Abstract
Eslicarbazepine is a new dibenzazepine antiepileptic agent. It is a high affinity antagonist of the voltage-gated sodium channel. It is closely related to both carbamazepine and oxcarbazepine. Eslicarbazepine has similar affinity to inactivated sodium channels (channels in just activated neurons) as carbamazepine, and greater efficacy in animal models of seizure than oxcarbazepine. In human placebo-controlled trials of a single daily dose of eslicarbazepine added to other anti-epileptic agents, significant seizure reductions occurred with 800 and 1200 mg daily, with nearly half of the patients experiencing a greater than 50% reduction in seizure frequency. Adverse events (AEs) occurred in over 50% of patients receiving therapeutic doses of eslicarbazepine (compared to 31.4%–44.7% of placebo-treated subjects), but were generally mild or moderate. Eight to 19.6% of eslicarbazepine treated patients discontinued due to AEs (compared to 3.9%–8.5% of placebo-treated subjects). In these patients receiving combination anticonvulsant therapy, the most common AEs were dizziness, nausea and vomiting, somnolence, and diplopia. Eslicarbazepine is an effective and reasonably well-tolerated adjunct in patients with suboptimal control of their partial seizures.
Seizures are among the most common chronic neurologic problems encountered in medical practice. Focal- or partial-onset epilepsy, defined as recurrent, unprovoked episodes of abnormal electrical activity that begin in one part of the brain, is the most common form of epilepsy diagnosed in adults with an annual incidence of 10 to 15 per 100,000 in young- to middle-aged adults and an annual incidence as high as 70 per 100,000 in adults over age 60.Citation1 The prevalence of partial onset epilepsy in the United States and Europe has been estimated between 3 and 10 per 1000.Citation2,Citation3 The goal of seizure management is complete seizure control with minimal side effects. Quality of life (QoL) studies have suggested that patients who suffer even a single seizure per year have a reduced QoL.Citation4 Seizures, especially convulsive seizures, are associated with significant morbidity and mortality, including a higher incidence of accidental drowning, fractures, head and soft-tissue injuries, and serious motor vehicle accidents.Citation5 Severe burn injuries are also more likely as patients with epilepsy are overrepresented in burn units.Citation6 The economic and social impact of uncontrolled seizures is also significant. Lost productivity due to seizures is a major ‘indirect cost’ of epilepsy.Citation7 Driving restrictions in the United States vary by state with some states prohibiting driving for as long as 12 months after a single seizure.Citation8
Complete seizure control is not easily achieved. In one large observational study, only 47% of patients became seizure free following initial monotherapy with an appropriately chosen anti-epileptic drug (AED), and only 63% of patients ultimately became seizure-free with medical management.Citation9 Side-effects of AEDs are common, and frequently contribute to non-compliance. Newer AEDs, while not necessarily more effective at controlling seizures, clearly have fewer drug-drug interactions and may be better tolerated.Citation10 Laboratory monitoring for hematologic and metabolic effects is often unnecessary with newer AEDs, although idiosyncratic reactions still occur. On the other hand, potential teratogenicity and effects of long-term therapy are better understood in older AEDs. Given the prevalence of epilepsy which is refractory to currently available medications, new agents with favorable efficacy and tolerability are desirable.
Eslicarbazepine acetate (Stedesa™ in the United States; Zebinix®, Exalief® in Europe; chemical name (S)-(–)-10-acetoxy-10,11-dihydro-5H-dibenz[b,f]azepine-5-carboxamide; development name BIA 2-093), is a new dibenzazepine that has documented efficacy as an adjunct agent in patients with inadequately controlled partial-onset seizures. It is currently being reviewed by the United States Food and Drug Administration and has been approved by the European Medicines Agency (EMEA) in the European Union. Additionally, it is undergoing investigation for mono-therapy treatment of partial epilepsy and bipolar illness.
Pharmacology
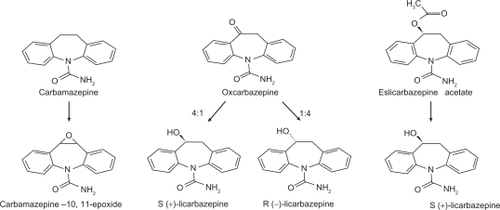
Eslicarbazepine is administered as the acetate salt which is rapidly and nearly completely reduced by esterases in the liver to the S enantiomer, S-licarbazepine or eslicarbazepine (BIA 2-005) (). This is the active form in the brain and accounts for approximately 95% of the metabolic product of the parent pro-drug.Citation11 The inactive R enantiomer and oxcarbazepine account for less than 5% of the metabolic product.Citation11,Citation12 It is important to note that eslicarbazepine is the active metabolite of oxcarbazepine. Oxcarbazepine is actually a pro-drug that is metabolized into both the S and R enantiomers of licarbazepine at a ratio of 4 or 5 to 1.Citation12,Citation13 The nearly complete conversion of eslicarbazepine acetate to the active eslicarbazepine is believed to be the mechanism leading to fewer adverse neurological consequences in rats than oxcarbazepine,Citation14 and more consistent anti-seizure effect than oxcarbazepine in a rat electroshock seizure model.Citation12
Figure 1 Eslicarbazepine is formed by reduction of the acetate salt (shown on the right) or may be found as the predominant (4:1) active metabolite of oxcarbazepine (middle). Carbamazepine and its active epoxide metabolite are shown on the left. Reprinted with permission from Almeida L, Soares-da-Silva P. Eslicarbazepine acetate (BIA 2-093). Neurotherapeutics. 2007;4:88–96.Citation12 Copyright © 2007 Elsevier.
Mechanism of action
Eslicarbazepine binds avidly and blocks the inactivated voltage-gated sodium channel (VGSC). The VGSC is the major source of sodium entry when a neuron depolarizes, and consequently allows for the action potential to propagate. VGSCs have 3 states. In the deactivated or resting state, the VGSC is closed, but the channel is responsive to a depolarization signal. When the cell depolarizes, the VGSC opens to allow sodium ion entry. After the action potential, the VGSC enters an inactivated state, in which it is closed and not responsive to voltage changes.Citation15 Eslicarbazepine binds to the inactivated form of the VGSC and prevents its reversion to the receptive resting or deactivated form.Citation16,Citation17 This means that eslicarbazepine binds to more active neurons preferentially. This mechanism is shared by carbamazepine, oxcarbazepine, and other anticonvulsants.Citation17,Citation18 The affinity of eslicarbazepine to the inactivated form of the VGSC is similar to that of carbamazepine, but its affinity to the resting form of VGSC is some 3 times less.Citation12,Citation17 This suggests that eslicarbazepine is less likely to bind to normally active neurons, and therefore, less likely to cause adverse neurological consequences. Indeed when compared with either carbamazepine or oxcarbazepine, eslicarbazepine had less neurologic impairment in rats,Citation14 and was less toxic to cultured hippocampal neurons.Citation19
Pharmacokinetics
Bioavailability of eslicarbazepine in a liquid suspension or tablet formulations is equivalent.Citation20 Food does not affect the absorption or subsequent drug levels.Citation21,Citation22 The possible effect of gender on pharmacokinetics was studied in 24 healthy subjects (12 male) who received eslicarbazepine for 8 days. There were no significant differences in the bioavailability of the drugs, although women absorbed more drug than men.Citation23 Finally, age did not affect absorption when young (age 18–40 years, n = 12) and older (age > 65 years, n = 12) subjects received 600 mg in a single dose.Citation11
The time to maximal serum concentration for the therapeutic doses of 900 or 1200 mg/day, or up to 2400 mg/day, ranges from 2.3 to 4 hours.Citation12 Both the rate and the area under the curve (AUC) increased in a linear fashion with increasing dose (400–2400 mg/day). The effective half-life of eslicarbazepine is approximately 20 to 24 hours, with steady state being reached in 4 to 5 days.Citation12
Eslicarbazepine acetate is metabolized to eslicarbazepine very rapidly in the liver. Levels of the parent drug, eslicarbazepine acetate, are too low to be measureable after single or multiple doses.Citation12 Eslicarbazepine is eliminated exclusively by the kidney and 91% of the drug is recovered in the urine.Citation24 Clearance from the plasma occurs at a consistent rate of 20 to 30 mL/min.Citation12 Approximately 20% of the dose is recovered in the urine after 12 hours, and 40% within 24 hours.Citation12,Citation25 Subjects with moderate hepatic impairment (n = 8) break down eslicarbazepine acetate more slowly, so that its levels can actually be detected, but this difference does not significantly alter the pharmacokinetics.Citation24 Subjects with mild renal impairment (n = 8) eliminate eslicarbazepine more slowly than healthy controls (10.2 mL/min vs 17.3 mL/min in controls), but this not clinically significant.Citation26 However, subjects with moderate (n = 8) or severe renal impairment (n = 8) clear eslicarbazepine much more slowly (3.7 mL/min and 1.5 mL/min, respectively).Citation26 Eslicarbazepine is cleared with dialysis in subjects with end-stage kidney disease requiring dialysis.Citation26
Enantiomer-specific levels can be measured with high performance liquid chromatography separation and ultraviolet light detection method.Citation27 Levels at therapeutic doses ranged from 4.7 ± 4.0 μg/mL for 800 mg/day to 8.9 ± 6.6 μg/mL for 1200 mg/day.Citation28
Pharmacokinetic interactions have been observed between eslicarbazepine and other commonly used antiepileptic drugs, similar to interactions seen with oxcarbazepine ().Citation29 Steady state levels of eslicarbazepine were associated with a significant increase in both phenytoin and phenobarbital, possibly due to inhibition of the hepatic enzyme CYP2C19.Citation29 Conversely, phenytoin and phenobarbital increased clearance of eslicarbazepine, and a 33% decrease in eslicarbazepine exposure was noted with concomitant phenytoin therapy.Citation29 Small, possibly insignificant increases in clearance of topiramate, lamotrigine and carbamazepine were seen with concomitant use of eslicarbazepine, while a significant increase in eslicarbazepine clearance was noted with concomitant carbamazepine therapy.Citation29 Other commonly used medications which may be affected by eslicarbazepine include warfarin and hormonal contraceptives.Citation12 Eslicarbazepine may lower levels of ethinylestradiol, possibly interfering with the efficacy of certain hormonal contraceptives, and may increase levels of tolbutamide, a first generation sulfonylurea.Citation12 There are no kinetic interactions between eslicarbazepine and digoxin,Citation30 or metforminCitation31 when studied in healthy subjects taking both medications.
Table 1 Summary of potential pharmacokinetic interactions between eslicarbazepine and other medicationsCitation29
Efficacy studies
Eslicarbazepine has been shown to be effective in several animal models of epilepsy. In maximal electroshock seizures, eslicarbazepine was equal to carbamazepine, and superior to oxcarbazepine at 2 and 4 hours after the dose. At 8 hours after dose, all three drugs were equivalent.Citation12 Eslicarbazepine was equivalent to carbamazepine in prevention of seizures in the amygdala kindling model.Citation12 Furthermore, eslicarbazepine has been shown to be effective in the control of seizures induced by proconvulsant agents such as metrazole, bicuculline, 4-amino-pyridine,Citation12 latruncullin A,Citation32 and picrotoxin.Citation33
In humans, the clinical trials have focused on partial-onset seizures. In the first published study, 143 patients with ≥4 partial onset seizures/month, were recruited in a 12-week, multi-center, randomized, double-blind, placebo-controlled comparison of eslicarbazepine once daily (n = 50), twice daily (n = 46), or placebo (n = 47) added to their existing anticonvulsant regimen.Citation34 The dosage of eslicarbazepine was increased every 4 weeks from 400 mg/day to 800 mg/day, to 1200 mg/day. One hundred thirteen (78.5%) patients completed the study. Mean age was approximately 39, and mean body mass index (BMI) was approximately 25. Nearly half (40.6%) were male.Citation34
Partial seizures with secondary generalization were the most common (77.6%), followed by complex partial seizures (74.8%), and simple partial seizures (32.9%). Concomitant anticonvulsants consisted of: valproic acid (65.0%), topiramate (30.8%), lamotrigine (30.1%), clonazepam (15.4%), and phenytoin (7.7%). Patients receiving oxcarbazepine were excluded from the study. Phenytoin was over represented in the placebo group (17% of placebo treated patients) compared to single daily dose group (2%) or twice daily dose group (4%).Citation34
Response was defined as a minimum of 50% reduction in seizure frequency versus baseline. Single daily dosed eslicarbazepine was more effective than placebo (54% vs 28%, respectively; 90% CI = −∞, −14, P = 0.008). Twice daily dosing was not significantly better than placebo (41% vs 28%, respectively; 90% CI = −∞, −1, P = 0.12). The greatest reduction in seizure number occurred in subjects receiving a single dose of 1200 mg/day with a 60% reduction compared to a 30% reduction in those receiving placebo (P = 0.002).Citation34 Elimination of seizures occurred in 24% of those receiving eslicarbazepine compared to only 9% of those receiving placebo (P < 0.05).Citation34
In a similar, larger study, 402 patients were recruited in a 12-week, randomized, double-blind, placebo-controlled study of single daily dose of 400 mg (n = 100), 800 mg (n = 98), 1200 mg (n = 102), or placebo (n = 102).Citation28 Of the 402 patients, 330 (82%) completed the study. The mean age was 39 years (range 18–76 years). Half (51%) were women, and all were Caucasian. The mean BMI was 24.5. Most patients were receiving 2 concomitant anticonvulsants (n = 257, 63.9%), only 2 were receiving 3 anticonvulsants, and the remainder (n = 143, 35.6%) were taking only one concomitant anticonvulsant. The most common concomitant anticonvulsant was carbamazepine (58.5%), followed by lamotrigine (26.1%), valproic acid (25.6%), topiramate (13.7%), levetiracetam (8.5%), phenobarbital (8.2%), clonazepam (7.5%), and gabapentin (5.5%) (oxcarbazepine excluded).Citation28
The most common seizure type was complex partial seizures (69.7%). Nearly half of the patients had secondarily generalized seizures (46.3%) and simple partial seizures (44.0%). A small fraction had unclassified seizures (4.5%).Citation28 Duration of epilepsy was approximately 21 years, and the mean baseline seizure frequency was 2.9 seizures/week.
There was a dose related increase in the fraction of patients who responded (≤50% reduction in seizure frequency). Twenty percent of placebo-treated patients responded, compared to 23% of those receiving eslicarbazepine 400 mg/day (ns), 34% of 800 mg/day (P < 0.05), and 43% of 1200 mg/day (P < 0.001).Citation28 The likelihood of being free of seizures was only slightly higher with eslicarbazepine compared to placebo (8% of those receiving 1200 mg/day, P < 0.05, 4% of those receiving 800 mg/day, ns, 2% of those receiving 400 mg/day, ns, and 2 % of those receiving placebo).Citation28 The statistical methodology used in this study of the last observation carried forward generally underestimates the utility of the drug.
There is only one published study in a paediatric population.Citation35 Eleven young children (ages 2–7 years, mean age 4.1 ± SD 1.4 years), 8 older children (7–11 years, mean age 9.1 ± 1.6 years), and 10 adolescents (12–17 years, mean age 14.5 ± 1.6 years) were given single daily doses of eslicarbazepine in an open fashion. Forty-one percent were male. The majority were on 3 concomitant anticonvulsants (55.2%), nearly one-third were on 2 anticonvulsants (27.6%), and the rest were on 1 anticonvulsant (17.2%). The most common concomitant agents were lamotrigine (65.5%) and valproic acid (65.5%), followed by topiramate (48.3%), clonazepam (27.6%), phenobarbital (13.8%), and gabapentin (10.3%).Citation35
Eslicarbazepine doses were initiated at 5 mg/kg/day for 4 weeks, and increased to 15 mg/kg/day for an additional 4 weeks, and then to 30 mg/kg/day (or 1800 mg/day, whichever was less) for the last 4 weeks.Citation35 Young children and adolescents experienced a dose related reduction in seizure frequency. In young children there was a 28.2%, 24.8%, and 40.6% reduction with doses of 5, 15, and 30 mg/kg/day, respectively. In adolescents there was a 17.1%, 31.7%, and 43.1% reduction in seizure frequency with ascending doses. This pattern was not observed in older children (11.7%, 5.0%, and 12.2% reduction in seizure frequency at doses of 5, 15, and 30 mg/kg/day).Citation35
Safety and tolerability
Eslicarbazepine does not form the 10–11 epoxycarbamazepine metabolite that is formed when carbamazepine is prescribed. Consequently, it does not carry the same adverse consequences of that drug. However, when given as an add-on drug to other anticonvulsants in a placebo-controlled fashion, eslicarbazepine is associated with adverse events (AEs) in 41% to 61% of subjects (). In one study of 143 patients, the overall rate of AEs was not significantly different than placebo (ie, concomitant anticonvulsant) ().Citation34 In a study of 402 patients, AEs for the highest dose were twice as common as seen in placebo (ie, concomitant anticonvulsant) ().Citation28 The likelihood of adverse consequence is dose related with a higher rate of discontinuation for AE at higher doses (). The adverse effect profile is similar to that seen with both carbamazepine and oxcarbazepine and likely reflects a common mechanism of action. In all of the studies, there was only one death, a placebo-treated patient (ie, receiving concomitant anticonvulsants) who died from hypothermia. Electrocardiogram changes, specifically a mild prolongation of the PR interval, have been observed in patients taking eslicarbazepine.Citation29 In recommending approval of eslicarbazepine in Europe, the European Medicines Agency advised a contraindication to the administration of eslicarbazepine to patients with 2nd or 3rd degree heart block and caution with co-administration of any drugs known to increase the PR interval.Citation29
Table 2 Summary of percentage of adverse events across two placebo-controlled trialsCitation27,Citation33
There were no significant changes in blood cell parameters or serum sodium levels. Among the two placebo-controlled studies, there were 4 cases of abnormal laboratory findings. One case of hyponatremia (123 mmol/L) occurred in a patient receiving eslicarbazepine 800 mg once daily with concomitant carbamazepine and a baseline sodium of 133 mmol/L.Citation28 Additionally there was one case each of mild electrolyte imbalance, mild anemia, and a moderate elevation of creatine kinase.Citation34
The overall plasma levels of eslicarbazepine varied in a linear fashion with dose over the therapeutic dose range ().Citation28 None of the studies reported side effects as a function of concomitant anticonvulsant medication. This is an important point since AEDs with a similar mechanism (sodium channel blockade) might have an additive effect on observed AEs.
Table 3 Eslicarbazepine levels as a function of doseCitation27
Among 29 children receiving eslicarbazepine in addition to other anticonvulsants, 21 subjects reported 54 AEs.Citation35 The frequency of reported AEs varied with dose so that 11 occurred with low dose of 5 mg/kg/day, 15 occurred with the moderate dose of 15 mg/kg/day, and 28 were reported with the high dose of 30 mg/kg/day.Citation35 All AEs at lower doses were mild. At 30 mg/kg/day there were 9 moderate AEs and 2 severe AEs. Moderate AEs included somnolence (n = 3), vomiting (n = 2), diplopia (n = 2), dizziness (n = 1), and disequilibrium (n = 1). The severe cases were both related to worsening seizure disorder.Citation35
Conclusions
Eslicarbazepine acetate is a prodrug which is rapidly and almost completely metabolized to the active metabolite (S) licarbazepine. It is a member of the dibenzazepine family, which includes carbamazepine and oxcarbazepine. In animal studies, it has similar potency to the active metabolite of carbamazepine with fewer adverse effects and interactions, including cytochrome oxidases. Its preferential binding to VGSC in the inactivated state should result in selective inhibition of the most rapidly firing sodium channels, thereby limiting the excessive neuronal activity of seizures. It does not form the epoxide intermediate which is thought to be responsible for many of the adverse effects of carbamazepine. Its estimated half-life of 20–24 hours makes once-daily dosing a possibility. Dosage adjustments will be necessary in patients with moderate to severe renal impairment. Eslicarbazepine may affect levels of other medications including phenytoin, warfarin and estrogen-containing oral contraceptives, and certain enzyme-inducing AEDs may lower levels of eslicarbazepine. A contraindication to eslicarbazepine has been recommended in patients with 2nd or 3rd degree heart block, otherwise eslicarbazepine appears to be very safe. Efficacy has been demonstrated in at least three clinical trials of eslicarbazepine as adjunctive therapy for seizures, with a significant reduction in seizures as compared to placebo. Eslicarbazepine was well-tolerated in these trials, with the most common side effects being dizziness, nausea, vomiting, somnolence and diplopia. Hyponatremia, an idiosyncratic reaction occasionally seen with oxcarbazepine, was only reported in one study patient who was on both eslicarbazepine and carbamazepine.
The published studies investigated a relatively small number of patients with few comorbid medical problems. The effectiveness of eslicarbazepine in a typical clinical population still needs to be investigated. Initial use of eslicarbazepine will likely be as adjunctive therapy in adults with complex partial seizures who may be on a variety of other medications, including those affected by the CYP3A4 (including certain calcium channel blockers and zonisamide) and the CYP2C19 enzyme systems. Additionally, an examination of the side effect profile may be warranted on patients on other psychotropics (eg, antidepressants or antipsychotic medications) or cardiovascular agents that may accentuate the AE profile of eslicarbazepine. Finally, a study of endocrinologic effects of ESL may be warranted as changes in thyroid functionCitation36,Citation37 and vitamin D levelsCitation38,Citation39 have been observed in adults and children on oxcarbazepine and decreased bone mineral density has been observed in pediatric patients receiving oxcarbazepine.Citation39
In the past few years, as AEDs with less toxicity and fewer interactions have become available, emphasis on monotherapy in treatment resistant epilepsy has begun to give way to a sort of ‘rational polytherapy’ as means of controlling seizures,Citation40,Citation41 by using smaller doses of a combination of AEDs with different mechanisms of action to attain the goal of complete seizure control with fewer side-effects. As a group, the sodium channel blockers are among the most frequently prescribed medications in the management of epilepsy. Although a direct comparison has not been performed, eslicarbazepine may be better tolerated and more effective in controlling partial onset seizures than oxcarbazepine. The added benefit of once-daily dosing, which is not possible with carbamazepine or oxcarbazepine, may improve patient compliance with therapy and thereby further improve seizure control. Eslicarbazepine appears to be a safe and effective addition to the armamentarium of physicians managing patients with epilepsy.
Disclosures
The authors declare no conflicts of interest.
References
- HauserWAAnnegersJFKurlandLTPrevalence of epilepsy in Rochester, Minnesota: 1940–1980Epilepsia19913244294451868801
- HauserWAAnnegersJFKurlandLTIncidence of epilepsy and unprovoked seizures in Rochester, Minnesota: 1935–1984Epilepsia19933434534688504780
- ForsgrenLBeghiEOunASillanpaaMThe epidemiology of epilepsy in Europe – a systematic reviewEur J Neurology200512245253
- BirbeckGLHaysRDCuiXPVickreyBGSeizure Reduction and Quality of Life Improvements in People with EpilepsyEpilepsia200243553553812027916
- WirrellECEpilepsy-related InjuriesEpilepsia200647Suppl 1798617044832
- JostyICNarayananVDicksonWABurns in patients with epilepsy: changes in epidemiology and implications for burn treatment and preventionEpilepsia200041445345610756412
- HamerHMSpottkeAAletseeCDirect and indirect costs of refractory epilepsy in a tertiary epilepsy center in GermanyEpilepsia200647122165217217201718
- KraussGLAmpawLKrumholzAIndividual state driving restrictions for people with epilepsy in the USNeurology200157101780178511723263
- KwanPBrodieMJEarly identification of refractory epilepsyN Engl J Med2000342531431910660394
- FaughtEMonotherapy in adults and elderly personsNeurology200769Suppl 3S3S918071156
- AlmeidaLFalcãoAMaiaJMazurDGellertMSoares-da-SilvaPSingle-dose and steady-state pharmacokinetics of eslicarbazepine acetate (BIA 2-093) in healthy elderly and young subjectsJ Clin Pharmacol2005451062106616100301
- AlmeidaLSoares-da-SilvaPEslicarbazepine acetate (BIA 2-093)Neurotherapeutics20074889617199020
- VolosovAXiaodongSPeruccaEYagenBSintovABialerMEnantioselective pharmacokinetics of 10-hydroxycarbazepine after oral administration of oxcarbazepine to health Chinese subjectsClin Pharmacol Ther199966654755310613609
- BenesJParadaAFigueiredoAAAnticonvulsant and sodium channel-blocking properties of novel 10,11-dihydro-5H-dibenz[b,f]azepine-5-carboxamide derivativesJ Med Chem199942142582258710411478
- YamaokaKVogelSMSeyamaINa+ channel pharmacology and molecular mechanisms of gatingCurr Pharm Des200612442944216472137
- ParadaASoares-da-SilvaPThe novel anticonvulsant BIA 2-093 inhibits transmitter release during opening of voltage-gated sodium channels: a comparison with carbamazepine and oxcarbazepineNeurochem Int20024043544011821151
- BonifácioMJSheridanRDParadaACunhaRAPatmoreLSoares-da-SilvaPInteraction of the novel anticonvulsant, BIA 2-093, with voltage-gated sodium channels: comparison with carbamazepineEpilepsia200142560060811380566
- El-MallakhRSHuffMOMood stabilizers and ion regulationHarv Rev Psychiatry20019233211159930
- AraújoIMAmbrósioAFLealECNeurotoxicity induced by antiepileptic drugs in cultured hippocampal neurons: a comparative study between carbamazepine, oxcarbazepine, and two new putative antiepileptic drugs, BIA 2–024 and BIA 2-093Epilepsia200445121498150515571507
- Fontes-RibeiroCNunesTFalcäoAEslicarbazepine acetate (BIA 2-093): Relative bioavailability and bioequivalence of 50 mg/mL oral suspension and 200 mg and 800 mg tablet formulationsDrugs R D20056525326016128595
- MaiaJVas-da-SilvaMAlmeidaLEffect of food on the pharmacokinetic profile of eslicarbazepine acetate (BIA 2-093)Drugs R D20056420120615991880
- Fontes-RibeiroCMacedoTNunesTDosage form proportionality and food effect of the final tablet formulation of eslicarbazepine acetate: randomized, open-label, crossover, single-centre study in healthy volunteersDrugs R D20089644745418989993
- FalcãoAMaiaJAlmeidaLMazurDGellertMSoares-da-SilvaPEffect of gender on the pharmacokinetics of eslicarbazepine acetate (BIA 2-093), a new voltage-gated sodium channel blockerBiopharm Drug Dispos200728524925617443646
- AlmeidaLPotgieterJLMaiaJPotgieterMAMotaFSoares-da-SilvaPPharmacokinetics of eslicarbazepine acetate in patients with moderate hepatic impairmentEur J Clin Pharmacol200864326727318157705
- AlmeidaLSoares-da-SilvaPSafety, tolerability and pharmacolokinetic profile of BIA 2-093, a novel putative antiepileptic, in a rising multiple-dose study in young healthy humansJ Clin Pharmacol20044490691815286095
- MaiaJAlmeidaLFalcãoAEffect of renal impairment on the pharmacokinetics of eslicarbazepine acetateInt J Clin Pharmacol Ther200846311912018397682
- AlvesGFigueiredoICastel-BrancoMBiomed Chromatogr200721111127113417594694
- ElgerCHalászPMaiaJAlmeidaLSoares-da-SilvaPBIA-2093–301 Investigators Study GroupEfficacy and safety of eslicarbazepine acetate as adjunctive treatment in adults with refractory partial-onset seizures: A randomized, double blind, placebo-controlled, parallel-group phase III studyEpilepsia200950345446319243424
- European Medicines AgencyCHMP Assessment Report for Exalief: International Nonproprietary Name: eslicarbazepine acetateLondon1922009http://www.emea.europa.eu/humandocs/PDFs/EPAR/exalief/H-987-en6.pdf, accessed 13 October 2009.
- Vas da SilvaMCostaRSoaresEEffect of eslicarbazepine acetate on the pharmacokinetics of digoxin in healthy subjectsFundam Clin Pharmacol2009Epub ahead of print.
- RochaJFCaz-da-SilvaMAlmeidaLEffect of eslicarbazepine acetate on the pharmacokinetics of metformin in healthy subjectsInt J Clin Pharmacol Ther200947425526119356391
- Sierra-ParedesGOreiro-GarcíaTVázquez-IllanesMDSierra-MarcuňoGEffect of eslicarbazepine acetate (BIA 2–093) on latrunculin A-induced seizures and extracellular amino acid concentrations in the rat hippocampusEpilepsy Res2007771364217890056
- Sierra-ParedesGNúňez-RodriguezAVázquez-LópezAOreiro-GarcíaTSierra-MarcuňoGAnticonvulsant effect of eslicarbazepine acetate (BIA 2-093) on seizures induced by microperfusion of picrotoxin in the hippocampus of freely moving ratsEpilepsy Res2006722–314014616920333
- ElgerCBialerMCramerJAMaiaJAlmeidaLSoares-da-SilvaPEslicarbazepine acetate: A double-blind, add-on, placebo-controlled, exploratory trial in adult patients with partial-onset seizuresEpilepsia200748349750417319919
- AlmeidaLMinciuINunesTPharmacokinetics, efficacy, and tolerability of eslicarbazepine acetate in children and adolescents with epilepsyJ Clin Pharmacol200848896697718508949
- IsojarviJITurkkaJPakarinenAJKotilaMRattyaJMyllylaVVThyroid function in men taking carbamazepine, oxcarbazepine, or valproate for epilepsyEpilepsia200142793093411488894
- HirfanogluTSerdarogluACamurdanOThyroid function and volume in epileptic children using carbamazepine, oxcarbazepine and valproatePediatrics International200749682282618045279
- MintzerSBoppanaPToguriJDeSantisAVitamin D levels and bone turnover in epilepsy patients taking carbamazepine or oxcarbazepineEpilepsia200647351051516529614
- CansuAYesilkayaESerdaroğluAEvaluation of bone turnover in epileptic children using oxcarbazepinePediatr Neurol20083926627118805365
- DeckersCCzuczwarSHeksterYSelection of antiepileptic drug polytherapy based on mechanisms of action: the evidence reviewedEpilepsia200041111364137411077449
- LeppikIEMonotherapy and polypharmacyNeurology20005511 Suppl 3S25S2911147565