Abstract
Medical educators have called for new teaching methods and materials that supplement the traditional lecture format, and education in a range of health professions, including medicine, nursing, and pharmacy, is using a game-based approach to teach learners. Here, we describe a novel teaching tool in a case-based debate using the game format. Two teams of first- and second-year nephrology fellows participated in a PowerPoint game-based debate about which tests to order to diagnose transplant-related case. Our pilot study assessed the participant acceptance of case-based debate sessions and rewards system, and participant perceptions of using this approach to teach fellows and residents the importance of each test ordered and its cost-effectiveness in medicine. Each test ordered requires an explanation and has a point value attached to it (based on relevance and cost of positive and negative test results). The team that comes up with the diagnosis with most points wins the game. A faculty member leads a short concluding discussion. Subjective evaluations found these case-based debates to be highly entertaining and thought-provoking and to enhance self-directed learning.
INTRODUCTION
“Education is not the learning of facts, but the training of the mind to think”– Sir Albert Einstein
BACKGROUND
Interest in pursuing fellowship training in nephrology continues to steadily decline in the United States, especially among US medical graduates.Citation1 In 2010, a task force of the American Society of Nephrology mentioned the need to develop innovative teaching tools.Citation1 In response, our institution has developed several innovative tools in nephrology.Citation2–5 These tools are meant not only to increase interest in nephrology among medical students and residents, but also to enhance education and training of nephrology fellows. Some of these tools (crossword, anagrams, etc.) have been appreciated and recently showcased in peer-reviewed journals.Citation3–5 In this article, we introduce “Case-Based Debates” as a novel tool to teach transplant nephrology and kidney transplant pathology.
INTERVENTION
Pre-Session Preparation
| (A) | Faculty preparation of case. Two weeks prior to the scheduled Case-Based Debates session, a faculty member (who also moderates the session) chooses a challenging transplant nephrology case and sends a brief medical history and preliminary set of laboratory test results via e-mail to the fellows and other faculty members in the division. Laboratory and imaging data are collected for the patient, and the faculty member creates a PowerPoint (Microsoft, Redmond, WA, USA) presentation that includes a summary of the case, and a list of activities (e.g., taking family or social history, completing a physical exam, taking vitals, or ordering certain laboratory tests or consultations) that can be done with the case (). Full PowerPoint version of a sample case can be found on the Renal Failure journal website as a supplementary material. When chosen (clicked on), each test hyperlinks to a page that has the answer with its corresponding score as detailed below in the section of “Debate Session.” The initial tool takes about 1–2 h to create. Subsequently, less time is required as the only pertinent changes to make are the cases and test results. Figure 1. The main PowerPoint slide showing all tests that can be ordered by the teams. 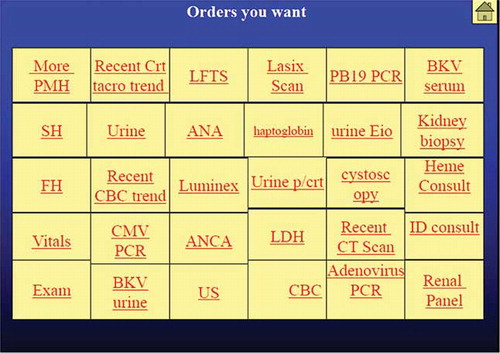 | ||||
| (B) | Fellow preparation for the session. Fellows are divided into two teams, each of which designates a person (likely senior fellow) as their spokesperson for the session. Each team has a faculty member (lifeline), who can be referenced twice during the debate. Each team meets for 10–15 min before the session (on the day of session or the day before) and formulates a differential diagnosis and comes up with a diagnostic plan involving the minimum number of tests that would lead them to most likely diagnosis. Residents, if present, are equally distributed to the two teams on the day of session. | ||||
Debate Session
The Debate Session usually lasts an hour during which the case is reviewed. In addition to discussing the differential diagnosis of the case (which is based on the initial clinical and laboratory test results presentation), significant time is dedicated to discuss the appropriate approach to further evaluate the case. The need for a particular laboratory test, radiological images, and pathology slides is reviewed in depth. The first team then selects a test. Each test that is ordered requires an explanation of that test—how it is done, its significance, and operational characteristics in terms of sensitivity and specificity. Next, the second team is asked to pick a test of their choice, with the same requirement for explaining the purpose.
A faculty member helps with keeping the scores. Faculty observers are present but are not allowed to help the fellows. After three “diagnostic orders” per team, the moderator asks each team for an update on their differential diagnosis for the case. After the initial break, the teams continue to use the diagnostic tests on the master slide. After 40 min into the session, the teams are asked to select a “final diagnosis.” The team that comes closest to correct diagnosis is then asked to predict the specific biopsy findings. Next, the pathology slides are reviewed, which earn bonus points to the team who reads them accurately.
At the conclusion of the session, the faculty moderator gives a 5-min review on a unique aspect of the case or treatment options as applicable. Faculty observers also can provide their input on the case before the session concludes. The process is repeated on a monthly basis, using different cases.
Scoring
Each test links to a page that has the answer with its corresponding score. A master slide is designed and displayed by the faculty listing all the obtainable tests and information (). Investigations and questions are graded or rewarded with points according to their relevance (determined subjectively by the moderator) and diagnostic importance. Points are awarded for choosing a more relevant and inexpensive test and points are deducted for choosing an unnecessary test. For example, proceeding straight to a renal biopsy disqualifies the team. The team with most points wins the game.
Acceptance by Participants
Fellows and faculty members participating in these debates were asked to rate the following statements on a scale of 1–5, with 5 being the highest score of agreement:
| 1. | The activity was enjoyable. | ||||
| 2. | It supplemented and enhanced my existing knowledge on the topic. | ||||
| 3. | It is an effective use of my time and emphasizes all the key points. | ||||
| 4. | I am willing to use the same activity for other topics. | ||||
A total of 15 participants completed the survey and all rated the session with a 4 or 5 on the four assessment dimensions. Both fellows and faculty members who participated in our conferences reported finding the activity highly enjoyable. They also agreed that it enhanced their knowledge and that they would want to use this tool for other topics in nephrology.
DISCUSSION
Medical educators have called for novel teaching methods and materials to supplement the traditional lecture format. Many health professions such as nursing, pharmacy, and medicine utilize PowerPoint games to teach students.Citation6–9 The game (Jeopardy) format has been reported to increase participation grades of students, as well as improve their self-directed learning skills.Citation10 The case-based debate format is one of these methods. In our intervention, the fellows and residents learn the value of a specific test, the implications of a false negative and false positive test result, and the effect of ordering unnecessary tests. This tool can also be used to teach learners about cost-effectiveness of a particular diagnostic test. We believe that our case-based style of teaching not only encourages learners to participate, but also promotes understanding and retention of medical knowledge. This tool creates an interactive learning environment that leads to informative discussions among team members about the appropriate diagnostic approach and management of the case. This can include heated but healthy debates on what certain diagnostic tests will reveal or not reveal regarding a particular diagnosis. This educational tool also fulfills the Accreditation Council for Graduate Medical Education core competencies of medical knowledge, practice-based learning and improvement, and systems-based practice.
We believe that this enjoyable, interactive educational tool will enhance the diagnostic and management skills of fellows and residents, as well as improve their self-directed learning skills. This tool was recently introduced and taught with other teaching tools at the “Resident as Teacher” conference at our institution. Residents were polled at the end of the conference to determine which of these tools they would use as their preferred teaching method. The case-based debate teaching method turned out to be the most preferred teaching tool among residents who participated in this conference. Although we are hopeful that this along with other teaching toolsCitation2–4 will create interest in nephrology careers among medical students and residents, we have not evaluated this at the present time. We also plan to use this tool to teach other aspects of nephrology and internal medicine. We encourage all medical educators to consider this interactive teaching tool in their respective field of medicine.
Declaration of interest: The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
REFERENCES
- Parker MG, Ibrahim T, Shaffer R, Rosner MH, Molitoris BA. The Future Nephrology Work Force: Will there be one? Clin J Am Soc Nephrol. 2011;6(6):1501–1506.
- Calderon KR, Vij RS, Mattana J, Jhaveri KD. Innovative teaching tools in nephrology. Kidney Int. 2011;79(8):797–799.
- Jhaveri KD. Nephrology crossword: Glomerulonephritis. Kidney Int. 2010;77(12):1141–1142.
- Chawla A, Jhaveri KD. Quiz page March 2011: Hypokalemia anagrams. Am J Kidney Dis. 2011;57(3):A25–8.
- Malieckal D, Jhaveri KD, Chawla A. Nephrology teaching tool: Anagrams. Ren Fail. 2011;33(7):736–740.
- LeCroy C. Games as an innovative teaching strategy for overactive bladder and BPH. Urol Nurs. 2006;26(5):381–384.
- Persky AM, Stegall-Zanation J, Dupris RE. Students’ perceptions of the incorporation of games into classroom instruction for basic and clinical pharmacokinetics. Am J Pharma Educ. 2007;71(2):21.
- Urlich D, Glendon K. Interactive Group Learning: Strategies for Nurse Educators. 2nd ed. New York: Springer; 2005.
- Latessa R, Harman JH, Hardee S, . Teaching medicine using interactive games: Development of the “stumpers” quiz show game. Fam Med. 2004;36(6):616.
- Patel J. Using game format in small group classes for pharmacotheraeutics case studies. Am J Pharm Educ. 2008;72(1):21.