
Abstract
Purpose
Community pharmacies provide access to medicines and pharmaceutical services. Consequently, adequate availability and sufficient workforce capacity must be ensured for effective healthcare delivery. This study assessed the community pharmacy sector in Saudi Arabia, including density, workforce capacity, and evolution from 2007 to 2022.
Methods
This retrospective study measured community pharmacy infrastructure and workforce capacity using international indicators and standardized measures, including community pharmacy and community pharmacist density per 10,000 people and ratio of community pharmacists per pharmacy. Several data sources and platforms were used to collect the data including the Ministry of Health, Saudi General Authority for Statistics, and Ministry of Human Resources and Social Development.
Results
The number of community pharmacies increased by 89.30%, from 5466 in 2007 to 10,347 in 2022, and density increased from 2.25 to 3.22. However, density varied by region, from 3.97 to 1.95. The number of community pharmacists increased by 98.02%, from 10,932 in 2007 to 21,648 in 2022, and community pharmacist density increased from 4.51 to 6.73. However, the ratio of community pharmacists per pharmacy remained unchanged (2.0 in 2007 and 2.1 in 2022). Female pharmacists were first issued licenses to practice in community pharmacies in 2016, and the proportion of female pharmacists to total increased from 0.29% (n=42) in 2016 to 10.95% (n=2370) in 2022. The nationalization policy for community pharmacies was implemented in 2020, and the proportion of Saudi pharmacists increased from 3.08% (n=581) in 2019 to 19.90% (n=4306) in 2022, while proportion of expatriate pharmacists decreased from 96.92% (n=18,292) to 80.10% (n=17,342).
Conclusion
The findings showed that the community pharmacy sector in Saudi Arabia recently experienced substantial growth comparable to high-income countries. However, further improvements are required in some regions to increase community pharmacy density. Moreover, the ratio of pharmacists per pharmacy should be improved to meet the healthcare system needs.
Introduction
Community pharmacies are among the most accessible healthcare facilities in primary care settings. In addition, as healthcare professionals trusted by patients and community members, community pharmacists are often the first point of contact for patients and clients, particularly for self-care therapies, other-the-counter (OTC) medications, healthcare items, and advice and information on medications, diseases and medical equipment.Citation1–5 In addition, a key role of community pharmacies is dispensing prescription medications. Furthermore, other professional activities and patient care services have been increasingly introduced in community pharmacies in recent years in many countries, including Saudi Arabia.Citation1,Citation6–10 These include medication reviews, minor ailment management, smoking cessation programs, vaccination and immunization services,Citation11,Citation12 and point-of-care (POC) testing for chronic diseases.Citation13
Community pharmacists play an essential role in the healthcare system. They contribute to the safe, effective, and quality use of medicines, convenient access to medicines, and other health-related products and equipment in the primary care setting.Citation11,Citation13 Moreover, the current evidence suggests that community pharmacy-based interventions improve medication adherence and clinical management and control of chronic diseases,Citation14–17 reduce opioid-related harms,Citation18 facilitate smoking sessions and weight management,Citation16,Citation19 and have a positive impact on continuity of care for post-discharge patients.Citation20
Therefore, adequate availability, convenient access, and sufficient workforce capacity must be ensured to allow community pharmacies to play their roles in healthcare delivery.Citation21 Key indicators and standard measures, including community pharmacy and community pharmacist density per 10,000 people and ratio of community pharmacists per community pharmacy, are used to provide essential information about the community pharmacy infrastructure and workforce capacity.Citation22,Citation23 Community pharmacy density provides an indication of national pharmacy capacity and availability and accessibility of medicines and pharmaceutical services in the primary healthcare settings.Citation22,Citation24 The density of pharmacist per 10,000 people is a standardized measure of the availability of pharmacists in the healthcare system.Citation22,Citation23,Citation25,Citation26 The ratio of pharmacists per community pharmacy indicates the capacity to deliver pharmaceutical and healthcare services to the patients.Citation22 The community pharmacy infrastructure and workforce capacity vary widely across countries, regions, and states.Citation21,Citation22,Citation24,Citation27 For instance, according to a report by International Pharmaceutical Federation (FIP), the average density of community pharmacies per 10,000 people in Europe, Africa, and the Western Pacific in 2021 was 3.26, 0.95, and 2.62, respectively.Citation22
In Saudi Arabia, there have been major developments in community pharmacy practices in recent years, particularly in terms of regulations and policies related to human resources. Female pharmacists were previously unable to work in community pharmacies. However, in 2016, the Ministry of Health issued licenses to female pharmacists allowing them to work in private pharmacies. This was initially limited to pharmacies and herbal medicine stores located inside shopping malls and gradually expanded to the entire community pharmacy sector.Citation28,Citation29 This empowered female pharmacists to practice their profession in this large sector of the pharmacy profession and serve their communities. The other development included the decisions by Ministry of Human Resources and Social Development (HRSD) in early 2020 to increase the percentage of Saudi pharmacists working in community pharmacies.Citation30,Citation31 This was done because this sector is completely dependent on expatriate pharmacists (ie, over 98%) as well as to address the issue of increasing rate of unemployment of graduates from Pharmacy Colleges in Saudi Arabia.Citation32 Consequently, a nationalization/Saudization initiative of the pharmacy profession and its related specializations were issued in February 2020. This applied to all pharmacy entities with five or more pharmacists working in a pharmacy chain or group. The initiative required 20% Saudization by July 2020 and 30% by July 2021.Citation30,Citation31
However, studies utilizing standard measures to assess the community pharmacy landscape, workforce capacity, and temporal changes as well as studies assessing the impact of recent regulations and policies on the community pharmacy workforce in Saudi Arabia are lacking. Therefore, this study aimed to fill this gap by conducting a comprehensive analysis of community pharmacy density, community pharmacists’ workforce capacity, and evolution of the sector from 2007 to 2022. This study provides health policymakers and pharmacy leaders with valuable data and insights into this large sector of the healthcare system. This is particularly important, as the responsibility of dispensing of medicines and pharmaceutical services in primary care settings and many hospitals was transferred from government facilities to community pharmacies throughout Saudi Arabia using the national e-prescribing service Wasfaty.Citation33 The study findings could be used to provide further guidance for improving the pharmaceutical and patient care services in community pharmacies.
Materials and Methods
Study Design and Setting
This retrospective study was conducted to evaluate the state of the community pharmacy sector in Saudi Arabia and its progress from 2007 to 2022. This study measured the indicators of community pharmacy infrastructure and workforce capacity using internationally agreed-upon indicators and standardized measures by the International Pharmaceutical Federation (FIP) and World Health Organization (WHO), including community pharmacy density per 10,000 people, community pharmacist density per 10,000 people, ratio of community pharmacists per pharmacy, percentage of female community pharmacists, and percentage of foreign pharmacists.Citation22–26,Citation34
Data Sources and Collection
Several data sources and platforms were used to collect data, including the Ministry of Health website and statistical yearbooks for the years 2007–2022 (for data on the number of community pharmacists and community pharmacies),Citation35–50 the Saudi General Authority for Statistics (for data on the total population and population of each administrative region using the Saudi Census 2022),Citation51 the Ministry of Human Resources and Social Development (HRSD) website (for data, information, and ministerial decisions related to nationalization policy, date of implementation, targets, etc.),Citation30,Citation31 and media reports of authorities decisions to allow female pharmacists to work in private pharmacies.Citation28,Citation29 The collected data were used to measure the density of community pharmacies and community pharmacists per 10,000 people, calculate the ratio of community pharmacists per community pharmacy, determine growth trends, and assess the impact of regulations related to the community pharmacy workforce and other relevant aspects of community pharmacy practices.
Study Outcomes, Variables, and Calculation Methods
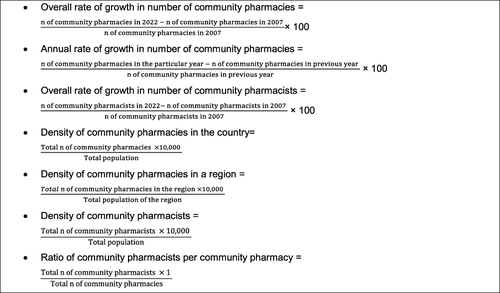
The study reported the total number of community pharmacies in Saudi Arabia in each year during the 16-year period of the study, calculated the annual and overall growth rates in the number of community pharmacies from 2007 to 2022, and assessed the distribution of pharmacies in the 13 administrative regions of Saudi Arabia. Moreover, the current density of community pharmacies and changes over the 16-year period were calculated. Furthermore, the study reported the number of community pharmacists each year during the study period and calculated the overall rate of growth. In addition, demographic data, including gender distribution (men and women) and nationality (Saudi and expatriate pharmacists), were analyzed and compared with other government and private healthcare sectors. The proportion of community pharmacists in the healthcare sector was determined and compared with that of other healthcare sectors. The evolution and current density of community pharmacists and ratio of community pharmacists to pharmacies were calculated. Moreover, the impact of recent policies and regulations related to community pharmacy human resources was assessed. Calculations were performed using the equations shown in .
Figure 1 Calculation methods used to measure the indicators (ie, rate, density and ratio).
In this study, community pharmacists were defined as licensed pharmacists who practice and work in community pharmacy settings, including chain and independent pharmacies. The healthcare sector included public and private institutions. The public healthcare sector included the Ministry of Health and other governmental agencies, such as the Armed Forces Medical Services, National Guard Medical Services, Ministry of Interior Medical Services, King Faisal Specialist Hospital and Research Center, Aramco Hospitals, Royal Commission Hospitals, and Ministry of Education Health Facilities. The private healthcare sector included hospitals, medical complexes, supportive service centers, and community pharmacies.Citation49 The percentage of community pharmacists was determined and compared to that of all practicing pharmacists in the healthcare sector (ie, direct services to clients/patients). Thus, pharmacists working in other non-healthcare sectors or in the pharmaceutical industry were excluded because the main focus was on the healthcare sector.
Data Management and Analysis
Data were entered into Microsoft Excel and organized. Data analysis included descriptive statistics, namely, frequencies, percentages, rates, and ratios. Data were visualized using bar and line charts.Citation52–54
Results
Current Status of Community Pharmacy Sector
As shown in , there were 10,347 community pharmacies in the 13 administrative regions of Saudi Arabia in 2022. These pharmacies serve a total population of 32,175,224 in Saudi Arabia. The average density of community pharmacies per 10,000 people is 3.22. In terms of the distribution of community pharmacies per region, the majority were located in the Riyadh region (32.95%) and Makkah region (25.14%), followed by the eastern region (9.65%), Aseer region (6.81%), Madinah region (5.63%), Jazan region (5.31%), and Qassim region (4.81%). The density of community pharmacies per 10,000 people varied among regions from 3.97 (Riyadh region), 3.91 (Jazan region) and 3.89 (Tabuk region) to 2.33 (Najran region), 2.25 (northern borders) and 1.95 (Eastern region).
Table 1 Number, Percentage, and Density of Community Pharmacies in Saudi Arabia by Administrative Region in 2022
Moreover, there were 21,648 community pharmacists in Saudi Arabia in 2022, with a density of 6.73 per 10,000 people. The ratio of community pharmacists per community pharmacy is 2.1.
The Rate of Growth of Community Pharmacies Over the Period of 2007-2022
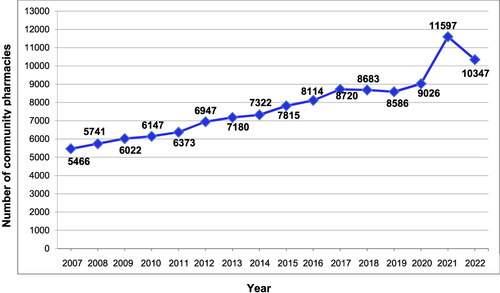
Over a period of 16 years, as shown in , the total number of community pharmacies increased from 5466 in 2007 to 10,347 in 2022, with an overall growth rate of 89.30%.
Figure 2 Number of community pharmacies in Saudi Arabia (2007–2022).
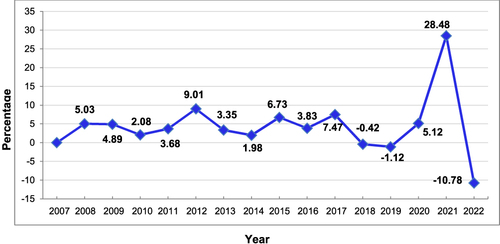
As shown in , at the national level, the highest overall growth rate was recorded in 2021 (28.48%), followed by 2012 (9.01%), 2017 (7.47%), and 2015 (6.73%). Conversely, 2018 and 2019 witnessed a slight decline in the growth of community pharmacies (–0.42% and –1.12%, respectively), and 2022 witnessed the highest decline (–10.78%).
Figure 3 Annual rate of growth of community pharmacies in Saudi Arabia (2007–2022).
Current State and Rate of Growth of Community Pharmacy Workforce
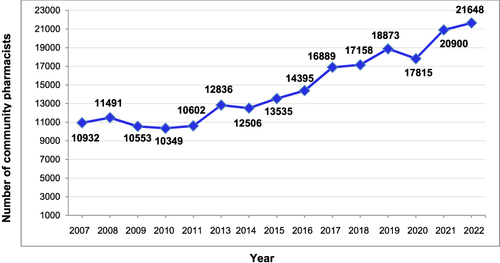
The number of community pharmacists increased from 10,932 in 2007 to 21,648 in 2022, with an overall growth rate of 98.02% ().
Figure 4 Number of community pharmacists (2007–2022).
Trends in Community Pharmacy and Pharmacist Density and Ratio of Pharmacists per Pharmacy
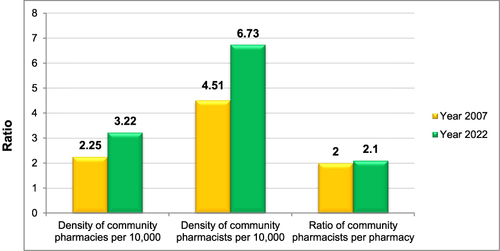
Trends in the availability and capacity of community pharmacies were compared between 2007 and 2022. As shown in , the density of community pharmacies per 10,000 people increased from 2.25 to 3.22 and that of community pharmacists increased from 4.51 to 6.73. However, the ratio of community pharmacists per pharmacy remained unchanged (2.0 in 2007 and 2.1 in 2022).
Figure 5 Density of community pharmacies and community pharmacists per 10,000 people and ratio of pharmacists per pharmacy in 2007 and 2022.
Number of Community Pharmacists in the Healthcare Sector
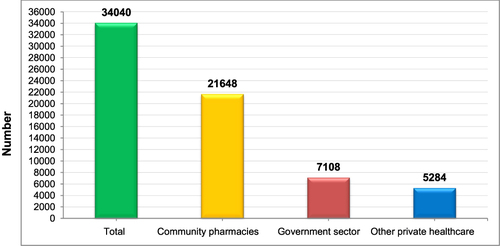
I calculated the proportion of community pharmacists to the total pharmacy workforce. In addition, I compared the number of community pharmacists with that of pharmacists in other areas of healthcare in the government (Ministry of Health and other government sectors: hospitals, and primary care centers) and private healthcare sectors (hospitals, medical complexes, and supportive service centers). As shown in , in 2022, community pharmacists represented 63.60% of the pharmacy workforce in the total healthcare sector and 80.38% of the pharmacists in the private healthcare sector.
Figure 6 Number of pharmacists by healthcare sector in 2022.
Trends in Workforce Proportions of Women and Saudi Community Pharmacists
As shown in , in the years 2016–2019, almost all the community pharmacists were male (over 99%). However, the proportion of female pharmacists has begun to increase. It increased from 0.29% (n=42) in 2016 to 10.95% (n=2370) in 2022. Similarly, the proportion of Saudi community pharmacists increased gradually from 1.49% (n=214) in 2016 to 19.90% (n=4306) in 2022.
Table 2 Distribution of Gender and Nationality of Pharmacists Working in Community Pharmacies in Saudi Arabia (2016–2022)a
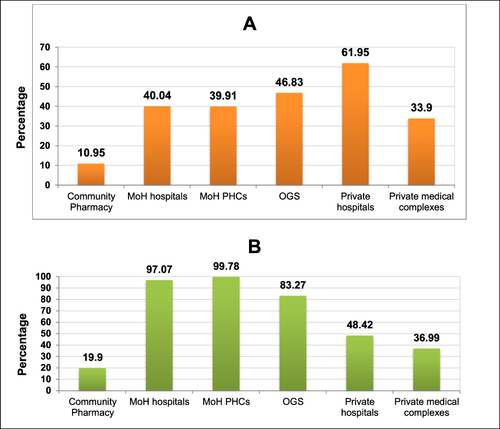
In addition, the proportions of female and Saudi community pharmacists were compared with that in other practice areas (ie, hospitals and institutional pharmacies) in government and private healthcare sectors. The results are presented in . The proportion of female pharmacists in community pharmacies was lower than in other practice areas. For example, female pharmacists represented only 10.95% of pharmacists in community pharmacies, compared with 61.95% and 40.04% of hospital pharmacists in private hospitals and MoH hospitals, respectively. Similarly, fewer Saudi pharmacists practice in community pharmacies than in other areas of pharmacy practice ( and ).
Table 3 Comparison of Community Pharmacists with Other Healthcare Sectors by Gender and Nationality (2022)
Figure 7 (A) Percentage of female pharmacists in community pharmacies compared to other healthcare sectors; (B) Percentage of Saudi pharmacists in community pharmacies compared to other healthcare sectors.
Impact of Policies and Regulations on Workforce Gender Distribution and Nationalization
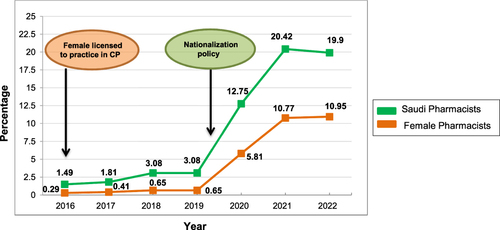
illustrates the impact of the regulations allowing women to practice in community pharmacies and of the nationalization policy of human resources in community pharmacies. More than 2370 female pharmacists were employed in community pharmacies between 2016 and 2022 (now represents 10.95% of the entire sector). The impact of the nationalization policy is illustrated in . The analysis showed that the number of Saudi pharmacists increased from 581 (3.08%) in 2019 to 4306 (19.90%) in 2022. A major increase in the number of female and Saudi pharmacists was witnessed in 2020, 2021, and 2022, with the combined effect of both regulations related to female pharmacists and nationalization policy.
Figure 8 Growth in percentage of female and Saudi pharmacists and association with regulations and policies.
Discussion
The findings showed that the community pharmacy sector witnessed rapid and substantial growth in recent years in Saudi Arabia. The number of community pharmacies tremendously increased by 89.30% during the period of 2007–2022. The rate of growth was higher than that reported in other countries, such as the US, Germany, and Jordan.Citation21,Citation55,Citation56 For instance, in the US, the number of community pharmacies increased by 6.3% from 63,752 in 2007 to 67,753 in 2015.Citation21 In Germany, the number of community pharmacies decreased from 21,476 in 2005 to 18,461 in 2021 (−14.0%).Citation56 The growth in the number of community pharmacies in Saudi Arabia led to an increase in the density of community pharmacies from 2.25 in 2007 to 3.22 in 2022. The density was higher than the community pharmacy density in 2019 in Sweden (1.4), Finland (1.5), the USA (1.9), the UK (2.1), Australia (2.3), and Hungary (2.3). The 2022 density in Saudi Arabia was similar to France (3.2) and Turkey (3.2) but lower than Ireland (3.8), Latvia (4.0), Belgium (4.2) and Spain (4.7).Citation27 The variation in community pharmacy density among countries could be attributed to the differences in healthcare systems in terms of common distribution channels of medicines and pharmaceutical products. Some countries rely on hospital pharmacies to dispense medications for outpatients, whereas other countries rely on community pharmacies.Citation27 In addition, in some countries (eg, Australia, Belgium, Spain), geographical criteria are used to prevent the concentration of pharmacies in the same area, and the minimum distance between community pharmacies is regulated.Citation27,Citation57 Moreover, in some countries (eg, Italy, France, Portugal), demographic criteria are used to issue a license to open a new pharmacy, with the most common criterion being the minimum number of inhabitants per new community pharmacy in a given county, city, municipality, or administrative region.Citation27,Citation57,Citation58 The growth in community pharmacies could be attributed to several factors. Community pharmacies in Saudi Arabia diversified their businesses and range of products to include medicines, non-pharmaceutical products, cosmetics, medical equipment and devices, and other items related to health and well-being. In addition, no restrictions were imposed on the minimum distances between community pharmacies. This sector recently appealed for investments, resulting in growth to meet the health and daily essential needs of the community members.
The density of community pharmacies varied widely among regions in Saudi Arabia from 3.97 in the Riyadh region to a lower density in other regions, eg, 2.25 in the northern borders region and 1.95 in the Eastern region. The variation among regions or states within the country has been reported in many countries, such as USA, Canada, and Germany.Citation21,Citation24,Citation56,Citation59 For instance, in Germany, in 2021, the community pharmacy density at the national level was 2.2 per 10,000 people, whereas the density varied among federal states: 2.0 in Berlin, 2.1 in Schleswig-Holstein, 2.6 in Saxony-Anhalt, and 2.9 in Saarland.Citation56 Similarly, in Canada, in 2019, the community pharmacy density at the national level was 2.8 per 10,000 people, whereas the density varied among provinces: 2.0 in Newfoundland, 2.7 in British Columbia, 3.2 in Nova Scotia, and 3.3 in Saskatchewan.Citation24 Thus, the community pharmacy density in Saudi Arabia could be further improved, particularly in regions with lower density, to ensure more convenient access to community pharmacy services.
The number of community pharmacists tremendously increased by 98.02%. Considering the increasing role of community pharmacists of healthcare delivery and ensuring safe, effective, and efficient access to medicines, community pharmacists density are increasing globally.Citation60 In Japan, number of community pharmacists increased by 32.9% from 135,716 in 2008 to 180,415 in 2018.Citation60 The increase in community pharmacy workforce led to an increase in the density of community pharmacists per 10,000 people in Saudi Arabia to be 6.73 in 2022. This density was higher than the global average of 5.14, similar to that in high-income countries (ie, 6.66) but lower than that in the European region (7.23).Citation22
The ratio of community pharmacists to pharmacies remained unchanged (2.00 in 2007 and 2.1 in 2022). This could be because the growth rate of community pharmacies was comparable to that of community pharmacists. In comparison, according to a FIP report, the global average was 1.68, with large variations across countries with different income levels (0.46 in low-income countries; 2.21 in high-income countries) and across WHO regions (eg, 2.19 in European region, 1.69 Western Pacific region, and 0.71 in African region).Citation22 Consequently, there is a scope for further improvements in this indicator. This is particularly important, as increasing the ratio would help community pharmacies diversify their pharmaceutical services and provide more patient care services. Community pharmacies in Saudi Arabia operate for extended hours, including 24 hours.Citation33 Consequently, a pharmacist cannot manage all the functions of the pharmacy, including dispensing prescriptions and OTC medicines, patient counselling, and handling patient requests, as well as provide patient care services, such as vaccination and chronic disease management, in one shift. In 2019, the service of dispensing medicines was transferred from government public primary care centers (PHCs) and hospitals to community pharmacies using the national e-prescribing service (Wasfaty service). As of September 2023, community pharmacies served more than 2191 PHCs and 236 hospitals.Citation61 This led to a higher workload, stress and difficulties in smoothly incorporating the service into routine practice due to the shortage in the current number of pharmacists per community pharmacy.Citation62 This emphasizes the need to improve the ratio of pharmacists per community pharmacy to ensure quality patient care services.
The study results showed that community pharmacists were the largest sector of pharmacy practices in Saudi Arabia representing 63.60% of all pharmacists practicing in the healthcare sector (ie, patient care settings). This was consistent with previous reports.Citation34,Citation55,Citation63,Citation64 For instance, in Canada, approximately 70% of pharmacists work in community pharmacies, 15% in hospitals, and 15% in other settings.Citation65 According to data from the US Bureau of Labor Statistics in 2022, the largest employers for pharmacists were pharmacies and drug stores (42%) and hospitals (27%).Citation66 This emphasizes the importance of this sector, as it has the most job opportunities for pharmacy graduates, considering the limited vacancies in other areas, such as government hospitals.Citation32,Citation67,Citation68 Moreover, as previously mentioned, medicine dispensing services were transferred to community pharmacies. Consequently, community pharmacies have become the main channel of medicine supply in ambulatory care settings.
Before 2016, the community pharmacy sector in Saudi Arabia was entirely dependent on expatriate pharmacists (>99%). However, the Ministry of Human Resources and Social Development (HRSD) issued ministerial decisions to increase the percentage of Saudi graduates working in community pharmacies in early 2020.Citation30,Citation31 This study findings showed that the number of Saudi pharmacists increased significantly after the implementation of this regulation. This increase is expected to continue, considering the limited employment opportunities in hospital pharmacy settings, particularly in the public health sector (ie, Ministry of Health and other public health institutions), due to saturationCitation67–69 and the trend of employment in the private sector, including community pharmacies.Citation70 In addition, the impact of the Ministry of Health decision in 2016 to issue licenses to female pharmacists for employment in private pharmacies was evident.Citation28,Citation29 This decision empowered female pharmacists in Saudi Arabia to practice their profession in this large pharmaceutical sector and overcome the unemployment of pharmacists, particularly female graduates.Citation67 Although the proportion of female pharmacists increased, it remains low, particularly in the community pharmacy sector, as it currently stands at 10.95%. The global average of female pharmacists in the pharmacy workforce was estimated to be 56%, exceeding 65% in some WHO regions, such as Europe and the Americas.Citation34 Therefore, efforts to address barriers and challenges in the employment of female pharmacists in this sector are needed. This is particularly important, as women represented 54.20% of all students enrolled in 21 pharmacy colleges in the public sector (6628 out of 12,228) in the 2022/2023 academic year.Citation50
The results of this study have several implications. Although the average community pharmacy density at the national level was comparable to that of high-income countries, it varied widely among administrative regions. Therefore, the community pharmacy density in some regions requires improvements. In addition, the ratio of community pharmacists to pharmacies should be increased to ensure that pharmacies deliver high-quality pharmaceutical and patient care services. This is particularly important considering the recent expansion in the role of community pharmacists in primary care settings. Thus, the current ratio could be insufficient, particularly because pharmacies often operate extended hours. Scarcity of pharmacists could limit the scope of professional services and delivery of advanced patient care services due to focusing on essential roles, such as dispensing medications. Considering the recent policies and regulations, community pharmacies are currently the largest sector with the most job opportunities for pharmacy graduates. Consequently, pharmacy colleges in Saudi Arabia should ensure that their graduates are fully prepared to work in this sector. This includes adequate components in both didactic and experiential curricula regarding community pharmacy practices. This is particularly essential, as previous studies have indicated that education and training in some undergraduate pharmacy curricula are inadequate.Citation67,Citation71
Strengths and Limitations
This study provided original contributions and insights into the current landscape of community pharmacies in Saudi Arabia. This was the first study to comprehensively assess community pharmacy density and workforce capacity, including trends and capacity growth, over a 16-year period. Moreover, this study used internationally standardized measures, indicators, and calculation methods to determine density and capacity. This allowed for comparison with other countries and regions. However, this study had some limitations. The study did not assess community pharmacy support personnel, as data on this aspect were not available. However, this was beyond the scope of the present study. Future studies should address this issue. In addition, future studies could examine the geographic distribution and locations of pharmacies in cities, governorates, and towns, including utilizing geographic information systems to quantify population access and driving distance to community pharmacies. This study provided valuable data and insights into the current state of community pharmacies. In addition, this study could provide guidance for healthcare policymakers in planning human resources and community pharmacies, which is particularly important considering the new developments and additional roles of community pharmacists in Saudi Arabia.
Conclusion
The community pharmacy sector recently witnessed rapid and substantial growth in Saudi Arabia, with the density of community pharmacies and community pharmacists comparable to that of high-income countries. However, further improvements are required in some regions to increase community pharmacy density and improve pharmacy accessibility. In addition, the ratio of community pharmacists per pharmacy should be improved to expand professional pharmaceutical services and meet the needs of the healthcare system. Moreover, efforts should be made to increase the numbers of female and Saudi pharmacists in the pharmacy workforce.
Abbreviations
CPs, community pharmacists; FIP, International Pharmaceutical Federation; MoH, Ministry of Health; HRSD, Ministry of Human Resources and Social Development; OGS, other government sector; OTC, over-The-counter; PHCs, primary health centers; POC, point-of-care; UK, United Kingdom; US, United States; WHO, World Health Organization.
Data Sharing Statement
The data associated with this study are available from the corresponding author upon reasonable request.
Ethics Statement
The data analyzed in this study were collected from publicly available sources in the public domain. Hence, no ethics approval was required.Citation24,Citation72–74
Disclosure
The author reports no conflicts of interest in this work.
Additional information
Funding
References
- Melton BL, Lai Z. Review of community pharmacy services: what is being performed, and where are the opportunities for improvement? Integrat Pharm Res Pract. 2017;6:79–89.
- Eades CE, Ferguson JS, O’Carroll RE. Public health in community pharmacy: a systematic review of pharmacist and consumer views. BMC Public Health. 2011;11:582. doi:10.1186/1471-2458-11-582
- Kelling SE. Exploring accessibility of community pharmacy services. Innov Pharm. 2015;2015:6.
- Hermansyah A, Sainsbury E, Krass I. Community pharmacy and emerging public health initiatives in developing S outheast A sian countries: a systematic review. Health Soc Care Community. 2016;24:e11–e22. doi:10.1111/hsc.12289
- Alrasheedy AA, Abdulsalim S, Farooqui M, Alsahali S, Knowledge GB. Attitude and Practice About Coronavirus Disease (COVID-19) pandemic and its psychological impact on students and their studies: a cross-sectional study among pharmacy students in Saudi Arabia. Risk Manag Healthc Policy. 2021;14:729–741. doi:10.2147/RMHP.S292354
- Urick BY, Meggs EV. Towards a greater professional standing: evolution of pharmacy practice and education, 1920–2020. Pharmacy. 2019;7. doi:10.3390/pharmacy7030098
- Thomson K, Hillier-Brown F, Walton N, Bilaj M, Bambra C, Todd A. The effects of community pharmacy-delivered public health interventions on population health and health inequalities: a review of reviews. Preventive Med. 2019;124:98–109. doi:10.1016/j.ypmed.2019.04.003
- DiPietro Mager N, Bright D. Advancing public health through community pharmacy practice. Pharmacy. 2023;11:56. doi:10.3390/pharmacy11020056
- Algarni MA, Alsheikh MY, Fathelrahman AI, et al. Home drug delivery service from the perspective of community pharmacy staff in Saudi Arabia. Pharmacy. 2022;10:162. doi:10.3390/pharmacy10060162
- Almanasef M, Almaghaslah D, Kandasamy G, Vasudevan R, Batool S. Involvement of community pharmacists in public health services in Asir Region, Saudi Arabia: a cross-sectional study. Int J Clin Pract. 2021;75:e14940. doi:10.1111/ijcp.14940
- Raiche T, Pammett R, Dattani S, et al. Community pharmacists’ evolving role in Canadian primary health care: a vision of harmonization in a patchwork system. Pharm Pract. 2020;2020:18.
- Bach AT, Goad JA. The role of community pharmacy-based vaccination in the USA: current practice and future directions. Integrat Pharm Res Pract. 2015;4:67–77. doi:10.2147/IPRP.S63822
- Strand MA, Bratberg J, Eukel H, Hardy M, Williams C. Community pharmacists’ contributions to disease management during the COVID-19 pandemic. Prev Chronic Dis. 2020;17:E69. doi:10.5888/pcd17.200317
- Milosavljevic A, Aspden T, Harrison J. Community pharmacist-led interventions and their impact on patients’ medication adherence and other health outcomes: a systematic review. Int J Pharm Pract. 2018;26:387–397. doi:10.1111/ijpp.12462
- Mehuys E, Van Bortel L, De Bolle L, et al. Effectiveness of a community pharmacist intervention in diabetes care: a randomized controlled trial. J Clin Pharm Therapeutics. 2011;36:602–613. doi:10.1111/j.1365-2710.2010.01218.x
- Buss VH, Shield A, Kosari S, Naunton M. The impact of clinical services provided by community pharmacies on the Australian healthcare system: a review of the literature. J Pharm Policy Pract. 2018;11:22. doi:10.1186/s40545-018-0149-7
- DiDonato KL, May JR, Lindsey CC. Impact of wellness coaching and monitoring services provided in a community pharmacy. J Am Pharm Assoc. 2013;53:14–21. doi:10.1331/JAPhA.2013.11227
- Bach P, Hartung D. Leveraging the role of community pharmacists in the prevention, surveillance, and treatment of opioid use disorders. Addict Sci Clin Pract. 2019;14:30. doi:10.1186/s13722-019-0158-0
- Tamara JB, Adam T, Claire O, et al. Community pharmacy-delivered interventions for public health priorities: a systematic review of interventions for alcohol reduction, smoking cessation and weight management, including meta-analysis for smoking cessation. BMJ Open. 2016;6:e009828. doi:10.1136/bmjopen-2015-009828
- Melody KT, McCartney E, Sen S, Duenas G. Optimizing care transitions: the role of the community pharmacist. Integrat Pharm Res Pract. 2016;5:43–51. doi:10.2147/IPRP.S87947
- Qato DM, Zenk S, Wilder J, Harrington R, Gaskin D, Alexander GC. The availability of pharmacies in the United States: 2007–2015. PLoS One. 2017;12:e0183172. doi:10.1371/journal.pone.0183172
- International Pharmaceutical Federation. FIP Community pharmacy at a glance 2021 - Regulation, scope of practice, remuneration and distribution of medicines through community pharmacies and other outlets. Available from: https://www.fip.org/file/5015. Accessed February 4, 2023.
- World Health Organization. National health workforce accounts: a handbook. Available from: https://score.tools.who.int/tools/optimize-health-service-data/tool/national-health-workforce-accounts-nhwa-a-handbook-44/. Accessed February 4, 2023.
- Grootendorst P. Pharmacy location and medical need: regional evidence from Canada. BMC Health Serv Res. 2022;22:1309. doi:10.1186/s12913-022-08709-5
- International Pharmaceutical Federation (FIP). Pharmacy workforce intelligence: global trends report. Available from: https://www.fip.org/file/2077. Accessed March 4, 2023.
- World Health Organization. Pharmacists (per 10 000 population). Available from: https://www.who.int/data/gho/data/indicators/indicator-details/GHO/pharmacists-(per-10-000-population). Accessed March 4, 2023.
- OECD. ”Pharmacists and pharmacies” in Health at a Glance 2021: OECD Indicators. Available from: https://www.oecd-ilibrary.org/sites/d6227663-en/index.html?itemId=/content/component/d6227663-en. Accessed March 4, 2023.
- Alriyadh Newspaper. Saudi Women are allowed to work in pharmacies located in shopping malls Available from: https://www.alriyadh.com/1545443. Accessed March 10, 2023.
- Saudi Gazette. Women allowed to work in pharmacies. Available from: https://saudigazette.com.sa/article/166667. Accessed March 10, 2023.
- Ministry of Human Resources and Social Development (HRSD) SA. Ministerial Decision to localize the pharmacy profession and its related disciplines. Available from: https://www.hrsd.gov.sa/sites/default/files/2023-02/e109044_0.pdf. Accessed March 3, 2023.
- Ministry of Human Resources and Social Development (HRSD) SA. Procedural guide on the decision to localize pharmacy profession and its specializations Available from: https://www.hrsd.gov.sa/sites/default/files/2020-02/11102021.pdf. Accessed March 3, 2023.
- AlRuthia Y, Alsenaidy MA, Alrabiah HK, AlMuhaisen A, Alshehri M. The status of licensed pharmacy workforce in Saudi Arabia: a 2030 economic vision perspective. Hum Resour Health. 2018;16:28. doi:10.1186/s12960-018-0294-8
- Al Aloola N, Aljudaib S, Behery F, Alwhaibi M, Alhawassi T. Perception of the community toward transition of pharmaceutical care services from ministry of health primary healthcare centers to community pharmacies. Int J Healthc. 2013;9:21–29. doi:10.5430/ijh.v9n1p21
- Bates I, John C, Bruno A, Fu P, Aliabadi S. An analysis of the global pharmacy workforce capacity. Hum Resour Health. 2016;14:61. doi:10.1186/s12960-016-0158-z
- Ministry of Health SA. Statistical Yearbook 2007. Available from: https://www.moh.gov.sa/Ministry/Statistics/book/Pages/default.aspx. Accessed February 21, 2023.
- Ministry of Health SA. Statistical Yearbook 2008. Available from: https://www.moh.gov.sa/Ministry/Statistics/book/Pages/default.aspx. Accessed February 21, 2023.
- Ministry of Health SA. Statistical Yearbook 2009. Available from: https://www.moh.gov.sa/Ministry/Statistics/book/Pages/default.aspx. Accessed February 21, 2023.
- Ministry of Health SA. Statistical Yearbook 2010. Available from: https://www.moh.gov.sa/Ministry/Statistics/book/Pages/default.aspx. Accessed February 21, 2023.
- Ministry of Health SA. Statistical Yearbook 2011. Available from: https://www.moh.gov.sa/Ministry/Statistics/book/Pages/default.aspx. Accessed February 21, 2023.
- Ministry of Health SA. Statistical Yearbook 2012. Available from: https://www.moh.gov.sa/Ministry/Statistics/book/Documents/1433.pdf. Accessed February 21, 2023.
- Ministry of Health SA. Statistical Yearbook 2013. Available from: https://www.moh.gov.sa/Ministry/Statistics/book/Documents/%D8%A7%D9%84%D9%83%D8%AA%D8%A7%D8%A8%20%D8%A7%D9%84%D8%A5%D8%AD%D8%B5%D8%A7%D8%A6%D9%8A%20%D8%A7%D9%84%D8%B3%D9%86%D9%88%D9%8A%201434%D9%87%D9%80.pdf. Accessed February, 21, 2023.
- Ministry of Health SA. Statistical Yearbook 2014. Available from: https://www.moh.gov.sa/Ministry/Statistics/book/Documents/1435.pdf. Accessed February 21, 2023.
- Ministry of Health SA. Statistical Yearbook 2015. Available from: https://www.moh.gov.sa/Ministry/Statistics/book/Documents/%D8%A7%D9%84%D9%83%D8%AA%D8%A7%D8%A8%20%D8%A7%D9%84%D8%A5%D8%AD%D8%B5%D8%A7%D8%A6%D9%8A%20%D8%A7%D9%84%D8%B3%D9%86%D9%88%D9%8A%20%D9%84%D8%B9%D8%A7%D9%85%201436%D9%87%D9%80.pdf. Accessed February 21, 2023.
- Ministry of Health SA. Statistical Yearbook 2016. Available from: https://www.moh.gov.sa/Ministry/Statistics/book/Documents/2017-08-24-01000.pdf. Accessed February 21, 2023.
- Ministry of Health SA. Statistical Yearbook 2017. Available from: https://www.moh.gov.sa/Ministry/Statistics/book/Documents/%D8%A7%D9%84%D9%83%D8%AA%D8%A7%D8%A8%20%D8%A7%D9%84%D8%A5%D8%AD%D8%B5%D8%A7%D8%A6%D9%8A%201438.pdf. Accessed February, 21, 2023.
- Ministry of Health SA. Statistical Yearbook 2018. Available from: https://www.moh.gov.sa/Ministry/Statistics/book/Documents/book-Statistics-2018.pdf. Accessed February, 21, 2023.
- Ministry of Health SA. Statistical Yearbook 2019. Available from: https://www.moh.gov.sa/Ministry/Statistics/book/Pages/default.aspx. Accessed February 21, 2023.
- Ministry of Health SA. Statistical Yearbook 2020. Available from: https://www.moh.gov.sa/Ministry/Statistics/book/Pages/default.aspx. Accessed February 21, 2023.
- Ministry of Health SA. Statistical Yearbook 2021. Available from: https://www.moh.gov.sa/Ministry/Statistics/book/Documents/1Statistical-Yearbook-2021.pdf. Accessed February 21, 2023.
- Ministry of Health SA. Statistical Yearbook 2022. Available from: https://www.moh.gov.sa/Ministry/Statistics/book/Pages/default.aspx. Accessed September 21, 2023.
- General Authority for Statistics SA. Saudi Census 2022. Available from: https://portal.saudicensus.sa/portal/public/1/15/101462. Accessed March 3, 2023.
- Cooksey RW. Descriptive Statistics for Summarising Data. In: Cooksey RW, editor. Illustrating Statistical Procedures: Finding Meaning in Quantitative Data. Singapore: Springer Singapore; 2020:61–139.
- Kaliyadan F, Kulkarni V. Types of variables, descriptive statistics, and sample size. Indian Dermatol Online J. 2019;10:82–86. doi:10.4103/idoj.IDOJ_468_18
- Kaur P, Stoltzfus J, Yellapu V. Descriptive statistics. Int J Acad Med. 2018;2018:4.
- Basheti IA, Mhaidat NM, Alqudah R, Nassar R, Othman B, Mukattash TL. Primary health care policy and vision for community pharmacy and pharmacists in Jordan. Pharm Pract. 2020;18:2184. doi:10.18549/PharmPract.2020.4.2184
- ABDA – Federal Union of German Associations of Pharmacists. German pharmacies – figures, data, and facts 2022. Available from: https://www.abda.de/fileadmin/user_upload/assets/ZDF/ZDF22/ABDA_ZDF_2022_Brosch_english.pdf. Accessed March 7, 2023.
- World Health Organization. Regional Office for Europe. The legal and regulatory framework for community pharmacies in the WHO European Region. Available from: https://iris.who.int/handle/10665/326394. Accessed April 4, 2023.
- Pagano E, Pagliero M, Pivetta EEG, Richiardi L. “Pharmacists in Italy”, in Grease or Grit? International case studies of occupational licensing and its effects on efficiency and quality. Upjohn Institute for Employment Research; 2022:51–74.
- Berenbrok LA, Tang S, Gabriel N, et al. Access to community pharmacies: a nationwide geographic information systems cross-sectional analysis. J Am Pharm Assoc. 2022;62:1816–22.e2. doi:10.1016/j.japh.2022.07.003
- Iguchi K, Ueyama M, Nishio H, et al. Impact of the increase in the number of community pharmacists on their geographical distribution in Japan: a retrospective survey. J Pharm Policy Pract. 2022;15:96. doi:10.1186/s40545-022-00499-9
- Wasfaty, an electronic prescribing service by NUPCO. Available from: https://wasfaty.sa/. Accessed September 25, 2023.
- Khardali A, Qadri M, Saad SA. Exploring community pharmacists’ attitudes towards the use of wasfaty (e-Prescribing) Service in Jazan Province, Saudi Arabia. Lat Am J Pharm. 2022;41:2375–2382.
- Eickhoff C, Griese-Mammen N, Müeller U, Said A, Schulz M. Primary healthcare policy and vision for community pharmacy and pharmacists in Germany. Pharm Pract. 2021;2021:19.
- Melo AC, Trindade GM, Freitas AR, Resende KA, Palhano TJ. Community pharmacies and pharmacists in Brazil: a missed opportunity. Pharm Pract. 2021;2021:19.
- Canadian Pharmacists Association. Pharmacists in Canada. Available from: https://www.pharmacists.ca/pharmacy-in-canada/pharmacists-in-canada/. Accessed April 7, 2023.
- Bureau of Labor Statistics at U.S. Department of Labor. Occupational Outlook Handbook, Pharmacists. Available from: https://www.bls.gov/ooh/healthcare/pharmacists.htm#tab-3. Accessed September 20, 2023.
- Balkhi B, Alghamdi A, Alhossan A, Alhamami A, Asiri YA. Pharmacy students attitude and perception toward working in community pharmacy in Saudi Arabia. Saudi Pharm J. 2020;28:397–402. doi:10.1016/j.jsps.2020.01.021
- Almaghaslah D, Alsayari A. Using a global systematic framework tool to identify pharmacy workforce development needs: a national case study on Saudi Arabia. Risk Manag Healthc Policy. 2021;14:3233–3245. doi:10.2147/RMHP.S322577
- Almaghaslah D, Alsayari A, Asiri R, Albugami N. Pharmacy workforce in Saudi Arabia: challenges and opportunities: a cross‐sectional study. Int J Health Plann Manag. 2019;34:e583–e93. doi:10.1002/hpm.2674
- Alrasheedy AA, Ibrahim MH, Alsahali S, et al. Current state of career placement and employment opportunities for Doctor of Pharmacy graduates: a cross-sectional analysis from a college of pharmacy, Saudi Arabia. Saudi Pharm J. 2022;30:1479–1485. doi:10.1016/j.jsps.2022.07.010
- Almaghaslah D, Alsayari A, Almanasef M, Asiri A. A cross-sectional study on pharmacy students’ career choices in the light of Saudi vision 2030: will community pharmacy continue to be the most promising, but least preferred, sector? Int J Environ Res Public Health. 2021;18. doi:10.3390/ijerph18094589
- Basudan AM. Breast cancer incidence patterns in the Saudi female population: a 17-year retrospective analysis. Medicina. 2022;58:1617. doi:10.3390/medicina58111617
- Stoecker C. Shooting from the ‘Scrip: scope of practice laws and access to immunizations in the pharmacy setting. Vaccines. 2021;9:444. doi:10.3390/vaccines9050444
- Alshammari TM, Alsubait SI, Alenzi KA, Almalki ZS. Estimating the potential economic impact of the Wasfaty program on costs of antidiabetic treatment: an initiative for the digital transformation of health. Saudi Pharm J. 2023;31:1029–1035. doi:10.1016/j.jsps.2023.04.026