment of Cancer 08012 multicenter randomized trial studied by Gilligan et al,Citation17 519 patients were randomized to receive either surgery alone or 3 cycles of platinum-based chemotherapy followed by surgery. The results of this trial failed to indicate the benefits of preoperative chemotherapy in terms of OS. Consistent with these previous studies, our study also demonstrated that preoperative chemotherapy does not produce significant benefits for NSCLC patients.
On the other side, many trials have demonstrated that preoperative chemotherapy is beneficial for NSCLC patients. A trial conducted by Rosell et alCitation8 assigned 60 patients with stage IIIA NSCLC to either have preoperative chemotherapy plus surgery or surgery alone. When an analysis was performed 7 years after patient enrollment, patients in the preoperative chemotherapy arm showed a significant gain in survival. The median survival of the preoperative chemotherapy arm (26 months) was dramatically longer than the surgery-alone arm (8 months) (P < 0.01). Roth et alCitation18,Citation19 conducted a similar trial using chemotherapy, consisting of cyclophosphamide, etoposide, and cisplatin. In that study, the benefit in OS to the preoperative arm was statistically significant (P < 0.008). Meta-analysis of randomized trials has also shown that preoperative chemotherapy improves survival in NSCLC patients. An updated meta-analysis of 13 RCTs, conducted by Song et al,Citation20 showed that preoperative chemotherapy significantly improved the OS of operable NSCLC patients, including patients with stage III NSCLC. However, the benefits of preoperative chemotherapy demonstrated in these trials appear to be modified by multiple factors, such as the number of enrolled patients, the differences between chemotherapy regimens, and the differences between the clinical and pathological stages.
The secondary objective of our trial was to assess the survival rate associated with clinical remission induced by preoperative chemotherapy. Although OS was higher with clinical remission after preoperative chemotherapy, the difference was not statistically significant, indicating preoperative chemotherapy was not beneficial to patients even when chemotherapy successfully acted on tumors.
There are several factors that may have affected the efficacy of preoperative chemotherapy in our trial. Because patients received at least 1–2 cycles of preoperative mitomycin-cisplatin-vindesine, chemotherapy toxicity may have been responsible for a shortened survival time in the preoperative chemotherapy arm compared with the surgery-alone arm. Furthermore, the mitomycin-cisplatin-vindesine regimen we used in this study is no longer considered to be the first-line chemotherapy regimen for NSCLC. We cannot exclude the possibility that the mitomycin-cisplatin-vindesine regimens may have been a factor that contributed to the negative effect of preoperative chemotherapy in the NSCLC patients. However, recent studies using the same chemotherapy regimen have demonstrated inconsistent results in the benefits of neoadjuvant chemotherapy in NSCLC, suggesting that the choice of chemotherapy regimen may not be a key factor in determining the efficacy of preoperative chemotherapy.Citation10,Citation16 Nevertheless, minimizing chemotherapy-related morbidity and mortality should be given careful consideration when designing future trials, and this may be achieved by choosing less toxic chemotherapy regimens than the one we chose for this trial.Citation21–Citation23
In summary, we found that preoperative chemotherapy had no survival benefits for NSCLC patients with stage I, II, and IIIA diseases. This finding emphasizes the need to develop new strategies to identify the patient subgroups that will be benefited or harmed by preoperative chemotherapy.
Acknowledgments
This study was supported by Shanghai Chest Hospital, Shanghai Pulmonary Hospital, and Shanghai Huadong Hospital. The authors thank all patients for study participation and the following study investigators.
Disclosure
The authors report no conflicts of interest in this work.
References
- ParkinDMBrayFFerlayJPisaniPGlobal cancer statistics, 2002CA Cancer J Clin20055527410815761078
- SchillerJHCurrent standards of care in small-cell and non-small-cell lung cancerOncology200161Suppl 1S3S13
- MountainCFRevisions of the International System for Staging Lung CancerChest19971116171017179187198
- GoldstrawPCrowleyJChanskyKInternational Association for the Study of Lung Cancer International Staging CommitteeParticipating InstitutionsThe IASLC Lung Cancer Staging Project. proposals for the revision of the TNM stage groupings in the forthcoming (seventh) edition of the TNM Classification of malignant tumoursJ Thorac Oncol20072870671417762336
- Non-Small Cell Lung Cancer Collaborative GroupNon-small Cell Lung Cancer Collaborative Group: chemotherapy in non-small cell lung cancer: a meta-analysis using updated data on individual patients from 52 randomised clinical trialsBMJ199531170108999097580546
- ArriagadaRBergmanBDunantALe ChevalierTPignonJPVansteenkisteJInternational Adjuvant Lung Cancer Trial Collaborative GroupCisplatin-based adjuvant chemotherapy in patients with completely resected non-small-cell lung cancerN Engl J Med2004350435136014736927
- FujitaSKatakamiNTakahashiYPostoperative complications after induction chemoradiotherapy in patients with non-small-cell lung cancerEur J Cardiothorac Surg200629689690116675259
- RosellRGómez-CodinaJCampsCA randomized trial comparing preoperative chemotherapy plus surgery with surgery alone in patients with non-small-cell lung cancerN Engl J Med199433031531588043059
- BozcukHAbaliHCoskunSLung Cancer Committee of Turkish Oncology GroupThe correlates of benefit from neoadjuvant chemotherapy before surgery in non-small-cell lung cancer: a metaregression analysisWorld J Surg Oncol201210116116622877422
- FelipERosellRMaestreJASpanish Lung Cancer GroupPreoperative chemotherapy plus surgery versus surgery plus adjuvant chemotherapy versus surgery alone in early-stage non-small-cell lung cancerJ Clin Oncol201028193138314520516435
- KaplanELMeierPNonparametric estimation from incomplete observationsJournal of the American Statistical Association195853282457481
- MantelNEvaluation of survival data and two new rank order statistics arising in its considerationCancer Chemother Rep19665031631705910392
- CoxDRRegression models and life tablesJournal of the Royal Statistical Society B1972342187220
- WesteelVMilleronBJQuoixEALong-term results of the French randomized trial comparing neoadjuvant chemotherapy followed by surgery versus surgery alone in resectable non-small cell lung cancer [Abstract]J Clin Oncol201028Suppl 157003
- KimAWBoffaDJWangZDetterbeckFCAn analysis, systematic review, and meta-analysis of the perioperative mortality after neoadjuvant therapy and pneumonectomy for non-small cell lung cancerJ Thorac Cardiovasc Surg20121431556322056364
- PistersKMVallièresECrowleyJJSurgery with or without preoperative paclitaxel and carboplatin in early-stage non-small-cell lung cancer: southwest Oncology Group Trial S9900, an intergroup, randomized, phase III trialJ Clin Oncol201028111843184920231678
- GilliganDNicolsonMSmithIPreoperative chemotherapy in patients with resectable non-small cell lung cancer: results of the MRC LU22/NVALT 2/EORTC 08012 multicentre randomised trial and update of systematic reviewLancet200736995771929193717544497
- RothJAFossellaFKomakiRA randomized trial comparing perioperative chemotherapy and surgery with surgery alone in resectable stage IIIA non-small-cell lung cancerJ Natl Cancer Inst19948696736808158698
- RothJAAtkinsonENFossellaFLong-term follow-up of patients enrolled in a randomized trial comparing perioperative chemotherapy and surgery with surgery alone in resectable stage IIIA non-small-cell lung cancerLung Cancer1998211169792048
- SongWAZhouNKWangWSurvival benefit of neoadjuvant chemotherapy in non-small cell lung cancer: an updated meta-analysis of 13 randomized control trialsJ Thorac Oncol20105451051620107424
- TomaszekSCWigleDASurgical management of lung cancerSemin Respir Crit Care Med2011321697721500126
- StamatelopoulosAZaragkasSSofoudisCNon-small cell lung cancer: the role of surgery after induction chemo and/or radiotherapyJ Buon201015221322020658712
- GadgeelSMThe optimal chemotherapy for stage III non-small cell lung cancer patientsCurr Oncol Rep201113427227921479993