
ABSTRACT
This article examines tensions that professionals in healthcare settings in low-to-middle income countries (LMICs) face in the evolving field around surveillance of antimicrobial resistance (AMR). Few public health problems are of greater global importance today than AMR, that poses a threat to our ability to treat infections. In this context, the microbiology laboratory occupies a prominent place and the knowledge field of microbiology is expanding. In this study, we interviewed twenty-three (n = 23) professionals with expertise on AMR and public health systems to synthesise knowledge on strengthening AMR surveillance in LMICs. By drawing on a practice approach [Schatzki, T. R. 2001. “Practice Ttheory.” In The Practice Turn in Contemporary Theory (1–14), edited by T. R. Schatzki, K. Knorr-Cetima, and E. von Savigny. New York: Routledge.] combined with socio-cultural and cultural-historical theories (CHAT) [Engeström, Y. 1987. Learning by Expanding: An Activity-Theoretical Approach to Developmental Research. Helsinki: Orienta-Konsultit] the analysis reveals seven tensions between elements of the systems and discusses how such tensions serve to frame implications for implementing a capacity strengthening programme. The analysis shows that the novelty of the AMR as well as being a multi-disease and multisectoral by nature challenges existing forms of professional practice in healthcare settings. It also suggests that AMR requires to be dealt with through inter-professional and inter-sectoral approaches, while maintaining a focus across the local, national, and global systems, which is essential for initiatives that are set to address challenges to global health.
Introduction
Antimicrobial resistance (AMR), is recognised as one of the most serious global threats to human health in the twenty-first century. AMR is defined as the ability of a microorganism (bacteria, viruses, parasites) to stop an antimicrobial (an antibiotic, antiviral or antimalarial) from working against it (WHO Citation2020a). Without effective antibiotics, routine medical procedures will be less safe in the future and even minor infections will no longer be treatable. The effects of AMR are predicted to be more acute in resource-limited settings such as in low-to-middle income countries (LMICs). However, no country can view itself in isolation and addressing this serious threat to public health is a global priority that requires collective action across all countries.
To this end, in 2015 the World Health Assembly endorsed a Global Action Plan on Antimicrobial resistance (WHO Citation2015). In response to this action, the UK Government launched a major UK Aid initiative, the Fleming Fund,Footnote1 to support LMICs to improve the surveillance of AMR. Surveillance of AMR tracks changes in microbial populations, permits the early detection of resistant strains of public health importance, and supports the prompt notification and investigation of outbreaks (WHO Citation2020b). For this global initiative to be effective, there has to be consideration of areas where action and change will have the greatest impact. WHO (Citation2015) has already established that, since AMR is evolving rapidly, professionals involved in the surveillance of AMR need regular opportunities to develop and apply new knowledge and this can be supported through targeted professional learning. However, less is known about what forms of professional learning are likely to support professionals as they learn and apply knowledge about AMR in microbiology laboratories in resource-limited settings. This paper is set to address this gap by elucidating forms of professional practice that are needed to improve AMR surveillance.
AMR surveillance relates specifically to the field of microbiology and can be positioned at the intersection between established microbiology and new scientific knowledge that de-stabilises how microbiology is understood. In parallel with the emergence of these new forms of knowledge is an increasing diversity in specialist roles and practices, with new actors involved in surveillance activity from diverse fields such as public health, medicine, policy development and so on. This expansion of knowledge and proliferation of job roles sit alongside the rapid production of a range of new knowledge resources, operating procedures, national and international policies, conventions and protocols which can be viewed as socio-material artefacts. As professionals use these artefacts, knowledge is expanded and professional work is transformed. Under these conditions the established rules and conventions that guide professional work become increasingly blurred and, as a consequence, the epistemic spaces for professional work – spaces for action comprising knowledge resources, norms and rules for interpreting professional problems – become more fluid (Markauskaite and Goodyear Citation2017). This fluidity makes it difficult to introduce new forms of practice to professionals who already are finding it difficult to keep up with rapid developments in their field. Yet, little is known about the tensions professionals face in their everyday work practice and how these tensions may influence learning.
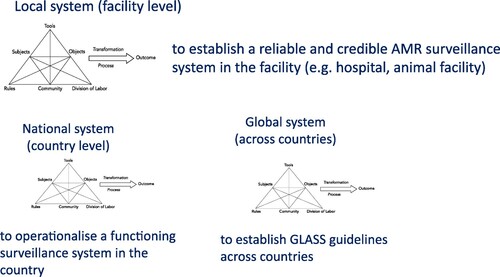
This study presented in this paper was funded by the Fleming Fund as part of a larger study of professional learning for AMR that took place from April 2018 to September 2019. This article lays out foundational research that was conducted during the initial scoping phase between April and December 2018. In this study, we draw on the notion of practice (Schatzki Citation2001) as a lens through which to analyse human activity and the organisation of the contexts in which people act. In using this, we are attentive to tensions in the context of AMR surveillance work, both at a particular point in time, and as they evolve over time. To examine these tensions we draw on the tradition of socio-cultural and cultural-historical activity theory (CHAT) (Engeström Citation1987). We conceptualise AMR surveillance as an activity system that constantly evolves through collective learning actions in response to systemic tensions (or contradictions, in Engeström's terms). This conceptualisation facilitates a multi-faceted analysis of the complex practices of professional work as it evolves. We thus use as a theoretical lens a set of activity systems that are complemented and extended through interconnection with other activity systems. An example of an AMR activity system is an AMR national system, led by a Health Ministry, which has the objective to establish an AMR surveillance system within a country (see ). Analysis of these activity systems enables identification of specific tensions, either within a single system or across parallel activity systems that may inhibit expansion of work practices to tackle AMR. By attending to these tensions, this study provides insights into forms of professional practice that are needed to improve AMR surveillance and addresses the following questions: What tensions do laboratory professionals face as they engage in AMR surveillance? Can professional learning support professionals in addressing these tensions?
Figure 1. Surveillance of AMR in interconnected-activity systems.
The paper is structured as follows: First, we outline recent developments affecting the role of the microbiology laboratory in the surveillance of AMR. Next, we reflect on the relationship between professional work and learning through a practice approach. Following this, we present the research context and method for the fieldwork, followed by discussion on specific emerging tensions in the field of laboratory surveillance as perceived by people with knowledge about the local, national and global AMR systems. Finally, the ways that professional learning can support professionals in addressing these tensions will be discussed in the conclusions.
The expanded role of the microbiology laboratory in the surveillance of AMR
Laboratory-based surveillance is a fundamental priority to reduce AMR (WHO Citation2015). It relies on the ability of laboratory staff to provide accurate, reliable and timely laboratory testing. In many LMICs lab-based surveillance systems have either not yet been established or have only partially been set up (Opintan et al. Citation2015). To address this gap in provision, numerous national and international agreements have been agreed and are being rolled-out across LMICsFootnote2 and resources related to AMR are being created. These take various forms, including national policies; guidelines for policy makers and health workers; clinical and animal health protocols and frameworks; and operating procedures for health services.Footnote3 These resources can be sourced and adapted for local use in healthcare facilities leading to new requirements being placed upon workers (i.e. laboratory professionals) who are expected to use them, expand their knowledge and engage in new forms of professional practice. However, changing established practice is not straightforward (Nerland Citation2018).
Furthermore, AMR surveillance activity is expanding to include a multitude of professionals beyond the microbiology laboratory and these actors may influence professional practice in different ways, as new forms of relationships are established (Littlejohn, Charitonos, and Kaatrakoski Citation2019). These include lab staff, medical and para-medical professionals, epidemiologists, surveillance officers, statisticians, government units, donor agencies. As a result, knowledge and ways of knowing are enacted by an expanding range of professionals distributed across a variety of different sites (Nerland and Jensen Citation2014; Littlejohn, Charitonos, and Kaatrakoski Citation2019).
Against this background, the microbiology laboratory becomes an increasingly important professional setting. However, as discussed in the Lancet Series on pathology and laboratory medicine in LMICs (see Wilson et al. Citation2018), the laboratory often is a neglected part of public health systems, especially in LMICs. In the Lancet series, Sayed et al. (Citation2018) point to on-going professional development as a way to maintain a professionalised lab workforce and argue that opportunities to enhance training by increasing and improving education provision should be explored and implemented. It remains unclear, though, how professional learning can be implemented in laboratory settings in ways that support AMR surveillance.
This paper is set to address this gap by examining how professionals involved in laboratory-based surveillance can be supported in expanding their practice. However, laboratory work influences and is influenced by work at the national and global levels. AMR surveillance activity cannot be viewed merely as actions within a microbiology laboratory, ignoring the inherent dynamics that exist between these actions and other actors (Leont’ev Citation1978), for example between lab professionals and clinicians. It is only by examining surveillance in its totality and the tensions that exist within and between these system elements that we identify the actions needed to support learning and changes in work practice. To achieve this goal, we applied methodological and analytical tools from CHAT.
The next section provides a brief description of practice approach in professional learning, followed by a description of the research context and fieldwork and details the methodological approach used to generate data to answer the research questions.
Perspectives on professional work and learning through a practice approach
Developments in lab-based AMR surveillance involve the lab professionals operating in complex systems, often with others, in particular environments that have unique characteristics of their own. The work environment both creates opportunities for learning and limits them. In other words, professional learning is inherently linked with the workplace (Fuller and Unwin Citation2003). This means that professional learning has to be located within professional practice settings and to extend current practice. However, current forms of Continuing Professional Development (CPD) restrain the opportunities to link professional learning with everyday work practice (Boud and Hager Citation2012). CPD within organisations has become synonymous with formal training and participation in courses or seminars in classrooms rather than integrated with everyday work (Littlejohn and Margaryan Citation2014). Often large numbers of people are supported in reaching a specific level of competency in a curriculum with pre-prescribed learning objectives (Littlejohn and Margaryan Citation2014). These events are specified and delivered by ‘experts’, often in settings outside the workplace itself, and have a focus on delivering content rather than enhancing learning (Webster-Wright Citation2009). The knowledge acquired in CPD events is supposed to be ‘transferred’ back to the workplace, but often is not applied to work (Littlejohn and Margaryan Citation2014). This view of CPD disconnects professional learning from professional practice taking place in the workplace and assumes that practice can be changed or updated by acquisition of knowledge independent of the work context. Another problem with this view is the assumption that professional development focuses exclusively on individuals and individual learning, failing to take account of the reflexive relationship between learning and working and overlooking workplaces as sites for ‘ participating in the social relations of production’ (Fuller, Munro, and Rainbird Citation2004, 299) where individuals learn through membership of social groups.
In this research, we draw on the notion of practice (Schatzki Citation2001) as a lens through which to analyse human activity and the organisation of the contexts in which people act – an ‘embodied, materially mediated arrays of human activity centrally organised around shared practical understanding’ (Schatzki Citation2001, 2). In the context of this study, for professionals involved in AMR surveillance activity to evolve a shared way of working, the practice of surveillance should be ‘stabilised’ and ‘institutionalised’ (Gherardi Citation2009) across involved institutions as a recognised form of collective doing, albeit not necessarily uncontested. Surveillance is not yet a stabilised, consolidated practice in LMICs as it will be discussed in later sections of this paper. As professionals deal with constant changes in their work environment, they need to learn new forms of knowledge and practice on an ongoing basis to solve emerging problems (Hager Citation2004; Hadwin, Järvelä, and Miller Citation2011; Illeris Citation2011). Understanding the processes at play in generating, expanding, stabilising and sustaining forms of practice around surveillance are critical when planning professional learning and CPD.
Within a ‘practice approach’ to CPD, knowledge is no longer considered to be an ‘object’ that is discovered, acquired or transferred. Instead, knowledge is viewed as a practical, distributed and collective activity, ‘entangled in systemic webs’ (Fenwick, Nerland, and Jensen Citation2012, 6) and situated in time and space through work practices (Gherardi Citation2009). This aligns with Boud and Hager’s (Citation2012) view that CPD must be located ‘in what professionals do and the circumstances under which they learn’ (22). From this perspective, professional practice links each professional carrying out an activity within the historical and social contexts in which the activity occurs; the practices are emergent from the context and therefore cannot be anticipated or predicted. What this means is that the direction of learning equally cannot be specified in advance. That said, ‘learning is directly implicated in practice, and learning can be represented as an outcome of participating in practice’ (Boud and Hager’s Citation2012, 23). Adopting this perspective of learning and practice in professional settings, places emphasis on how practice is evolving in the context of changing social and institutional arrangements and foregrounds how each professional becomes a proficient practitioner. In using a practice-based approach with CHAT, this paper draws attention to tensions that may affect processes of knowing and learning around AMR within the context of a workplace culture and offers new insights into how professional educational provision could be developed to support professional practice around AMR surveillance.
Surveillance of AMR in interconnected-activity systems
CHAT views human activity as systemic, driven by an object (i.e. the main motive behind the activity) and involving interconnected tools, rules and social practices (Engeström Citation1987). By viewing AMR surveillance as a system comprising a number of interrelated elements, it is possible to identify tensions and contradictory dynamics that exist within the system, which have not systematically been examined until now. Hence, in this study we analyse AMR surveillance in a holistic way and allow it to reveal itself in its totality, by examining the multiplicity of motives, tools and social practices that have historically shaped this activity. Identifying these tensions within the AMR system is an important step forward in being able to address these issues.
In this analysis, we drew on the tradition of CHAT (Engeström Citation1987), by using an expanded activity system (see ) to analyse AMR surveillance work environments. Engeström (Citation1987) describes human relationships as interwoven with multiple contradictions, and conceptualises learning as a dynamic and non-linear process. An activity system can have internal tensions (contradictions in Engeström's work), observed either within or between the components of a single system (e.g. rules, division of labour, community) or between interacting activity systems. Contradictions are not isolated problems within an activity system but ‘historically accumulating structural tensions within and between activity systems’ (Engeström Citation2005, 137). Therefore, there is a distinction between a tension that may be noticed as an isolated event and a tension that is experienced repeatedly by participants.
In our work, we focused on the tensions that professionals in a health facility may face when they have to accommodate the new AMR surveillance practices within their existing work. We viewed the work of laboratory professionals at the level of a single facility (ie a hospital lab, an animal health lab and so on) as the core activity system, since these facilities aim to contribute high quality data to a regional or national AMR surveillance system in a reliable way. This is complemented and extended with models of multiple neighbouring, interconnected activity systems, including national activity systems overseen by health ministries. There are also trans-national systems that feed national AMR data into a global system, led by WHO and other UN agencies. Tensions identified in the neighbouring activity systems do affect the core activity. For example, procurement rules that are established at a national level affect access to materials and resources at a facility. This relationship influences how often or well laboratory staff perform AMR tests; if a sufficient amount of the right materials are procured, tests can go ahead at the right frequency and accuracy, but if there are too few materials or the resources are too low quality, the reliability of the data are compromised.
The next section provides a description of the research context and fieldwork and details the methodological approach used to generate data to answer the research question.
Method and context of study
Participants
Data was gathered within the period April to June 2018 through a series of face-to-face and online interviews with twenty-three (n=23) participants. Each participant was selected because of his/her good knowledge about AMR and/or public health systems a experience of work in multiple countries across the world, including: Vietnam, Malawi, Cambodia, Philippines, Pakistan, Mali, Tanzania, Ghana, Uganda, Nepal, India, Laos, Kenya, Bhutan, New Zealand, Myanmar, Zimbabwe, France and the UK.
In particular, seven participants were based in an LMIC when the interview took place and were considered to have good knowledge of local and/or national systems. Other participants had strong knowledge about the global AMR system (see below e.g. Experts’ Advisory Group). Purposive sampling was performed on the basis of having representatives of all three systems outlined earlier from a list of potential participants that was compiled through recommendations from the UK DHSC and the Management Agency leading the implementation of the Fleming Fund.
In total twenty-three people were interviewed (n=23; 6 female, 17 male), as illustrated below:
(1) members of staff at a research institution in a LMIC, leading a capacity programme on AMR (n=2, knowledge of local and national systems);
(2) members of staff of the Management Agency leading the implementation of the Fleming Fund (n=8, local, national and global systems);
(3) members of the Technical Advisory Group (TAG) of the Fleming Fund (n=3, local, national and global systems);
(4) members of the Experts Advisory Group (EAG) of the Management Agency leading the implementation of the Fleming Fund (n=7, global system);
(5). secondees from the UK DHSC in international organisations such as WHO, OIE and Food and Agriculture Organisation (FAO) (n=3, global system),
Participants were invited to be interviewed via an email outlining the purpose of the study. When a positive response was received, a follow-up email outlined the interview arrangements as well as information about the participation in the study. The process for data gathering, analysis, and storage along with their rights to choose whether to participate and information about data withdrawal were also sent to the participant.
Interviews lasted from 30min to 60min (average duration 50min), and were audio recorded and transcribed verbatim. Each interview was guided by a semi-structured instrument previously used in studies of self- regulated, professional learning (Littlejohn et al. Citation2016). The study received a favourable response by the Research Ethics Committee at the Open University.
In this paper, we use the term LMICs, but we acknowledge that despite the strong work experience our participants had across numerous countries, their views cannot claim to address the diverse range of LMICs in unison, considering their varied health systems and responses to AMR surveillance. It is also noted that most participants had experience in human health systems, rather than animal health or agriculture. We recognise that these were recommendations by two of our collaborating organisations and as such they may have shared favourable views towards the Fleming Fund. Finally, we recognise that despite our work and experience in this research area we enjoy a relative privilege as researchers in the Global North. To mitigate the reproduction of unequal power relations and hierarchies of knowledge through our work we devised a research design which attends to the ‘voice’ of professionals as a lens through which researchers understand their experiences. This was operationalised through collaboration with local actors and institutions in three LMICs and in-country fieldwork. For a discussion concerning the fieldwork with lab professionals in LMICs see Littlejohn, Charitonos, and Kaatrakoski Citation2019 and Charitonos et al. Citation2019.
Analytical approach
The aim of the analysis was to address the question: What tensions do laboratory professionals face as they engage in AMR surveillance? Can professional learning support professionals in addressing these tensions? Data were analysed using the CHAT framework (Engeström Citation2015). Analysis involved assembling a range of factors associated with each professional's work and learning recorded during the interviews, for example the context of strengthening surveillance and professional development opportunities. Analysis of these data enabled the development of in-depth understanding of the characteristics of the laboratory setting, including the various roles involved in surveillance and their working relationships with other professionals; current forms of work practice in AMR surveillance in the surveillance networks; and forms of professional learning that are used to build capacity in this context. Through the analysis we could also identify existing and potential future tensions associated with implementing a capacity strengthening programme. The interviews were transcribed in full. Transcriptions were uploaded to the analysis software application, NVivo 11. Two researchers carried out comparative analysis to ensure consistency of coding. The analysis identified seven emerging tensions affecting professionals’ knowing and learning which are outlined in the next section.
Findings
Tension #1: There is a need for laboratory professionals to prioritise the reduction of AMR, however some professional groups have limited awareness of the global threat posed by microbial resistance
A consensus among interviewees was that professionals involved in AMR surveillance, including laboratory workers, often are not aware of the critical nature of increasing microbial resistance (local and national systems, tension between subject and tools). Those we interviewed signalled that as well as poor public awareness, knowledge about AMR is limited amongst professionals in public health facilities. Some interviewees suggested this was due to limited mobilisation of resources (e.g. funding) to tackle AMR within health systems in LMICs (national and global systems, tension between tools and rules). However, this may have reflected their own experience in particular LMICs as there are variations within countries.
The interviewees referred to AMR as gaining a growing interest, creating thus a work environment that is ‘dynamic’ and ‘fluid’ where an increasing number of actors (e.g. donors), viewpoints and controversies have entered the workplace and led to conflicting interests. The following quote highlights some of the vested interests as well as competing concerns and priorities amongst diverse stakeholder groups (national and global systems, tension between subject, community and rules):
It [AMR] is an up and coming subject. So people [donors] are investing […] and taking up the resources of a very limited number of people. […] the absorptive capacity of the countries … has been limited … [P3, member of staff of the Management Agency]
The analysis identified tensions associated with vested interests and competing priorities amongst various actors across activity systems. These interests influence the production and transformation of practices and thus become ‘networks of influence’ (Fenwick, Nerland, and Jensen Citation2012, 7) that exert power, generate knowledge and enable new possibilities for professionals who may take on new responsibilities and new opportunities for engagement in this field.
Tension #2: AMR is a multi-sectoral challenge, but professional practices to reduce AMR are not always considered across sectors in a holistic way
The second challenge is concerned with AMR as multi-sectoral challenge that involves farming and agriculture, the environment, human health and animal health systems. However, an established norm is that facilities (e.g. hospitals, Animal Health Labs) are set up to work independently. Enabling these facilities to work together requires a number of architectural or organisational changes that will ensure responsibility for AMR is distributed across sectors. This requires the formation of new communication channels, as well as new collaborations and partnerships at the local and national level. However, the analysis of the interviews highlighted cross-sector working as an on-going challenge (tension between rules and division of labour).
An example provided by several interviewees was related to the ‘One Health’ principle, which underpins initiatives such as the Fleming Fund due to the inter – relatedness of human, animal and agriculture systems. Many interviewees referred to their work towards facilitating One Health approach while recognising that this is taking place in an environment where awareness about the One Health is low. ‘Everybody […] uses the words One Health, and understands that One Health is important […] but without really understanding how to achieve that’ [P23, member of staff in the management agency], pointing to a tension in how to operationalise this principle on the ground (tension between subject, tools and division of labour).
It is noted that the interviewees referred to specific mechanisms (i.e. tools) that have already been put in place to facilitate the One Health perspective: an example is the establishment of AMR Committees in various LMICs with representatives from across all sectors. Despite this positive development, it is noted that AMR Committees are formed by actors who themselves might not share high levels of awareness about AMR (as identified in Tension #1). Furthermore, the committee usually sits within the Ministry of Health in each country and is often chaired by the Health Minister, which may result in power relationships taking priority and agendas being driven by preferences and accountabilities that prioritising particular forms of action in the human health sector.
Interviews pointed to approaches to implementing One Health that often focus on strengthening each individual system (i.e. human, animal, environment). This approach, despite having some merits (e.g. each sector generating quality data), deprioritises multi-sectoral approaches, does not encourage learning across boundaries and sustains independent forms of work, where for example professionals in animal health facilities only take part in professional development programmes with people from the same sector. A well-functioning AMR surveillance system requires new forms of collaboration and ways of working (see Tension #4), which, in turn, require new roles (e.g. One Health officer), rules (e.g. lab professionals from human health and animal health in joint CPD) and division of labour (e.g. AMR work in association with other diseases e.g. HIV).
Tension #3: AMR Surveillance is an outcome of well-functioning lab networks, yet these networks are under-developed
The third challenge identified in the analysis focused on the creation of well-functioning surveillance networks. One of the key mandates of the Fleming Fund is to set-up and support AMR surveillance networks within LMICs, comprising Reference Labs (i.e. animal and human health) and sentinel sites. Some countries already have a network in place or may be developing a network as part of their participation in the Fleming Fund. Yet the scale varies substantially, not only across countries, but also within the country itself. Labs in urban settings are usually more advanced compared to those in rural settings, the capacity and expertise in AMR Reference labs is different from the sentinel sites whilst AMR surveillance for human health tends to be more advanced than in the animal health sector. Even when a network of labs appears to be established ‘these labs [in the capital in one LMIC] they don't talk to each other. They live alone (and only) talk to the public health regulatory bodies’ [P4, member of the EAG].
The interviewees suggested that the speed and extent to which AMR surveillance can be strengthened depends on how well networks function. Success largely depends on the resources available (including funding and human resources) and commitment from the government (national system, tension between tools and rules). A number of systemic issues related to the day-to-day operation of the laboratories were highlighted during the interviews. These issues include the infrastructure (i.e. power supply, equipment, lack of human capacity to use the equipment), quality of services (i.e. quality control, quality assurance) but also the procurement processes within the public health system in LMICs. High quality resource materials are needed for AMR lab tests, including reagents, but these were not always available due to high cost.
They [lab technicians] know that they need good reagents, but they don't have these reagents, because the national procurement agency is not supporting [purchase of] this reagent because they cost too much initially … [P5, member of staff of the management agency]
Tension #4: AMR surveillance relies on good practice, yet effective ways of working are not yet established
Several interviewees drew attention to examples of ingrained professional practices, including the pharmacist who sells antibiotics over-the-counter without a prescription or the farmer who uses antibiotics in agriculture in an indiscriminate way. Interviewees recognised that there are often cultural and economic reasons behind such practices (e.g. loss of income). An example of poor practice frequently used in the interviews concerned the clinicians often relying on empirical diagnosis to make decisions about treatments. In fact, one interviewee explained that
if you get a fever in Tanzania […] during the rainy season, 99% of the cases, you are diagnosed as suffering from malaria. Do they [clinicians] know that you have malaria? No, they don't. But they presume that you have malaria [P2, member of staff in the management agency]
Another interviewee viewed clinicians’ prescription practices as an ‘old practice’ that is still endured, despite recent developments. The following quote highlights the critical role of the lab professionals in enabling good clinical practice:
antibiotic prescribing was a very easy task when I [interviewee] was a young physician because we had a lot of antibiotics and every antibiotic was working on most bacteria […] Now it's very, very complicated […], because we have bacteria on which very few antibiotics which are working. […]. And very often, it's a great help for the clinicians to have the advice of the microbiologist to choose the right antibiotic […] [P18, member of EAG]
The expectations each professional has of their role and the behaviours observed in public health contexts in LMICs may also affect the way the various actors frame problems, draw on available resources and take action to determine potential solutions. Even when clinicians request lab tests they ‘are just getting figures on bacteria and resistance without knowing the broader demographic information around those samples’ [P23, member of staff in the management agency].
One tension relates to the interconnectedness of professional spaces and practices within AMR surveillance activity and how this relationship destabilises the association of various professionals, leading to disagreement about how practice should be advanced and potentially de-stabilising the work system.
Tension #5: AMR Surveillance requires data flow across local, national and global systems, yet professionals have limited conception of how these systems inter-relate
Three different visions of how data is used within a surveillance system were articulated during the interviews. First, good quality AMR data from the labs is shared within a local facility with clinicians or vets to support diagnosis, prophylaxis and treatment at an individual level. Second, AMR data is made available in aggregated forms at the local facility to support treatment guidelines and Standard Operating Procedures (SOPs) in ways that a ‘[clinician] can adapt your [his/her] empirical treatment using the retrospective data’ [P18, member of EAG]. The third vision of data use involves aggregating information from facilities across the country, thereby building a systematic map of the susceptibility pattern of each type of bacteria at a national level. This information is used to help shape public health policy and practice.
However, few LMICs have a systematic way of collecting and reporting these data. There are few standardised procedures and standardisation of reporting systems and data sharing and comparability with other countries is not yet possible (global system). Links between clinical data, samples and clinical outcomes are not usually made (local system) while any AMR data that are available often is generated by externally funded research projects. Although some facilities have capacity to perform complex tests, such as an AMR sensitivity test
it is not usually done […] Plus it takes time. Plus it involves resources. […] Or it may be done but then the information is not used, […] it is not reported. So we have a lot of black holes in our understanding of what bacteria are resistant to which antibiotics in each country [P2, member of staff in management agency]
Tension #6: AMR surveillance requires trust and openness among professionals, but this trust is not always evident, particularly where people are not in direct contact
Interviewees described strained relationships between clinicians and lab professionals at the local level, resulting in clinicians having little trust in the lab processes and the data generated:
Very often, they [clinicians] do not do the sampling, because … they don't trust the result of the lab. And […] they know that they will not use the result … They don't send [requests for] test, so the lab has very little tests to perform, and so they are not very good at performing tests and they are not very good at giving good results [P18, member of EAG].
Such a lack of trust creates a ‘vicious circle’ [P7, member of DHSC TAG] and influences the ways in which the microbiology labs operate: there may be an expectation from laboratory professionals that they will (indirectly) collaborate with clinicians in surveillance work and perform tests that generate data. However well-established rules in the system do not allow an easy negotiation of new rules. This may be because laboratories in LMICs are rarely run by microbiologists or people with a medical background, which may be perceived by clinicians as problematic. This issue is intensified by the ways results are communicated, since lab professionals have limited authority and ‘cannot exert a bit of weight when giving advice on what antibiotics should be used’ [P7, member of DHSC TAG].
The analysis suggests that lab professionals face tensions as they reach-out to clinical staff in other professional spaces (e.g. hospital wards or clinics). At the same time, AMR guidelines and policies are being developed, but these are not sufficient in circumventing this problem. AMR surveillance as an emerging practice creates new possibilities for action within and across professions. Yet the various actors encounter uncertainty about how to navigate the various possibilities and, as a consequence, experience lack of clarity about how their role inter-relates with other professionals.
Tension #7: AMR surveillance relies on motivated and skilful professionals, but laboratory professionals tend to perceive themselves as under-skilled
Almost all the interviewees referred to the technical skills required to perform the AMR susceptibility testing and suggested that many lab professionals are likely to face challenges in this task, mainly due to variations in their formal training and studies (local and national systems, tension between subject and tools).
Interviewees pointed to inadequate and sometimes non-existent training as another factor contributing to the poor functioning of AMR surveillance systems. Another concern expressed was related to the low retention rates of laboratory professionals, which is linked to low salaries and poor motivation (national system, tension between subject and tools). Furthermore, most lab staff is committed to tasks related to other diseases (i.e. malaria, HIV), resulting in managers not being able to allocate resources to AMR surveillance (local and national system, tension between tools and rules). These are viewed as major barriers in strengthening capacity – ‘it all comes back to resourcing: if you are a lab technician working in a poorly resourced lab … you will still feel undervalued and under-represented … ’ [P22, member of DHSC TAG].
There are other challenges that also have to be overcome: in many LMICs, laboratory work is neither an attractive nor a valued career choice; a considerable number of trained laboratory professionals leave the public health sector to work in the private sector where pay and conditions are better; and new diseases and the rising demands for new lab diagnostics require continued development of workforce with specialist knowledge and skills. These opportunities are limited in these settings (Littlejohn, Charitonos, and Kaatrakoski Citation2019).
Concluding remarks
The paper examined tensions that laboratory professionals in LMICs may encounter when engaging in a new work practice, namely the surveillance of AMR. It outlined recent developments in this field and provided empirical evidence to frame the emergent conditions for knowledge-based work around this practice. The study is situated in the context of AMR surveillance in LMICs, where new actors and tools have been introduced, but the context is not yet ‘stabilised’ (Gherardi Citation2009). The study identified seven tensions that serve to frame implications for developing professional programmes. These are discussed in the paragraphs that follow.
The analysis highlighted that AMR is an emerging global challenge, hence practices are not stable and homogeneous and lab professionals are not yet in a position to handle and engage adequately with knowledge about AMR in their field. In this context of professional work, professionals are often exposed to new, multiple and contradictory demands resulting in some of them finding it difficult to keep-up with developments in their field. New practices are emerging, often in unpredictable ways, and create a ‘fluid’ and dynamic environment. As such ‘traditional’ professional development programmes that focus on the delivery of content through workshops or courses are insufficient in dealing with such a complex problem. Instead professional programmes should be tied with practice at the workplace to allow professionals to learn new forms of knowledge and practice on an ongoing basis (Hager Citation2004; Hadwin, Järvelä, and Miller Citation2011; Illeris Citation2011). This is not to claim that all professional development programmes to date are problematic or redundant. However, a case is made here to consider professional learning as a more systemic concern to enable participation in active and critical ways, situated within professionals’ own workplace structures and resources in their environment rather than maintaining a focus on what individuals do or which content to deliver in those programmes.
The tensions identified through CHAT analysis reveal opportunities for professionals that may drive learning. A key recommendation from this study is related to encouraging inter-sectoral working (e.g. exchange of data between human health and animal health labs). This, alongside the creation of new mediating roles (e.g. One Health officer, Surveillance officer) and the formation of new collaborations and partnerships (e.g. reference labs with sentinel sites within a country, reference labs across countries), are important in the organisation of professional work around AMR. CPD programmes in this field should highlight new knowledge objects and tools that are essential in the surveillance activity across sectors and systems, such as the creation and interpretation of surveillance data. Whilst maintaining an overview across local, national and global systems is necessary in CPD programmes, they should place particular attention at the local workplace as a key activity setting to ensure that local systems function well to enable them to produce the high-quality data that forms the basis of those systems.
CPD programmes should further stimulate inter-system working by supporting networks of professionals to appreciate their position in the local, national and global system. For example, it is important to consider the distinct ways in which professionals in specific roles (e.g. clinician, lab assistant, policy maker) can get involved in decision-making based on the surveillance data (e.g. in clinical treatments, public health policy) or how this data is shared across disciplines and professional settings, including the microbiology labs. Programmes should also support professionals to become familiar with how their role is situated in, and contributes to, professional networks in the surveillance systems. For learning to be effective, practitioners need to see their role and work in relation to extended contexts and networks and familiarise themselves with collective knowledge around AMR surveillance.
Another important aspect in the provision of professional learning in this context is to consider the role of professional expertise (Edwards Citation2010), namely that professionals involved in AMR surveillance are increasingly required to work with others who bring their own expertise to the practice of surveillance. The analysis revealed mistrust between roles related to how they know what is known (e.g. clinicians in empirical treatment), how knowledge is distributed and how knowledge receives legitimacy between involved professionals (e.g. which antibiotics to prescribe). CPD programmes should support workers to develop confidence in their own specific domains but also to build trust and value ways of working and knowing of others. A critical awareness of the wider networks of knowledge in this field through inter-professional work is needed in dealing with a problem as complex as AMR.
The analysis further revealed existing rigid workplace structures and rules that hinder new AMR surveillance practice. Addressing such issues at the local, institutional level may encourage organisations involved in surveillance activity reviewing their policies and existing practices and reflecting on how work is structured, considering roles involved in key surveillance practices and introducing alternative processes in the work environment that may support new practices. Such a process of ‘reflecting together on work issues generates considerable collective learning that may contribute to the development not just of the individuals concerned but to the enterprise itself’ (Boud and Hager Citation2012, 25). In doing this, the organisation will support its workers in developing a critical new skillset which relates to working together across professional networks to keep considering complex areas of work and evolving knowledge and professional cultures.
In conclusion, we are currently witnessing a growing interest to aspects of professional work as part of capacity strengthening programmes in resource-limited environments, particularly around global challenges associated with expanding and evolving knowledge fields. The findings of this study highlight the need to avoid simplified conceptions about professional programmes that take the form of ‘training’ and to develop learning that will align with changes in the field, workplace structures and professional roles. Responding to Enqvist-Jensen (Citation2018) call for more research on knowing and learning in navigating fluid epistemic spaces, this paper offered an empirical account of how learning can support professionals in the AMR field as it evolves. This is particularly important for initiatives that are set to address challenges to global health.
Acknowledgements
The authors wish to thank all the participants of this study. Thanks also to Mott Macdonald and the UK Government Department for Health and Social Care for funding this study and the support they provided in the recruitment of participants. We are also grateful to Mr. Tim Seal, Senior Project Manager at the Open University, for his work on project management and support in data collection.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
Notes
1 The Fleming Fund is a £265 million UK aid investment to tackle antimicrobial resistance in low- and middle-income countries around the world. The programme is managed by the UK Department of Health and Social Care, in partnership with Mott MacDonald, the Fleming Fund Grants Management Agent.
3 See e.g. the GLASS Resource Centre https://www.who.int/glass/resources/en/
References
- Boud, D., and P. Hager. 2012. “Re-thinking Continuing Professional Development Through Changing Metaphors and Location in Professional Practices.” Studies in Continuing Education 34 (1): 17–30. doi: 10.1080/0158037X.2011.608656.
- Charitonos, K., A. Littlejohn, H. Kaatrakoski, A. Fox, V. Chaudhari, T. Seal, and N. Tegama. 2019. “Technology-Supported Capacity Building on AMR Surveillance: Findings from the Pilot Phase.” p94. Internal Report, The Open University. 11 October 2019.
- Edwards, A. 2010. Being an Expert Professional Practitioner: The Relational Turn in Expertise. Dordrecht: Springer.
- Engeström, Y. 1987. Learning by Expanding: An Activity-Theoretical Approach to Developmental Research. Helsinki: Orienta-Konsultit.
- Engeström, Y. 2005. Developmental Work Research: Expanding Activity Theory Into Practice. Berlin: Lehmanns Media.
- Engeström, Y. 2015. Learning by Expanding: An Activity-Theoretical Approach to Developmental Research. 2nd ed. Cambridge: Cambridge University Press.
- Enqvist-Jensen, C. 2018. “Navigating Fluid Epistemic Spaces: Emerging Challenges for Student Knowing and Learning in Public International law.” Studies in Continuing Education 40 (3): 257–272. doi:10.1080/0158037x.2018.1445984.
- Fenwick, T., M. Nerland, and K. Jensen. 2012. “Sociomaterial Approaches to Conceptualising Professional Learning and Practice.” Journal of Education and Work 25 (1): 1–13. doi:10.1080/13639080.2012.644901.
- Fuller, A., A. Munro, and H. Rainbird. 2004. “Conclusions.” In Workplace Learning in Context, edited by H. Rainbird, A. Fuller, and A. Munro, 299–306. New York: Routledge.
- Fuller, A., and L. Unwin. 2003. “Learning as Apprentices in the Contemporary UK Workplace: Creating and Managing Expansive and Restrictive Participation.” Journal of Education and Work 16 (4): 407–426.
- Gherardi, S. 2009. “Knowing and Learning in Practice-Based Studies: an Introduction.” The Learning Organization 16 (5): 352–359. doi:10.1108/09696470910974144.
- Hadwin, A. F., S. Järvelä, and M. Miller. 2011. “Self-regulated, Co-regulated, and Socially Shared Regulation of Learning.” In Educational Psychology Handbook Series. Handbook of Self-Regulation of Learning and Performance, edited by B. J. Zimmerman and D. H. Schunk, 65–84. New York, NY: Routledge/Taylor & Francis Group.
- Hager, P. 2004. “Lifelong Learning in the Workplace? Challenges and Issues.” Journal of Workplace Learning 16: 22–32. doi:10.1108/13665620410521486.
- Illeris, K. 2011. “Workplaces and Learning.” In The SAGE Handbook of Workplace Learning, edited by M. Malloch, L. Cairns, K. Evans, and B. N. O’Connor, 32–45. London: SAGE.
- Jensen, K., M. Nerland, and C. Enqvist-Jensen. 2015. “Enrolment of Newcomers in Expert Cultures: An Analysis of Epistemic Practices in a Legal Education Introductory Course.” Higher Education 70 (5): 867–880. doi:10.1007/s10734-015-9872-z.
- Leont’ev, A. N. 1978. Activity, Consciousness, and Personality. Trans. M.J. Hall. Englewood Cliffs: Prentice-Hall.
- Littlejohn, A., K. Charitonos, and H. Kaatrakoski. 2019. “The Role of Professional Learning in Addressing Global Challenges: Tensions and Innovations Associated With AMR.” Frontiers in Education 4: 73–12.
- Littlejohn, A., N. Hood, C. Milligan, and P. Mustain. 2016. “Learning in MOOCs: Motivations and Self-Regulated Learning in MOOCs.” Internet Higher Educ 29: 40–48. doi:10.1016/j.iheduc.2015.12.003.
- Littlejohn, A., and A. Margaryan. 2014. “Technology-enhanced Professional Learning.” In International Handbook of Research in Professional and Practice-Based Learning, edited by S. Billett, C. Harteis, and H. Gruber, 1187–1212. Dordrecht: Springer.
- Markauskaite, L., and P. Goodyear. 2017. Epistemic Fluency. Innovation, Knowledgeable Action and Actionable Knowledge. Dordrecht: Springer. doi:10.1007/978-94-007-4369-4.
- Nerland, M. 2018. “Knowledge Practices and Relations in Professional Education.” Studies in Continuing Education 40 (3): 242–256.
- Nerland, M., and K. Jensen. 2014. “Learning Through Epistemic Practices in Professional Work: Examples from Nursing and Computer Engineering.” In Reconceptualizing Professional Learning, edited by T. Fenwick and M. Nerland, 25–37. London: Routledge.
- Opintan, A. J., J. M. Newman, E. R. Arhin, E. S. Donkor, M. Gyansa-Lutterodt, and W. Mills-Pappoe 2015. “Laboratory-based Nationwide Surveillance of Antimicrobial Resistance in Ghana.” Infection and Drug Resistance 8: 379–316.
- Sayed, S., W. Cherniak, M. Lawler, S. Y. Tan, W. El Sadr, N. Wolf, S. Silkensen, et al. 2018. “Pathology and Laboratory Medicine in low-Income and Middle-Income Countries 2 Improving Pathology and Laboratory Medicine in low-Income and Middle-Income Countries: Roadmap to Solutions.” The Lancet 391: 1939–1939.
- Schatzki, T. R. 2001. “Practice Theory.” In The Practice Turn in Contemporary Theory, edited by T. R. Schatzki, K. Knorr-Cetima, and E. von Savigny, 1–14. New York: Routledge.
- Webster-Wright, A. 2009. “Reframing Professional Development Through Understanding Authentic Professional Learning.” Review of Educational Research 79 (2): 702–739.
- WHO. 2015. Global Action Plan on Antimicrobial Resistance. ISBN: 9789241509763. Accessed February 3 2020. https://www.who.int/antimicrobial-resistance/global-action-plan/en/.
- WHO. 2020a. Antimicrobial Resistance. World Health Organisation. Accessed February 2 2020. https://www.who.int/antimicrobial-resistance/en/.
- WHO. 2020b. Essential Medicines and Health Products. Accessed February 2 2020. https://www.who.int/medicines/areas/rational_use/AMR_Surveillance/en/.
- Wilson, M. L., K. A. Fleming, M. Kuti, L. M. Looi, N. Lago, and K. Ru. 2018. “Access to Pathology and Laboratory Medicine Services: a Crucial gap.” The Lancet 391 (10133): 1927–1938.