
Abstract
Objective
The antineutrophil cytoplasmic antibody (ANCA)-associated vasculitides (AAVs) are multisystem diseases of the small blood vessels. Patients experience irreversible damage and psychological effects from AAV and its treatment. An international collaboration was created to investigate the impact of AAV on health-related quality of life (HRQoL), and develop a disease-specific patient-reported outcome measure to assess outcomes of importance to patients.
Methods
Patients with AAV from the UK, USA, and Canada were interviewed to identify salient aspects of HRQoL affected by AAV. The study was overseen by a steering committee including four patient research partners. Purposive sampling of interviewees ensured representation of a range of disease manifestations and demographics. Inductive analysis was used to identify themes of importance to patients; these were further confirmed by a free-listing exercise in the US. Individual themes were recast into candidate items, which were scrutinized by patients, piloted through cognitive interviews and received a linguistic and translatability evaluation.
Results
Fifty interviews, conducted to saturation, with patients from the UK, USA, and Canada, identified 55 individual themes of interest within seven broad domains: general health perceptions, impact on function, psychological perceptions, social perceptions, social contact, social role, and symptoms. Individual themes were constructed into >100 candidate questionnaire items, which were then reduced and refined to 35 candidate items.
Conclusion
This is the largest international qualitative analysis of HRQoL in AAV to date, and the results have underpinned the development of 35 candidate items for a disease-specific, patient-reported outcome questionnaire.
Introduction
Granulomatosis with polyangiitis (GPA), microscopic polyangiitis (MPA), and eosinophilic granulomatosis with polyangiitis (EGPA) are organ- and life-threatening multisystem diseases of small arteries, known as the antineutrophil cytoplasmic antibody (ANCA)-associated vasculitides (AAVs).Citation1 Patients present with inflammation in multiple body areas, including the lungs, ear, nose, kidneys, joints, and nerves,Citation2 with fevers, weight loss, and fatigue.Citation3 Treatment is with glucocorticoids and other immunosuppressants.Citation4 A third of patients will have irreversible damage at diagnosis,Citation5 and 40% will suffer relapse.Citation6 One-year mortality in AAV has been >15%,Citation7 a poorer survival rate than breast or prostate cancer;Citation8 however, mortality in AAV has improved, likely due to the adoption of newer treatment regimens.Citation9,Citation10 Surveys have demonstrated impairments in health-related quality of life (HRQoL) in AAV, in particular fatigue.Citation3,Citation11–Citation18 A clinician-derived survey to assess patient perspectives in granulomatosis with polyangiitis was developed in 1998;Citation19 however, there have been no in-depth qualitative studies to capture patient perspectives on the full range of HRQoL in the AAVs as a whole.
Due to the relative rarity of AAV, with three overlapping disease phenotypes, patients with AAV are frequently considered together,Citation4 with patients with GPA and MPA included within the same randomized controlled trials (RCTs).Citation20–Citation22 Primary outcomes are based on the physician-based Bir-mingham Vasculitis Activity Score,Citation23,Citation24 which records the presence or absence of disease activity.Citation20–Citation22,Citation25 Patients with AAV, however, often have different perceptions of what is important to their physicians, for example, they rank fatigue as more important than dialysis or oxygen dependence.Citation11 To guage the efficacy of treatments within RCTs, validated measurement of both physician- and patient-focused outcomes is key.Citation11,Citation26
The Outcome Measurement in Rheumatology (OMER-ACT) Vasculitis Working Group has consistently highlighted the need for a disease-specific patient-reported outcome (PRO) measure for patients with AAV,Citation25,Citation27 due to concern that the generic Medical Outcomes Short Form-36 (SF-36) may not capture all themes of importance. Since OMERACT 2012,Citation27,Citation28 an international collaboration (the UK, the USA, and Canada) has been developing an AAV disease-specific PRO measure, in line with the US Food and Drug Administration (FDA) guidelines for the development of PROs.Citation29 The development of a new PRO instrument involves three distinct stages with patient involvement at each step: 1) item generation and piloting, 2) item reduction and scale generation, and 3) testing reliability and validity.
This paper describes the themes of importance in HRQoL in relation to AAV, identified through in-depth qualitative analysis in three countries in order to produce candidate questionnaire items for a new disease-specific PRO for AAV.
Methods
The study steering committee included members from the UK, USA, and Canada: four patient partners; medical sociologists with extensive experience in PROM development, testing, and application; qualitative researchers; and clinical researchers with an interest in vasculitis. An initial conceptual framework was developed, through literature review and steering committee input, to explore domains of interest, and this framework evolved during the study.
A core qualitative working group (CQWG), comprising researchers from the three countries, performed the qualitative analysis, developed a collaborative code book of themes, and produced and refined candidate items. The steering committee gave critical feedback throughout on developing themes and items and the project received critical scrutiny at three successive Vasculitis Workshop sessions at Outcome Measures in Rheumatology (OMERACT) conferences.Citation27,Citation28
Patient study sample
Patients diagnosed with AAV were recruited from three rheumatology centers in the UK, USA, and Canada. Inclusion criteria were age ≥18, ability to give informed consent, and a clinically verified diagnosis of GPA, MPA, or EGPA. Patients were purposively sampled to assure adequate representation of all three diseases, chronicity of disease, different age ranges, sex, and organ involvement. Study approvals were given by the NHS Research Committee South West-Central Bristol, the University of Pennsylvania Office of Regulatory Affairs, and the Ottawa Hospital’s Research Ethics Board. All patients provided written informed consent.
In-depth interviews
Exploratory semi-structured patient interviews were conducted to identify the range of salient aspects of HRQoL affected by AAV and its treatment. An interview guide of prompts and cues was developed by the steering committee. Interviews were performed by a qualitative researcher in the US (KK) and two clinical research fellows trained in qualitative interview techniques in the UK (JCR) and Canada (NM).
Analysis
Interviews were recorded and transcribed, anonymized, and systematically analyzed using a modified framework method.Citation30–Citation32 Coding was carried out using both an inductive (codes emerged during analysis) and deductive (codes anticipated) approach,Citation33 with NVivo computer software used to index transcripts.Citation34 Interviews continued until no new substantive themes arose indicating data saturation.Citation35 The CQWG defined the themes of interest, produced a common thematic framework, and ensured uniformity of coding across sites. A proportion of transcripts from each site was double coded, to ensure common approaches.
Candidate item development
Members of the CQWG recast themes as candidate items, using patients’ descriptions throughout. Items were amended, and sometimes deleted by the CQWG, to reduce ambiguity and duplication. Piloting and further item amendment was conducted following feedback from steering committee patient partners.
US participants were invited to participate in a free-listing activity, a semi-structured interview technique in which participants are given a question or statement and asked to identify words they associate with that phrase.Citation36 This method uncovers how groups of people with shared experiences create, associate, and categorize topics.Citation36,Citation37
The following questions were asked: “Which words would you use to describe your symptoms when your vasculitis: 1) first started; 2) is under control; and 3) is starting to flare?” Patient partners on the study team performed pile-sorting of the responses independently, with disagreement resolved through consensus. Following free-listing and pile-sorting, the Smith’s Salience Index (SSI)Citation38,Citation39 was used to identify the most salient terms. SSI scores were calculated using ARTHROPAC software. The identified salient terms were contrasted across interview themes to provide additional lens of validation for candidate item development.
Patient refinement
Three rounds of patient cognitive interviews were completed, in order to check understanding and interpretation of the candidate items.Citation40,Citation41 This was an iterative process, with items refined or rejected by the CQWG between each round.
In parallel, a readability and translatability assessment was completed in collaboration with a specialist UK company (Pharmaquest – translation and linguistic validation company for PROs).Citation42 A breakout session was also held at the Vasculitis Workshop at OMERACT 2014, which sought feedback about 1) inclusion of contextual factors within the PRO and 2) attribution within the stem (or lead in sentence), to vasculitis and/or its treatment. All proposed item changes were tested by further cognitive interviews and steering committee review.
Results
Fifty participants, 24 men and 26 women, were interviewed in the UK, USA, and Canada. Participants’ characteristics are shown in . Interview transcripts were analyzed, identifying 55 individual themes of interest, grouped into seven domains (definitions of individual themes within the codebook in Table S1). The domains identified were general health perceptions, impact on function, psychological perceptions, social perceptions, social contact, social roles, and symptoms (Box 1 shows domain structure and individual themes). The saturation table of emergent themes is shown in Table S2.
Table 1 Demographic and disease features of 50 patients with ANCA-associated vasculitis
General health perceptions
Eighty-six percent of patients used descriptions of how their general sense of self and wellness had been affected by developing AAV. Concerns about the future and difficulties making long-term plans were prominent, as was a sense of vulnerability in one’s own body.
Domains and individual themes of interest in ANCA-associated vasculitis, n=50 (number of interviews from which the theme emerged)
General health perceptions
General sense of self and wellness (43)
Lack of confidence in one’s body (27)
Poor response to treatment (25)
Vulnerability to infection or illness (22)
Impact on function
Level of physical function (45)
Personal mobility (41)
Scope for travel (38)
Household tasks (36)
Treatment consumes time/focus (33)
Adaptation (necessary) (27)
Hobbies and interests (23)
Use of everyday transport (17)
Eating and drinking (16)
Everyday technology (10)
Washing self (10)
Dressing and undressing (9)
Psychological perceptions
Uncertainty/concerns about future (43)
Fear, anxiety, stress (37)
AAV dominates (33)
Self-efficacy (33)
Information and knowledge (32)
Support (29)
Depression, low mood (25)
Anger and irritation (23)
Social perceptions
Visibility of condition or side effects (34)
Empathy and emotional connections (33)
Source of other people’s worry (30)
Social contact
Impact on social life (40)
Social activities and participation (31)
Adaptations to facilitate social life (26)
Quality of communication (14)
Sex and intimate relationships (7)
Social role
Occupation or finances (41)
Family and family planning (35)
Dependency on others (34)
Role identity and status (25)
Symptoms
Fatigue (44)
Cognition and poor concentration (9)
Issues related to body weight (37)
Sleep symptoms (27)
Temperature instability (11)
Skin and nail problems (25)
Earache and hearing difficulties (19)
Upper respiratory tract (35)
Eye symptoms and affected sight (22)
Cardiorespiratory symptoms (38)
Gastrointestinal symptoms (18)
Muscle symptoms (16)
Numbness and nerve symptoms (12)
Joint symptoms (31)
Kidney and urinary tract (13)
Appetite (14)
Sense of taste (3)
Feeling unsteady or faint (13)
Pain: pain unspecified (13), pain in feet and legs (23), pain in arms and hands (19), facial and head pain (18)
Abbreviation: ANCA, antineutrophil cytoplasmic antibody.
“If I compare to 3 years ago… I was the guy who was working 7 days a week, 16 hour days, never tired. Now… Ufff. It’s not the same guy anymore.” [47-year-old male with EGPA]
“I didn’t want to set foot outside the door. Simply because I thought … I can’t trust my body anymore”. [53-year-old female with EGPA]
Impact on function
Ninety percent of participants described difficulties with reduced levels of physical function, over 80% had a reduction in mobility, and 20% described difficulties in washing and dressing. These impairments led to frustration and impacted finances and work (82%), the ability to perform household tasks (72%), taking part in hobbies and interests (46%), and restricted travel (76%).
“Weakness, inability to walk, to use my arms, to bathe, to do anything – I just laid in bed”. [82-year-old male with MPA]
“TV was a no-no. I got a telephone with a light on it, because it [the deafness] was that bad… I felt very isolated and very stupid”. [57-year-old male with GPA]
Psychological
Concerns about the future were highlighted in 86% of interviews with over 70% reporting experiencing fear, anxiety, or stress, and 50% describing depression or low mood. Anger or irritation was reported by almost 50%. Difficulties in making plans and the potential for premature death were described by patients of all ages.
“For the first year after I was diagnosed, I did nothing, apart from cope with me, my illness and trying to live as normal a life as possible”. [67-year-old female with GPA]
“I was only [age], my first year of college – everything is falling apart and I think I’m dying”. [36-year-old female with GPA]
Social perceptions
Participants were aware of the visibility of the condition, and its treatment side-effects, particularly in relation to glucocorticoids; these issues were discussed in 64% of interviews. A lack of empathy from others was reported by around 60% of interviewees, as was being the source of worry to others.
“To have a big puffy moon face [due to glucocorticoids] is really hard for me. Well, you’re not attractive anymore – it’s weird”. [33-year-old female with GPA]
“I think some people were more supportive than others, and it wasn’t always the people I expected to be”. [67-year-old female with GPA]
Social contact
Eighty percent of interviewees described an impact on their social life, because of fatigue, difficulties with joining in physical activities or communicating, or concerns about letting people down by having to break plans.
“If we had a dinner date on the weekend I had to rest coming up to that day just to be able to have enough energy. I got to a point where I just didn’t bother”. [51-year-old female with EGPA]
“Meetings were the worst. Because I found that I was lip-reading. In an open room with a number of people, it was a nightmare”. [57-year-old male with GPA]
Social role
Eighty-two percent of participants discussed their occupation or finances, specifically stemming from difficulties with concentration and fatigue. Roles beyond work were also discussed, within the family (70%), and changes to role and status when having to rely on others for help (64%).
“When I was getting sick in the beginning I gave up my position as the executive director of the organization and I moved into a position with less responsibility”. [52-year-old female with GPA]
“It was hard on my son as well, so he started goofing off in school. I felt like I wasn’t a good mom, I wasn’t a good wife, and I was isolated”. [51-year old female with EGPA]
Symptoms
All of the patients described symptoms due to disease and treatment in depth. Nineteen different sets of symptoms were identified, most frequently fatigue (88%), cardiorespiratory symptoms (76%), issues related to body weight (74%), and upper respiratory tract symptoms (70%). A full list of symptoms is given in Box 1, with quotes in Box 2.
Free-listing and pile-sorting items of importance to patients with AAV
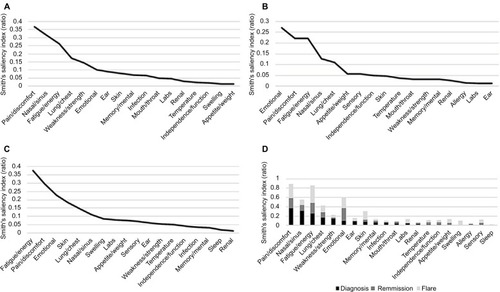
All 17 US patients interviewed were invited to free-list terms they associated with the onset, remission, and flaring of their AAV (). The most salient themes at onset were pain and discomfort (SSI=0.37), nasal and sinus problems (SSI=0.32), and fatigue and energy levels (SSI=0.27). Emotional effects were within the top three during flare (SSI=0.28) and remission (SSI=0.27). Themes identified were compared with the individual themes of interest and domains from the in-depth patient interviews and no new themes were identified (Box 1 for overview and Table S1 for detailed descriptions).
Figure 1 Smith’s Salience Indices of patient’s free-listed and ranked terms.
Abbreviations: AAV, associated vasculitis; labs, laboratory tests.
Candidate item development
Fifty-five individual themes were identified from the qualitative work (Box 1), and these were recast into an initial list of 105 candidate items by members of the CQWG. Patient descriptions informed the design of the candidate questionnaire items and response options, resulting in different sections. Patients described the overall severity of their symptoms, rather than the frequency; pain was usually described in relation to specific body areas, such as joints or muscles; and ability to function was described in terms of the amount of difficulty with completing a specific task. The candidate items were scrutinized for duplication and ambiguity of items, reducing the item pool to 42 items. Patients made it clear that it was difficult to tease apart symptoms caused by AAV versus its treatment, so both were included within the stem of the question. Items related to contextual factors (eg, support and self-efficacy – Box 1 and Table S1) were not included within the PRO itself, after discussion at an OMERACT 2014 breakout session with patient participants.Citation28
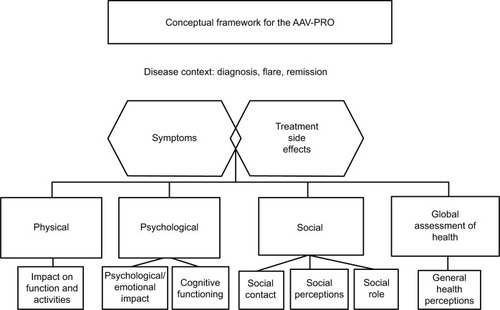
Three rounds of cognitive interviews were conducted in the UK and USA, using the 42-item version of the questionnaire, with amendments after each round. Word changes were suggested by patients, for example, clarification of the word essential in relation to activities, and change to the period of recall from 7 days to 4 weeks. All participants reported that the questionnaire captured content relevant to them. Seven items were rejected because of ambiguity, repetition, or being contextual factors. Following the translatability assessment (Box S1), minor changes were made to a few items, and these revisions were piloted in the last round of interviews. The conceptual framework evolved in response to insights from the qualitative research, feedback from the steering committee, and breakout sessions at OMERACT, and the final version is shown in . The resulting 35-item candidate pool is shown in Box 3.
Figure 2 Conceptual framework for the AAV-PRO.
Abbreviations: AAV, ANCA-associated vasculitis; ANCA, antineutrophil cytoplasmic antibody; PRO, patient-reported outcome.
Discussion
This is the most comprehensive evaluation of the patient perspective in AAV to date. Patients have been an integral part of this work as key members of the steering committee and qualitative interview participants, reflecting all three diseases, differing disease manifestations, a wide demographic range, and three different countries. The item generation for a novel, disease-specific PRO measure is underpinned by this qualitative research, which should ensure that the final candidate items have good face validity within each country. Themes identified in previous quantitative studies are confirmed, for example, fatigue,Citation13 anxiety, and depression,Citation16 and the impact on everyday function and employment.Citation17,Citation43 Newer themes include difficulties in making plans, from short-term social engagements to life planning, previously reported in patients with systemic lupus erythematosus, rheumatoid arthritis, and GPA.Citation19,Citation44,Citation45
The strengths of this study include a high level of patient involvement, and ongoing critical review through OMER-ACT Workshops, which have helped to ensure that each stage was consistent with best practice. Patients were pur-posively sampled to include a range of disease features and demographics, including a high proportion of patients with recent active disease. This was to ensure a focus on themes (and then items), which would exhibit greatest change in the context of a RCT. A third of patients had longer-standing disease, and saturation of themes was also reached within this patient group. The high rate of relapsing disease may also be a reflection of the fact that patients with GPA, who have a higher rate of relapse,Citation46 were slightly over-represented compared with patients with MPA; this may be a potential bias of the sample. That only English-speaking participants were included is a limitation of this study. However, a trans-latability assessment was performed for the questionnaire items, to ensure that any future translation into a range of languages should be straightforward.Citation47 In addition, care was taken to develop items that were not overly culture-specific, for example, describing “difficulties with traveling far from home,” rather than “going on holidays.” Interviews were performed by clinical fellows in the UK and Canada, and this may have changed the way that patients described problems in relation to their disease or treatment. Training was, therefore, provided by experienced social scientists, who also evaluated all interview transcripts.
The OMERACT Vasculitis Working Group has highlighted the lack of a disease-specific PRO for AAV.Citation27 As per FDA guidance, the development of a PRO instrument should start with qualitative analysis involving patients with the disease, in order to identify themes of importance. However, generic PRO instruments, such as the SF-36,Citation48 can be used to measure and compare HRQoL between patients with different chronic conditions, and population norms. A combined approach of using disease-specific and generic PRO measures may, therefore, be the optimum way of comprehensively measuring HRQoL in AAV.Citation49
The 35-item candidate questionnaire will need to be shortened to reduce responder burden and optimize feasibility within RCTs. The next stage of development will involve a large-scale survey to facilitate further item reduction, and determine the underlying scale structure and measurement properties (reliability, validity, and responsiveness) of the final AAV-PRO instrument.
Fatigue: “So with the severe flares, the fatigue is indescribable. Looking back, I don’t know how I got up and went to work every day last year”. [30-year-old. F, GPA]
Cognition/concentration: “You feel like you have the flu, sort of achy and really tired, your head is kind of fuzzy, it’s hard to think and concentrate”. [52-year-old. F, GPA]
Issues related to body weight: “Taking too many prednisolone really made me eat a lot and gain weight”. 58-year-old. M, EGPA.
Sleep symptoms: “I wake up tired, just really tired. There doesn’t seem to be any refreshing sleep, no matter how long I try and sleep for”. [53-year-old. F, EGPA]
Temperature instability: “I’d have high fevers and night sweats, tremendous night sweats”. 51-year-old. F, EGPA.
Skin problems: “Your skin is so thin that it tears” 04.202. “I had a rash, and I couldn’t get rid of it, breaking out down my arms and chest… it drove me crazy”. [68-year-old. F, EGPA]
Earache/hearing difficulties/upper respiratory tract: “I’m coughing up blood and I’ve got bloody noses. I can’t hear on the phone. I’ve lost my hearing”. [36-year-old. F, GPA]
Eye symptoms and affected sight: “It was very, very red, very painful like in the back of my eye, it was very painful, and I was sensitive to light, I couldn’t read”. [61-year-old. F, GPA]
Cardiorespiratory symptoms: “I could barely walk a few yards down the road without having to stop and really catch my breath”. [48-year-old. F, GPA]
Gastrointestinal symptoms: “I had been starting to get a lot of side effects from the prednisone it was really causing havoc in my digestive system”. [52-year-old. F, GPA]
Muscle symptoms: “…I just don’t have the muscle power in my legs. And also my arms… its worse when I’m on the steroids”. [53-year-old. F, EGPA]
Nerve symptoms: “I couldn’t walk, the sheer agony of the pain was bad as well, I couldn’t use the hand, it went tingly and dropped, the same as the foot”. [67-year-old. F, EGPA]
Joint symptoms: “I started having “rotating joint pain”. It would be mostly in my legs, but sometimes in my wrists, in my elbow, but especially in my legs”. [64-year-old. M, GPA]
Kidney and urinary tract: “They discovered that there was something wrong with my kidneys which was really quite a shock”. [68-year-old. F, MPA]
Appetite: “And then I lost a lot of weight, I lost a stone and a half in weight even though I was trying to eat but I hadn’t got a lot of appetite”. [67-year-old. F, EGPA]
Feeling unsteady or faint: “I would take my bath or my shower but my husband would insist that I do it when he was there because I would feel faint”. [51-year-old. F, EGPA]
Pain: “And then the joint pains started. And that’s when it became, you know, quite an issue. You know, so I had a real, real problem with pain”. [66-year-old. M, GPA]
Abbreviations: ANCA, antineutrophil cytoplasmic antibody; F, female; GPA, granulomatosis with polyangiitis; EGPA, eosinophilic granulomatosis with polyangiitis; M, male; MPA, microscopic polyangiitis.
Due to having vasculitis or its treatment….
…please rate your experience of the following problems, in general, during the past 4 weeks.
Candidate items (….abridged wording)
| 1 | Chest problems …. | ||||
| 2 | Problems with your ears…. | ||||
| 3 | Problems with your eyes …. | ||||
| 4 | Problems with your nose or …. | ||||
| 5 | Problems with your mouth or …. | ||||
| 6 | Problems with your joints…. | ||||
| 7 | …Cramps or weakness affecting your muscles…. | ||||
| 8 | Nerve pain or numbness …. | ||||
| 9 | Problems with your skin …. | ||||
| 10 | Tiredness or fatigue…. | ||||
| 11 | Feeling uncomfortably hot, cold, or …. | ||||
| 12 | Indigestion, heartburn, nausea, or …. | ||||
…how difficult have you found the following activities, in general, during the past 4 weeks?
| 13 | Walking around …. | ||||
| 14 | Walking up ….. | ||||
| 15 | Doing physical activities …. | ||||
| 16 | Doing activities …. | ||||
| 17 | Using your hands to do ….. | ||||
| 18 | Washing and drying yourself….. | ||||
| 19 | Getting enough good sleep | ||||
| 20 | Sexual activity …. | ||||
…how often have the following applied to you, in general, during the past 4 weeks
| 21 | Concerned about weight….. | ||||
| 22 | ….Upset or frustrated | ||||
| 23 | ….Worried about the future | ||||
…how often have the following applied to you, in general, during the past 4 weeks?
| 24 | ….Worried or stressed | ||||
| 25 | ….Difficulty concentrating | ||||
| 26 | ….Down or depressed | ||||
| 27 | ….Dependent on other people | ||||
| 28 | ….Current or future income | ||||
| 29 | ….Long-term plans | ||||
| 30 | ….Social life is limited | ||||
| 31 | ….Traveling a long distance from home | ||||
| 32 | ….Embarrassed or self-conscious because of appearance …. | ||||
| 33 | ….Let other people down | ||||
| 34 | ….Life is now focused on coping | ||||
| 35 | ….Long-term effects of treatment | ||||
Notes: Abridged wording given (….); survey to determine scale structure and measurement properties needed to determine final PRO items.
Abbreviation: PRO, patient-reported outcome.
Acknowledgments
Sponsored by the University of Oxford, the Vasculitis Clinical Research Consortium and the University of Ottawa. With support from the Medical Research Fund, Oxford, the Oxford-shire Health Services Research Committee (Ref 1098), the US National Institute of Arthritis and Musculoskeletal and Skin Diseases (U54 AR057319 and U01 AR51874), the National Center for Research Resources (U54 RR019497), and the Office of Rare Diseases Research. Oxford University Innovation funded the translatability exercise. Additional support received by a Patient-Centred Outcomes Research Institute Pilot Project Grant.
Supplementary materials
Table S1 Codebook descriptions of individual themes. Collaborative codebook by core qualitative group using consensus methods
Table S2 Saturation table: domains and subcodes of emergent themes from 50 in-depth individual patient interviews within the US, Canada (CAN), and UK. 0 = theme not present; 1 = theme present
The translatability of the questionnaire refers to whether items can be meaningfully translated into other languages in the future.50
First, a concept elaboration document is produced, which clarifies any ambiguities or nuances within the candidate items and instructions.
For each item and instruction, concepts and wording are then checked to ensure equivalence between the original and target language, and whether they remain linguistically and culturally appropriate. A sample of different types of languages is tested.
Arabic (Egypt), Finnish (Finland), German (Germany), Greek (Greece), Russian (Russia), Spanish (Argentina), and Xhosa (South Africa) were the languages tested in this study.
The questionnaire items were then refined to enable better cultural and linguistic equivalence across future translations, and thereby to improve the measure’s performance when used in international studies.
A translatability assessment does not go as far as conducting full-scale translation/back-translation process, with testing for validity in another language(s). This is for the future (once the number of questionnaire items has been finalized) and would require a full study for each language. However, the translatability assessment that was undertaken should ensure that future translations are more straightforward and will better facilitate equivalence.
Reference
- ConwayKPatrickDLGauchonTAcquadroCEnhancing crosscultural appropriateness for newly developed patient-reported outcome (PRO) instruments: the use of translatability assessmentPatient Reported Outcomes Newsl201044912
Disclosure
Dr Robson and Professor Luqmani were supported in part by the National Institute for Health Research Musculoskeletal Biomedical Research Unit, Oxford, UK. Dr Robson was supported by a National Institute for Health Research (NIHR) clinical lectureship. Dr Milman was supported by a UCB/Canadian Rheumatology Association/Arthritis Society postgraduate rheumatology fellowship award and a research fellowship from the Department of Medicine at the Ottawa Hospital. The authors report no other conflicts of interest in this work.
References
- JennetteJCFalkRJBaconPA2012 revised international chapel hill consensus conference nomenclature of vasculitidesArthritis Rheum201365111123045170
- McNicholasBAGriffinTPDonnellanSANCA-associated vasculitis: a comparison of cases presenting to nephrology and rheumatology servicesQJM20161091280380927318367
- BasuNJonesGTFluckNFatigue: a principal contributor to impaired quality of life in ANCA-associated vasculitisRheumatology (Oxford)20104971383139020400759
- YatesMWattsRABajemaIMEULAR/ERA-EDTA recommendations for the management of ANCA-associated vasculitisAnn Rheum Dis20167591583159427338776
- RobsonJDollHSuppiahRDamage in the anca-associated vasculitides: long-term data from the European vasculitis study group (EUVAS) therapeutic trialsAnn Rheum Dis201574117718424243925
- WalshMFlossmannOBerdenARisk factors for relapse of antineutrophil cytoplasmic antibody-associated vasculitisArthritis Rheum201264254254821953279
- FlossmannOBerdenAde GrootKEuropean Vasculitis Study GroupLong-term patient survival in ANCA-associated vasculitisAnn Rheum Dis201170348849421109517
- QuaresmaMColemanMPRachetB40-year trends in an index of survival for all cancers combined and survival adjusted for age and sex for each cancer in England and Wales, 1971–2011: a population-based studyLancet201538599741206121825479696
- HilhorstMWildeBvan PaassenPWinkensBvan Breda VriesmanPCohen TervaertJWLimburg Renal RegistryImproved outcome in anti-neutrophil cytoplasmic antibody (ANCA)-associated glo-merulonephritis: a 30-year follow-up studyNephrol Dial Transplant201328237337923223225
- RheeRLHoganSLPoultonCJTrends in long-term outcomes among patients with ANCA-associated vasculitis with renal diseaseArthritis Rheumatol20166871711172026814428
- HerlynKHellmichBSeoPMerkelPAPatient-reported outcome assessment in vasculitis may provide important data and a unique perspectiveArthritis Care Res (Hoboken)201062111639164520556814
- WalshMMukhtyarCMahrAHealth-related quality of life in patients with newly diagnosed antineutrophil cytoplasmic antibody-associated vasculitisArthritis Care Res (Hoboken)20116371055106121452254
- BasuNMcCleanAHarperLThe characterisation and determinants of quality of life in ANCA associated vasculitisAnn Rheum Dis201473120721123355077
- CarpenterDMThorpeCTLewisMDevellisRFHoganSLHealth-related quality of life for patients with vasculitis and their spousesArthritis Rheum200961225926519177525
- TomassonGBoersMWalshMAssessment of health-related quality of life as an outcome measure in granulomatosis with polyan-giitis (Wegener’s)Arthritis Care Res2012642273279
- KoutantjiMHarroldELaneSEPearceSWattsRAScottDGInvestigation of quality of life, mood, pain, disability, and disease status in primary systemic vasculitisArthritis Rheum200349682683714673970
- BenarousLTerrierBLaborde-CasterotHFrench Vasculitis Study Group (FVSG)Employment, work disability and quality of life in patients with ANCA-associated vasculitides. The EXPOVAS studyClin Exp Rheumatol201710314046
- BoomsmaMMBijlMStegemanCAKallenbergCGHoffmanGSTervaertJWPatients’ perceptions of the effects of systemic lupus erythematosus on health, function, income, and interpersonal relationships: a comparison with Wegener’s granulomatosisArthritis Rheum200247219620111954014
- HoffmanGSDruckerYCotchMFLockerGAEasleyKKwohKWegener’s granulomatosis: patient-reported effects of disease on health, function, and incomeArthritis Rheum19984112225722629870883
- JonesRBTervaertJWHauserTEuropean Vasculitis Study GroupRituximab versus cyclophosphamide in ANCA-associated renal vasculitisN Engl J Med2010363321122020647198
- StoneJHMerkelPASpieraRRAVE-ITN Research GroupRituximab versus cyclophosphamide for ANCA-associated vasculitisN Engl J Med2010363322123220647199
- GuillevinLPagnouxCKarrasAFrench Vasculitis Study GroupRituximab versus azathioprine for maintenance in ANCA-associated vasculitisN Engl J Med2014371191771178025372085
- LuqmaniRABaconPAMootsRJBirmingham vasculitis activity score (BVAS) in systemic necrotizing vasculitisQJM199487116716787820541
- MukhtyarCLeeRBrownDModification and validation of the birmingham vasculitis activity score (version 3)Ann Rheum Dis200968121827183219054820
- MerkelPAAydinSZBoersMThe OMERACT core set of outcome measures for use in clinical trials of ANCA-associated vasculitisJ Rheumatol20113871480148621724720
- KirwanJRHewlettSEHeibergTIncorporating the patient perspective into outcome assessment in rheumatoid arthritis progress at OMERACT 7J Rheumatol200532112250225616265712
- MerkelPAAydinSZBoersMCurrent status of outcome measure development in vasculitisJ Rheumatol201441359359824429177
- RobsonJCMilmanNTomassonGExploration, development, and validation of patient-reported outcomes in antineutrophil cytoplasmic antibody-associated vasculitis using the OMERACT processJ Rheumatol201542112204220926329344
- Guidance for Industry: Patient-Reported Outcome Measures: Use in Medical Product Development to Support Labelling Calims(FDA) USDoHaHSFaDAMarylandFDA2009
- McCollEDeveloping questionnairesFayersPHaysRAssessing Quality of Life in Clinical Trials2nd edOxford, UKOxford Medical Publications2005
- RitchieJSpencerLQualitative data analysis for applied policy researchBrymanABurgessRGAnalysing Qualitative DataLondon, UKRoutledge1994
- PopeCZieblandSMaysNQualitative research in health care. Analysing qualitative dataBMJ2000320722711411610625273
- FeredayJMuir-CochraneEDemonstrating rigor using thematic analysis: a hybrid approach of inductive and deductive coding and theme developmentInt J Qual Meth20065122
- International QVivo qualitative data analysis software. Version 10QSR International2012 Available from: qsrinternational.comAccessed October 11, 2017
- KerrCNixonAWildDAssessing and demonstrating data saturation in qualitative inquiry supporting patient-reported outcomes researchExpert Rev Pharmacoecon Outcomes Res201010326928120545592
- BorgattiSPElicitation techniques for cultural domain analysis. Enhanced ethnographic methods: audiovisual techniques, focused group interviews, and elicitation techniquesEthnographer ToolkitWalnut Creek, CAAlta Mira1999115151
- SchraufRWSanchezJUsing freelisting to identify, assess, and charac-terize age differences in shared cultural domainsJ Gerontol B Psychol Sci Soc Sci2008636S385S39319092048
- BorgattiSPCarboniIOn measuring individual knowledge in organizationsOrgan Res Methods2007103449462
- HandwekerWPBorgattiSPReasoning with numbersBernardHRThe Handbook of Methods in Cultural AnthropologyLanham, MDAltamira Press1998549593
- DrennanJCognitive interviewing: verbal data in the design and pretesting of questionnairesJ Adv Nurs2003421576312641812
- ConradFBlairJFrom impressions to data: increasing the objectivity of congitive interviewsPaper presented at: American Statistical Association1996Alexandria, VA, USA
- PharmaQuest [homepage] Available at: http://www.corptransinc.com/pharmaquestAccessed January 5, 2017
- BasuNMcCleanAHarperLMarkers for work disability in anti-neutrophil cytoplasmic antibody-associated vasculitisRheumatology (Oxford)201453595395624489015
- CleanthousSNewmanSPShipleyMIsenbergDACanoSJWhat constitutes uncertainty in systemic lupus erythematosus and rheumatoid arthritis?Psychol Health201328217118822775405
- CleanthousSIsenbergDANewmanSPCanoSJPatient Uncertainty Questionnaire-Rheumatology (PUQ-R): development and validation of a new patient-reported outcome instrument for systemic lupus erythematosus (SLE) and rheumatoid arthritis (RA) in a mixed methods studyHealth Qual Life Outcomes2016143326927364
- PuechalXPagnouxCPerrodeauELong-term outcomes among participants in the WEGENT trial of remission-maintenance therapy for granulomatosis with polyangiitis (Wegener’s) or microscopic poly-angiitisArthritis Rheumatol201668369070126473755
- WildDGroveAMartinMISPOR Task Force for Translation and Cultural AdaptationPrinciples of good practice for the translation and cultural adaptation process for patient-reported outcomes (PRO) measures: report of the ISPOR task force for translation and cultural adaptationValue Health2005829410415804318
- WareJEJrSherbourneCDThe MOS 36-item short-form health survey (SF-36). I. conceptual framework and item selectionMed Care19923064734831593914
- RobsonJCMilmanNTomassonGExploration, development, and validation of patient-reported outcomes in antineutrophil cytoplasmic antibody-associated vasculitis using the OMERACT processJ Rheumatol201542112204220926329344