
Figures & data
Figure 1. Skin manifestation of a 30-year-old African American male that presented with lesion on upper extremity and hemolytic anemia.
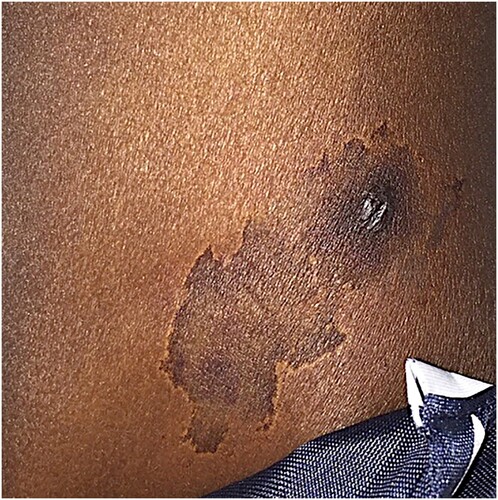
Table 1. Case 1 Laboratory data from admission to discharge (Dr. Dickey case).
Table 2. Case 2 Laboratory data from admission to discharge (Moore case).
Figure 2. A Brown Recluse spider (Loxosceles reclusa). Note the dark brown violin shaped image located on the spiders back. This can be utilized to identify L. reclusa.

Figure 3. Geographical distribution of the brown recluse spider (Loxosceles reclusa). Black dots represent L. reclusa populations. The highest density of L. reclusa is localized to Texas, Illinois, Missouri, Kansas, Oklahoma, and Kentucky.
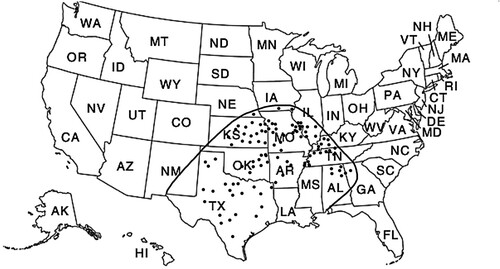
Figure 6. Intravascular and extravascular hemolysis secondary to L. reclusa envenomation. Note that RBC hemolysis leads to the release of intracellular LDH thereby leading to an elevated serum LDH level. In addition, intravascular RBC hemolysis leads to the release of free hemoglobin which eventually binds serum haptoglobin thereby forming a haptoglobin-hemoglobin complex (Hap-Hem). The Hap-Hem complex results in the reduction of circulating free haptoglobin. Importantly, high concentrations of intraluminal hemoglobin within the kidney predisposes to nephrotoxic acute tubular necrosis. Therefore it is important to aggressive hydrate patients with severe hemolytic anemia, such as in systemic loxoscelism.
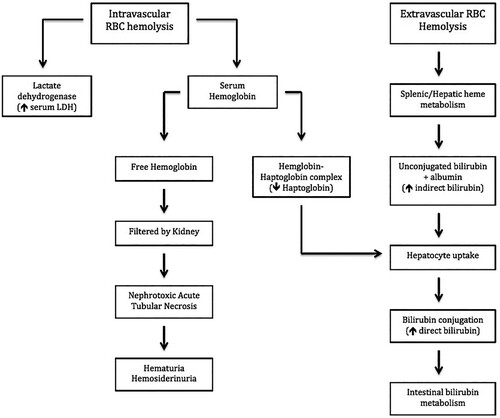
Figure 5. Hypothesized pathophysiological response to L. reclusa induced hemolytic anemia. Note that complement factor C3b and IgG deposit onto the RBC surface thereby initiating RBC phagocytosis. Importantly, the direct antiglobulin test (DAT or Coomb’s test) identifies the deposition of C3b and IgG deposition, which makes the DAT extremely valuable in detecting warm AIHA. In addition, activation of the classical complement pathway results in the assembly of C1 complex, C4, and C2 thereby forming the C3 convertase (C2aC4b), which leads to a reduction of circulating complement factors C3 and C4.
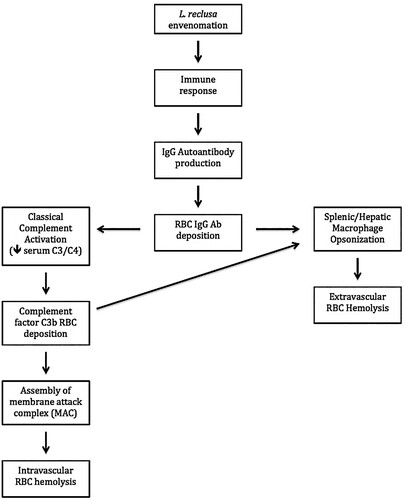
Table 3. Signs and symptoms of systemic loxoscelism.
Figure 4. (A) Purulent cutaneous lesion due to L. reclusa approximately 1 week after the initial bite. (B) Dermonecrosis due to L. reclusa 2 weeks after the initial bite. (Yigit). The combination of venom components, cellular death, and aggressive inflammatory response leads to hemorrhagic necrosis and ultimately the formation of dermonecrosis with a central black eschar.
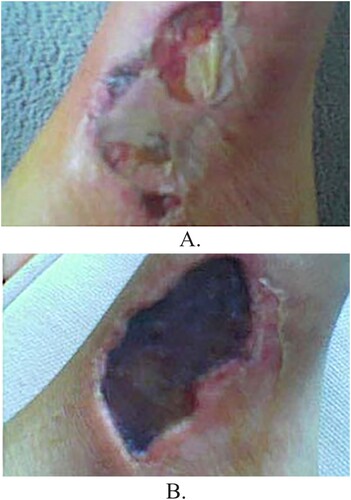
Table 4. Laboratory findings associated with systemic loxoscelism.
Table 5. Diagnosing warm (IgG) autoimmune hemolytic anemia.
Table 6. Treatment modalities with response rate (RR) for systemic loxoscelism.
Table 7. Summary.