Abstract
Increased longevity and population aging will increase the number of men with late onset hypogonadism. It is a common condition, but often underdiagnosed and undertreated. The indication of testosterone-replacement therapy (TRT) treatment requires the presence of low testosterone level, and symptoms and signs of hypogonadism. Although controversy remains regarding indications for testosterone supplementation in aging men due to lack of large-scale, long-term studies assessing the benefits and risks of testosterone-replacement therapy in men, reports indicate that TRT may produce a wide range of benefits for men with hypogonadism that include improvement in libido and sexual function, bone density, muscle mass, body composition, mood, erythropoiesis, cognition, quality of life and cardiovascular disease. Perhaps the most controversial area is the issue of risk, especially possible stimulation of prostate cancer by testosterone, even though no evidence to support this risk exists. Other possible risks include worsening symptoms of benign prostatic hypertrophy, liver toxicity, hyperviscosity, erythrocytosis, worsening untreated sleep apnea or severe heart failure. Despite this controversy, testosterone supplementation in the United States has increased substantially over the past several years. The physician should discuss with the patient the potential benefits and risks of TRT. The purpose of this review is to discuss what is known and not known regarding the benefits and risks of TRT.
Introduction
Hypogonadism is a clinical condition in which low levels of serum testosterone are found in association with specific signs and symptoms. When hypogonadism occurs in an older man, the condition is often called andropause or androgen deficiency of the aging male or late onset hypogonadism (LOH).Citation1 The most easily recognized clinical signs of relative androgen deficiency in older men are a decrease in muscle mass and strength, a decrease in bone mass and osteoporosis, and an increase in central body fat. However, symptoms such as a decrease in libido and sexual desire, forgetfulness, loss of memory, anemia, difficulty in concentration, insomnia, and a decreased sense of well-being are more difficult to measure and differentiate from hormone-independent aging. This condition may result in significant detriment to quality of life and adversely affect the function of multiple organ systems.Citation1–Citation3 A health factor-independent, age-related longitudinal decrease in serum testosterone levels has been reported.Citation4 This LOH is important since it features many potentially serious consequences that can be readily avoided or treated, and the affected sector of the population is currently expanding in number. Prospective population-based studies reported in the past decade indicate that low testosterone levels are associated with an increase in the risk for developing type 2 diabetes mellitus and metabolic syndrome and possibly a reduction in survival. Results were similar for bioavailable testosterone.Citation5–Citation7 In men, endogenous testosterone concentrations are inversely related to mortality due to cardiovascular disease and all causes. Low testosterone may be a predictive marker for those at high risk of cardiovascular disease.Citation8 Also, low testosterone levels were associated with increased mortality in male veteransCitation9 but this association could not be confirmed in the Massachusetts Male Aging StudyCitation10 or the New Mexico Aging Study.Citation11
As the clinical symptoms of hormone deficiency in older males may be nonspecific, and since a substantial number of relatively asymptomatic elderly men have testosterone levels outside the normal range for young adults, investigators have suggested that testosterone replacement therapy is only warranted in the presence of both clinical symptoms suggestive of hormone deficiency and decreased hormone levels.Citation12 Restoring serum testosterone levels to the normal range using testosterone replacement therapy results in clinical benefits in some of these areas. Successful management of testosterone replacement therapy requires appropriate evaluation and an understanding of the benefits and risks of treatment.
Aging and hypogonadism
Due to the baby boom that occurred after World War II, the percentage of population in the older age group in developed countries is increasing. Testosterone deficiency is a common disorder in middle-aged and older men but it is underdiagnosed and often untreated. Clinicians tend to overlook it, and the complaints of androgen-deficient men are merely considered part of aging. Hypogonadism affects an estimated 2 million to 4 million men in the United States. Many patients can derive significant benefits from treatment. Testosterone supplementation in the United States has increased substantially over the past several years.Citation13 However, it has been estimated that only 5% of affected men currently receive treatment.
The decline of serum testosterone levels appears to be a gradual, age-related process resulting in an approximate 1% annual decline after age 30. In cross-sectional and longitudinal studies of men aged 30 or 40 years and above, total, bioavailable and free testosterone concentrations fall with increasing age with a steeper decline in bioavailable and free compared with total testosterone concentrations.Citation4,Citation14,Citation15 In older men above the age of 65 or 70 years, the changes in total testosterone are overshadowed by a more significant decline in free testosterone levels.Citation16,Citation17 This is a consequence of the age-associated increase of the levels of sex hormone binding globulin (SHBG) demonstrated by cross-sectional studies, and has now been confirmed by longitudinal studies.Citation18,Citation19 Although the fall is gradual, by the eighth decade, according to the Baltimore Longitudinal Study, 30% of men had total testosterone values in the hypogonadal range, and 50% had low free testosterone values. The rate of age-related decline in serum testosterone levels varies in different individuals and is affected by chronic disease and medications.Citation20 There is evidence that many of these men are not symptomatic.Citation21
Multiple mechanisms are likely to influence the decline in testosterone levels in aging men.Citation22 Lower testosterone levels may result from reduced testicular responses to gonadotrophin stimuli with aging, coupled with incomplete hypothalamo–pituitary compensation for the fall in total and free testosterone levels.Citation23,Citation24 Whether the age-dependent decline in androgen levels leads to health problems in older men is being debated vigorously.Citation21,Citation25
Diagnosis
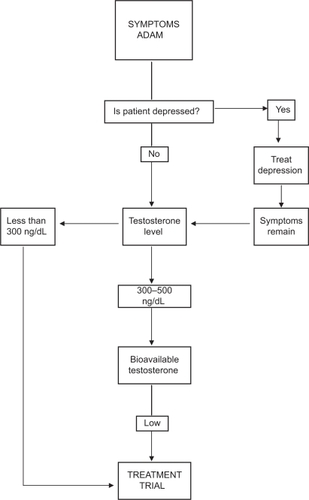
At present, the diagnosis of hypogonadism requires the presence of symptoms and signs suggestive of testosterone deficiency.Citation1,Citation26 The symptom most associated with hypogonadism is low libido.Citation27–Citation29 Other manifestations of hypogonadism include erectile dysfunction, decreased muscle mass and strength, increased body fat, decreased bone mineral density and osteoporosis, mild anemia, breast discomfort and gynecomastia, hot flushes, sleep disturbance, body hair and skin alterations, decreased vitality, and decreased intellectual capacity (poor concentration, depression, fatigue).Citation30 The problem is many of the symptoms of late life hypogonadism are similar in other conditionsCitation31,Citation32 or are physiologically associated with the aging process.Citation33 One or more of these symptoms must be corroborated with a low serum testosterone level.Citation21,Citation25,Citation34 Depression, hypothyroidism and chronic alcoholism should be excluded, as should the use of medications such as corticosteroids, cimetidine, spironolactone, digoxin, opioid analgesics, antidepressants and antifungal drugs. Of course, diagnosis of LOH should never be undertaken during an acute illness, which is likely to result in temporarily low testosterone levels ().
Figure 1 Approach to the diagnosis and treatment of late onset hypogonadism (ADAM = St. Louis University Androgen Deficiency in Aging Males Questionnaire).
The problem with symptoms associated with low serum testosterone is that they may be found in other conditions, which become increasingly common as men age. While the questionnaires, the Androgen Deficiency in Aging Male (ADAM)Citation35,Citation36 and the Aging Male Symptoms Scale (AMS)Citation37,Citation38 (), may be sensitive markers of the low testosterone state (97% and 83%, respectively), they are not tightly correlated with low testosterone (specificity 30% and 39%), particularly in the borderline low serum testosterone range. Therefore, questionnaires are not recommended for screening of androgen deficiency in men receiving health care for unrelated reasons.Citation26 Moreover, healthy ambulatory elderly males over 70, assessed by the AMS, had a high perception of sexual symptoms with mild psychological and mild to moderate somatovegetative symptoms.Citation39 Note also that there is marked inter-individual variation of the testosterone level at which symptoms occur.Citation28,Citation34,Citation40 A low libido by itself is insufficient to allow the diagnosis of hypogonadism.Citation41
Table 1 Androgen Deficiency In Ageing Male (ADAM) questionnaire
Laboratory diagnosis
A thorough physical and biochemical work-up is necessary. Transient decreases of serum testosterone levels such as those due to acute illnesses should be excluded by careful clinical evaluations and repeated hormone measurement. Hypogonadism (primary or secondary) can occur at all ages, including in elderly men. Risk factors for hypogonadism in older men may include chronic illnesses (including diabetes mellitus, chronic obstructive lung disease, and inflammatory arthritic, renal, and HIV-related diseases), obesity, metabolic syndrome, and hemachromatosis.Citation26 Such chronic diseases should be investigated and treated.Citation42 Primary hypogonadism is characterized by raised levels of luteinizing hormone (LH) and follicle-stimulating hormone (FSH) in response to diminished testosterone (and estradiol and inhibin B) feedback. Secondary hypogonadism is characterized by low levels of testosterone associated with low or normal levels of FSH and/or LH.Citation43 However, in older men, the figure is less clear-cut, testosterone deficiency being both primary and secondary.
Serum testosterone has a diurnal variation and levels peak between 08.00 and 10.00 h, a serum sample should be obtained between 07.00 and 11.00 h.Citation44 The most widely accepted parameters to establish the presence of hypogonadism is the measurement of serum total testosterone. Total testosterone levels above 500 ng/dL do not require substitution; patients with serum total testosterone levels below 300 ng/dL will usually benefit from testosterone treatment. If the serum total testosterone level is between 230 and 350 ng/dL in males under 50 years or between 300 and 500 ng/dL in older males, repeating the measurement of total testosterone with sex hormone binding globulin (SHBG) to calculate free testosterone or measuring free testosterone by equilibrium dialysis or bioavailable testosterone is recommended.Citation45 Note that SHBG is elevated in elderly patients and effected by many diseases.Citation30 Measurements of serum LH will assist in differentiating between primary and secondary hypogonadism and serum prolactin is indicated when the serum testosterone is lower than 150 ng/dlCitation46–Citation49 or when secondary hypogonadism is suspected.Citation50,Citation51 Measurement of free or bioavailable testosterone (BT, free plus albumin bound) should be considered when the serum total testosterone concentration is not diagnostic of hypogonadism, particularly in obese men. Bioavailable testosterone appears to correlate better with potential hypogonadal symptoms than does total testosterone.Citation52 A free testosterone level below 65 pg/mL can provide supportive evidence for testosterone treatment.Citation53,Citation54 The gold standard for bioavailable testosterone measurement is by sulphate precipitation and equilibrium dialysis for free testosterone. However, both techniques are not usually available in local laboratories so that calculated values seem preferable. Salivary testosterone, a proxy for unbound testosterone, has also been shown to be a reliable substitute for free testosterone measurements.Citation55–Citation57 Diagnosis of late life hypogonadism requires both symptoms and low testosterone ().
Treatment and delivery systems
Testosterone replacement therapy aims at restoring hormone levels in the normal range of young adults and should, in theory, approximate the natural, endogenous production of the hormone produces and maintains physiologic serum concentrations of the hormone and its active metabolites without significant side effects or safety concerns and, more importantly, alleviates the symptoms suggestive of the hormone deficiency. However, the ultimate goals are to maintain or regain the highest quality of life, to reduce disability, to compress major illnesses into a narrow age range, and to add life to years.
Several different types of testosterone replacement exist including tablets, injections, transdermal systems, oral, pellets, and buccal preparations of testosterone. Selective androgen receptor modulators (SARMs) are under development but not yet clinically available.
The selection of the preparation should be a joint decision of an informed patient and physician.Citation58 Short-acting preparations may be preferred over long-acting depot preparations in the initial treatment of patients with LOH.Citation59 It has been recommended that the optimal serum testosterone level for efficacy and safety should be in the mid range to lower young-adult-male serum testosterone levels as the therapeutic goal.Citation60 However, older males need higher levels to obtain a therapeutic benefit.
Oral agents
The oral form of 17-alpha-alkylated androgen should not be used because of their potential liver toxicity including the development of benign and malignant neoplasmCitation61 in addition deleterious effects on levels of both LDL cholesterol (LDL-C) and HDL cholesterol (HDL-C).Citation62 Testosterone undecanoate, which is absorbed predominantly through the lymphatic system, is widely used outside the United States and has the best safety data. However, it can rarely raise testosterone levels above the mid-range.
Intramuscular injection
Until recently, testosterone cypionate and enanthate were frequently used by intramuscular injection of short-acting testosterone esters that usually produces supraphysiological peaks and hypogonadal troughs in testosterone levels. These fluctuations in testosterone levels may yield variations in libido, sexual function, energy, and mood.Citation63 A “roller coaster” effect can also occur, characterized by alternating periods of symptomatic benefit and a return to base-line symptoms, corresponding to the fluctuations in serum testosterone levels.Citation64,Citation65 However, in our experience many males eventually prefer this form of therapy to the others. Compared with conventional testosterone enanthate or cypionate treatment requiring injection intervals of 2 to 3 weeks, and resulting in supraphysiological serum testosterone levels, injections of testosterone undecanoate (TU) at intervals of up to 3 months offer an excellent alternative for substitution therapy of male hypogonadism.Citation66 The long duration of action creates a problem if there are complications of testosterone therapy.
Transdermal systems
Currently, transdermal testosterone is available in either a scrotal or a nonscrotal skin patch and more recently as a gel preparation, allowing a single application of this formulation to provide continuous transdermal delivery of testosterone for 24 hours, producing circulating testosterone levels that approximate the normal levels (eg, 300 to 1000 ng/dL) seen in healthy men. Daily application is required for each of these. They are designed to deliver 5 to 10 mg of testosterone per day. Scrotal patches produce high levels of circulating dihydrotestosterone (DHT) due to the high 5-alpha-reductase enzyme activity of scrotal skin. The advantages include ease of use and maintenance of relatively uniform serum testosterone levels over time,Citation67 in addition to their efficacy in providing adequate testosterone replacement therapy.Citation68 A reservoir-type transdermal delivery system of testosterone (TS) was developed using an ethanol/water (70:30) cosolvent system as the vehicle. This device is available in Europe as a body patch without reservoir and applied every 2 days.Citation69
Skin irritation may be associated with the use of transdermal systems especially with testosterone patches but is uncommon with gel preparations.Citation70 At present the two testosterone gel preparations (Androgel® and Testim®) are the most commonly used in the United States.
Sublingual and buccal
Cyclodextrin-complexed testosterone sublingual formulation is absorbed rapidly into circulation, where testosterone is released from the cyclodextrin shell.Citation71 This formulation has been suggested to have a good therapeutic potential, after adjustment of its kinetics, to produce physiologic levels of testosterone.
A novel sustained-release mucoadhesive buccal testosterone tablet (Striant®; Columbia Laboratories, Inc.), delivering 30 mg, applied to the upper gum region above the lateral incisors twice daily, in the morning and evening, approximately 12 hours apart. This formulation has been shown to restore serum testosterone concentrations to the physiological range within 4 hours of application, with steady-state concentrations achieved within 24 hours of twice-daily dosingCitation72 and achieves testosterone levels within the normal range.Citation73 Studies indicate that Striant® is an effective, well-tolerated, convenient and discreet treatment for male hypogonadism.Citation74 However, it has had minimal clinical uptake, due to the difficulty of maintaining the buccal treatment in the mouth.
Subdermal implants
Subdermal testosterone implants still offer the longest duration of action with prolonged zero-order, steady-state delivery characteristics lasting 4 to 7 months.Citation75,Citation76 The standard dosage is four 200 mg pellets (800 mg) implanted subdermally at intervals of 5 to 7 months.Citation77 Yet the in vivo testosterone release rate of these testosterone pellets and its determinants have not been studied systematically. However the risk of infection at the implant site and extrusion of the pellets which occurs in 5% to 10% of cases even with the most experienced limit their use.
Benefits of testosterone replacement therapy
Restoring testosterone levels to within the normal range by using testosterone replacement therapy can improve many of the effects of hypogonadism. Most importantly, these include beneficial effects on mood, energy levels and patients’ sense of well-being, sexual function, lean body mass and muscle strength, erythropoiesis and bone mineral density (BMD), cognition and some benefits on cardiovascular risk factors. These are summarized in . Testosterone is well known to help in libido, bone density, muscle mass, body composition, mood, erythropoiesis, and cognition. All these benefits made testosterone replacement therapy in the United States increase substantially over the past several years, with an increase of more than 500% in prescription sales of testosterone products since 1993.
Table 2 Potential benefits of testosterone replacement therapy
Improved sexual desire, function and performance
The prevalence of erectile dysfunction increases markedly with age.Citation78,Citation79 Serum-free testosterone was significantly correlated with erectile and orgasmic function domains of the International Index of Erectile Function (IIEF) questionnaire. Men with greater sexual activity had higher bio-T levels than men with a lower frequency and androgen deficiency may contribute to the age-related decline in male sexuality; correspondingly low levels of bio T were associated with low sexual activity.Citation80,Citation81 Compared with younger men, elderly men require higher levels of circulating testosterone for libido and erectile function.Citation82,Citation83 However, erectile dysfunction and/or diminished libido with or without a testosterone deficiency, might be related to other comorbidities or medications.Citation84
Men with erectile dysfunction (ED) and/or diminished libido and documented testosterone deficiency are candidates for testosterone therapy. Adequate testosterone treatment can restore venous leakage in the corpus cavernosum which is a frequent etiological factor in ED in elderly men.Citation85 Overviews of randomized controlled clinical trials indicate some benefit of testosterone therapy on sexual health-related outcomes; however further investigation in this area is warranted particularly in older men who are not clearly hypogonadal.Citation86,Citation87 Long-term follow-up of testosterone replacement in hypogonadal males and a control group indicates that self-assessment of libido was significantly higher in the testosterone-treated group.Citation88 Testosterone replacement has also been shown to enhance libido and the frequency of sexual acts and sleep-related erections.Citation89,Citation90 Wang et alCitation67 also reported improvement of sexual function; however, their data suggest that there is a threshold level of T above which there is no further enhancement of response. On the other hand, Two placebo-controlled trials reported on the effect of testosterone on overall sexual satisfaction, yielding imprecise results.Citation91,Citation92 Transdermal testosterone replacement therapy, in particular, has been linked to positive effects on fatigue, mood, and sexual function, as well as significant increases in sexual activity.Citation93 1% hydroalcoholic testosterone gel is an effective and safe treatment option in subjects with ED.Citation94
In the presence of a clinical picture of testosterone deficiency and borderline serum testosterone levels, a short therapeutic trial may be tried.Citation95 An inadequate response to testosterone treatment requires reassessment of the causes of the erectile dysfunction.Citation45 There is evidence that the combined use of testosterone and phosphodiesterase type 5 inhibitors in hypogonadal or borderline eugonadal men have a synergetic effect.Citation96–Citation101 The combination treatment should be considered in hypogonadal patients with erectile dysfunction (ED) failing to respond to either treatment alone. Testosterone produces this effect by enhancing the production of nitric oxide synthase. It is unclear whether PDE5-I, testosterone, or the combination of the two should be started first in men with hypogonadism and ED.Citation45 All men with ED should be screened for hypogonadism before treating for erectile dysfunction.Citation102
In addition to improvement in sexual function, testosterone therapy may also improve lower urinary tract symptomatology (LUTS)/bladder functions by increasing bladder capacity and compliance and decreasing detrusor pressure at maximal flow in men with SLOH.Citation103 However, the role of testosterone supplementation in men with erectile dysfunction who are not androgen deficient or in the low to normal range needs further investigation to determine whether testosterone therapy will improve erectile function in older men and to weigh the risk–benefit ratio for testosterone therapy in this setting.Citation86
Bone mineral density
Chronically ill men may have both apparent androgen deficiency and low bone mass.Citation104 Osteopenia, osteoporosis, and fracture prevalence rates are greater in hypogonadal younger and older men.Citation105 The prevalence of osteoporosis in testosterone deficient males is double that of those with normal testosterone level.Citation106,Citation107 Testosterone plays a major role in BMD.Citation108 Bone density in hypogonadal men of all ages increases under testosterone substitution provided the dose is high enough;Citation109–Citation111 although normal adult bone mass is not reached.Citation112 Testosterone produces this effect by increasing osteoblastic activity and through aromatization to estrogen reducing osteoclastic activity. The role of the partial androgen deficiency in aging males in bone fracture rate remains to be established.Citation113 Patients with prostate cancer treated with androgen deprivation therapy have an increased risk of osteoporotic fracture.Citation114 The long-term benefit of testosterone requires further investigation. However, the correlation with bioestradiol, the levels of which decline in elderly males, was even stronger, suggesting that part of the androgen effects on bone are at least partially indirect, mediated via their aromatization.Citation115,Citation116 An increase in osteocalcin levels, an index of osteoblast activity was observed,Citation90 and a decrease of hydroxyproline excretion, an index of bone resorption also was noted.Citation117
Assessment of bone density at 2-year intervals is advisable in hypogonadal men, and serum testosterone measurements should be obtained in all men with osteopenia.Citation118,Citation119 Trials of the effects of testosterone replacement therapy on bone mineral density yielded mixed results.Citation120 Increases in spinal bone density have been realized in hypogonadal men,Citation121 with most treated men maintaining bone density above the fracture threshold.Citation122 An improvement in both trabecular and cortical bone mineral density of the spine was seen, independent of age and type of hypogonadism; in addition, a significant increase in paraspinal muscle area has been observed, emphasizing the clinical benefit of adequate replacement therapy for the physical fitness of hypogonadal men.Citation123 The pooled results of a meta-analysis suggest a beneficial effect on lumbar spine bone density and equivocal findings on femoral neck BMD. Trials of intra muscular testosterone reported significantly larger effects on lumbar bone density than trials of transdermal testosterone, particularly among patients receiving chronic glucocorticoids.Citation124 Also in eugonadal men with osteoporosis, Testosterone esters (250 mg/2 weeks) increased BMD;Citation125 again, the effects in elderly men are less convincing, though the 3 year study of Amory et alCitation126 showed a significant increase in hip BMD. None of studies have been large enough to show a fracture risk reduction with testosterone replacement therapy.
Improved body composition and muscle mass and strength
The aging process is accompanied by significant changes in body composition characterized by decreased fat free mass and increased and redistributed fat mass. These changes can impose functional limitations and increase morbidity.Citation127,Citation128 Maximal muscle strength correlates with muscle mass independently of age.Citation129 In men, declining testosterone levels that occur with aging can be a contributing factor to these changes by direct effect on muscle cells by testosterone or by stimulating IGF-1 expression directly and indirectly leading to increased muscle protein synthesis and growth.Citation130 Epidemiologic studies have demonstrated a correlation between bioavailable testosterone concentrations and fat-free mass;Citation131 however the correlation with grip strength is not clear.Citation131,Citation132
Testosterone replacement may be effective in reversing age-dependent body composition changes and associated morbidity.Citation133 Testosterone administration improves body composition decrease of fat mass, increase of lean body mass.Citation134–Citation136 In most of these studies, the body weight change did not differ significantly. After androgen supplementation to elderly men, generally at a biweekly dose of 200 mg T enanthate, there is a relatively modest increase in muscle mass (±2 kg)Citation117 and/or arm circumference and grip strength, whereas fat mass was decreased modestly.Citation137–Citation139
Testosterone therapy was associated with a greater improvement in grip strength than placebo.Citation135,Citation139,Citation140 Changes in lower-extremity muscle strength and measures of physical function were reported in only a few studies and were inconsistent. Recent cross-sectional studies showed that in aging men there are also positive correlations between testosterone and muscle strength parameters of upper and lower extremities, as measured by leg extensor strength and isometric hand grip strength.Citation141 Moreover, testosterone was positively associated with functional parameters, including the doors test as well as “get up and go” test, and 5-chair sit/stand test.Citation142 On the other hand, some reported an increase in lean body mass (LBM) but no change in physical function,Citation92 or an increase in strength of knee extension or flexion.
Although there is a potential role of testosterone in the management of frailty, we do not know whether testosterone replacement improves physical function and other health-related outcomes, or reduces the risk of disability, falls, or fractures in older men with low testosterone levels in addition to the long-term risks and benefits of testosterone supplementation in older men.Citation143
Mood and energy and quality of life
Men older than 50 years with low free testosterone levels had poorer quality of life. Hypogonadal men commonly complain of loss of libido, dysphoria, fatigue, and irritability.Citation67,Citation70,Citation144,Citation145 These symptoms overlap with signs and symptoms of major depression. There is significant inverse correlation between bioavailable testosterone and a depression score in elderly men, independent of age and weight but not with total testosterone levels.Citation146 There was a reduced libido and reduced feelings of well being and minimal effect on mood in patients with induced testosterone deficiency; the depressive symptoms during the hypogonadal state were reversed by testosterone replacement.Citation147 One study showed that the relationship between testosterone level and depression was nonlinear and may be idiosyncratic.Citation148 The risk of depression was increased for hypogonadal and hypergonadal men, but this effect was only detectable in underweight and obese men, not in ‘normal’ weight men in whom a linear decrease in the risk of depression with increasing testosterone level was noted.Citation149
Testosterone replacement therapy has variable effects on mood, energy and sense of well being. The results of placebo-controlled randomized trials on testosterone’s effect on quality of life and depressive mood were inconsistent across trials and imprecise.Citation150–Citation152 Testosterone administered to nondepressed eugonadal men at physiological doses, did not result in significant effects on mood.Citation153,Citation154 Administration of supraphysiological doses of testosterone to eugonadal men has been associated with mania in a small proportion of men.Citation155,Citation156
In hypogonadal men, testosterone replacement was associated with improved mood and well-being, and reduced fatigue and irritability.Citation157–Citation159 Randomized controlled trials of testosterone therapy in men without or with underlying chronic illness using a variety of testosterone formulations report equivocal improvements in quality of life measures, including general well-being and fatigue.Citation41,Citation86,Citation160 Testosterone replacement of hypogonadal men with MDD might be an effective antidepressantCitation161,Citation162 or augmentation to partially effective antidepressant,Citation163 Testosterone gel had significantly greater improvement as augmentation therapy in depressive symptoms than subjects receiving placebo in hypogonadal men with selective serotonin reuptake inhibitor (SSRI) partial response.Citation164 In one study, the improvements in mood persisted.Citation67 These significant correlations with T levels were only observed when T levels were below the normal range, which suggests that once a minimally adequate T/dihydrotestosterone (DHT) level was achieved, further increase did not further contribute to improvement of mood.Citation67,Citation157 However, the studies reported tend to be of limited size and duration, with a lack of large-scale trials with extended long-term follow-up. In HIV-infected men, testosterone therapy was well tolerated and effective in ameliorating symptoms of hypogonadism. For patients with major depression and/or dysthymia, improvement was equal to that achieved with standard antidepressants with significant improvement in depression inventory score. This effect may be a direct effect of testosterone or related to positive effects of testosterone on weight and/or other anthropometric indices. Additional studies are needed to assess the effects of testosterone on clinical depression indices in human immunodeficiency virus-infected patients.Citation165,Citation166
On the other hand, several placebo-controlled testosterone replacement studies did not show a testosterone-placebo difference distinguishable with respect to mood.Citation150,Citation164,Citation167,Citation168 No relationship between testosterone level and depressive symptoms was found in the Massachusetts Male Aging Study (MMAS).Citation14 This discrepancy in the results of the effects of testosterone replacement therapy on mood may be explained by the genetic polymorphism in the androgen receptor which defines a vulnerable group in whom depression is expressed when testosterone levels fall below a particular threshold.Citation169,Citation170
Finally, the available controlled studies using exogenous testosterone for depression in elderly men are limited, and testosterone treatment must be considered experimental. The best candidates for treatment may be hypogonadal men who are currently taking an existing antidepressant with inadequate response.Citation171–Citation173 Additional studies have been recommended incorporating vitality, well-being and/or quality of life as end points.
Cognitive function
Subclinical androgen deficiency was hypothesized to enhance the expression of AD related peptides in vivo.Citation174 Age-related decreases in bioavailable T predicted age-related decline in visual and verbal memory.Citation175 Men with a higher ratio of total testosterone to SHBG predict a reduced incidence of Alzheimer’s diseaseCitation176 and patients with Alzheimer’s disease had a lower ratio of total testosterone to SHBG compared with age-matched controls.Citation177 In the Baltimore Longitudinal Study of Aging (BLSA), a prospective longitudinal studyCitation176 risk for AD was reduced by 26% for each 10 unit (nmoL/nmoL) increase in free T at 2, 5 and 10 years prior to AD diagnosis. Altered T levels in AD may precede rather than follow diagnosis.
There is good evidence for a strong correlation between T levels and cognitive performance such as spatial abilities or mathematical reasoning.Citation178 Higher bioavailable and free testosterone concentrations have each been associated with better performance in specific aspects of memory and cognitive function, with optimal processing capacity found in men ranging from 35 to 90 years of age even after adjustment for potential confounders including age, educational attainment and cardiovascular morbidity;Citation179–Citation181 whereas total testosterone was not.Citation182 However, contradictory findings have also been reported, two cross-sectional studies did not show a relationship between total or free testosterone and measures of working memory, speed/attention or spatial relations in men aged from 48 to 80 years.Citation184 In another cross-sectional analyses of similarly aged men, no association was found between lower free testosterone levels and higher performance on spatial visualization tasks, and between higher free and total testosterone levels and poorer verbal memory and executive performance; however there is correlation with faster processing speed.Citation184,Citation185 A possible source of conflicting results in these studies may stem from interactions between testosterone levels and other risk factors for cognitive impairment such as apolipoprotein E 4 genotypeCitation186 and systemic illness which cause low testosterone.Citation24,Citation177,Citation187
In men undergoing hormonal therapy for prostate cancer, suppression of endogenous testosterone synthesis and blockade of the androgen receptor resulted in a beneficial effect on verbal memory but an adverse effect on spatial abilityCitation188 and visuomotor slowing and slowed reaction times in several attentional domains;Citation189 plasma amyloid levels increased as T levels decreased.Citation190 Discontinuation of treatment resulted in improved memory but not visuospatial abilities.Citation190 One of the possible protective mechanisms of action of T would be through its conversion into estradiol (E2), the most potent estrogen. Both serum E2 and T levels were lower in men with AD compared to age-matched controls.Citation191,Citation192 E2 could exert protective effects on the brain structures in aging patients.Citation193
Trials of testosterone therapy in men to evaluate its effects on measures of cognitive function and memory to date were all relatively small and of a relatively short duration and have shown mixed results.Citation177,Citation194 Small-scale T intervention trials in elderly men suggest that some cognitive deficits may be reversed, at least in part, by short term T supplementation.Citation178 Androgen supplementation in elderly hypogonadal men improves spatial cognitionCitation117,Citation195 and verbal fluencyCitation196,Citation197 and in elderly men without dementia, it may reduce working memory errors.Citation198 In addition, transdermal testosterone or DHT treatment in men aged 34 to 70 years improved verbal memory and spatial memory respectively,Citation199 and intramuscular testosterone improved verbal and spatial memory and constructional abilities in non-hypogonadal men with mild cognitive impairment and Alzheimer’s disease.Citation200 In one study of healthy men aged 50 to 90 years, intramuscular testosterone alone or in combination with anastrozole improved spatial memory, whereas verbal memory only improved in testosterone-treated men in the absence of anastrozole, raising the possibility that part of the effect of exogenous testosterone is mediated by its aromatization to estradiol.Citation200
However, in men with Alzheimer’s disease testosterone treatment appeared to improve quality of life without impacting on measures of cognition.Citation201 In a randomized, placebo-controlled crossover trial intramuscular testosterone therapy resulted in decreased verbal memory.Citation202 In other placebo-controlled randomized trials, one of which studied patients with Alzheimer’s dementia and low testosterone levels,Citation203 reported imprecise effects on several dimensions of cognition, none of which was significant after pooling.Citation203,Citation204
Therefore, although the evidence from observational studies is not uniform, lower free testosterone appears to be associated with poorer outcomes on measures of cognitive function, particularly in older men and testosterone therapy in hypogonadal men may have some benefit for cognitive performance.
Improving metabolic syndrome and diabetes type 2, cardiovascular disease
Many of the components of the metabolic syndrome (obesity, hypertension, dyslipidemia impaired glucose regulation, and insulin resistance) are also present in hypogonadal men. Lower testosterone levels are associated with surrogate markers for cardiovascular disease, including less favorable carotid intima medial thicknessCitation205–Citation207 ankle/brachial index as a measure of peripheral arterial diseaseCitation208 and calcific aortic atheroma.Citation209 Endogenous testosterone concentrations are inversely related to mortality due to cardiovascular disease and all causes. Low testosterone may be a predictive marker for those at high risk of cardiovascular disease.Citation8 Thus, lower testosterone levels, erectile dysfunction and conditions associated with higher cardiovascular risk appear to be interrelated.Citation210,Citation211 Obesity induces a decrease of T levels via a decrease in SHBG levels, and morbid obesity also induces a decrease of FT.Citation212 There is evidence to suggest that an inverse relationship exists between serum testosterone levels and the degree of obesity in men.Citation213,Citation214 There is a close relationship between obesity and low serum testosterone levels in healthy men.Citation215 Twenty percent to 64% of obese men have a low serum total or free testosterone level.Citation216 Visceral obesity is more strongly inversely related to total and free testosterone levels than other forms of obesity.Citation217,Citation218 The Relationship between reduced testosterone and obesity in men can be explained by the hypogonadal-cytokine-obesity cycleCitation219,Citation220 and it exhibits antiatherogenic effects at the tissue level, whether mediated by classical or nonclassical pathways.Citation221,Citation222
Initially cross-sectional studies but later also longitudinal studies were able to confirm that low testosterone levels and sex hormone-binding globulin (SHBG) were predictive of the metabolic syndrome, not only in obese men but also in men with a body mass index (BMI) <25 kg/m 2.Citation223,Citation224 The metabolic syndrome and type 2 diabetes mellitus are associated with low plasma testosteroneCitation34,Citation225,Citation226 and insulin sensitivity.Citation34,Citation227,Citation228 There is positive correlation between serum testosterone levels and insulin sensitivity in men across the full spectrum of glucose toleranceCitation229 and an improvement of insulin sensitivity was noted after replacement.Citation230 Although Abate et al Citation231 found no association between low plasma levels of bioavailable testosterone and insulin resistance in eugonadal men; a recent larger study (NHANES [National Health and Nutrition Examination Survey]) showed that low free and bioavailable testosterone levels, even in the normal range, are associated with diabetes, independent of adiposity.Citation216 Serum testosterone should be measured in men with type 2 diabetes mellitus with symptoms suggestive of testosterone deficiency. The effects of testosterone administration on glycemic control of men with diabetes mellitus are much less certain.Citation232–Citation234 By increasing lean body mass and reducing fat mass, testosterone therapy modulates insulin resistance and risk of metabolic syndrome.Citation232
Studies on androgen replacement in elderly men on LDL-C and HDL-C are controversial.Citation235,Citation236 The correlation between testosterone levels and HDL-C and insulin sensitivity is only observed within the physiologic male concentration range of testosterone.Citation237 A physiologic dose of androgens did not cause significant change in lipids.Citation238 A recent randomized controlled trial showed decrease in high-density lipoprotein cholesterol.Citation239 A 24-week, multi-center, randomized, parallel-group study by Dobs et alCitation240 of transdermal and intramuscular administration of androgens in 58 men did not detect any significant change in HDL levels or in the ratio of total cholesterol to HDL in either group, apart from the mode of therapy. In addition, testosterone replacement decreases lipoprotein (a).Citation19 The mechanism of the fall in lipids might be related to the decrease in the visceral abdominal fat massCitation241 under the influence of androgens, which inhibit lipoprotein lipase activity and increase lipolysisCitation242,Citation243 with improvement of insulin sensitivity and mobilization of triglycerides from abdominal fat tissue.Citation244 Supraphysiological T levels induce an increase in LDL-C and a decrease of HDL-CCitation245–Citation247 and may increase the risk of cardiovascular disease.
Low androgen levels increase the risk of cardiovascular disease in men.Citation236 Data are lacking as to whether higher testosterone levels predict reduced incidence of combined nonfatal and fatal major cardiovascular events.Citation101 The inverse correlation between T levels and the severity of coronary artery diseaseCitation248 may be related to the fact that low androgen levels are accompanied by an accumulation of abdominal visceral fat,Citation249–Citation251 which is known to be associated with increased cardiovascular risk factorsCitation252 impaired glucose tolerance, and non-insulin-dependent diabetes mellitus (syndrome X).Citation253
No consistent relationship between the levels of free or total testosterone and coronary atherosclerosis in men undergoing coronary angiography has been observed.Citation151,Citation254 Testosterone-replacement therapy does not increase the incidence of cardiovascular disease or events such as myocardial infarction, stroke, or angina.Citation88 A meta-analysisCitation255 in 2007 concluded that the current available evidence shows no association between testosterone replacement therapy and cardiac events. Transdermal testosterone replacement therapy was found to be beneficial for men with chronic stable angina as they had greater angina-free exercise tolerance than placebo-treated controls.Citation151
However, trials of testosterone therapy generally have not been designed or adequately powered to detect effects on clinically significant cardiovascular events.Citation86,Citation256 The outcome of most studies in men report either a favorable or neutral effect of normal T levels on cardiovascular disease in men. The administration of T in physiological concentration increases coronary blood flow in patients with coronary heart disease.Citation257 Beneficial effects on endothelial functionCitation258 and myocardial ischemia have also been demonstrated,Citation248,Citation259,Citation260 but not with cardiovascular mortality.Citation257,Citation258 In addition, testosterone has a negative correlation with fibrinogen, plasminogen activator inhibitor-1Citation261 and a direct effect on several vasoactive factors such as endothelin,Citation262 prostacyclin, thromboxane A2 and platelet aggregation,Citation263 blood coagulation, and fibrinolysis, respectively.Citation248,Citation261
Thus, although lower testosterone levels are associated with higher cardiovascular risk and to an extent with mortality in aging men, randomized controlled clinical trials of adequate size and duration are needed to determine whether testosterone therapy will reduce morbidity and mortality from cardiovascular disease in hypogonadal or eugonadal men.
Improving anemia
Endogenous androgens are known to stimulate erythropoiesis; increase reticulocyte count, blood hemoglobin levels and bone marrow erythropoietic activity in mammals, whereas castration has opposite effects. Testosterone deficiency results in a 10% to 20% decrease in the blood hemoglobin concentration, which can result in anemia.Citation264,Citation265 Young hypogonadal men usually have fewer red blood cells and lower hemoglobin levels than age-matched controls, whilst healthy older men also may have lower hemoglobin than normal young men. The main androgen involvement in the mechanism of normal hematopoiesis is thought to involve direct stimulation of renal production of erythropoietin by testosterone. Moreover, the latter may also act directly on erythropoietic stem cells.Citation265
Risks of testosterone replacement therapy
The risks of testosterone replacement therapy depend upon age, life circumstances, and other medical conditions.Citation26 There is a risk for prostate cancer and worsening symptoms of benign prostatic hypertrophy, liver toxicity and tumor, worsening symptoms of sleep apnea and congestive heart failure, gynecomastia, infertility and skin diseases. Testosterone replacement therapy is not appropriate for men who are interested in fathering a child because exogenous testosterone will suppress the HPT axis. The risks of testosterone replacement therapy are summarized in .
Table 3 Potential risks for testosterone replacement therapy
The prostate and testosterone replacement therapy
In aging men with late-onset hypogonadism, TRT may normalize serum androgen levels but appears to have little effect on prostate tissue androgen levels and cellular functionsCitation266 and causes no significant adverse affects on the prostate.Citation267 At the present time, there is no conclusive evidence that testosterone therapy increases the risk of prostate cancer or benign prostatic hyperplasia (BPH).Citation45,Citation268,Citation269
Benign prostatic hyperplasia
It is well known that the presence of androgen is required for the development of benign prostatic hyperplasia. Testosterone supplements increase prostate volume with, eventually mild increase in prostate specific antigen (PSA) levels in old men.Citation90,Citation117,Citation270 Although a meta-analysisCitation58 showed that the total number of prostate events combined was significantly greater in testosterone-treated men than in placebo-treated men, the majority of events are due to prostate biopsy; and the marked reduction in serum testosterone caused by chemical or surgical castration causes reduced prostate volume. At the same time, many studiesCitation271–Citation273 have failed to show significant exacerbation of voiding symptoms attributable to benign prostatic hyperplasia during testosterone supplementation, and complications such as urinary retention have not occurred at higher rates than in controls receiving placebo nor has there been any difference in the urine flow rates, postvoiding residual urine volumes, and prostate voiding symptoms with patients receiving treatment in these studies. The poor correlation between prostate volume and urinary symptoms explain this illogicality.
Finally, although there are no compelling data to suggest that testosterone treatment exacerbates lower urinary tract symptoms (LUTS) or promotes acute urinary retention, severe LUTS, due to BPH, represent a relative contraindication which is no longer applicable after successful treatment of lower urinary tract obstruction.Citation45
Prostate cancer
Prostate cancer is well known to be, in the majority of cases, an androgen sensitive disease, and prostate cancer has been treated in patterns designed to lower testosterone levels.Citation270 Androgen replacement therapy is an absolute contraindication. There is also no good evidence that testosterone treatment will convert subclinical prostate cancer to clinically detectable prostate cancer,Citation45 although some case reports reported this correlation.Citation274,Citation275 In a retrospective analysis of hypogonadal men who underwent prostate biopsy prior to testosterone replacement therapy, no increase in the risk of prostate cancer in men was revealed compared to those without prostatic intraepithelial neoplasia at baseline.Citation276
The prevalence of prostate cancer in many studies receiving testosterone replacement therapy was similar to that in the general population.Citation67,Citation277 So far, there is no compelling evidence that testosterone has a causative role in prostate cancer.Citation271,Citation272,Citation278,Citation279 In fact, it should be recognized that prostate cancer becomes more prevalent exactly at the time of a man’s life when testosterone levels decline. At a median of 19 months of TRT hypogonadal patients with a history of prostate cancer had no PSA recurrence and had statistically significant improvements in total testosterone and hypogonadal symptoms. In highly select patients after radical retropubic prostatectomy TRT can be administered carefully and with benefit to hypogonadal patients with prostate cancer.Citation280 Hormonal replacement in patients that underwent castration seems to be feasible in improving intense symptoms associated with androgen deprivation. After 18 months, no evidence of recurrence was noted. It is an experimental alternative for highly symptomatic patients, but the short follow-up and the small number of patients cannot allow for definitive conclusions and should be studied further.Citation281 A recent prospective studyCitation282 did not show definitive data to confirm the relationship between serum sex hormones and prostate cancer. There is, however, unequivocal evidence that testosterone can stimulate growth and aggravate symptoms in men with locally advanced and metastatic prostate cancer.Citation283,Citation284 Men successfully treated for prostate cancer and diagnosed with hypogonadism are candidates for testosterone replacement after a prudent interval if there is no clinical or laboratory evidence of residual cancer.Citation285,Citation286 In addition, no effect was found of testosterone replacement therapy on PSA levelsCitation287–Citation289 and the change in PSA were not influenced by the mode of testosterone replacement therapy, patient age, or baseline levels of PSA or testosterone.Citation290
The online prostate cancer risk calculator is one of the most commonly used tools to assist the clinician in assessing the risk of prostate cancer.Citation291–Citation293 All men who present for TRT should undergo prostate biopsy if they have abnormal PSA level or abnormal result on digital rectal examination with low threshold to do or repeat prostate biopsy if the PSA level or digital rectal exam changes. Prostatic biopsy or referral to a urologist is recommended if PSA rises above 4.0 ng/mL or if it increases either by more than 1.5 ng/mL/year or by more than 0.75 ng/mL/year over 2 years,Citation294 or if PSA rises by more than 1.0 ng/mL in the first 6 months of treatment or by more than 0.4 ng/mL/year thereafter.Citation295
In summary, there is no convincing evidence that the normalization of testosterone serum levels in men with low levels is deleterious. TRT can be cautiously considered in selected hypogonadal men treated with curative intent for prostate and without evidence of active disease.Citation296
Liver problems
Benign and malignant hepatic tumors, intrahepatic cholestasis, hepatotoxicity, and liver failure have been reported with testosterone replacement therapy.Citation297,Citation298 These unfavorable hepatic effects do not appear to be associated with transdermal or intramuscular injections. For this reason the oral forms of testosterone, with the exception of testosterone undecanoate, are discouraged. Other liver abnormalities associated with TRT include Peliosis hepatis, hepatocellular adenoma, and carcinoma.Citation299
The risk of polycythemia
There is a correlation between high testosterone levels and high hemoglobin, most likely because testosterone stimulates erythropoiesis. Erythrocytosis can develop during testosterone treatment, especially in older men treated by injectable testosterone preparations.Citation45 Hemoglobin at puberty increases 15% to 20% in boys, men have higher levels of hemoglobin than women, and hypogonadism causes a decline in hemoglobin levels that can be restored with testosterone replacement therapy.Citation139,Citation300 But the elevation in hemoglobin above certain levels may have bad outcomes, particularly in elderly, because the increase in blood viscosity could exacerbate vascular disease in the coronary, cerebrovascular, or peripheral vascular circulation, especially in people with other diseases that cause secondary polycythemia, ie, chronic obstructive pulmonary disease.Citation301–Citation303 Injection is associated with higher potentials for erythrocytosis than topical preparations.Citation240 Snyder et al noticed that erythrocytosis occurred in 5.5% of scrotal transdermal users, and the majority of changes took place over the first three months of treatment.Citation92 It has been demonstrated that testosterone dosage correlates with the incidence of erythrocytosis,Citation67 The frequency of polycythemia (hematocrit over 51%) is related most of the time to supra-physiological levels.Citation240 The resolution of erythrocytosis (hematocrit >52%), untreated obstructive sleep apnea, or untreated severe congestive heart failure, is required before starting on testosterone treatment.Citation19,Citation58,Citation304
Periodic hematological assessment is indicated (ie, before treatment, then at 3 to 4 months and at 12 mo in the first year of treatment and annually thereafter). While it is not yet clear what critical threshold is a desirable, dose adjustment and/or periodic phlebotomy may be necessary to keep hematocrit below 52% to 55%.Citation45,Citation58,Citation305
Other effects of testosterone replacement therapy
Psychotic symptoms, excessive libido and aggression, in addition to physical and psychological dependence and withdrawal syndromes have been rarely described with testosterone treatment,Citation306,Citation307 though the validity of testosterone or the cause is uncertain. Kenny et alCitation204 did not find that significant changes in behavior, function, depression, or cognitive performance occurred following 12 weeks of testosterone replacement in men with low testosterone levels and early-to-moderate cognitive impairment.
Gynecomastia is a benign complication of testosterone treatment. It is related to aromatization of testosterone into estradiol in peripheral fat and muscle tissue. Even the ratio of estradiol to testosterone usually remains normal. It occurs especially with testosterone enanthate or cypionate. Dose adjustment may be necessary.
Diminished testicular size and compromised fertility during testosterone replacement therapy occur because of the down-regulation of gonadotropins.Citation308 The administration of exogenous testosterone as a means of male contraception is under study.Citation309 In these men, azoospermia usually results within approximately 10 weeks of beginning therapy. Rebound of the sperm count to baseline levels occurs within six to 18 months of cessation, and subsequent fertility has been demonstrated.Citation310 Supraphysiologic doses of androgens may cause decreased testicular size, and azoospermia.Citation311
Testosterone-replacement therapy has been associated with exacerbation of sleep apnea.Citation312,Citation313 The effect of testosterone is not on the dimensions of the upper airway, but it most likely contributes to sleep disorder breathing by central mechanisms.Citation314 The development of signs and symptoms of obstructive sleep apnea during testosterone therapy warrants a formal sleep study and treatment with continuous positive airway pressure (CPAP) if necessary. If the patient is unresponsive or cannot tolerate CPAP, the testosterone must be reduced or discontinued.
Transdermal testosterone-replacement therapy is associated with a variety of skin reactions, mainly erythema or pruritus, which are more common with patches than with gel preparations.Citation67 Intramuscular injections of testosterone can cause local pain, soreness, bruising, erythema, swelling, nodules, or furuncles.Citation315 Supraphysiologic doses of androgens may cause acne.Citation311
Testosterone is anabolic, and it will cause some nitrogen, sodium and water retention. Edema may be worsened in patients with preexisting cardiac, renal, or hepatic disease. Hypertension has rarely been reported.Citation316
Hyperandrogenism was reported in a female whose partner was using testosterone gel.Citation317
Monitoring patients on testosterone replacement
Laboratory parameters that should be monitored before and during treatment include PSA, hemoglobin, hematocrit, lipid profiles, and liver function tests. Patients should also be monitored for signs of edema, gynecomastia, sleep apnea, lower urinary tract symptoms, and low BMD. There are clinical practice guidelines from the Endocrine Society for monitoring patients receiving TRT.Citation45 Testosterone level, digital rectal exam, PSA, hematocrit, BMD, lipids, and liver function tests should be checked at baseline then evaluate the patient 3 and 6 months after treatment starts and then annually to assess whether symptoms have responded to treatment and whether the patient is suffering from any adverse effects.
Testosterone levels should be monitored 3 months after initiation of testosterone therapy. A mid-morning total serum testosterone level should be obtained. A target range of 400 to 500 ng/dL (14.0 to 17.5 nmol/L) for older men is suggested. However, if there is no symptomatic response, higher levels may be necessary. For injectable testosterone, the serum level can be measured between injections. For men treated with a transdermal testosterone patch, the serum level should be measured 3 to 12 hours after patch application. In patients receiving buccal testosterone tablets, the serum level should be measured immediately before application of a fresh system. Patients on testosterone gel may have levels checked anytime after at least 1 week of therapy.Citation45 In all cases, bioavailable testosterone levels should also be monitored as testosterone therapy lowers SHBG.
The hematocrit should be checked at baseline, at 3 and 6 months, and then annually. If hematocrit is more than 54%, stop therapy until hematocrit decreases to a safe level; evaluate the patient for hypoxia and sleep apnea; reinitiate therapy with a reduced dose. BMD of lumbar spine and/or femoral neck should be measured at baseline every 1 to 2 years of testosterone therapy in hypogonadal men with osteoporosis or low trauma fracture. A digital rectal examination and PSA level should be obtained before initiating treatment, at 3 months, and then in accordance with guidelines for prostate cancer screening, depending on the age and race of the patient. A urologic consultation is mandatory if any of the following is present ().
Table 4 When a urological consultation is needed
The use of testosterone preparations should be discussed with patients and then closely monitored for efficacy and toxicities.Citation3,Citation318–Citation320 Failure to benefit from clinical manifestations should result in discontinuation of treatment after 3 months for libido and sexual function, muscle function, and improved body fat; and a longer interval for bone mineral density. Further investigation for other causes of symptoms is then mandatory.Citation45
Contraindications to testosterone replacement therapy
Before starting patients on TRT, health care providers must rule out contraindications to treatment (). The presence of a clinical prostatic carcinoma is an absolute contraindication for HRT and should be carefully excluded by PSA, rectal examination and, eventually, biopsy before starting any therapy.Citation45 There is also no clear recommendation for men successfully treated for prostate cancer who would be potential candidates for testosterone substitution after a ‘prudent’ interval if there is no clinical or laboratory evidence of residual cancer.Citation45
Table 5 Contraindications to testosterone replacement therapy
The presence of breast cancer is also a contraindication for TRT as well as a prolactinoma, as their growth may be stimulated by HRT.Citation26 Very high risk of serious adverse outcomes, undiagnosed prostate nodules or indurations, unexplained PSA elevation, erythrocytosis (hematocrit > 50%), severe lower urinary tract symptoms with benign prostatic hyperplasia with an International Prostate Symptom Score (IPSS) >19, and unstable congestive heart failure (class III or IV), untreated obstructive sleep apnea are considered as moderate- to high-risk factors for potential adverse outcomes.Citation26,Citation45,Citation319
Conclusion
Male hypogonadism and its treatment is a rapidly evolving area. While male hypogonadism has previously been underdiagnosed, the apparently increasing incidence and expanding range of treatment options may facilitate greater awareness of the condition. The symptoms in the elderly have a complex origin. It may be reasonably assumed that the age-associated decrease in T levels is in part responsible for the symptoms of aging. The benefits and risks of testosterone therapy must be clearly discussed with the patient and assessment of prostate and other risk factors considered before commencing testosterone treatment. There is some benefit from testosterone replacement therapy on muscle mass and strength, fat mass, BMD, sexual function, mood and general sense of well-being. Therefore, it seems logical to consider that in elderly men with subnormal T levels and clinical symptoms suggestive of androgen deficiency, hormone replacement therapy in combination with physical activity (resistance training) and adequate nutrition will result in an optimal increase in muscle strength, BMD, and general sense of well-being. However, data on clinical effects of androgen substitution, such as cardiovascular morbidity and mortality, falls and bone fracture rates are not yet available. Response to testosterone treatment should be assessed. If there is no improvement of symptoms and signs, treatment should be discontinued and the patient investigated for other possible causes of the clinical presentations. The major contraindication for androgen supplementation is the presence of a prostatic carcinoma.
Future of TRT
Hypogonadism may present to a range of specialties. Previously, late-onset hypogonadism has not been well understood. Studies conducted to date have been too small to address potential long-term adverse effects, and there are risks in extrapolating benefit from epidemiological studies. Many questions in the treatment of hypogonadism remain unanswered, and there is a need for large clinical trials; or at least a meta-analysis of the extensive short-term data combined with analysis of long-term clinical experience which many physicians working in the field now have; to assess the long-term benefits and risks of TRT in older men with late-onset hypogonadism.
Disclosures
The authors disclose no conflicts of interest.
References
- NieschlagESwerdloffRBehreHMInvestigation, treatment and monitoring of late-onset hypogonadism in malesAging Male20058565816096159
- MoralesASchulmanCCTostainJWuFCWTestosterone deficiency syndrome (TDS) needs to be named appropriately – the importance of accurate terminologyEur Urol20065040740916854520
- RhodenELMorgentalerARisks of testosterone-replacement therapy and recommendations for monitoringN Engl J Med2004350548249214749457
- HarmanSMMetterEJTobinJDPearsonJBlackmanMRBaltimore Longitudinal Study of Aging. Longitudinal effects of aging on serum total and free testosterone levels in healthy menJ Clin Endocrinol Metab20018672473111158037
- DingELSongYMalikVSLiuSSex differences of endogenous sex hormones and risk of type 2 diabetes: a systematic review and meta-analysisJAMA20062951288129916537739
- LaughlinGABarrett-ConnorEBergstromJLow serum testosterone and mortality in older menJ Clin Endocrinol Metab200893687517911176
- LaaksonenDENiskanenLPunnonenKTestosterone and sex hormone binding globulin predict the metabolic syndrome and diabetes in middle-aged menDiabetes Care2004271036104115111517
- KhawKTDowsettMFolkerdEEndogenous testosterone and mortality due to all causes, cardiovascular disease, and cancer in men: European prospective investigation into cancer in Norfolk (EPIC-Norfolk) Prospective Population StudyCirculation20074116232694270118040028
- ShoresMMMatsumotoAMSloanKLKivlahanDRLow serum testosterone and mortality in male veteransArch Intern Med20061661660166516908801
- AraujoAKupelianVPageSTHandelsmanDJBremnerWJMcKinlayJBSex steroids and all-cause mortality and cause-specific mortality in menArch Intern Med20071671252126017592098
- LindemanRDYauCLBaumgartnerRNMorleyJEGarryPJNew Mexico Aging Process Study. Longitudinal study of fasting serum glucose concentrations in healthy elderly. The New Mexico Aging Process StudyJ Nutr Health Aging20037317217712766795
- VermeulenAAndrogen replacement therapy in the aging male – a critical evaluationJ Clin Endocrinol Metab200186238039011397827
- BhasinSBuckwalterJGTestosterone supplementation in older men: a rational idea whose time has not yet comeJ Androl20012271873111545281
- FeldmanHALongcopeCDerbyCAAge trends in the level of serum testosterone and other hormones in middle-aged men: longitudinal results from the Massachusetts Male Aging StudyJ Clin Endocrinol Metab20028758959811836290
- LiuPYBeilinJMeierCNguyenTVCenterJRLeedmanPJAge-related changes in serum testosterone and sex hormone binding globulin in Australian men: longitudinal analyses of two geographically separate regional cohortsJ Clin Endocrinol Metab2007923599360317595245
- OrwollELambertLCMarshallLMTestosterone and estradiol in older menJ Clin Endocrinol Metab2006911336134416368750
- YeapBBAlmeidaOPHydeZIn men older than 70 years, total testosterone remains stable while free testosterone declines with age. The Health in Men StudyEur J Endocrinol200715658559417468195
- KrithivasKYurgalevitchSMMohrBAEvidence that the CAG repeat in the androgen receptor is associated with age related decline in serum androgens levels in menJ Endocrinol199916213714210396030
- ZmudaJMCauleyJAKriskaAGlynnNWGutaiJPKullerLHLongitudinal relation between endogenous testosterone and cardiovascular disease risk factors in middle age men: a 13 year follow-up of former Multiple Risk Factors Intervention Trial participantsAm J Epidemiol199746609617
- GrayAFeldmanHAMcKinlayJBLongcopeCAge, disease, and changing sex hormone levels in middle-aged men: results of the Massachusetts Male Aging StudyJ Clin Endocrinol Metab199173101610251719016
- AraujoABEscheGRKupelianVPrevalence of symptomatic androgen deficiency in menJ Clin Endocrinol Metab2007924241424717698901
- WuFCWTajarAPyeSRHypothalamic–pituitary–testicular axis disruptions in older men are differentially linked to age and modifiable risk factors: The European Male Aging StudyJ Clin Endocrinol Metab2008932737274518270261
- VeldhuisJDAging and hormones of the hypothalamo–pituitary axis: gonadotropic axis in men and somatotropic axes in men and womenAgeing Res Rev2008718920818343203
- KaufmanJMVermeulenAThe decline of androgen levels in elderly men and its clinical and therapeutic implicationsEndocr Rev20052683387615901667
- MoralesASpevackMEmersonLAdding to the controversy: pitfalls in the diagnosis of testosterone deficiency syndromes with questionnaires and biochemistryAging Male200710576517558969
- BhasinSCunninghamGRHayesFJTestosterone therapy in adult men with androgen deficiency syndromes: an endocrine society clinical practice guidelineJ Clin Endocrinol Metab2006911995201016720669
- SchiaviRCSchreiner-EngelPWhiteDMandeliJThe relationship between pituitary-gonadal function and sexual behavior in healthy aging menPsychosom Med1991533633741924649
- TravisonTGMorleyJEAraujoABO’DonnellABMcKinlayJBThe relationship between libido and testosterone levels in aging menJ Clin Endocrinol Metab2006912509251316670164
- MorleyJEKimMJHarenMTKevorkianRBanksWAFrailty and the aging maleAging Male2005813514016390735
- BaumNCandaceACrespiCATestosterone replacement in elderly men. Testosterone replacement in elderly menGeriatrics2007621518
- ShoresMMMoceriVMSloanKLMatsumotoAMKivlahanDRLow testosterone levels predict incident depressive illness in older men: effects of age and medical morbidityJ Clin Pyschiatry200566714
- LunenfeldBSaadFHoeslCEISA, ISSAM and EAU recommendations for the investigation, treatment and monitoring of late-onset hypogonadism in males: scientific background and rationaleAging Male20058597416096160
- MorleyJEBaumgartnerRNRoubenoffRMayerJNairKSSarcopeniaJ Lab Clin Med200113723124311283518
- ZitzmannMFaberSNieschlagEAssociation of specific symptoms and metabolic risks with serum testosterone in older menJ Clin Endocrinol Metab2006914335434316926258
- MorleyJECharltonEPatrickPValidation of a screening questionnaire for androgen deficiency in aging malesMetabolism2000491239124211016912
- MorleyJEPerryHMIIIKevorkianRTPatrickPComparison of screening questionnaires for the diagnosis of hypogonadismMaturitas20065342442916140484
- HeinemannLASaadFHeinemannKThaiDMCan results of the Aging Males’ Symptoms (AMS) scale predict those of screening scales for androgen deficiencyAging Male2004721121815669540
- MooreCHueblerDZimmermannTHeinemannLASaadFThaiDMThe Aging Males’ Symptoms scale (AMS) as outcome measure for treatment of androgen deficiencyEur Urol200446808715183551
- T’SjoenGGoemaereSDe MeyereMKaufmanJMPerception of males’ aging symptoms, health and well-being in elderly community-dwelling men is not related to circulating androgen levelsPsychoneuroendocrinology20042920121414604601
- KelleherSConwayAJHandelsmanDJBlood testosterone threshold for androgen deficiency symptomsJ Clin Endocrinol Metab2004893813381715292310
- IsidoriAMGiannettaEGianfrilliDEffects of testosterone on sexual function in men: results of a meta-analysisClin Endocrinol200563601602
- MorleyJEMelmedSGonadal dysfunction in systematic disordersMetabolism19792810511073386028
- MatsumotoAMAndropause: Clinical implications of the decline in serum testosterone levels with aging in menJ Gerontol Med Sci2002577699
- DiverMJImtiazKEAhmadAMVoraJPFraserWDDiurnal rhythms of serum total, free and bioavailable testosterone and of SHBG in middle-aged men compared with those in young menClin Endocrinol (Oxf)20035871071712780747
- WangCNieschlagESwerdloffRInvestigation, treatment and monitoring of late-onset hypogonadism in males: ISA, ISSAM, EAU, EAA and ASA recommendationsEur J Endocrinol200815950751418955511
- CitronJTEttingerBRubinoffHPrevalence of hypothalamic-pituitary imaging abnormalities in impotent men with secondary hypogonadismJ Urol19961555295338558653
- BunchTJAbrahamDWangSMeikleAWPituitary radiographic abnormalities and clinical correlates of hypogonadism in elderly males presenting with erectile dysfunctionAging Male20025384612040974
- RhodenELEstradaCLevineLMorgentalerAThe value of pituitary magnetic resonance imaging in men with hypogonadismJ Urol200317079579812913700
- BuvatJLemaireAEndocrine screening in 1, 022 men with erectile dysfunction clinical significance and cost effective strategyJ Urol1997158176417679334596
- AraujoABO’DonnellABrambillaDJPrevalence and incidence of androgen deficiency in middle-aged and older men: estimates from the Massachusetts Male Aging StudyJ Clin Endocrinol Metab2004895920592615579737
- VermeulenAHormonal cut-offs of partial androgen deficiency: a survey of androgen assaysJ Endocrinol Invest200528283116042357
- van den BeldAWde JongFHGrobbeeDEPolsHALambertsSWMeasures of bioavailable serum testosterone and estradiol and their relationships with muscle strength, bone density, and body composition in elderly menJ Clin Endocrinol Metab2000853276328210999822
- RosnerWAuchusRJAzzizRSlussPMRaffHUtility, limitations, and pitfalls in measuring testosterone: an Endocrine Society position statementJ Clin Endocrinol Metab2007924051317090633
- VermeulenAVerdonckLKaufmanJMA critical evaluation of simple methods for the estimation of free testosterone in serumJ Clin Endocrinol Metab1999843666367210523012
- WangCPlymateSNieschlagEPaulsenCASalivary testosterone in men: further evidence of a direct correlation with free serum testosteroneJ Clin Endocrinol Metab198153102110247197285
- MorleyJEPerryHMIIIPatrickPDollbaumCMKellsJMValidation of salivary testosterone as a screening test for male hypogonadismAging Male2006916516917050116
- GonacharovNKatsyaGDobrachevaANizhnikAKolesnikovaGHerbstVWestermannJDiagnostic significance of free salivary testosterone measurement using a direct luminescence immunoassay in healthy men and in patients with disorders of androgenic statusAging Male2006911112216916746
- CalofOMSinghABLeeMLAdverse events associated with testosterone replacement in middle-aged and older men: a meta-analysis of randomized, placebo-controlled trialsJ Gerontol A Biol Sci Med Sci2005601451145716339333
- ParsonsJKCarterHBPlatzEAWrightEJLandisPMetterEJSerum testosterone and the risk of prostate cancer: potential implications for testosterone therapyCancer Epidemiol Biomarkers Prev2005142257226016172240
- ZitzmannMNieschlagEAndrogen receptor gene CAG repeat length and body mass index modulate the safety of long-term intramuscular testosterone undecanoate therapy in hypogonadal menJ Clin Endocrinol Metab2007923844385317635942
- VelazquezIAlterBPAndrogens and liver tumors: Fanconi’s anemia and non-Fanconi’s conditionsAm J Hematol200477325726715495253
- ImamotoTSuzukiHFukasawaSPretreatment serum testosterone level as a predictive factor of pathological stage in localized prostate cancer patients treated with radical prostatectomyEurUrol200547308312
- McClureRDOsesRErnestMLHypogonadal impotence treated by transdermal testosteroneUrology19913732242000678
- BhasinSBremnerWJEmerging issues in androgen replacement therapyJ Clin Endocrinol Metab199782388989221
- ComhaireFHAndropause: hormone replacement therapy in the aging maleEurUrol200038655662
- Von EckardsteinNieschlagETreatment of male hypogonadism with testosterone undecanoate injected at extended intervals of 12 weeks: a phase II studyJ Androl200223341942512002444
- WangCSwerdloffRSIranmaneshATransdermal testosterone gel improves sexual function, mood, muscle strength, and body composition parameters in hypogonadal menJ Clin Endocrinol Metab2000852839285310946892
- YuZGuptaSKHwangSSTestosterone pharmacokinetics after application of an investigational transdermal system in hypogonadal menJ Clin Pharmacol199737113911459506009
- KimMKZhaoHLeeCHKimDDFormulation of a reservoir-type testosterone transdermal delivery systemInt J Pharm20012191–2515911337165
- McNicholasTADeanJDMulderHCarnegieCJonesNAA novel testosterone gel formulation normalizes androgen levels in hypogonadal men, with improvements in body composition and sexual functionBJU Int200391697412614254
- SalehianBWangCAlexanderGPharmacokinetics, bioefficacy, and safety of sublingual testosterone cyclodextrin in hypogonadal men: comparison to testosterone enanthate – a clinical research center studyJ Clin Endocrinol Metab199580356735758530600
- KorbonitsMSlawikMCullenDRossRJA comparison of a novel testosterone bioadhesive buccal system, striant, with a testosterone adhesive patch in hypogonadal malesJ Clin Endocrinol Metab2004892039204315126518
- RossCNFrenchJAPateraKJIntensity of aggressive interactions modulates testosterone in male marmosetsPhysiol Behav200483343744515581666
- WangCSwerdloffRKipnesMMatsumotoAMNew testosterone buccal system (Striant) delivers physiological testosterone levels: pharmacokinetics study in hypogonadal menJ Clin Endocrinol Metab2004893821382915292312
- JockenhovelFVogelEKreutzerMReinhardtWLederbogenSReinweinDPharmacokinetics and pharmacodynamics of subcutaneous testosterone implants in hypogonadal menClin Endocrinol1996456171
- KelleherSConwayAJHandelsmanDJInfluence of implantation site and track geometry on the extrusion rate and pharmacology of testosterone implantsClin Endocrinol200155531536
- HandelsmanDJClinical pharmacology of testosterone pellet implantsNieschlagEBehreHMTestosterone action deficiency substitution2nd edBerlinSpringer-Verlag1998349364
- LyngdorfPHemmingsenLEpidemiology of erectile dysfunction and its risk factors: a practice-based study in DenmarkInt J Impot Res20041610511114973529
- SelvinEBurnettALPlatzEAPrevalence and risk factors for erectile dysfunction in the USAm J Med200712015115717275456
- SchiaviRCSchreiner-EngelPWhiteDMandeliJPituitary-gonadal function during sleep in men with hypoactive sexual desire and in normal controlsPsychosomat Med198850304318
- NilssonPMollerLSolkadKAdverse effects of psychosocial stress on gonadal function and insulin levels in middle aged malesJ Intern Med19952374794867738488
- SchiaviRCRehmanJSexuality and agingUrol Clin North Am1995227117267483124
- GrayPBSinghABWoodhouseLJDose-dependent effects of testosterone on sexual function, mood, and visuospatial cognition in older menJ Clin Endocrinol Metab2005903838384615827094
- MoralesABuvatJGoorenLJEndocrine aspects of sexual dysfunction in menJ Sex Med20041698116422986
- YassinAASaadFDramatic improvement of penile venous leakage upon testosterone administration. A case report and review of literatureAndrologia200638343716420241
- LivermanCTBlazerDGTestosterone and aging: clinical research directionsWashington, DCInstitute of Medicine. The National Academies Press2004
- KrauseWMuellerUMazurATestosterone supplementation in the aging male: which questions have been answered?Aging Male20058313816106921
- HajjarRRKaiserFEMorleyJEOutcomes of long-term testosterone replacement in older hypogonadal males: a retrospective analysisJ Clin Endocrinol Metab19978237939360543
- ShabsighRThe effects of testosterone on the cavernous tissue and erectile functionWorld J Urol19971521269066090
- MorleyJEPerryHMKaiserFEEffect of testosterone replacement therapy in old hypogonadal males: a preliminary studyJ Am Geriatr Soc1993411491528426037
- CavalliniGCaraccioloSVitaliGModeniniFBiagiottiGCarnitine versus androgen administration in the treatment of sexual dysfunction, depressed mood, and fatigue associated with male agingUrology20046364164615072869
- SnyderPJPeacheyHHannoushPBerlinJALohLLenrowDAEffect of testosterone treatment on body composition and muscle strength in men over 65 years of ageJ Clin Endocrinol Metab1999842647265310443654
- MeikleAWArverSDobsASSandersSWMazerNAAndroderm: A permeation-enhanced, non-scrotal testosterone transdermal system for the treatment of male hypogonadismBhasinPharmacology, biology, and clinical applications of androgensNew York, NYWiley Liss, Inc1996449457
- CoronaGPetroneLFisherADMansaniRBandiniESix-month administration of 1% testosterone gel is able to restore erectile function in hypogonadal patients with erectile dysfunctionArch Ital Urol Androl200880310310819009866
- BlackAMDayAGMoralesAThe reliability of clinical and biochemical assessment in symptomatic late-onset hypogonadism: Can a case be made for a 3-month therapeutic trial?BJU Int2004941066107015541129
- ShabsighRKaufmanJMSteidleCPadma-NathanHRandomized study of testosterone gel as adjunctive therapy to sildenafil in hypogonadal men with erectile dysfunction who do not respond to sildenafil aloneJ Urol200417265866315247755
- GreensteinAMabjeeshNJSoferMKaverIMatzkinHChenJDoes sildenafil combined with testosterone gel improve erectile dysfunction in hypogonadal men in whom testosterone supplement therapy alone failed?J Urol200517353053215643239
- BehreHMTestosterone and erectionNieschlagEBehreHMTestosterone: action, deficiency, substitutionCambridgeCambridge University Press2004333346
- KalintchenkoSYKozlovGIGontcharovNPOral testosterone undecanoate reverses erectile dysfunction associated with diabetes mellitus in patients failing on sildenafil citrate therapy aloneAging Male20036949912898793
- GrecoEASperaGAversaACombining testosterone and PDE5 inhibitors in erectile dysfunction: basic rationale and clinical evidencesEur Urol20065094094716979814
- AversaAIsidoriAMGrecoEAGiannettaEGianfrilliDSperaEHormonal supplementation and erectile dysfunctionEur Urol20044553553815082192
- MinerMCantyDJShabsighRTestosterone replacement therapyPostgrad Med2008120313015318824832
- KarazindiyanoğluSCayanSThe effect of testosterone therapy on lower urinary tract symptoms/bladder and sexual functions in men with symptomatic late-onset hypogonadismAging Male200811314614918821291
- FairfieldWPFinkelsteinJSKlibanskiAGrinspoonSKOsteopenia in eugonadal men with acquired immune deficiency syndrome wasting syndromeJ Clin Endocrinol Metab2001862020202611344201
- MeierCNguyenTVHandelsmanDJEndogenous sex hormones and incident fracture risk in older men: the Dubbo Osteoporosis Epidemiology StudyArch Intern Med2008168475418195195
- KennyAMPrestwoodKMMarcelloKMRaiszLGDeterminants of bone density in healthy older men with low testosterone levelsJ Gerontol A Biol Sci Med Sci200055M492M49710995046
- FinkHAEwingSKEnsrudKEAssociation of testosterone and estradiol deficiency with osteoporosis and rapid bone loss in older menJ Clin Endocrinol Metab2006911039083901516849417
- CompstonJESex steroids and bonePhysiol Rev200181141944711152762
- AmoryJKWattsNBEasleyKAExogenous testosterone or testosterone with finasteride increases bone mineral density in older men with low serum testosteroneJ Clin Endocrinol Metab20048950351014764753
- SvartbergJAgledahlIFigenschauYSildnesTWaterlooKJordeRTestosterone treatment in elderly men with subnormal testosterone levels improves body composition and BMD in the hipInt J Impot Res200820437838718480825
- BehreHHKlieschSLeifkeELinkTMNieschlagELong term effect of testosterone therapy on bone mineral density in hypogonadal menJ Clin Endocrinol Metab199782238623909253305
- SaggeseGBertelloniSBaroncelliGISex steroids and acquisition of bone massHorm Res19974865729434047
- CenterJRNguyenTVSambrookPNEismanJAHormonal and biochemical parameters in the determination of osteoporosis in elderly menJ Clin Endocrinol Metab1999843626363510523006
- HolzbeierleinJMCastleEThrasherJBComplications of androgen deprivation therapy: prevention and treatmentOncology (Williston Park)200418330330915065701
- Van den BeldAWde JongFHGrobbeeDEPolsHALambertsSWMeasures of bioavailable serum testosterone and estradiol and their relationships with muscle strength, bone density, and body composition in elderly menJ Clin Endocrinol Metab20008593276328210999822
- MichaelHHärkönenPLVäänänenHKHentunenTAEstrogen and testosterone use different cellular pathways to inhibit osteoclastogenesis and bone resorptionJ Bone Miner Res200520122224223216294275
- TenoverJSEffects of testosterone supplementation in the aging maleJ Clin Endocrinol Metab199275109210981400877
- FreitasSSBarrett-ConnorEEnsrudKERate and circumstances of clinical vertebral fractures in older menOsteoporos Int20081961562318038109
- SchousboeJTTaylorBCFinkHACost-effectiveness of bone densitometry followed by treatment of osteoporosis in older menJAMA200729862963717684185
- KennyAMPrestwoodKMGrumanCAMarcelloKMRaiszLGEffects of transdermal testosterone on bone and muscle in older men with low bioavailable testosterone levelsJ Gerontol A Biol Sci Med Sci200156266272
- De RosaMPaesanoLNuzzoVBone mineral density and bone markers in hypogonadotropic and hypergonadotropic hypogonadal men after prolonged testosterone treatmentJ Endocrinol Invest200124424625211383911
- BehreHMKlieschSLeifkeELinkTMNieschlagELong-term effect of testosterone therapy on bone mineral density in hypogonadal menJ Clin Endocrinol Metab19978223869253305
- LeifkeEKornerHCLinkTMBehreHMPetersPENieschlagEEffects of testosterone replacement on cortical and trabecular bone mineral density, vertebral body area and paraspinal muscle area in hypogonadal menEur J Endocrinol1991385158
- MichalJTraczSiderasKBolonERAClinical review: testosterone use in men and its effects on bone health. A systematic review and meta-analysis of randomized placebo-controlled trialsJ Clin Endocrinol Metab9162011201616720668
- AndersonFHFrancisRMFaulknerKAndrogen supplementation in eugonadal men with osteoporosis. Effects of 6 months of treatment on bone mineral density and cardiovascular risk factorsBone1996181711788833211
- AmoryJKWattsNBEasleyKAExogenous testosterone or testosterone with finasteride increases bone mineral density in older men with low serum testosteroneJ Clin Endocrniol Metab200489503510
- BhasinSregulation of body composition by androgensJ Endocrinol Invest200326981482214964432
- FronteraWRHughesVVFiataroneMAFieldingRAAging and skeletal muscle: a 12 year longitudinal studyJ Appl Physiol2000881321132610749826
- ReedRLPearlmutterLJochumKMeredithKEMooradianADThe relationship between muscle mass and muscle strength in the elderlyJ Am Geriatr Soc1991395555911805811
- MaurasNHayesVWelchSTestosterone deficiency in young men; marked alterations in whole body protein kinetics, strength, and adiposityJ Clin Endocrinol Metab199838618861892
- BaumgartnerRNWatersDLGallagherDMorleyJEGarryPJPredictors of skeletal muscle mass in elderly men and womenMech Ageing Dev199910712313610220041
- VerhaarHJJSamsonMMAlemanAde VriesWRde VreedePLKoppeschaarHPFThe relationship between indices of muscle function and circulating anabolic hormones in healthyAging Male200037580
- MudaliSDobsASEffects of testosterone on body composition of the aging maleMech Ageing Dev2004125429730415063106
- FerrandoAASheffield-MooreMPaddon-JonesDWolfeRRUrbanRJDifferential anabolic effects of testosterone and amino acid feeding in older menJ Clin Endocrinol Metab20038835836212519877
- PageSTAmoryJKBowmanFDExogenous testosterone (T) alone or with finasteride increases physical performance, grip strength, and lean body mass in older men with low serum TJ Clin Endocrinol Metab2005901502151015572415
- HarmanSMBlackmanMRThe effects of growth hormone and sex steroid on lean body mass, fat mass, muscle strength, cardiovascular endurance and adverse events in healthy elderly women and menHorm Res200360121124
- TenoverJSAndrogen administration in aging menEndocrinol Metab Clin199423877889
- UrbanRJBodenburgCGilkisonCTestosterone administration to elderly men increases skeletal muscle strength and protein synthesisAm J Physiol1995269E820E8267491931
- SihRMorleyJEKaiserFEPerryHMIIIPatrickPRossCTestosterone replacement in older hypogonadal men: a 12 months randomized controlled studyJ Clin Endocrinol Metab199782166116679177359
- MorleyJEPerryHM3rdKaiserFEEffects of testosterone replacement therapy in old hypogonadal males: a preliminary studyJ Am Geriatr Soc1993411491528426037
- PerryHMMillerDKPatrickPTestosterone and leptin in older African-American men: relationship to age, strength, function, and seasonMetabolism2000491085109110954031
- BreuerBTrungoldSMartucciCRelationship of sex hormone levels to dependence of daily living in the frail elderlyMaturitas20013914715911514113
- BhasinSTestosterone supplementation for aging-associated sarcopeniaJ Gerontol A Biol Sci Med Sci200358111002100814630881
- SteidleCSchwartzSJacobyKAA2500 testosterone gel normalizes androgen levels in aging males with improvements in body composition and sexual functionJ Clin Endocrinol Metab2003882673268112788872
- WangCCunninghamGDobsALong-term testosterone gel (AndroGel) treatment maintains beneficial effects on sexual function and mood, lean and fat mass, and bone mineral density in hypogonadal menJ Clin Endocrinol Metab2004892085209815126525
- Barrett-ConnorEVon MuhlenDGKritz-SilversteinDBioavailable testosterone and depressed mood in older men: the Rancho Bernardo StudyJ Clin Endocrinol Metab19998457357710022418
- SchmidtPJBerlinKLDanaceauMAThe effects of pharmacologically induced hypogonadism on mood in healthy menArch Gen Psychiatry200461997100415466673
- BoothAJohnsonDRGrangerDATestosterone and men’s depression: the role of social behaviorJ Health Soc Behav19994013014010467760
- KratzikCWSchatzlGLacknerJEMood changes, body mass index and bioavailable testosterone in healthy men: results of the Androx Vienna Municipality StudyBJU Int200710061461817550413
- SeidmanSNSpatzERizzoCRooseSPTestosterone replacement therapy for hypogonadal men with major depressive disorder: a randomized, placebo-controlled clinical trialJ Clin Psychiatry200162640641211465516
- EnglishKMSteedsRPJonesTHDiverMJChannerKSLow-dose transdermal testosterone therapy improves angina threshold in men with chronic stable angina: a randomized, double-blind, placebo-controlled studyCirculation20001021906191111034937
- ReddyPWhiteCMDunnABMoynaNMThompsonPDThe effect of testosterone on health-related quality of life in elderly males: a pilot studyJ Clin Pharm Ther20002542142611123495
- TrickerRCasaburiRStorerTWThe effects of supraphysiological doses of testosterone on angry behavior in healthy eugonadal men: a clinical research center studyJ Clin Endocrinol Metab199681375437588855834
- HarenMTWittertGAChapmanIMEffect of oral testosterone undecanoate on visuospatial cognition, mood and quality of life in elderly men with low–normal gonadal statusMaturitas20055012413315653010
- PopeHGJKouriEMHudsonJIEffects of supraphysiologic doses of testosterone on mood and aggression in normal men. A randomized controlled trialArch Gen Psychiatry20005713314010665615
- SuTPPagliaroMSchmidtPJNeuropsychiatric effects of anabolic steroids in male normal volunteersJAMA1993269276027648492402
- WangCWAlexanderGBermanNTestosterone replacement therapy improves mood in hypogonadal menóa clinical research center studyJ Clin Endocrinol Metab19968135788855804
- LunenfeldBNieschlagETestosterone therapy in the aging maleAging Male20071013915317701658
- MorleyJETestosterone replacement in older men and womenJ Gend Specif Med20014495311480098
- GruenewaldDAMatsumotoAMTestosterone supplementation therapy for older men: potential benefits and risksJ Am Geriatr Soc20035110111512534854
- EhrenreichHHalarisARuetherEPsychoendocrine sequelae of chronic testosterone deficiencyJ Psychiatr Res199933b379387
- HeuserIHartmannAOertelHAndrogen replacement in a 48, XXYY-male patientArch Gen Psychiatry19995619419510025446
- SeidmanSNRabkinJGTestosterone replacement therapy for hypogonadal men with SSRI-refractory depressionJ Affect Disord1998482–31571619543205
- OrengoCAFullertonLKunikMESafety and efficacy of testosterone gel 1% augmentation in depressed men with partial response to antidepressant therapyJ Geriatr Psychiatry Neurol200518202415681624
- RabkinJGWagnerGJRabkinRTestosterone therapy for HIV+ men with and without clinical hypogonadismJ Clin Psychopharmacol19991919279934939
- GrinspoonSCorcoranCStanleyTEffects of hypogonadism and testosterone administration on depression indices in HIV-infected menJ Clin Endocrinol Metab200085606510634364
- SeidmanSNMiyazakiMRooseSPIntramuscular testosterone supplementation to selective serotonin reuptake inhibitor in treatment-resistant depressed men: randomized placebo-controlled clinical trialJ Clin Psychopharmacol20052558458816282843
- PerryPJYatesWRWilliamsRDTestosterone therapy in late-life major depression in malesJ Clin Psychiatry2002631096110112523867
- SeidmanSNAraujoABRooseSPMcKinlayJBTestosterone level, androgen receptor polymorphism, and depressive symptoms in middle-aged menBiol Psychiatry20015037137611543741
- HarkonenKHuhtaniemiIMakinenJThe polymorphic androgen receptor gene CAG repeat, pituitary-testicular function and andropausal symptoms in ageing menInt J Androl20032618719412755998
- AmiazRASeidmanSNStuartNBTestosterone and depression in menCurr Opin Endocrinol Diabetes Obes200815327828318438177
- ShamlianNTColeMGAndrogen treatment of depressive symptoms in older men: a systematic review of feasibility and effectivenessCan J Psychiatry20065129529916986819
- KanayamaGAmiazRSeidmanSNPopeHGJTestosterone supplementation for depressed men: current research and suggested treatment guidelinesExp Clin Psychopharmacol20071552953818179305
- GillettMJMartinsRNClarnetteRMChubbSABruceDGYeapBBRelationship between testosterone, sex hormone binding globulin and plasma amyloid beta peptide 40 in older men with subjective memory loss or dementiaJ Alzheimers Dis2003526726914624021
- MorleyJEKaiserFRaumWJPotentially predictive and manipulable blood serum correlates of aging in the healthy human male: progressive decreases in bioavailable testosterone, dehydroepiandrosterone sulfate, and the ratio of insulin-like growth factor 1 to growth hormoneProc Natl Acad Sci U S A199794753775429207127
- MoffatSDZondermanABMetterEJKawasCBlackmanMRHarmanSMFree testosterone and risk for Alzheimer disease in older menNeurology20046218819314745052
- HogervorstEBandelowSCombrinckMSmithADLow free testosterone is an independent risk factor for Alzheimer’s diseaseExp Gerontol2004391633163915582279
- McKeeverWFDeyoATestosterone, dihydrotestosterone and spatial task performance of malesBull Psychonomic Soc199028305308
- Barrett-ConnorEGoodman-GruenDPatayBEndogenous sex hormones and cognitive function in older menJ Clin Endocrinol Metab1999843681368510523014
- YaffeKLuiL-YZmudaJCauleyJSex hormones and cognitive function in older menJ Am Geriatr Soc20025070771211982672
- ThilersPPMacDonaldSWSHerlitzAThe association between endogenous free testosterone and cognitive performance: a population-based study in 35–90 year-old men and womenPsychoneuroendocrinology20063156557616487665
- YeapBBAlmeidaOPHydeZChubbSAPHankeyGJJamrozikKHigher serum free testosterone is associated with better cognitive function in older men, whilst total testosterone is not. The Health In Men StudyClin Endocrinol200868404412
- FondaSJBertrandRO’DonnellALongcopeCMcKinlayJBAge, hormones, and cognitive functioning among middle aged and elderly men: cross-sectional evidence from the Massachusetts Male Aging StudyJ Gerontol A Biol Sci Med Sci20056038539015860479
- YonkerJEErikssonENilssonL-GHerlitzANegative association of testosterone on spatial visualisation in 35 to 80 year old menCortex20064237638616771043
- MartinDMWittertGBurnsNRHarenMTSugarmanRTestosterone and cognitive function in ageing men: data from the Florey Adelaide Male Ageing Study (FAMAS)Maturitas20075718219417287097
- BurkhardtMSFosterJKClarnetteRMChubbSAPBruceDGDrummondPDInteraction between testosterone and apolipoprotein E e4 status on cognition in healthy older menJ Clin Endocrinol Metab2006911168117216368754
- ChuLWTamSLeePWBioavailable testosterone is associated with a reduced risk of amnestic mild cognitive impairment in older menClin Endocrinol (Oxf)200868458959817973937
- CherrierMMRoseALHiganoCThe effects of combined androgen blockade on cognitive function during the first cycle of intermittent androgen suppression in patients with prostate cancerJ Urol20031701808181114532781
- SalminenEKPortinRIKoskinenAHeleniusHNurmiMAssociations between serum testosterone fall and cognitive function in prostate cancer patientsClin Cancer Res2004107575758215569988
- AlmeidaOPWaterreusASpryNFlickerLMartinsRNOne year follow-up study of the association between chemical castration, sex hormones, beta-amyloid, memory and depression in menPsychoneuroendocrinology20042981071108115219659
- HogervorstEWilliamsJBudgeMBarnetsonLCombrinckMSmithADSerum total testosterone is lower in men with Alzheimer’s diseaseNeuro Endocrinol Lett200122316316811449190
- BowenRLIsleyJPAtkinsonRLAn association of elevated serum gonadotropin concentrations and Alzheimer disease?J Neuroendocrinol200012435135410718932
- GibbsRBGaborREstrogen and cognition: applying preclinical findings to clinical perspectivesJ Neurosci Res200374563764314635215
- BeauchetOTestosterone and cognitive function: current clinical evidence of a relationshipEur J Endocrinol200615577378117132744
- OrwollESOviattSKBiddleJTransdermal testosterone supplementation in normal older menProc 74th Meeting of The Endocrine SocSan Antonio, TX1992319
- AlexanderGMSwerdloffRSWangCAndrogen-behavior correlations in hypogonadal men and eugonadal menHorm Behav19983385949647934
- JanowskiSCOviattSKOrwollESTestosterone influences spatial cognition in older menBehav Neurosci19941083253328037876
- JanowskyJSChavezBJOrwollESex steroids modify working memoryCogn Neurosci200012407414
- CherrierMMCraftSMatsumotoAHCognitive changes associated with supplementation of testosterone or dihydrotestosterone in mildly hypogonadal men: a preliminary reportJ Androl20032456857612826696
- CherrierMMMatsumotoAMAmoryJKAsthanaSBremnerWPeskindERTestosterone improves spatial memory in men with Alzheimer disease and mild cognitive impairmentNeurology2005642063206815985573
- LuPHMastermanDAMulnardRCotmanCMillerBYaffeKEffects of testosterone on cognition and mood in male patients with mild Alzheimer disease and healthy elderly menArch Neurol20066317718516344336
- MakiPMErnstMLondonEDMordecaiKLPerschlerPDursoSCIntramuscular testosterone treatment in elderly men: evidence of memory decline and altered brain functionJ Clin Endocrinol Metab2007924107411417726086
- TanRSCulbersonJWAn integrative review on current evidence of testosterone replacement therapyfor the andropauseMaturitas200345152712753940
- KennyAMFabregasGSongCBiskupBBellantonioSEffects of testosterone on behavior, depression, and cognitive function in older men with mild cognitive lossJ Gerontol A Biol Sci Med Sci200459757814718489
- van den BeldAWBotsMLJanssenJAPolsHALambertsSWGrobbeeDEEndogenous hormones and carotid atherosclerosis in elderly menAm J Epidemiol2003157253112505887
- MakinenJJarvisaloMJPollanenPPerheentupaAIrjalaKKoskenvuoMIncreased carotid atherosclerosis in andropausal middle-aged menJ Am Coll Cardiol2005451603160815893174
- MullerMvan den BeldAWBotsMLGrobbeeDELambertsSWvander SchouwYTEndogenous sex hormones and progression of carotid atherosclerosis in elderly menCirculation20041092074207915096452
- TivestenAMellstromDJutbergerHFagerbergBLernfeltBOrwollELow serum testosterone and high serum estradiol associate with lower extremity peripheral arterial disease in elderly men. The MrOS Study in SwedenJ Am Coll Cardiol2007501070107617825717
- HakAEWittemanJCMde JongFHGeerlingsMIHofmanAPolsHAPLow levels of endogenous androgens increase the risk of atherosclerosis in elderly men: the Rotterdam studyJ Clin Endocrinol Metab2002873632363912161487
- KapoorDClarkeSChannerKSJonesTHErectile dysfunction is associated with low bioactive testosterone levels and visceral adiposity in men with type 2 diabetesInt J Androl20073050050718028199
- MaRC-WSoW-YYangXYuLW-LKongAP-SKoGT-CErectile dysfunction predicts coronary heart disease in type 2 diabetesJ Am Coll Cardiol2008512045205018498959
- VermeulenAKaufmanJMGiagulliVAInfluence of some biological indices on the sex hormone binding globulin and androgens in aging and obese menJ Clin Endocrinol Metab199681182118278626841
- ZumoffBStrainGWMillerLKPlasma free and non sex-hormone-binding-globulin-bound testosterone are decreased in obese men in proportion to their degree of obesityJ Clin Endocrinol Metab1990719299312401718
- PasqualiRCasimirriFCantobelliSEffect of obesity and body fat distribution on sex hormones and insulin in menMetabolism1991401011041984562
- KalyaniRRDobsASAndrogen deficiency, diabetes, and the metabolic syndrome in menCurr Opin Endocrinol Diabetes Obes20071422623417940444
- SelvinEFeinleibMZhangLAndrogens and diabetes in men: results from the Third National Health and Nutrition Examination Survey (NHANES III)Diabetes Care20073023423817259487
- HaffnerSMValdezRASternMPObesity, body fat distribution and sex hormones in menInt J Obes199317634639
- PhillipsGBRelationships in men of sex hormones, insulin, adiposity, and risk factors for myocardial infarctionMetabolism20035278479012800107
- CohenPGThe hypogonadal-obesity cycleMed Hypotheses199952495110342671
- JonesTHTestosterone associations with erectile dysfunction, diabetes and the metabolic syndromeEur Urol (Suppl)20076847857
- ErFMichelsGGassanovNRiveroFHoppeUCTestosterone induces cytoprotection by activating ATPsensitive Kþ channels in the cardiac mitochondrial inner membraneCirculation20041103100310715520315
- NettleshipJEJonesTHChannerKSJonesRDPhysiological testosterone replacement therapy attenuates fatty streak formation and improves high-density lipoprotein cholesterol in the Tfm mouseCirculation20071162427243417984376
- KalmeTSeppalaMQiaoQSex hormone-binding globulin and insulin-like growth factor-binding protein-1 as indicators of metabolic syndrome, cardiovascular risk, and mortality in elderly menJ Clin Endocrinol Metab2005901550155615613437
- KupelianVPageSTAraujoABLow sex hormone-binding globulin, total testosterone, and symptomatic androgen deficiency are associated with development of the metabolic syndrome in nonobese menJ Clin Endocrinol Metab20069184385016394089
- DerbyCAZilberSBrambillaDMoralesKHMcKinlayJBBody mass index, waist circumference and waist to hip ratio and change in sex steroid hormones: the Massachusetts Male Ageing StudyClin Endocrinol (Oxf)20066512513116817831
- RodriguezAMullerDCMetterEJAging, androgens, and the metabolic syndrome in a longitudinal study of agingJ Clin Endocrinol Metab2007923568357217595254
- SimonDPreziosiPBarrett-ConnorEInterrelation between plasma testosterone and plasma insulin in healthy adult men: the Telecom StudyDiabetologia1992351731771547923
- Barrett-ConnorEKhawKTEndogenous sex hormones and cardiovascular disease in men: a prospective population-based studyCirculation1988785395453409497
- PitteloudNMoothaVKDwyerAARelationship between testosterone levels, insulin sensitivity, and mitochondrial function in menDiabetes Care2005281636164215983313
- MünzerTHarmanSMChristmasCEffects of administration of testosterone and/or GH in healthy aged men [abstract]Presented at 2nd World Congress on the Aging MaleGeneva, Switzeland2000Aging Male200033
- AbateNHaffnerSMGargASex steroid hormones, upper body obesity and insulin resistanceJ Clin Endocrinol Metab2002874522452712364429
- KapoorDGoodwinEChannerKSJonesTHTestosterone replacement therapy improves insulin resistance, glycaemic control, visceral adiposity and hypercholesterolaemia in hypogonadal men with type 2 diabetesEur J Endocrinol200615489990616728551
- CorralesJJBurgoRMGarca-BerrocalBPartial androgen deficiency in aging type 2 diabetic men and its relationship to glycemic controlMetabolism20045366667215131775
- BasuRDallaMCCampioniMEffect of 2 years of testosterone replacement on insulin secretion, insulin action, glucose effectiveness, hepatic insulin clearance, and postprandial glucose turnover in elderly menDiabetes Care2007301972197817496236
- TenoverJLEffects of androgen supplementation in aging malesOddensBVermeulenAAndrogens and the aging maleNew York, LondonParthenon Publishing Group1996191204
- HaffnerJMAndrogens in relation to cardiovascular disease and insulin resistance in aging menOddensBVermeulenAAndrogens and the aging maleNew York, LondonParthenon Publishing Group19966584
- MoorjaniSDupontALabrieFIncrease in plasma high density lipoprotein concentration following complete androgen blockade in men with prostatic carcinomaMetabolism1987362442503102895
- WhitselEABoykoEJMatsumotoAMAnawaltBDSiscovickDSIntramuscular testosterone esters and plasma lipids in hypogonadal men: a meta-analysisAm J Med200111126126911566455
- Emmelot-VonkMHVerhaarHJNakhai PourHREffect of testosterone supplementation on functional mobility, cognition, and other parameters in older men: a randomized controlled trialJAMA20082996634
- DobsASMeikleAWArverSSandersSWCaramelliKEMazerNAPharmacokinetics, efficacy, and safety of a permeation enhanced testosterone transdermal system in comparison with bi-weekly injections of testosterone enanthate for the treatment of hypogonadal menJ Clin Endocrinol Metab1999843469347810522982
- MarinPHolmängSGustafsonCAndrogen treatment of abdominally obese menObesity Res19931245248
- MarinPLonnBAnderssonBOdenBOlbeLBengtssonBAAssimilation of triglycerides in subcutaneous and intra-abdominal adipose tissues in vivo in menJ Clin Endocrinol Metab199681101810228772568
- XuXDe PergolaGBjorntorpPTestosterone increases lipolysis and the number ß-adrenoreceptors in male rat adipocytesEndocrinology19911283793811846106
- MarinPOdenBBjörntorpPAssimilation and mobilization of triglycerides in subcutaneous abdominal and femoral adipose tissue in vivo in men: effects of androgensJ Clin Endocrinol Metab1995802392437829619
- ZmudaJMFahrenbachMCYounkinBTThe effect of testosterone aromatization on high-density lipoprotein cholesterol level and postheparin lipolytic activityMetabolism1993424464508487666
- JacobsDRJrMebaneILBangdiwalaSICriquiMHTyrolerHAHigh density lipoprotein cholesterol as a predictor of cardiovascular disease mortality in men and women: the follow-up study of the Lipid Research Clinics Prevalence StudyAm J Epidemiol199013132472293751
- SinghABHsiaSAlaupovicPThe effects of varying doses of T on insulin sensitivity, plasma lipids, apolipoproteins, and C-reactive protein in healthy young menJ Clin Endocrinol Metab20028713614311788637
- PhillipsGPinkernellBHJingTYThe association between hypotestosteronemia and coronary heart disease in menArterioscler Thromb1994147017068172848
- VermeulenAGoemaereSKaufmanJMSex hormones, body composition and agingAging Male19992815
- SeidellJCBjörntorpPSjöströmLKvistHSannerstedtRVisceral fat accumulation in men is positively associated with insulin, glucose and C-peptide levels, but negatively with testosterone levelsMetabolism1990398979012202881
- TchernofALabrieFBelangerARelationships between endogenous sex steroid hormones, sex hormone binding globulin and lipoprotein levels in men: contribution of visceral obesity, insulin levels and other metabolic variablesAtherosclerosis19971332352449298684
- KannellWBCupplesLARamaswamiRStokesJJrKregerBEHiggingsMRegional obesity and the risk of coronary disease: The Framingham StudyJ Clin Epidemiol1991441831901995775
- BjörntorpPVisceral obesity: a civilisation syndromeObes Res1993120622216350574
- KabakciGYildirirACanIUnsalIErbasBRelationship between endogenous sex hormone levels, lipoproteins and coronary atherosclerosis in men undergoing coronary angiographyCardiology19999222122510844380
- HaddadRMKennedyCCCaplesSMTestosterone and cardiovascular risk in men: a systematic review and meta-analysis of randomized placebo-controlled trialsMayo Clin Proc2007821111317285780
- AllanCAMcLachlanRIAge-related changes in testosterone and the role of replacement therapy in older menClin Endocrinol200460653670
- HaffnerJEMossSEKleinBEKKleinRSex hormones and DHEASO4 in relation to ischemic heart disease in diabetic subjects. The WESDR StudyDiabetes Care199619104510508886548
- Barrett-ConnorEKhawKSEndogenous sex hormone levels and cardiovascular disease in men: a prospective population based studyCirculation1988788539543
- CauleyJAGutaiJPKullerLHDaiWSUsefulness of sex steroid hormone levels in predicting coronary artery disease in menAm J Cardiol1987607717773661391
- GoldbergRBRabinANAlexanderANDoelleGCGetzGSSuppression of plasma testosterone leads to an increase in serum total and high density lipoprotein cholesterol and Apo A and BJ Clin Endocrinol Metab1985602032073917267
- CaronPBennetACamareLLouvetJPBoneuSSiePPlasminogen activator inhibitor in plasma is related to testosterone in manMetabolism198938101010132507874
- PoldermanKHStehouwerCDAvan de KampGJDekkerGHVerheugtFWAGoorenLJGInfluence of sex hormones on plasma endothelin levelsAnn Intern Med19931184294318439117
- AjayiAATestosterone increases platelet thromboxane A2 receptor densityCirculation19959127402747
- SpivakJLThe blood in systemic disordersLancet20003551707171210905258
- ZitzmannMNieschlagEAndrogens and erythropoiesisNieschlagEBehreHMTestosterone: action, deficiency, substitutionCambridgeCambridge University Press2004283296
- MarksLSMazerNAMostaghelEEffect of testosterone replacement therapy on prostate tissue in men with late-onset hypogonadism: a randomized controlled trialJAMA2006296192369237117105801
- HolyoakJDCrawfordEDMeachamRBtestosterone and the testosterone: implications for the treatment of hypogonadal menCurr Urol Rep2008950050518947516
- RoddamAWAllenNEApplebyPKeyTJEndogenous sex hormones and prostate cancer: a collaborative analysis of 18 prospective studiesJ Natl Cancer Inst20081001708318230794
- CarpenterWRRobinsonWRGodleyPAGetting over testosterone: postulating a fresh start for etiologic studies of prostate cancerJ Natl Cancer Inst200810015815918230791
- HolmängSMarinPLindstedtGHedelinHEffect of long-term oral testosterone-undecanoate treatment on prostatic volume and serum prostate specific antigen in eugonadal middle-aged menProstate199323991067690956
- KriegMNassRTunnSEffect of aging on endogenous level of 5a-dihydrotestosterone, testosterone, estradiol, and estrone in epithelium and stroma of normal and hyperplastic human prostateJ Clin Endocrinol Metab1993773753817688377
- SlaterSOliverRTDTestosterone: its role in development of prostate cancer and potential risk from use as hormone replacement therapyDrugs Aging20001743143911200304
- PecherskyAVMazurovVISemiglazovVFKarpischenkoAIMikhailichenkoVVUdintsevAVAndrogen administration in middle-aged and ageing men: effects of oral testosterone undecanoate on dihydrotestosterone, oestradiol and prostate volumeInt J Androl20022511912511903662
- CurranMJBihrleWIIIDramatic rise in prostate-specific antigen after androgen replacement in a hypogonadal man with occult adenocarcinoma of the prostateUrology1999534234249933071
- LoughlinKRRichieJPProstate cancer after exogenous testosterone treatment for impotenceJ Urol199715718459112543
- RhodenELMorgentalerATestosterone replacement therapy in hypogonadal men at high risk for prostate cancer: results of 1 year of treatment in men with prostatic intraepithelial neoplasiaJ Urol20031706 pt 12348235114634413
- SnyderPJPeacheyHBerlinJAEffects of testosterone replacement in hypogonadal menJ Clin Endocrinol Metab2000852670267710946864
- CarterHBPearsonJDMetterEJLongitudinal evaluation of serum androgen levels in men with and without prostate cancerProstate19952725317541528
- HeikkilaRAhoKHeliovaaraMSerum testosterone and sex hormone-binding globulin concentrations and the risk of prostate carcinoma: a longitudinal studyCancer19998631231510421267
- AgarwalPKOefeleinMGTestosterone replacement therapy after primary treatment for prostate cancerJ Urol200517353353615643240
- FerreiraULeitaoVADenardiFMatheusWEStopigliaRMNettoNRJrIntermittent androgen replacement for intense hypogonadism symptoms in castrated patientsProstate Cancer Prostatic Dis20069394116276352
- WeissJMHuangWYRinaldiSEndogenous sex hormones and the risk of prostate cancer: a prospective studyInt J Cancer2008122102345235018172860
- FowlerJEJrWhitmoreWFJrConsiderations for the use of testosterone with systemic chemotherapy in prostatic cancerCancer198249137313777059952
- McConnellJDProstatic growth: new insights into hormonal regulationBr J Urol199576Suppl 15107544215
- SarosdyMFTestosterone replacement for hypogonadism after treatment of early prostate cancer with brachytherapyCancer200710953654117183557
- KheraMLipshultzLIThe role of testosterone replacement therapy following radical prostatectomyUrol Clin North Am20073454955317983894
- SwerdloffRSWangCThree-year follow-up of androgen treatment in hypogonadal men: preliminary report with testosterone gelAging Male2003620721114628501
- El-SakkaAIHassobaHMElbakryAMHassanHAProstatic specific antigen in patients with hypogonadism: effect of testosterone replacementJ Sex Med2005223524016422891
- RhodenELMorgentalerAInfluence of demographic factors and biochemical characteristics on the prostate-specific antigen (PSA) response to testosterone replacement therapyInt J Impot Res20061820120516177827
- KuhnertBByrneMSimoniMTestosterone substitution with a new transdermal, hydroalcoholic gel applied to scrotal or non-scrotal skin: a multicentre trialEur J Endocrinol200515331732616061839
- ParekhDJAnkerstDPHigginsBAExternal validation of the Prostate Cancer Prevention Trial risk calculator in a screened populationUrology2006681152115517169636
- ThompsonIMAnkerstDPChiCAssessing prostate cancer risk: results from the Prostate Cancer Prevention TrialJ Natl Cancer Inst20069852953416622122
- ThompsonIMCarrollPRCarducciMARecommendations for defining and treating high risk localized prostate cancerJ Urol2006176S6S1017084170
- Summary from the second annual andropause consensus meetingChevy Chase, MdEndocrine Society2001
- BhasinSSinghABMacRPCarterBLeeMICunninghamGRManaging the risks of prostate disease during testosterone replacement therapy in older men: recommendations for a standardized monitoring planJ Androl20032429931112721204
- RhodenELAverbeckMATelokenPEAndrogen replacement in men undergoing treatment for prostate cancerJ Sex Med2008592202220818638000
- WestabyDOgleSJParadinasFJRandellJBMurray-LyonIMLiver damage from long-term methyltestosteroneLancet1977226226369876
- GurakarACaraceniPFagiuoliSVan ThielDHAndrogenic/anabolic steroid-induced intrahepatic cholestasis: a review with four additional case reportsJ Okla State Med Assoc1994873994047996313
- SoeKLSoeMGluudCLiver pathology associated with the use of anabolic-androgenic steroidsLiver19921273791535676
- BasariaSDobsASRisks versus benefits of testosterone therapy in elderly menDrugs Aging19991513114210495072
- The Endocrine SocietyClinical bulletins in andropause: benefits and risks of treating hypogonadism in the aging maleEndocr Rep2002216
- KimYCTestosterone supplementation in the aging maleInt J Impot Res19991134335210637467
- ViallardJFMaritGMerciePLengBReiffersJPellegrinJLPolycythaemia as a complication of transdermal testosterone therapyBr J Haematol200011023723810931008
- DrinkaPJJochenALCuisinierMBloomRRudmanIRudmanDPolycythemia as a complication of testosterone replacement therapy in nursing home men with low testosterone levelsJ Am Geriatr Soc1995438999017636099
- NieschlagETestosterone treatment comes of age: new options for hypogonadal menClin Endocrinol (Oxf)20066527528116918944
- UzychLAnabolic-androgenic steroids and psychiatric-related effects: a reviewCan J Psychiatry19923723281551042
- BahrkeMSYesalisCEIIIWrightJEPsychological and behavioural effects of endogenous testosterone levels and anabolic-androgenic steroids among males: a reviewSports Med1990103033372263798
- BagatellCJBremnerWJAndrogens in men – uses and abusesN Engl J Med19963347077148594431
- World Health OrganizationContraceptive efficacy of testosterone-induced azoospermia in normal men. World Health Organization Task Force on methods for the regulation of male fertilityLancet33695519901977002
- World Health OrganizationContraceptive efficacy of testosterone-induced azoospermia and oligozoopermia in normal menFertil Steril1996658218654646
- WilsonJDAndrogen abuse by athletesEndocr Rev198891811993042375
- LuboshitzkyRAvivAHefetzAHererPShen-OrrZLavieLLaviePDecreased pituitary-gonadal secretion in men with obstructive sleep apneaJ Clin Endocrinol Metab2002873394339812107256
- SchneiderBKPickettCKZwillichCWInfluence of testosterone on breathing during sleepJ Appl Physiol1986616186233745052
- MatsumotoAMSandblomRESchoeneRBTestosterone replacement in hypogonadal men: effects on obstructive sleep apnea, respiratory drives, and sleepClin Endocrinol (Oxf)1985227137214017261
- von EckardsteinSNieschlagETreatment of male hypogonadism with testosterone undecanoate injected at extended intervals of 12 weeks: a phase II studyJ Androl20022341942512002444
- TangrediJFBuxtonLLHypertension as a complication of topical testosterone therapyAnn Pharmacother2001351205120711675846
- de RondeWHyperandrogenism after transfer of topical testosterone gel: case report and review of published and unpublished studiesHum Reprod200924242542818948313
- CunninghamGRTestosterone replacement therapy for late-onset hypogonadismNat Clin Pract Urol20063526026716691239
- CunninghamGRMale hypogonadism: management strategies. News and views on male testosterone deficiencyA Supplement to Renal &Urology News200613
- KalyaniRRGaviniSDobsASMale hypogonadism in systemic diseaseEndocrinol Metab Clin North Am200736633334817543722