
Abstract
Hepatitis C virus (HCV) was identified for the first time more than 20 years ago. Since then, several studies have highlighted the complicated aspects of this viral infection in relation to its worldwide prevalence, its clinical presentation, and its therapeutic response. Recently, two landmark scientific breakthroughs have moved us closer to the successful eradication of chronic HCV infection. First, response rates in treatment-naïve patients and in prior non-responders to pegylated-interferon-α and ribavirin therapy are increasing as a direct consequence of the development of direct-acting antiviral drugs. Secondly, the discovery of single-nucleotide polymorphisms near the interleukin 28B gene significantly related to spontaneous and treatment-induced HCV clearance represents a milestone in the HCV therapeutic landscape. The implementation of this pharmacogenomics finding as a routine test for HCV-infected patients has enhanced our understanding of viral pathogenesis, has encouraged the design of ground-breaking antiviral treatment regimens, and has become useful for pretreatment decision making. Nowadays, interleukin 28B genotyping is considered to be a key diagnostic tool for the management of HCV-infected patients and will maintain its significance for new combination treatment schemes using direct-acting antiviral agents and even in interferon-free regimens. Such pharmacogenomics insights represent a challenge to clinicians, researchers, and health administrators to transform this information into knowledge with the aim of elaborating safer and more effective therapeutic strategies specifically designed for each patient. In conclusion, the individualization of treatment regimens for patients with hepatitis C, that may lead to a universal cure in future years, is becoming a reality due to recent developments in biomarker and genomic medicine. In light of these advances, we review the scientific evidence and clinical implications of recent findings related to host genetic factors in the management of HCV infection.
Introduction
Modern therapeutics requires adequate drug prescription, which implies the selection of the correct drug, dose, and duration of administration. However, it has been reported that, in approximately 30%–60% of patients, drugs that are correctly prescribed cannot provide the desired outcome.Citation1
The consequence of a series of pharmacokinetic processes, which take place at dissimilar levels in different subjects, determines the pharmacological effects of the majority of drugs, the host genetic background being involved in this variability. In fact, the existence of genetic variants could alter the structure, function, and expression of most of the enzymes that are engaged in drug transport and metabolism or the particular drug receptors, so the phenotypic behavior of the patient can be predicted by genotyping, which sets the basis for pharmacogenomics studies.Citation2
Modifications of a single base in the nucleotide sequence, known as single-nucleotide polymorphisms (SNPs), are the most common variants and targets of pharmacogenetic tests. Although there are hundreds of thousands of SNPs, the kinetics or dynamics of drugs seem to be influenced by only a small minority of them.Citation3
Recently, a revolutionary era in scientific research has been established after the culmination of the Human Genome Project, and a new approach, ie, the genome-wide association study, represents its main success. Genetic factors strongly related to disease susceptibility and drug response are finally being identified as a result of the use of this modern high-throughput genotyping technology, which analyzes 300,000–900,000 SNPs in each sample.Citation4
Following the rise of the genomic era, the clinical and therapeutic management of many diseases, including even those of infectious origin, was expected to evolve. Nonetheless, up to the present, there are scarce examples of the use of such new data in routine clinical practice, hepatitis C virus (HCV) being one of the most encouraging cases.
The identification of key molecular biomarkers for HCV has brought understanding of the dissimilarities observed in disease progression and treatment response, helping us to comprehend the natural history of HCV, estimate the burden of infection, and develop preventive measures.Citation5–Citation9
These findings impact the prognosis and treatment of HCV infection. Further, the ability to identify patients with an unfavorable allele, in whom the response to treatment would be very poor, would spare some patients the side effects of standard treatment that is unlikely to be beneficial, thereby making them candidates for alternative emerging therapies.
Such pharmacogenomics insights represent a challenge for clinicians, researchers, and health administrators to transform this information into knowledge with the aim of elaborating safer and more effective therapeutic strategies specifically designed for each patient.
Similarly to what is observed in other areas of modern therapeutics, pharmacogenomics tests are acquiring a position in the treatment of infectious diseases. However, these analyses do not elucidate all of the variability in treatment response. Therefore, as the goal is to enhance the patient’s therapeutic experience, genetic and non-genetic information, such as sex, age, viral load, genotype, drug interactions, and clinical observations, must be merged in this modern paradigm of individualized HCV therapy in order to decide the most suitable treatment for a given patient.Citation10,Citation11
In this review, we summarize the scientific evidence and clinical implications of recent findings related to host genetic factors in the management of HCV infection.
Genetics of IL28B: impact and effect on treatment response in HCV patients
HCV was identified for the first time more than 20 years ago.Citation12 Since then, several studies have highlighted the complicated aspects of this viral infection in relation to its worldwide prevalence, its clinical presentation, and its response to therapy.Citation13–Citation17
With approximately 3% of the world population, that is, more than 170 million people, now infected, HCV is considered to be a major health problem. The clinical manifestations are varied, ranging from an asymptomatic self-limiting infection to liver cirrhosis and hepatocellular carcinoma, which are the main indications for liver transplantation in developed countries. As a consequence, the socioeconomic implications of the infection are enormous, and the burden of the disease is expected to intensify worldwide as the liver damage progresses in patients who acquired HCV many years earlier.Citation13
In spite of the high costs and substantial toxicity of pegylated-interferon-α and ribavirin (PEG-IFN-α/RBV) combination therapy, a sustained virological response (SVR), that is, undetectable HCV RNA in serum 6 months after treatment completion, can be obtained by less than 50% of patients infected with the most prevalent HCV genotype.Citation14 Despite the fact that direct-acting antiviral agents are expected to increase the response rate markedly, these new drugs must currently be administered in combination with PEG-IFN-α/RBV to help suppress viral breakthrough.Citation15
In addition, the achievement of SVR depends on several viral (eg, genotypes, viral load, mutations) and host (eg, age, sex, degree of liver fibrosis, alcohol consumption) factors. However, despite these influencing characteristics, a large proportion of the variability as well as the existence of ethnic disparities in treatment response cannot be completely explained. Therefore, it had been strongly suggested that host genetic risk factors might be also involved in the response of HCV to treatment.Citation16,Citation17
A few years ago, through the use of genome-wide association studies, four independent research groups analyzed the role of variation in host genetic markers in response to treatment with PEG-IFN-α/RBV for patients chronically infected with HCV genotype 1b.Citation5–Citation8 Despite the fact that patients from different ethnic origins (European, African American, Hispanic, Australian, and Japanese) were included in these studies, the definitive conclusion in all cases was that polymorphisms in or near the interleukin (IL) 28B gene, also known as interferon (IFN) lambda 3 (IFN-λ3 or IFNL3), on chromosome 19 significantly affect the response to HCV therapy. These SNPs are in high-linkage disequilibrium with each other, meaning that their variants are strongly related, so offer very similar genetic associations.
In fact, a response to PEG-IFN-α/RBV combination therapy in patients infected with HCV genotype 1b was significantly (P<7.1×10−08) more likely to occur in those with a particular genotype in the IL28B locus (rs12979860 CC or rs8099917 TT) than in patients with other IL28B variants.Citation5–Citation8 Such individuals were also more likely to spontaneously clear acute HCV infection without treatment.Citation9
As epidemiological studies have also demonstrated, these ground-breaking data confirmed that ethnicity is closely related to the response to treatment for HCV. The prevalence of these polymorphisms differs between ethnic groups,Citation9,Citation18 which could explain much of the recognized ethnic discrepancy in the frequency of SVR rates; for example, the treatment response rates in European (53%–85%), Asian (90%), and African-American (23%–55%) patients might be partly elucidated by the finding that the C allele of SNP rs12979860 is less prevalent among individuals of African descent than in those of European and Asian ancestry.Citation7,Citation9
The correlation between IL28B polymorphisms and therapeutic response was confirmed by various research groups and across different HCV genotypes,Citation19–Citation22 as well as in individuals coinfected with human immunodeficiency virus.Citation8,Citation23
Although on-treatment predictors, such as rapid virological response, defined as the lack of detection of HCV RNA in serum at the fourth week of treatment, are more precisely associated with therapeutic outcome,Citation24,Citation25 the IL28B SNP is considered the strongest pretreatment predictor of response.Citation26 This is explained by the fact that patients with the favorable IL28B genotype tend to have a higher initial baseline viral load, appear to eliminate the virus more efficiently at each time point of treatment, and, therefore, are more prone to achieving a rapid virological response.Citation7,Citation24,Citation26–Citation32
Recurrent HCV infection after liver transplantation is frequent and demands post-transplant antiviral treatment.Citation33–Citation35 In these patients, IL28B genotyping could also be beneficial to predict and control the risk of reinfection. It has been reported that a severe recurrence of HCV infection is more frequent among recipients with the unfavorable alleles, and that IL28B variants in donors and recipients are independently related to the post-transplant therapeutic response, indicating that donors with the favorable IL28B genotype might be more appropriate for HCV-infected patients.Citation34
IL28B gene family
The cytokines IL29, IL28A, and IL28B (also known as IFN-λ1, IFN-λ2, and IFN-λ3, respectively) are the three members of the type III IFN-λ family. In agreement with the knowledge that these cytokines act primarily as IFNs and not as ILs, the Human Genome Organization Gene Nomenclature Committee has changed the official symbols to IFNL1, IFNL2, and IFNL3, respectively.Citation36 The three IFN-λs, expressed at low levels by a wide array of human tissues, can be activated by viral infection and stimulate both innate and adaptive immune system pathways to fulfill their antiviral and antitumoral activity.Citation37,Citation38
While IFN-α and IFN-β is detected by the IFN receptor (IFNAR), IFN-λ is recognized by a heterodimer of the IL-10 and IFN-λ receptors (IL-10R2 and IFNλR1, respectively), which is tissue-dependent and expressed primarily in epithelial cells, liver tissue, and peripheral blood mononuclear cells.Citation39 However, both receptors trigger the Janus kinase-signal transducer and activator of transcription (JAK–STAT) pathway, activating a set of IFN-stimulated genes (ISGs) engaged in a wide range of antiviral and antiproliferative activities.Citation39–Citation41
Hypothetical role of IL28B SNP in response to PEG-IFN-α/RBV treatment
Evidence regarding the association between ISGs in the liver or peripheral blood mononuclear cells and IL28B genotype or response to IFN therapy is widely recognized by numerous studies. However, the biological pathways relating IL28B genetic variants to spontaneous and/or treatment-induced HCV clearance are still unknown.
When the innate immune system detects the presence of HCV RNA, mitochondrial antiviral-signaling protein stimulates expression and secretion of IFN-α, IFN-β, and IFN-λ. Cell surface receptors detect IFNs and trigger a signal cascade, stimulating a large number of ISGs that generate intracellular antiviral activity which eliminates viral replication.Citation42–Citation45
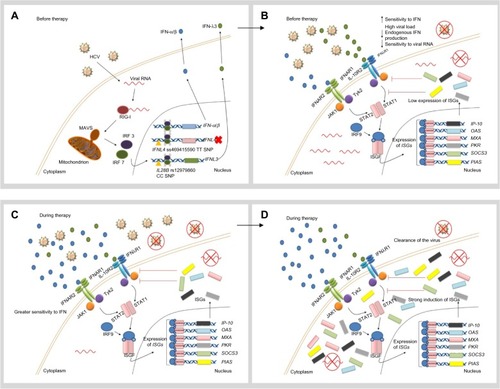
In individuals with the favorable IL28B allele (rs12979860 CC), low levels of IFN-λ and therefore weak ISG expression are observed. Despite the fact that this response might be enough to eliminate the virus at low viral loads, the cell is more sensitive to IFN and high viral loads can accumulate in the patient ().Citation46
Figure 1 Hypothetical role of favorable IL28B and IFNL4 genotypes in the response to IFN therapy.
Abbreviations: HCV, hepatitis C virus; IFN, interferon; IFIH1, IFN-induced helicase C domain-containing protein 1; IFNAR, IFN-α/β receptor 1; IFNL4, interferon lambda 4; L10R, IL-10 receptor; IL28B, interleukin 28B; IFNλR, IFNλ receptor; IP-10, IFN-γ-inducible protein 10; IRF, IFN regulatory factor; ISG, IFN-stimulated gene; ISGF, IFN-stimulated gene factor; JAK, Janus kinase; MAVS, mitochondrial antiviral-signaling protein; MXA, myxovirus resistance protein 1 (also known as MX1); OAS, 2′5′-oligoadenylate synthase; PIAS, protein inhibitor of activated STAT; PKR, protein kinase RNA-activated (also known as EIF2AK2); RIG-I, retinoic-acid inducible protein I; SNP, single-nucleotide polymorphism; SOCS3, suppressor of cytokine signaling 3; STAT, signal transducer and activator of transcription; Tyk2, tyrosine kinase 2.
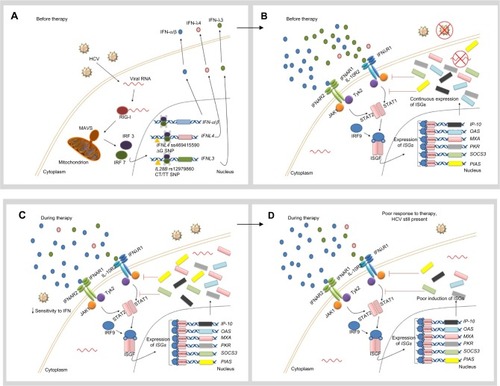
Constant induction of the IFN signaling pathway in the presence of the virus seems to be a common characteristic in patients with the unfavorable genotypes (rs12979860 CT/TT). In spite of higher baseline ISG expression levels, virus elimination is not possible, due to the fact that IFN-inhibitory molecules (SOCS3 [suppressor of cytokine signaling 3] and PIAS [protein inhibitor of activated STAT]) at the same time activate a negative regulation of the JAK-STAT pathway. Consequently, the cell is less sensitive to IFN, which means that the hepatocyte is not only unable to eliminate the virus but also lacks the ability to stimulate more powerful ISG expression when exogenous IFN-α is provided during treatment ().Citation47
Figure 2 Hypothetical role of unfavorable IL28B and IFNL4 genotypes in the response to IFN therapy.
Abbreviations: HCV, hepatitis C virus; IFIH1, IFN-induced helicase C domain-containing protein 1; IFNAR, IFN-α/β receptor 1; IFNL4, interferon lambda 4; IL10R, IL-10 receptor; IL28B, interleukin 28B; IFNλR, IFNλ receptor; IP-10, IFN-γ-inducible protein 10; IRF, IFN regulatory factor; ISG, IFN-stimulated gene; ISGF, IFN-stimulated gene factor; JAK, Janus kinase; MAVS, mitochondrial antiviral signaling protein; MXA, myxovirus resistance protein 1 (also known as MX1); OAS, 2′5′-oligoadenylate synthase; PIAS, protein inhibitor of activated STAT; PKR, protein kinase RNA-activated (also known as EIF2AK2); RIG-I, retinoic-acid inducible protein I; SNP, single-nucleotide polymorphism; SOCS3, suppressor of cytokine signaling 3; STAT, signal transducer and activator of transcription; Tyk2, tyrosine kinase 2.
When IFN-α therapy is administered, various possibilities might occur depending on the IL28B genotype. The development of a more vigorous therapeutic response and successful viral elimination can be detected in patients with the favorable IL28B allele (rs12979860 CC), as a consequence of unrestrained IFN signal transduction and strong ISG stimulation ().Citation46
Conversely, exogenous IFN-α is not able to stimulate ISG expression strongly enough to clear the virus in individuals with unfavorable genotypes (rs12979860 CT/TT). Therefore, the patient exhibits a poor therapeutic response ().Citation46
Extensive studies of the genetic region around the IFNL3 gene have recently revealed the existence of a novel gene, ie, the IFNL4 gene, which shows a dinucleotide variant (rs368234815 or ss469415590 TT/ΔG) in linkage disequilibrium with rs12979860.Citation48 Interestingly, the full-length protein is only expressed in patients with the ΔG allele, whereas the TT allele creates a frame shift in the gene that inactivates protein expression ( and ).Citation48 In humans, the TT allele is strongly and positively associated with spontaneous or treatment-induced HCV clearance. Thus, in the context of HCV infection, disruption of the IFNL4 gene is beneficial for humans, although the reason for this remains unclear.Citation48,Citation49
Like the other three members of the IFN-λ family, this new type III IFN binds to the same heterodimeric receptor and activates the JAK-STAT pathway. Moreover, it exhibits strong antiviral activity in vitro. However, unlike the majority of IFNs, IFN-λ4 protein is poorly secreted (), and it is hypothesized that it might block IL-10R2/IFNλR1 receptor binding for the remaining IFN-λs, thus impairing HCV clearance.Citation36
Moreover, it was determined that, in peripheral blood mononuclear cells, ss469415590 (but not rs12979860) is responsible for the stimulation of IL28B and IFN-γ-inducible protein 10 messenger RNA, high plasma levels of which have been also shown to be related to a poor therapeutic response in chronically infected HCV patients.Citation49 These observations offer a new understanding into the genetic mechanism of HCV clearance and have a strong and direct impact on the clinical management of HCV infection.
Other host genetic polymorphisms in the HCV treatment response
Although the influence of IL28B on HCV infection and treatment have been reviewed by numerous studies since publication of the landmark papers, it has been shown that SNPs at other genes could also be involved in HCV treatment susceptibility and the risk of drug-related toxicities.Citation50
Inosine triphosphatase
PEG-IFN-α/RBV therapy is associated with several treatment-limiting adverse effects. One of the most important is RBV-induced hemolytic anemia, which motivates withdrawal of HCV therapy in about 15% of patients.Citation51 In a recent genome-wide association study, it was concluded that the reduction in hemoglobin detected after 4 weeks of treatment is significantly associated with the genotypes of SNP rs6051702. The gene locus responsible for RBV-induced hemolytic anemia is in the inosine triphosphatase gene on chromosome 20, which encodes inosine triphosphate pyrophosphohydrolase, a protein that hydrolyses inosine triphosphate to its monophosphate derivative.Citation52 Two functional variants are involved in the reported association, ie, a missense variant in exon 2 (rs1127354) and a splice-altering SNP in intron 2 (rs7270101), which lead to inosine triphosphate pyrophosphohydrolase deficiency, a benign red cell enzymopathy characterized by accumulation of inosine triphosphate in erythrocytes and related to a protective effect against RBV-induced hemolytic anemia in HCV genotype 1-infected patients receiving PEG-IFN-α/RBV or telaprevir-based triple therapy.Citation53–Citation56
It is important to note that although related to a decreased risk of hemolytic anemia, patients carrying polymorphisms encoding reduced predicted inosine triphosphate pyrophosphohydrolase activity are more prone to develop thrombocytopenia.Citation57 Moreover, recent reports show that, in addition to a better prediction of anemia, RBV dose reduction, and need for erythropoietin, inosine triphosphatase deficiency is also associated with SVR in patients infected with HCV genotypes 1/4 or 2/3.Citation58,Citation59
Low-density lipoprotein cholesterol receptor gene
A higher plasma low-density lipoprotein (LDL) cholesterol level is an independent predictor of an SVR to PEG-IFN-α/RBV, and a genetic variant of the LDL cholesterol receptor gene (LDLR), an SNP located in the 3′ UTR region of the LDLR gene, has been shown to predict an SVR to PEG-IFN-α/RBV therapy in chronic HCV, as well as in patients coinfected with human immunodeficiency virus/HCV.Citation60,Citation61 Moreover, the LDLR and IL28B genotypes seem to have a synergistic effect on SVR.Citation62 Given that LDLR is one of the putative HCV receptors, both IL28B and LDLR genotypes could interact to regulate the life cycle of HCV.Citation62,Citation63 For this reason, combined use of both LDLR and IL28B genotypes is more potent in improving the prediction of SVR than separate analysis of these allelic variants.
Vitamin D receptor
Although IL28B variants are the strongest predictors of the response to PEG-IFN-α/RBV, recent data suggest that vitamin D may also be an important determinant of response to treatment.Citation60 A correlation between 25-OH vitamin D deficiency and non-response to PEG-IFN-α/RBV therapy has been observed.Citation64 Therefore, genetic variations of the vitamin D receptor offer a possibility to analyze further the effects of vitamin D on the outcome of HCV therapy.Citation65,Citation66
Impact of HCV pharmacogenomics on patient-focused perspectives
When compared with the general population or patients with chronic hepatitis B, patients with chronic HCV infection usually have lower health-related quality of life.Citation67 In particular, injecting drug users infected with HCV appear to have a lower health-related quality of life when compared with patients infected via blood transfusions.Citation67,Citation68
It has been reported that HCV infection rates are at least five times higher among patients with severe mental illness and that the prevalence of psychiatric and substance use disorders is more frequent among HCV-infected patients when compared with the general population. In fact, this correlation represents an obstacle to the therapeutic and clinical management of this infection.Citation69 Interestingly, other studies have indicated that another factor related to reduced health-related quality of life is awareness of the HCV infection per se.Citation68
While successful PEG-IFN-α/RBV treatment appears to ameliorate health-related quality of life, it is usually affected and declines during the therapeutic course as a consequence of severe side effects, such as RBV-induced hemolytic anemia.Citation70,Citation71 Moreover, a significant increase in psychiatric and substance abuse disorders during HCV antiviral treatment regimens has been reported, even in patients with no prior history.Citation72 As a result, HCV patients suffering from psychiatric disorders are less likely to be eligible for therapeutic schemes, thus increasing the morbidity and mortality rates in these individuals.Citation73
Interestingly, a recent Japanese study was the first to confirm that low health-related quality of life before treatment is significantly associated with SVR to PEG-IFN-α/RBV therapy.Citation74 Chronic HCV infection not only decreases quality of life in patients with the disease, but also represents a major public health burden.
As mentioned earlier, IL28B genotype testing could be useful to detect those patients who are less likely to adhere to treatment or to respond to it; therefore, it could be part of a cost-effective strategy that also improves individual outcomes and quality of life, as it would be able to decrease treatment-associated morbidity and costs.Citation75 For example, offering patients with favorable IL28B genotypes a shorter, lower-cost regimen with PEG-IFN-α/RBV, followed by direct-acting antiviral agents for those with unfavorable variants or those who relapse, could be more cost-effective than treating all patients initially with regimens that include direct-acting antiviral agents.Citation75,Citation76
In addition, since antiviral treatment is lengthy and often complicated, IL28B prediction may encourage patients with favorable genotypes to start therapy or to continue with their personalized treatment regimens. The number of therapeutic possibilities will increase in the near future, but IL28B genotyping will still be useful for optimization of treatment algorithms.
Conclusion
Knowledge related to host genetic factors represents a milestone in the treatment of HCV from a clinical and research point of view. In the coming years, the development of new and effective drugs included in quadruple or IFN-free regimens might eclipse the influence of IL28B. However, its genotyping will still be a useful tool to predict treatment outcome and may help to make decisions regarding adequate treatment schemes, especially for prior non-responding patients.
Moving forward, the major challenge will lie in effective interpretation of this new knowledge in clinical practice, which will need the commitment of patients, clinicians, researchers, health administrators, and the pharmaceutical industry. The main goal will be an ideal treatment for chronic HCV infection, which must be efficacious, simple, safe, and well tolerated, and also of short duration and cost-effective. The aim of personalized health care may now be one step closer for HCV-infected patients.
Acknowledgments
This work is supported by grants from the Instituto de Ciencias Básicas y Medicina Experimental, the La Fundación para el Desarrollo de las Ciencias Básicas, and the Italian Hospital of Buenos Aires Research Bureau.
Disclosure
The authors report no conflicts of interest in this work.
References
- WangLMcLeodHLWeinshilboumRLGenomics and drug responseN Engl J Med2011364121144115321428770
- WeinshilboumRMWangLPharmacogenetics and pharmacogenomics: development, science and translationAnnu Rev Genomics Hum Genet2006722324516948615
- International HapMap ConsortiumA haplotype map of the human genomeNature200543770631299132016255080
- ThurszMYeeLKhakooSUnderstanding the host genetics of chronic hepatitis B and CSemin Liver Dis201131211512721538279
- SuppiahVMoldovanMAhlenstielGInterleukin 28B is associated with response to hepatitis C interferon-alpha and ribavirin therapyNat Genet200941101100110419749758
- TanakaYNishidaNSugiyamaMGenome-wide association of interleukin 28B with response to interferon alpha and ribavirin therapy for chronic hepatitis CNat Genet200941101105110919749757
- GeDFellayJThompsonAJGenetic variation in interleukin 28B predicts hepatitis C treatment-induced viral clearanceNature2009461726239940119684573
- RauchAKutalikZDescombesPSwiss Hepatitis C Cohort Study and Swiss HIV Cohort StudyGenetic variation in interleukin 28B is associated with chronic hepatitis C and treatment failure: genome-wide association studyGastroenterology201013841338134520060832
- ThomasDLThioCLMartinMPGenetic variation in IL28B and spontaneous clearance of hepatitis C virusNature2009461726579880119759533
- RedalMBellosoWHGarfiIScibonaPIsolabellaSPharmacogenomics in gastroenterologySanoudouDClinical Applications of PharmacogeneticsRijeka, CroatiaIn Tech2012
- BellosoWHRedalMAPharmacogenomics and the path towards personalized medicineMedicina (B Aires)201070326527420529779
- ChooQLKuoGWeinerAJOverbyLRBradleyDWHoughtonMIsolation of a cDNA clone derived from a blood-borne non-A, non-B viral hepatitis genomeScience198924449023593622523562
- MühlbergerNSchwarzerRLettmeierBSroczynskiGZeuzemSSiebertUHCV-related burden of disease in Europe: a systematic assessment of incidence, prevalence, morbidity, and mortalityBMC Public Health200993419161623
- HadziyannisSJSetteHJrMorganTRPEGASYS International Study GroupPeginterferon-alpha2a and ribavirin combination therapy in chronic hepatitis C: a randomized study of treatment duration and ribavirin doseAnn Intern Med2004140534635514996676
- FowellAJNashKLTelaprevir: a new hope in the treatment of chronic hepatitis C?Adv Ther201027851252220652658
- ThomasDLAstemborskiJRaiRMThe natural history of hepatitis C virus infection: host, viral, and environmental factorsJAMA2000284445045610904508
- AborsangayaKBDembinskiIKhatkarSAlphonseMPNickersonPRempelJDImpact of aboriginal ethnicity on HCV core-induced IL-10 synthesis: interaction with IL-10 gene polymorphismsHepatology200745362363017326156
- TrinksJHulaniukMLCaputoMDistribution of genetic polymorphisms associated to hepatitis C virus (HCV) antiviral response in a multiethnic and admixed populationPharmacogenomics J5202014 [Epub ahead of print.]
- MangiaAThompsonAJSantoroRAn IL28B polymorphism determines treatment response of hepatitis C virus genotype 2 or 3 patients who do not achieve a rapid virologic responseGastroenterology2010139382182720621700
- SarrazinCSusserSDoehringAImportance of IL28B gene polymorphisms in hepatitis C virus genotype 2 and 3 infected patientsJ Hepatol201154341542121112657
- ScherzerTMStättermayerAFStrasserMImpact of IL28B on treatment outcome in hepatitis C virus G1/4 patients receiving response-guided therapy with peginterferon alpha-2a (40KD)/ribavirinHepatology20115451518152622006276
- Montes-CanoMAGarcía-LozanoJRAbad-MolinaCInterleukin-28B genetic variants and hepatitis virus infection by different viral genotypesHepatology2010521333720578254
- RallonNINaggieSBenitoJMAssociation of a single nucleotide polymorphism near the interleukin-28B gene with response to hepatitis C therapy in HIV/hepatitis C virus-coinfected patientsAIDS2010248F23F2920389235
- YuMLHuangCFHuangJFRole of interleukin-28B polymorphisms in the treatment of hepatitis C virus genotype 2 infection in Asian patientsHepatology201153171321254157
- MangiaAThompsonAJSantoroRLimited use of interleukin 28B in the setting of response-guided treatment with detailed on-treatment virological monitoringHepatology201154377278021626525
- ThompsonAJMuirAJSulkowskiMSInterleukin-28B polymorphism improves viral kinetics and is the strongest pretreatment predictor of sustained virologic response in genotype 1 hepatitis C virusGastroenterology2010139112012920399780
- ChayamaKTsubotaAKobayashiMPretreatment virus load and multiple amino acid substitutions in the interferon sensitivity-determining region predict the outcome of interferon treatment in patients with chronic genotype 1b hepatitis C virus infectionHepatology19972537457499049229
- HayesCNKobayashiMAkutaNHCV substitutions and IL28B polymorphisms on outcome of peg-interferon plus ribavirin combination therapyGut201160226126721068134
- LindhMLaggingMArnholmBIL28B polymorphisms determine early viral kinetics and treatment outcome in patients receiving peginterferon/ribavirin for chronic hepatitis C genotype 1J Viral Hepat2011187e325e33121692944
- OchiHMaekawaTAbeHIL-28B predicts response to chronic hepatitis C therapy – fine-mapping and replication study in Asian populationsJ Gen Virol201192Pt 51071108121228123
- StättermayerAFStauberRHoferHImpact of IL28B genotype on the early and sustained virologic response in treatment-naive patients with chronic hepatitis CClin Gastroenterol Hepatol20119434435020728570
- LinCYChenJYLinTNIL28B SNP rs12979860 is a critical predictor for on-treatment and sustained virologic response in patients with hepatitis C virus genotype-1 infectionPLoS One201163e1832221479134
- FukuharaTTaketomiAMotomuraTVariants in IL28B in liver recipients and donors correlate with response to peg-interferon and ribavirin therapy for recurrent hepatitis CGastroenterology201013951577158520708617
- CharltonMRThompsonAVeldtBJInterleukin-28B polymorphisms are associated with histological recurrence and treatment response following liver transplantation in patients with hepatitis C virus infectionHepatology201153131732421254179
- Coto-LlerenaMPérez-del-PulgarSCrespoGDonor and recipient IL28B polymorphisms in HCV-infected patients undergoing antiviral therapy before and after liver transplantationAm J Transplant20111151051105721466653
- O’BrienTRProkunina-OlssonLDonnellyRPIFN-λ4: the paradoxical new member of the interferon lambda familyJ Interferon Cytokine Res4302014 [Epub ahead of print.]
- YoshimotoKKishidaTNakanoHInterleukin-28B acts synergistically with cisplatin to suppress the growth of head and neck squamous cell carcinomaJ Immunother201134213914821304406
- MorrowMPYanJPankhongPIL-28B/IFN-lambda 3 drives granzyme B loading and significantly increases CTL killing activity in macaquesMol Ther20101891714172320571540
- KotenkoSVGallagherGBaurinVVIFN-lambdas mediate antiviral protection through a distinct class II cytokine receptor complexNat Immunol200341697712483210
- ZhangLJilgNShaoRXIL28B inhibits hepatitis C virus replication through the JAK-STAT pathwayJ Hepatol201155228929821147189
- ZhouZHammingOJAnkNPaludanSRNielsenALHartmannRType III interferon (IFN) induces a type I IFN-like response in a restricted subset of cells through signaling pathways involving both the Jak-STAT pathway and the mitogen-activated protein kinasesJ Virol200781147749775817507495
- RehermannBHepatitis C virus versus innate and adaptive immune responses: a tale of coevolution and coexistenceJ Clin Invest200911971745175419587449
- KawaiTTakahashiKSatoSIPS-1, an adaptor triggering RIG-I- and Mda5-mediated type I interferon inductionNat Immunol200561098198816127453
- XuLGWangYYHanKJLiLYZhaiZShuHBVISA is an adapter protein required for virus-triggered IFN-beta signalingMol Cell200519672774016153868
- SethRBSunLEaCKChenZJIdentification and characterization of MAVS, a mitochondrial antiviral signaling protein that activates NF-kappaB and IRF 3Cell2005122566968216125763
- HayesCNImamuraMAikataHChayamaKGenetics of IL28B and HCV – response to infection and treatmentNat Rev Gastroenterol Hepatol20129740641722641049
- AsahinaYTsuchiyaKMuraokaMAssociation of gene expression involving innate immunity and genetic variation in IL28B with antiviral responseHepatology2012551202921898478
- Prokunina-OlssonLMuchmoreBTangWA variant upstream of IFNL3 (IL28B) creating a new interferon gene IFNL4 is associated with impaired clearance of hepatitis C virusNat Genet201345216417123291588
- BibertSRogerTCalandraTIL28B expression depends on a novel TT/-G polymorphism which improves HCV clearance predictionJ Exp Med201321061109111623712427
- SorianoVPovedaEVispoELabargaPRallónNBarreiroPPharmacogenetics of hepatitis CJ Antimicrob Chemother201267352352922194301
- De FranceschiLFattovichGTurriniHemolytic anemia induced by ribavirin therapy in patients with chronic hepatitis C virus infection: role of membrane oxidative damageHepatology2000314997100410733558
- FellayJThompsonAJGeDITPA gene variants protect against anemia in patients treated for chronic hepatitis CNature2010464728740540820173735
- BierauJLindhoutMBakkerJAPharmacogenetic significance of inosine triphosphatasePharmacogenomics2007891221122817924837
- StoccoGCheokMHCrewsKRGenetic polymorphism of inosine triphosphate pyrophosphatase is a determinant of mercaptopurine metabolism and toxicity during treatment for acute lymphoblastic leukemiaClin Pharmacol Ther200985216417218685564
- ThompsonAFellayJPatelKVariants in the ITPA gene protect against ribavirin-induced hemolytic anemia and decrease the need for ribavirin dose reductionGastroenterology201013941181118920547162
- OgawaEFurusyoNNakamutaMClinical milestones for the prediction of severe anemia by chronic hepatitis C patients receiving telaprevir-based triple therapyJ Hepatol201359466767423707372
- ThompsonAJClarkPJSinghAGenome-wide association study of interferon-related cytopenia in chronic hepatitis C patientsJ Hepatol201256231331921703177
- ClarkPJAghemoADegasperiEInosine triphosphatase deficiency helps predict anaemia, anaemia management and response in chronic hepatitis C therapyJ Viral Hepat2013201285886624304455
- RembeckKWaldenströmJHellstrandKVariants of the inosine triphosphate pyrophosphatase gene are associated with reduced relapse risk following treatment for HCV genotype 2/3Hepatology20145962131213924519039
- AfdhalNMcHutchisonJZeuzemSHepatitis C pharmacogenetics: state of the art in 2010Hepatology201153133634521254181
- HeningBJHellierSFrodshamAJAssociation of low-density lipoprotein receptor polymorphisms and outcome of hepatitis C infectionGenes Immun20023635936712209363
- PinedaJACaruzADi LelloFALow-density lipoprotein receptor genotyping enhances the predictive value of IL28B genotype in HIV/hepatitis C virus-coinfected patientsAIDS201125111415142021572301
- PinedaJACaruzARiveroAPrediction of response to pegylated interferon plus ribavirin by IL28B gene variation in patients coinfected with HIV and hepatitis C virusClin Infect Dis201051778879520804372
- PettaSCammàCScazzoneCLow vitamin D serum level is related to severe fibrosis and low responsiveness to interferon-based therapy in genotype 1 chronic hepatitis CHepatology20105141158116720162613
- LangeCMBojungaJRamos-LopezEVitamin D deficiency and a CYP27B1-1260 promoter polymorphism are associated with chronic hepatitis C and poor response to interferon-alfa based therapyJ Hepatol201154588789321145801
- UitterlindenAGFangYVan MeursJBPolsHAVan LeeuwenJPGenetics and biology of vitamin D receptor polymorphismsGene2004338214315615315818
- FosterGRGoldinRDThomasHCChronic hepatitis C virus infection causes a significant reduction in quality of life in the absence of cirrhosisHepatology19982712092129425939
- DalgardOEgelandASkaugKVilimasKSteenTHealth-related quality of life in active injecting drug users with and without chronic hepatitis C virus infectionHepatology2004391748014752825
- RifaiMAGleasonOCSabouniDPsychiatric care of the patient with hepatitis C: a review of the literaturePrim Care Companion J Clin Psychiatry2010126PCC.09r0087721494349
- McHutchisonJGWareJEJrBaylissMSHepatitis Interventional Therapy GroupThe effects of interferon alpha-2b in combination with ribavirin on health related quality of life and work productivityJ Hepatol200134114014711211891
- WareJEJrBaylissMSMannocchiaMDavisGLHealth-related quality of life in chronic hepatitis C: impact of disease and treatment response. The Interventional Therapy GroupHepatology199930255055510421667
- BernsteinDKleinmanLBarkerCMRevickiDAGreenJRelationship of health-related quality of life to treatment adherence and sustained response in chronic hepatitis C patientsHepatology200235370470811870387
- RifaiMAMolesJKShortDDHepatitis C treatment eligibility and outcomes among patients with psychiatric illnessPsychiatr Serv200657457057216603757
- MatsushitaHIkedaFIwasakiYAssessment of health-related quality of life and how it predicts the outcome of pegylated interferon and ribavirin therapy for chronic hepatitis CJ Gastroenterol Hepatol201429233734323869873
- LiuSCiprianoLEHolodniyMOwensDKGoldhaber-FiebertJDNew protease inhibitors for the treatment of chronic hepatitis C: a cost-effectiveness analysisAnn Intern Med2012156427929022351713
- ThompsonAJMcHutchisonJGWill IL28B polymorphism remain relevant in the era of direct-acting antiviral agents for hepatitis C virus?Hepatology201256137338122511355