Abstract
Medication prescribed but not consumed represents a huge loss in drug and prescribing costs and an enormous waste of expensive medical time. In this article we discuss what is known about compliance and adherence, explore the concept of concordance and demonstrate its fundamental difference from both. Not all patients are ready or suitable for shared decision making in management of their condition, some still preferring a doctor-led decision but an increasing number want a partnership approach. By opening up and rebalancing the discussion about medication, we can expect a consultation which is more satisfying for both parties and flowing from this, more effective, focused prescribing of medication which is more likely to be adhered to by the patient. We examine the extent to which doctor and patient behaviors are currently compatible with this change of concept and practice, look at available consultation models which might be useful to the reflective practitioner and consider what actions on the part of the doctor and the healthcare system could promote medicine prescription and utilization in line with this new approach based on partnership.
Background
In the United Kingdom, it is estimated that about £100M each year, enough to build a sizeable hospital, is wasted on medication dispensed but returned to pharmacies (CitationNational Audit Office 2007). This is probably just the tip of the iceberg of medicines not consumed by the patients for whom they were prescribed (CitationMetcalfe 2005). Extensive reviews of the literature reveal that in developed countries adherence to therapies averages 50% (CitationWorld Health Organisation 2003; CitationCarter et al 2005). Approximately half of this non-adherence is intentional, an active “resistance” (CitationPound et al 2005) whilst the remainder occurs because patients are either unaware that they are not taking medication as prescribed or the regime is just too complex (CitationLey 1997). The consequences are waste, morbidity and hospital admissions (CitationWHO 2003).
The Evidence Based Clinical Outcomes movement now has a large database of information on effectiveness of therapies but even when good evidence is available, translation from theory to practice can be difficult and there are few rigorous trials of well-specified interventions to inform practice (CitationGriffin et al 2004). Clinical experience needs to be supplemented by outcomes research (CitationTannenbaum 1993) but efficacy in practice is less dependent on improvements in specific medical treatments than on adherence which is affected by patient, practitioner and healthcare system factors (CitationHaynes, Devereaux et al 2002; CitationHaynes, McDonald et al 2002). Hence it is suggested that a model for clinical decision making should use evidence but acknowledge the importance of patient factors and clinical expertise (CitationHaynes 2004).
Patient involvement in decision making is a specific example of an attitudinal shift in society towards greater individual autonomy and choice (CitationDepartment of Health 2001, Citation2002; CitationWanless 2002). With a shift of burden from acute to chronic disease in the population, the active and informed involvement of patients to prevent or manage their illnesses is desirable. Powerful, complex and intrusive therapies demand greater understanding and active participation by the patient in decisions about therapy in order to promote greater efficacy and patient safety (CitationDonaldson 2003; CitationWHO 2003; CitationNational Patient Safety Agency 2006). When appropriately provided with evidence, patients usually make rational choices that are often more conservative and involve less risk than their doctors would choose (CitationO’Connor et al 1999).
In this article we discuss what is known about compliance and adherence, explore the concept of concordance and demonstrate its fundamental difference from both compliance and adherence. We consider whether the behaviors of provider and patient are currently compatible with this change of concept and consider what actions on the part of individual practitioners and the healthcare systems in which they work could help to optimize medicine taking.
Compliance and adherence: Definitions and literature review
Compliance is defined as: “the extent to which the patient follows the health professionals’ advice and takes the treatment”. This view of a rather passive, obedient patient, whilst perhaps an approach expected and preferred by some patients is increasingly an obsolete model of care. Its practitioners have rarely recognized its inefficiency, though this is well recorded in even quite old literature (CitationLey 1982). Patients may be deferential in the presence of doctors whilst holding many reservations, which they fail to voice (CitationTuckett 1985). They actively make decisions not to take prescribed medication and fail to confide in their doctors (CitationStimson 1974; CitationBenson and Britten 2002; CitationPound et al 2005). They also use other self administered or complementary therapies which they do not declare (CitationElwyn 2003).
Whilst the term compliance remains in the literature it has been superseded more recently by the term adherence. Patient adherence is defined as: “… the extent to which a person’s behavior – taking medication, following a diet, and/or executing lifestyle changes, corresponds with agreed recommendations from a health-care provider” (CitationWHO 2003).
Detailed reviews reveal the complexity of adherence; the result of an interplay of a range of factors including patient views and attributes, illness characteristics, social contexts, access and service issues (CitationHaynes et al 1996; CitationHaynes, Devereaux et al 2002; CitationWHO 2003; CitationCox et al 2004). A recent meta-analysis by CitationSimpson et al (2006) showed that good adherence was associated with reduced mortality, though the reasons may not be as simple as at first appears since a similar benefit was also seen for adherence to placebo. It may be that good adherence behavior is a marker for overall healthy behavior but adherence also has its risks for good adherers experienced some increase in mortality from unwanted drug effects. This supports the point made by Pound et al (2006) who suggest the predominant need to make medicines themselves safer.
Failure to adhere is, not surprisingly, a particular problem in the management of chronic illness especially when patients do not feel ill (CitationCarter et al 2005). Asthma, diabetes and hypertension treatments seem to incur especially high levels of non-adherence and it is common for patients to alter or abandon therapy without telling their doctor (CitationSackett et al 1978; CitationLey 1982; CitationWHO 2003).
Patients with depression, anxiety or cognitive impairment, the elderly, those on multiple medications and with complex regimens, those on preventive medication and with chronic illnesses have lower adherence rates (CitationDiMatteo et al 2000; CitationZiegelstein et al 2000; Haynes et al 2000b; CitationClaxton et al 2001; CitationHeneghan et al 2006). However, non-adherence still occurs in other, more favorable settings and doctors themselves are similarly sometimes non-adherent (CitationLey 1981, Citation1982).
Evidence that interventions to improve adherence are effective is sparse. CitationCox et al (2004) in their comprehensive review suggest that changes to organizational practices can be beneficial. For example, increasing the frequency of visits to a nurse practitioner for medication review enhances attendance and subsequent discussions with a doctor. Advertising campaigns aimed at promoting the role of pharmacists have not been shown to increase adherence although they do positively influence pharmacists’ communication with patients (CitationAiraksinen et al 1998). Asking patients to write down questions before they see the pharmacist did result in more questions being asked but did not have any additional impact on adherence (CitationBarnett et al 2000).
Extensions in prescribing roles for nurses and supplementary prescribing by pharmacists mean that optimal medicines management is increasingly a team responsibility (CitationDepartment of Health 2002). Unfortunately, CitationHaynes et al (1996, Citation2002) show that even highly developed, complex, labor intensive and patient-focused interventions, whilst effective in the short term had no effect on adherence over a longer period. Use of patient groups to inform and support, expert patient programmes, monitoring by administrative staff and improved repeat prescribing systems are examples of mechanisms to support medicines management and adherence (CitationBodenheimer et al 2002; CitationDonaldson 2003). A “whole systems approach” to improving medicines management is intuitively sensible and supported by some evidence.
The strongest effects on treatment outcome would seem to derive from active involvement of individuals, the promotion of self care and social support (CitationCarter et al 2005) and thus, whilst recognizing the importance of system factors and the clinical team, we concentrate in this review on the interaction of the individual patient with the prescribing practitioner and the opportunity that this provides to enhance self care and active involvement.
Concordance: Redefining the issue
The term “concordance” relates to a process of the consultation in which prescribing is based on partnership. A subset of shared decision making, the concept was introduced by the Medicines Partnership Group established in 1996 by the Department of Health in conjunction with the Royal Pharmaceutical Society of Great Britain. It is defined as: “agreement between the patient and healthcare professional, reached after negotiation that respects the beliefs and wishes of the patient in determining whether, when and how their medicine is taken, and (in which) the primacy of the patient’s decision (is recognized)” (CitationMarinker et al 1997).
Concordance describes an agreement drawing upon the experiences of both provider and patient. Some authors warn against the concept being subverted into a subtle form of coercion, providing patients with more information but in such a way as to indirectly influence outcome (CitationHeath 2003; CitationPollock 2005).The proponents of concordance are, however, quite clear about the value of the concept when properly applied (CitationRPSGB 1997). There is therefore no such thing as patient concordance. The consultation is concordant when it involves two-way communication and informed, shared decision-making.
The degree to which patients want to be involved in decision-making with their practitioner is, in practice, variable. In some cases the patient with the aid of the practitioner reaches a decision that both parties think appropriate. The patient is better informed, more likely to be committed to the treatment regime and thus to adhere to a decision she has actively made for herself (CitationStewart et al 1999). In practice the patient often asks the practitioner’s opinion and defers to that. The challenge here is for the professional to delve beneath the surface of this deference to ensure that important issues which might affect adherence are not being ignored. A third possibility is that after considering the options, the patient reaches a decision which the practitioner, from a biomedical viewpoint, would not recommend. As long as the doctor believes the patient has understood the issues and there are no ethical concerns, then the patient’s decision is supported. At the extreme, the doctor may be faced with dissociating him or herself from the patient’s decision, though this is in practice likely to be a very rare event.
A major advantage to the concordance approach is that the doctor will have elicited the patient’s views and the decisions will be overt. The patient also knows his or her views are respected and any subsequent difficulties the patient has in following the treatment can be discussed. The patient is not, subsequently, likely to be in an uncomfortable position of either telling the doctor that he or she has not followed the advice or, alternatively of lying. To be fully committed to the concept of concordance means to see one’s responsibility in terms of providing information and opinion and in respecting patient autonomy in decision-making, rather than in deciding for them. In reality the patient always decides but without open communication they frequently do so without telling their doctor.
The need for expert knowledge and opinion is still important. CitationQuill and Brody (1996) advocate an “enhanced autonomy” model in which the patient’s best interests are served by actively exchanging ideas, openly discussing and negotiating differences and sharing power and influence. Even the most independent patient wants to hear their doctor’s opinion and some people prefer a more directive approach (CitationCox et al 2004; CitationSwenson et al 2006). The practitioner needs the flexibility and the skills to explore which approach the patient wants.
The practitioner’s most frequent role now becomes one of helping patients with decisions they make for themselves and supporting them in seeing these through. It requires a particular attitude accompanied by the necessary communication skills to put it into practice.
Concordance thus represents a radical model of care which challenges much of the medical training that many practitioners have undergone. The concept cannot be simply “bolted on” to traditional behavior. In order to understand what is required, we need to examine the processes of the consultation in more detail.
What usually happens in consultations?
Doctors regularly provide information but in only about 2% of consultations do they check what patients have understood or thought of these explanations. (CitationTuckett et al 1985; CitationLevinson 1997; CitationButler et al 1998; CitationKettunen et al 2001).
Patients are generally passive in consultations. Younger patients and white males are more likely to participate in discussions about their medication and younger doctors also seem to encourage this (CitationCox et al 2004). Many patients have their own ideas about what is wrong and what may have caused it but they do not always articulate them (CitationCockburn and Pit 1997).
Observations of consultations show that doctors rarely explore patients’ ideas, concerns and expectations or their understanding and intentions about management (CitationTuckett 1985; CitationLevinson 1997). Studies in which consultations were recorded showed that doctors think they discuss management issues more often than is actually the case and interestingly, patients also tended to overestimate how much they were told and involved in the consultation (CitationCox et al 2004).
Side effects are a concern that patients would like to be able to discuss with doctors (CitationCoulter 2005). Doctors themselves more commonly discuss benefits and the mechanics of taking medication (CitationCox et al 2004). When patients do raise the subject of side effects, doctors are more likely to either evade the issue or change the medication than enter into a discussion to help patients compare possible unwanted effects with anticipated benefits. CitationLevinson (1997) in her study found that only 10% consultations included mention of any adverse effects.
Doctors can draw unwarranted inferences about patient expectations, sometimes wrongly assuming patients want a prescription. CitationLittle et al (2004) found that in situations where the doctor thought there was little or no medical need, perceived patient pressure was a stronger predictor of prescribing than the patient’s actual preference. This may simply reflect the doctor’s own need to do something which is then projected as a patient expectation. The pressure to shorten visits and avoid exploring concerns in depth may also result in over-prescribing (CitationEpstein 2006).
Why aren’t patients more forthcoming?
Some 30-years ago CitationByrne and Long (1976) first described how doctors control the consultation process and CitationStrong (1979) described ritual aspects of interaction between doctors and parents in a pediatric setting. Patients have to manage both their illness and also their interaction with healthcare services. Questioning can be a risky business. The questioner gets more information at the risk of creating tension in the consultation if the practitioner is not comfortable or regards this as interrogation (CitationTuckett 1985; CitationMurray et al 2003). Active questioning by a patient sometimes reflects dissatisfaction linked to non-adherence, but admitting non-adherence risks provoking anger in the provider (CitationCox et al 2004; CitationCarter et al 2005). People frequently act to preserve their dignity and self esteem in the eyes of others by ‘saving face’ (CitationGoffman 1972; CitationLazare 1987). Thus maintaining a relationship is of concern to both patients and doctors (CitationPollock 2005).
Forms of politeness generally prevail to deal with asymmetric power relations (CitationBrown and Levinson 1978). This applies to patient interactions with all health-care workers as a result of both the professional role and the organizations within which they work (CitationKettunen et al 2001; CitationLatter and Courtenay 2004). Professional status is reinforced by patient deference and by avoiding open disagreement and conflict. If this results in patient agendas not being explored, the result may be unwanted prescriptions with potential for poor adherence and wasted resources (CitationButler et al 1998; CitationBarry et al 2000).
CitationDowell and colleagues (2002) applying a strategy based on concordance to consultations with patients who had a history of adherence problems found what they described as a ‘zone of discomfort’ marking a transition between a diagnostic and therapeutic encounter. This occurred when differences between patient and doctor views were revealed. They attributed the improved clinical control and medicines taking that subsequently occurred to the process of addressing the issue of acceptance of the illness. The ability to discuss feelings about the illness was dependent on an improvement in the doctor-patient relationship.
Patients recall about 60% of what they have been told and what they recall depends on salience and time of presentation, the first thing said being most likely to be remembered (CitationLey 1997). Interestingly, prior knowledge and consistency with their own views make recall and understanding more likely, even when the provider’s explanations are not very clear (Punamaki and Kokki 1995; CitationLey 1997). Further evidence of the importance of belief comes from CitationBritten et al (2000) who found that patients are much less likely to take medication if their own beliefs are in conflict with those of healthcare professionals and their concerns are not addressed.
Whilst healthcare professionals may feel frustrated by the apparent irrationality of patients, when viewed from a patient’s perspective, their reservations make absolute sense. For the most part they have good reasons for not taking their drugs: fear of dependency, concern about side effects and hopes that their condition has improved (CitationPound et al 2005). They therefore experiment by varying dosages and having drug-free intervals (CitationDonovan and Blake 1992).
Positive behaviors
Better adherence is obtained by practitioners who provide information, engage in “positive talk” and specifically enquire about adherence (CitationHall et al 1988). Warmth and empathy, self-disclosure, listening attentively to patients’ views and providing emotional support result in greater satisfaction, improved adherence and lower levels of litigation (CitationStewart 1996; CitationLevinson 1997; CitationAmbady et al 2002; CitationWhitcher-Alagna 2002). Patients who view themselves as active partners in the process have better adherence and health outcomes CitationSchulman (1979).
Creating the right atmosphere for allowing such discussions is important but not always easy. Patients are commonly anxious when they are ill and anxiety adversely affects cognition. Too much information too quickly may be overwhelming whilst evaluating different options can be equally stressful. Uncertainty provokes anxiety especially for people with a need for high levels of control (CitationKrupat et al 2000; CitationEpstein 2006).
It can be seen that the consultation process is complex and maximizing its therapeutic potential requires a relationship built on respect with considerable communication skills, careful pacing and a flexible approach to the condition, the context and the patient (CitationDiem 1997; CitationKrupat 2000; CitationEpstein 2006).
In summary the research reviewing the extent to which some elements of concordance occur in consultations found few examples of good practice. Crucially, doctors rarely ask patients for their own experiences or views about medication, a central need for a concordant discussion. Changes to the dynamic of the consultation have tended to be superficial and not addressed the patient as a real partner in the process. Awareness, commitment and skills are needed to transform the interaction to a genuine partnership. We would assert that most, if not all, patients would benefit from this approach.
Do doctors and patients want shared decision making?
Doctors appear supportive of shared decision making but are less confident that this is achieved in practice (CitationCox et al 2004; CitationEdwards and Elwyn 2004). Clinical autonomy is extremely important and highly valued by doctors. There is concern that a loss of traditional professionalism, greater regulation and public accountability, consumerism and a more confident, questioning and informed public will adversely affect the doctor-patient relationship (CitationMurray et al 2003; Pollock 2006, ch 5). Inevitably there is variation, and other doctors actively welcome the more informed and questioning patient (CitationMcMullan 2006).
Patients also show huge variation in their desire for level of involvement and shared decision making. A national survey in the USA found that whilst nearly everyone wants to be offered choices and asked their opinion, about half prefer to leave decisions ultimately to their doctor (CitationLevinson et al 2005). The Picker Institute surveyed eight European countries and found differences across countries but an average of 50% of people said they wanted shared decision making (CitationCoulter and Magee 2003). A shared decision-making approach inflexibly imposed by practitioners may be perceived as oppressive by some patients (CitationGambrill 1999; Pollock 2006). Whilst the majority of patients prefer patient-centered communication some say they actually dislike it and want more directive styles with clear and strong advice (CitationSwenson et al 2006). Even this group seems to gain satisfaction from an approach more patient-centered than that which they overtly espouse (CitationKrupat et al 2000).
Despite changes in society and increasing access to the Internet, patients still regard doctors as their primary source of information. They prefer to discuss medications with their usual doctor, suggesting that continuity of care and a successful relationship with their doctor remain important (CitationCox 2004). The quality of the relationship rather than just mechanical exchange of information alone is the key determinant for patients and patient-centeredness is preferred (CitationKrupat et al 2000; CitationCox et al 2004; CitationEpstein 2006; CitationLongo et al 2006). They want reassurance supported by clear information and tailored practical advice, to feel that their problems have been acknowledged and understood and that they are valued as a person rather than as a case (CitationRoter 1998; CitationCox et al 2004).
There continues to be a gap between the rhetoric of patient-centered medicine and its practice (CitationCoulter 1999, Citation2002b). Doctors face the challenge of creating effective dialogues with patients in a changing culture where individuals, government, media, the pharmaceutical industry and professional organizations produce conflicting expectations (CitationElwyn 2004). Despite professionals’ concerns, the evidence suggests that patients continue to want and need good therapeutic relationships with their doctors, albeit, for many, in a slightly different form (CitationCoulter 2005).
Barriers to a change in consulting behavior
Time
Intuitively, it would seem inevitable that consultations will be longer if doctors are actively exploring patients’ views about medication, helping them to weigh up risks and benefits in order to reach an informed decision (CitationEdwards and Elwyn 2004). Health service targets and a responsibility to manage time for the benefit of all patients constitute pressures within consultations. Health Services therefore need to be aware that encouragement of patient participation may require more investment of time at least initially (CitationEdwards et al 2004; CitationMetcalfe 2005). The potential benefits are however substantial and the extra time requirement is probably less than appears at first sight. Most patients are sensitive to the time pressures that doctors experience and restrain their desire to talk about their concerns (CitationPollock and Grime 2002). Whilst patient-centered consultations take more time initially, they are only marginally longer than disease-centered consultations as practitioners become more proficient in this approach (CitationLevinson 2000). CitationLacroix (1992) found that the consequence of doctors reflecting back the patient’s complaint and concerns and checking the patient’s understanding of medication instructions was to increase consultation time by an average of 37 seconds. Becoming more skilled can actually improve time control (CitationRoter et al 1995; Belle Brown 2003) and efficiency (CitationLevinson et al 2000).
Skills
Explaining risk is a complicated process and may partly explain why practitioners appear to avoid discussing side effects. CitationMisselbrook and Armstrong (2001) found that the decision to take an anti-hypertensive drug was affected by the way in which the health care professional explained risk. Practitioners may be concerned this will deter patients, reduce trust and hence chances of benefit from the drug. Some decision aids have been developed which show positive benefits for patients (CitationO’Connor et al 1999; CitationOttawa 2006) but there appears to be little guidance for physicians on using them with patients (CitationEpstein 2006).
Medical training
Scientific evidence, the dramatic success of its application to the art of medicine and the previously unquestioned belief that doctors expertise is paramount in decisions about management have been central to the training of doctors. Patients want knowledgeable and skilled doctors and at times, particularly in acute situations, doctors have to make unilateral decisions in the patient’s best interests. But often in healthcare there are a number of options. The emphasis on the biomedical model has not prepared doctors for a collaborative patient-centered approach to care that explicitly takes into account patients’ views.
A willingness to countenance the value and importance of the patient’s perspective in management decisions is however vital to progress, a fact emphasized by the enquiry into children’s heart surgery at CitationBristol Royal Infirmary (2001) reviewed by CitationCoulter (2002a).
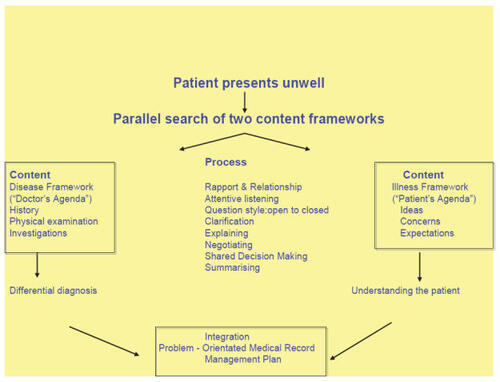
Conventionally doctors have focused on their agenda of identification and treatment of disease. Patients present with symptoms of illness and many do not have definable disease. Identification and incorporation of both agendas in a management plan provides satisfaction to both parties. CitationLevenstein’s (1989) model shown in diagrammatic form in provides a useful view of the relationships between disease and illness, doctor and patient agendas and the skills needed to reach a management plan. The physician is, at best, a bridge between the corpus of scientific knowledge, including what remains unknown, and the patient’s life. In the past 30-years, analysis of the consultation process itself and its social context has given us the tools to strengthen the bridge between what medicine can offer and what patients want but incorporation into actual practice has been patchy.
Figure 1 The patient-centered clinical interview (adapted from CitationLevenstein et al 1989).
Models for communication in shared decision making
Except when they are in hospital, it is patients who have to manage their medication. The paradox is that patients remain largely passive in consultations whilst needing to be active in their own medicines management and behavior changes. Despite a considerable body of knowledge about negotiation and helping behavior change, professional training has not drawn upon it. The usual approach in consultations remains giving advice with the expectation that professional expertise will lead to patient compliance. Health professionals are frustratingly aware that this doesn’t work but continue to struggle with it for want of a better strategy.
People are more committed to ideas if they hear themselves saying them and believe they can carry them out. (CitationBandura 1977; CitationAjzen and Fishbein 1980; CitationLeventhal 1998). Asking patients views, listening and helping them think the problem through and make a decision is more effective than telling people what to do. CitationMiller and Rollnick (2002) describe how motivation to adhere to treatment is influenced by the person’s assessment of cost versus benefit of following the regime and importantly by the person’s confidence in their ability to do so (self-efficacy). Adherence will be low if either are low. Rollnick provides an approach vividly encapsulated by the phrase “dancing not wrestling”; working with rather than struggling against the patient. Respecting the person’s right to their own choice is the flexible basis on which to create collaborative interactions (CitationRollnick et al 2000). This concept is illustrated in . It entails establishing rapport, checking what the patient wants to talk about and what the practitioner thinks is important and agreeing priorities.
Figure 2 Key tasks in consultations about behavior change. Reprinted from Health Behavior Change: A Guide for Practitioners. Rollnick S, Mason P and Butler C, p 12, London, Churchill Livingstone. Copyright (2000), with permission from Elsevier.
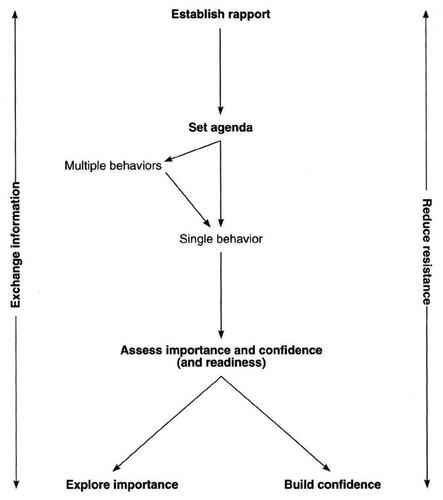
The patient decides how important the behavior is and how confident they are in their ability to make the change.
There are two tasks for the practitioner; exchanging information and helping the patient to reduce barriers (resistance) to making a change. Listening skills are important in information exchange so that both parties understand each other’s viewpoint. Reluctance or defensiveness either verbally or non-verbally indicates the patient is uncomfortable with the approach or information. It can be easily appreciated that this demands an increased level of sensitivity and understanding of the dynamics of the consultation. This approach to discussions on behavior change is equally applicable to shared decision-making about medication.
CitationTowle and Godolphin (1999) in defining a set of competences for both health professionals and patients stress the need to ascertain the level of information and involvement in decision making that a patient might want. Patients may sometimes take on more or less involvement depending on their circumstances, the context and the condition (CitationElwyn et al 2003; CitationMakoul and Clayman 2006). Moreover, decisions are not always made when the problem is first discussed and follow up is essential to come to a decision and to review ones that have been made. Relapse is common (CitationProchaska 1997) so open discussions which acknowledge the possibility that the patient may want to stop or change medication are essential.
The CitationOttawa Personal Decision Guide (2006) is a self assessment form designed to help individuals work through difficult decisions in a systematic way. Whilst not appropriate for everyone to complete independently, the analytical structure could also be useful to allow professionals to work through choices with their patients.
Implications for changes in practitioner behavior
The barriers to change of consulting behavior should not to be underestimated. The practitioner needs to recognize its importance and to feel it is achievable. The benefits include a greater understanding of management of patients’ conditions, better relationships with and hence more satisfied patients and, potentially at least, better health outcomes (CitationElwyn et al 2003).
CitationBritten (2004) cites five pre-requisites for concordance in consultations which include:
A willingness to share power and a commitment to giving appropriate weight to patient values and goals
Open discussion of the options with explicit enquiry as to patients views without making assumptions
Adequate sharing of information including uncertainties to arrive at a decision
Listening as much as talking
Time.
Specific problems in relation to medication discussions have been identified (CitationCox et al 2004) and we make some suggestions for how these could be addressed in . Steps for achieving concordant consultations are outlined in .
Table 1 Areas for improvement in medicines discussions and suggested actions
Table 2 Outline of steps to take for achieving concordance in the consultation
Training
A number of intervention studies have shown how training improves healthcare professionals’ shared decision making skills (CitationAufseesser-Stein et al 1992; CitationLacroix et al 1992; CitationClark et al 1998; CitationEdwards et al 2004; CitationLongo et al 2006). However to date the rigor of such studies has been poor and their translation into practice limited or questionable (CitationDavis et al 2003; CitationEdwards and Elwyn 2004; CitationGriffin et al 2004; CitationFellowes et al 2007).
Doctors communication skills do however change following intensive training and these changes persist into clinical practice (CitationFallowfield and Jenkins 2003).
Whilst undergraduate curricula have for some time included communication skill training (CitationHargie et al 1998), post-graduate competences and training needs, though well established in Primary Care are only just beginning to be addressed in hospitals. The junior doctor emerging into busy hospital practice easily forgets all he has learnt in the calm environment of medical school and will usually adopt a senior colleague, who may or may not be appropriate, as a role model. This tendency also leads to an inflexible consultation style which does not acknowledge that different patients need different approaches. Practice with feedback and support in clinical settings are essential parts of the training process (CitationMaguire and Pitceathly 2002; CitationHeaven et al 2006). It is difficult to incorporate this into the busy professional lives of both trainees and trainers and whilst there are many skilled communicators amongst the latter, the ability to analyze a consultation and thus aid learning is much less widely available.
Conclusion
In this article we have attempted to reframe the issue from one of adherence to a treatment defined by the doctor towards optimizing medicines management with patient involvement. We have described the communication process which is central to concordance and outlined the skills which health care professionals need to use if they wish to embrace the process. Concordance relies on open discussions about the condition and treatment options. Making decisions based upon shared information and respect for patient belief results in “compliance” and “adherence” becoming almost an irrelevance since the primary decision is made by the patient. The result is likely to be patients committed to actions they have chosen and thus optimized medicines management. It may also result in fewer prescriptions being issued.
The strategy is, therefore, one of establishing a relationship which promotes open discussion using communication skills effectively from the outset. Four areas need to be explored with patients:
Their understanding of the diagnosis and options for treatment.
Their beliefs and concerns about the condition and the options for treatment.
The challenges they anticipate in trying to adhere to a particular therapeutic regime.
Practical ways of helping them with these difficulties
Optimizing medicines management is not a tag-on at the end of a consultation but is dependant upon and part of the whole consultation. We hope to have encouraged the reader to see the value and satisfaction to be obtained from seeking a partnership with patients utilizing the approaches laid out in the last part of this paper. This change in clinical style cannot be achieved overnight or simply by reading a book. We would encourage the interested reader to consider one of the many courses on medical communication skills which are now available. On these, the doctor can try out new techniques in safety with the help of actors, role-play and group discussion to build their proficiency in communication skills for concordant consultations aimed at optimizing medicines management. Health-care systems would, in our opinion benefit from promotion of communication skills education and training particularly in the early post-graduate years of hospital practice.
References
- AiraksinenMAhonenREnlundHThe “Questions to Ask About Your Medicines” campaign – an evaluation of pharmacists and the public’s responseMedical Care19983642279520965
- AjzenIFishbeinMUnderstanding attitudes and predicting social behavior1980Englewood Cliffs, NYPrentice Hall
- AmbadyNLaplanteDNguyenTSurgeons’ tone of voice: a clue to malpractice historySurgery20021325912110787
- Aufseesser-SteinMRuttimannSLacroixASwiss educational experience with a prescription dialogue in ambulatory medicineSchweizerische Rundschau fur Medizin Praxis19928114261535945
- BanduraASocial learning theory1977Englewood Cliffs, NJPrentice Hall
- BarnettCWNykampDEllingtonAMPatient-guided counseling in the community pharmacy settingJ Am Pharm Assoc20004076572
- BarryCBradleyCBrittenNPatients’ unvoiced agendas in general practice consultationsBMJ200032012465010797036
- BensonJBrittenNPatients’ decisions about whether or not to take antihypertensive drugs: qualitative studyBMJ2002325873712386041
- BodenheimerTLorigKHolmanHPatient self-management of chronic disease in primary careJAMA200228824697512435261
- Bristol Royal Infirmary Enquiry. London Stationery Office 2001
- BrittenNStevensonFABarryCAMisunderstandings in prescribing decisions in general practice: qualitative studyBMJ2000320484810678863
- BrittenNPatients’ expectations of consultationsBMJ20043284161714976072
- BrownJBJonesRBrittenNCulpepperLTime and the consultationOxford textbook of primary medical care2003Oxford University Press
- BrownPLevinsonSGoodyENUniversals in language usage: politeness phenomenaQuestions and politeness: strategies in social interaction1978CambridgeCambridge University Press56289
- ButlerCCRollnickSPillRUnderstanding the culture of prescribing: qualitative study of general practitioners’ and patients’ perceptions of antibiotics for sore throatsBMJ1998317637129727992
- ByrnePSLongBELDoctors talking to patients1976LondonHMSO
- CarterSTaylorDLevensonRA question of choice – compliance in medicine taking. From compliance to concordance20053LondonMedicines Partnership http://www.medicines-partnership.org/research-evidence/major-reviews/a-question-of-choice
- ChewningBThe healthy adherer and the placebo effectBMJ2006333181916809709
- ClarkNMGongMSchorkAImpact of education for physicians on patient outcomesPediatrics199810183169565410
- ClaxtonAJCramerJPierceCA systematic review of the association between dose regimes and medication complianceClinical Therapeutics200123129631011558866
- CockburnJPitSPrescribing behavior in clinical practice: patients’ expectations and doctors’ perception of patient expectations – a questionnaire studyBMJ199731552039329308
- CoulterAPaternalism or partnership?BMJ19993197192010487980
- CoulterAAfter Bristol; putting patients at the centreBMJ2002a3246485111895824
- CoulterAThe Autonomous Patient. Ending paternalism in medical care2002bLondonThe Stationery Office
- CoulterAWhat do patients and the public want from primary careBMJ20053311199200116293845
- CoulterAMageeHThe European patient of the future2003MaidenheadOpen University Press
- CoxKStevensonFBrittenNA systematic review of communication between patients and health care professionals about medicine taking and prescribing. London GKT Concordance Unit Kings College2004 Published by Medicines Partnership http://www.medicines-partnership.org/research-evidence
- DavisREDolanGThomasSExploring doctor and patient views about risk communication and shared decision-making in the consultationHealth Expect2003319820712940793
- Department of HealthThe Expert Patient: a new approach to chronic disease management in the 21st century2001LondonDepartment of Health
- Department of HealthLearning from Bristol: the Department of Health response to the report of the public inquiry into children’s heart surgery at the Bristol Royal Infirmary 1984–19952002LondonDepartment of Health
- DiemSHow and when should physicians discuss clinical decisions with patients?J Gen Intern Med19971239789192259
- DiMatteoMRLepperHSCroghanTWDepression is a risk factor for noncompliance with medical treatment: meta-analysis of the effects of anxiety and depression on patient adherenceArch Intern Med20001602101710904452
- DonaldsonLExpert patients usher in a new era of opportunity for the NHSBMJ200332627980
- DonovanJLBlakeDRPatient non-compliance: Deviance or reasoned decision making?Soc Sci Med199234507131604357
- DowellJJonesASnaddenDExploring medication use to seek concordance with ‘non-adherent’ patients: a qualitative studyBr J Gen Pract200252243211791812
- EdwardsAElwynGInvolving patients in decision making and communication risk: a longitudinal evaluation of doctors’ attitudes and confidence during a randomized trialJ Eval Clin Pract20043431715304143
- EdwardsAElwynGHoodKPatient-based outcome results from a cluster randomized trial of shared decision making skill development and use of risk communication aids in practiceFam Pract2004213475415249521
- ElwynGArriving at the postmodern medical consultationEur J Gen Pract20041093715534573
- ElwynGEdwardsABrittenNDoing Prescribing: how doctors can be more effectiveBMJ2003327864714551110
- EpsteinRMMaking communication research matter: What do patients notice, what do patients want, and what do patients need?Patient Educ Couns200660272816426796
- FallowfieldLJenkinsVFarewellVEnduring impact of communication skills training: results of a 12-month follow-upBr J Cancer2003891445914562015
- FellowesDWilkinsonSMoorePCommunication skills training for health care professionals working with cancer patients, their families and/or carersCochrane Database Syst Rev2004CD00375115106217
- FitzgeraldFThe tyranny of healthN Engl J Med199433119688008035
- GambrillJCommentary: proposals based on too many assumptionsBMJ1999319783
- GoffmanIInteraction ritual, essays on face-to face behavior1972HarmondsworthPenguin
- GriffinSJKinmonthA-LVeltmanMWMEffect of health-related outcomes of interventions to alter the interaction between patients and practitioners: a systematic review of trialsAnnals of Family Medicine2004259560815576546
- HallJARoterDLKatzNRMeta-analysis of correlates of provider behavior in medical encountersMedical Care198826657753292851
- HargieODicksonDBoohanMA survey of communication skills training in UK schools of medicine: present practices and prospective proposalsMed Educ19983225349624396
- HaynesRBEvidence-based medicine and healthcare: advancing the practiceSingapore Med J200445407915334281
- HaynesRBDevereauxPJGuyattGHPhysicians’ and patients’ choices in evidence based practice. Evidence does not make decisions; people do (editorial)BMJ2002324135012052789
- HaynesRBMcKibbonKAKaraniRSystematic review of randomized trials of interventions to assist patients to follow prescriptions for medicationLancet199634838368709739
- HaynesRBMcDonaldHGargAXInterventions for helping patients to follow prescriptions for medication. Cochrane Library (Updated Feb 2002)Summary article in JAMA2002288286879
- HeathIA wolf in sheep’s clothing: a critical look at the ethics of drug takingBMJ2003327856814551104
- HeavenCCleggJMaguirePTransfer of communication skills training from workshop to workplace: the impact of clinical supervisionPatient Educ Couns2006603132516242900
- HeneghanCJGlasziouPPereraRReminder packaging for improving adherence to self-administered long-term medicationsCochrane Database Syst Rev20061CD00502516437510
- KettunenTPoskipartaMLiimatainenLTaciturn patients in health counseling at a hospital: passive recipients or active participators?Qual Health Res20011139941011339082
- KrupatERosenkranzSLYeagerCMThe practice orientations of physicians and patients: the effect of doctor-patient congruence on satisfactionPatient Educ Couns200039495911013547
- LacroixACourvoisierFAufseesser-SteinMThe dialogue of prescribing. Gaps and possibilities for improvement with a brief interactive seminarSchweizerische Rundschau fur Medizin Praxis199281138411535944
- LatterSCourtenayMEffectiveness of nurse prescribing: a review of the literatureJ Clin Nurs200413263214687290
- LazareAShame and Humiliation in the Medical EncounterArch Intern Med19879165383632171
- LevensteinJHBrownJBWestonWWStewartMRoterDPatient-centered clinical interviewing, ch 8 p109Communicating with medical patients1989LondonSage Publications
- LeventhalHLeventhalEAContradaRJSelf-regulation, health, and behavior: a perceptual-cognitive approachPsychol Health19981371733
- LevinsonWRoterDLMulloolyJPPhysician-patient communication. The relationship with malpractice claims among primary care physicians and surgeonsJAMA199727755399032162
- LevinsonWGorawara-BhatRLambJA study of patient clues and physician responses in primary care and surgical settingsJAMA20002841021710944650
- LevinsonWKaoAKubyANot all patients want to participate in decision making. A national study of public preferencesJ Gen Intern Med200520531515987329
- LeyPCommunicating with patients: improving communication, satisfaction and compliance1997CheltenhamStanley Thornes Pub Ltd
- LeyPProfessional non-compliance: a neglected problemBr J Clin Psychol19812015147284648
- LeyPSatisfaction, compliance and communicationBr J Clin Psychol198221241547171877
- LittlePDorwardMWarnerGImportance of patient pressure and perceived pressure and perceived medical need for investigations, referral, and prescribing in primary car: nested observation studyBMJ200432844414966079
- LongoMFCohenDRHoodKInvolving patients in primary care consultations: assessing preferences using discrete choice experimentsBr J Gen Pract200656522354216438813
- MaguirePPitceathlyCKey communication skills and how to acquire themBMJ200232569770012351365
- MakoulGClaymanMLAn integrative model of shared decision making in medical encountersPatient Educ Couns2006603011216051459
- MarinkerMBlenkinsoppABondCFrom compliance to concordance: achieving shared goals in medicine taking1997LondonRoyal Pharmaceutical Society of Great Britain
- McMullanMPatients using the Internet to obtain health information: how this affects the patient-health professional relationshipPatient Educ Coun200663248
- MetcalfeRCompliance, adherence, concordance – what’s in a name?Practical Neurology200551923
- MillerWRollnickSMotivational interviewing2002New YorkGuilford Press
- MisselbrookDArmstrongDPatients’ responses to risk information about the benefits of treating hypertensionBr J Gen Pract200151276911458479
- MurrayELoBPollackLThe impact of health information on the internet on the physician-patient relationship: patient perceptionsArch Intern Med200316317273412885689
- National Audit OfficePrescribing costs in primary care [online]2007 URL: http:/www.nao.org.uk/pn/06-070607454.htm
- National Patient Safety Agency Accessed 16 August 2006. URL: http://www.npsa.nhs.uk
- O’ConnorAMRostomAFisetVDecision aids for patients facing health treatment or screening decisions: systematic reviewBMJ1999319731410487995
- Ottawa Personal Decision Guide Accessed 16 August 2006. URL: http://204.187.39.28/decaids.htm
- PollockKGrimeJPatients’ perceptions of entitlement to time in general practice consultations for depression: qualitative studyBMJ20023256879212351362
- PollockKConcordance in medical consultations: a critical review2005Ch 6OxfordRadcliffe4565
- PoundPBrittenNMorganMResisting medicines: a synthesis of qualitative studies of medicine takingSoc Sci Med2005611335515847968
- ProchaskaJOVelicerWFThe transtheoretical model of health behavior changeAm J Health Promot199712384810170434
- QuillTEBrodyHPhysician recommendations and patient autonomy: finding a balance between physician power and patient choiceAnn Intern Med199612576398929011
- RollnickSMasonPButlerCHealth behavior change: a guide for practitioners2000LondonChurchill Livingstone12
- RoterDLHallJAKernDEImproving physicians’ interviewing skills and reducing patients’ emotional distress. A randomized clinical trialArch Intern Med19951551877847677554
- RoterDLHallJAMerisaREffectiveness of interventions to improve patient compliance: a meta-analysisMedical Care1998361138619708588
- RPSGBFrom compliance to concordance: achieving shared goals in medicine taking1997LondonRoyal Pharmaceutical Society of Great Britain
- SackettDHaynesRBGibsonESPatient compliance with antihypertensive regimensPatient Couns Health Educ19781182110238880
- SchulmanBAActive patient orientation and outcomes in hypertensive treatment: application of a socio-organizational perspectiveMedical Care19791726780763004
- SimpsonSHEurichDTMajumdarSRA meta-analysis of the association between adherence to drug therapy and mortalityBMJ2006333151816790458
- StewartMEffective physician-patient communication and health outcomes: a reviewCan Med Assoc J19951521423337728691
- StewartMAEffective physician–patient communication and health outcomes: a reviewCan Med Assoc J19961531423
- StewartMBrownJBBoonHEvidence on patient-doctor communicationCancer Prev Control19993253010474749
- StimsonGObeying doctor’s orders: a view from the other sideSoc Sci Med19748971044821252
- StrongPThe ceremonial order of the clinic: patients, doctors and medical bureaucracies1979LondonRoutledge and Kegan Paul
- SwensonSLZettlerPLoB‘She gave it her best shot right away’: Patient experiences of biomedical and patient-centered communicationPatient Educ Couns2006612001116154311
- TannenbaumSWhat physicians knowN Engl J Med19933291268718123111
- TuckettDBoultonMOlsonCMeetings between experts – an approach to sharing ideas in medical consultations1985LondonTavistock Publications
- TowleAGodolphinWFramework for teaching and learning informed shared decision makingBMJ19993197667110488010
- WanlessDSecuring our future health: taking a long term view2002LondonHM Treasury
- Whitcher-AlagnaSNadlerAFisherJDDePauloBMReceiving medical help: a psychosocial perspective on patient reactionsNew directions in helping2002New YorkAcademic Press
- World Health OrganizationAdherence to long term therapies: evidence for action [online]2003 URL: http://www.who.int/chronic_conditions/en/adherence_report.pdf
- ZiegelsteinRCFauerbachJAStevensSSPatients with depression are less likely to follow recommendations to reduce cardiac risk during recovery from a myocardial infarctionArch Intern Med200016018182310871976