ABSTRACT
Music therapy is increasingly being used as an intervention for stress reduction in both medical and mental healthcare settings. Music therapy is characterized by personally tailored music interventions initiated by a trained and qualified music therapist, which distinguishes music therapy from other music interventions, such as ‘music medicine’, which concerns mainly music listening interventions offered by healthcare professionals. To summarize the growing body of empirical research on music therapy, a multilevel meta-analysis, containing 47 studies, 76 effect sizes and 2.747 participants, was performed to assess the strength of the effects of music therapy on both physiological and psychological stress-related outcomes, and to test potential moderators of the intervention effects. Results showed that music therapy showed an overall medium-to-large effect on stress-related outcomes (d = .723, [.51–.94]). Larger effects were found for clinical controlled trials (CCT) compared to randomized controlled trials (RCT), waiting list controls instead of care as usual (CAU) or other stress-reducing interventions, and for studies conducted in Non-Western countries compared to Western countries. Implications for both music therapy and future research are discussed.
Introduction
Stress is a well-known risk factor for the onset and progression of a range of physical and emotional problems, such as cardiovascular diseases, cancers, anxiety disorders, depression, and burnout (American Psychological Association [APA], Citation2017; Australian Psychological Society [APS], Citation2015; Steptoe & Kivimäki, Citation2012). To cope with stress and the demands of today's society, millions of people over the world use tranquilizing medications, which have a lot of negative contraindications and side effects, including substance dependence and abuse (Bandelow et al., Citation2015; Olfson et al., Citation2015; Puetz et al., Citation2015; World Health Organization [WHO], Citation2010). Therefore, it is important to examine the effects of non-pharmacological therapeutic interventions for the prevention and management of stress (de Witte et al., Citation2020a; Kamioka et al., Citation2014; Martin et al., Citation2018; Raglio et al., Citation2015).
For decades and all over the world music has been used to provide calmness and relaxation. These stress reducing qualities are the most widely studied effects of music (Chanda & Levitin, Citation2013; de Witte et al., Citation2020a; Juslin & Västfjäll, Citation2008; Koelsch, Citation2015; Mehr et al., Citation2019). Therefore, music therapy interventions are increasingly being used to reduce stress and enhance the well-being of clients across a variety of clinical populations (Agres et al., Citation2020; Bainbridge et al., Citation2020; Juslin & Västfjäll, Citation2008; Kemper & Danhauer, Citation2005; Koelsch, Citation2012, Citation2015; Landis-Shack et al., Citation2017; Thaut & Hoemberg, Citation2014).
Music therapy is specifically characterized by using the specific qualities of music in a therapeutic relationship with a music therapist. This distinguishes music therapy from other music interventions, mostly offered by medical or healthcare professionals and referred to as music medicine (Agres et al., Citation2020; Bradt et al., Citation2013b; de Witte et al., Citation2020a; Gold et al., Citation2011; Magee, Citation2019). The body of research on music therapy is much smaller compared to the amount of research on music listening interventions. Our previous meta-analytic review (de Witte et al., Citation2020a) was focused on the effects of music interventions in general and included mainly music listening interventions. In none of these studies a trained music therapist was involved.
In order to integrate the available knowledge on the effects of music therapy on stress, we conducted a systematic review and meta-analysis of quantitative studies testing the effects of music therapy on both physiological and psychological stress-related outcomes in mental and medical healthcare settings.
The influence of music on the stress response
Stress can be regarded as the quality of an experience, produced through a person-environment transaction that may result in physiological or psychological distress (Aldwin, Citation2007). Responses to stress can be related to both increased physiological arousal and specific emotional states, while the underlying systems of those responses regulate and affect each other during stress (e.g., de Witte et al., Citation2020a; Linnemann et al., Citation2017; McEwen & Gianaros, Citation2010). The stress reducing effect of music therapy interventions is explained by music itself as well as the continuous attunement of music by the music therapist to the individual needs of a patient.
Music listening is strongly associated with stress reduction by the decrease of physiological arousal as indicated by reduced cortisol levels, lowered heart rate, and decreases in mean arterial pressure (e.g., Burrai et al., Citation2016; Koelsch et al., Citation2016; Kreutz et al., Citation2012; Linnemann et al., Citation2015). Music can also reduce negative emotions and feelings, such as subjective worry, state anxiety, restlessness or nervousness (Akin & Iskender, Citation2011; Cohen et al., Citation1983; Pittman & Kridli, Citation2011; Pritchard, Citation2009), and increase positive emotions and feelings, such as happiness (Jäncke, Citation2008; Juslin & Västfjäll, Citation2008). This is in line with studies showing that music modulates activity in brain structures, such as the amygdala and the mesolimbic reward brain system, which are known to be involved in emotional and motivational processes (Blood & Zatorre, Citation2001; Koelsch, Citation2015; Koelsch et al., Citation2016, Citation2016; Levitin, Citation2009; Moore, Citation2013; Salimpoor et al., Citation2013; Zatorre, Citation2015). Furthermore, it is assumed that the systematic application of music in therapy in response to the needs of the patient(s) can strengthen the impact of music (Agres et al., Citation2020; Bradt & Dileo, Citation2014). In addition, empirical evidence shows that music activities in a group may result in synchronization among group members, which leads to positive feelings of togetherness and bonding (Linnemann et al., Citation2016; Tarr et al., Citation2014). These feelings of togetherness and bonding may be explained by the release of the neurotransmitters endorphin and oxytocin, which both play an important role in the defensive response to stress (e.g., Amir et al., Citation1980; Dief et al., Citation2018; Myint et al., Citation2017). Lastly, music listening can help to lower stress levels through its quality to provide ‘distraction’ from stress-increasing feelings or thoughts (Bernatzky et al., Citation2011; Chanda & Levitin, Citation2013).
Music therapy
Music therapy can be defined as the clinical and evidence-informed use of music interventions to accomplish individualized goals within a therapeutic relationship in order to achieve physical, emotional, mental, social and cognitive needs (Aalbers et al., Citation2019; Agres et al., Citation2020; American Music Therapy Association [AMTA], Citation2018; de Witte et al., Citation2020a). Music therapy has been applied as a therapeutic intervention in a wide spectrum of health care contexts, such as mental health care, forensic care, nursing homes, rehabilitation, and oncology (e.g., Agres et al., Citation2020; Kamioka et al., Citation2014; Martin et al., Citation2018). Although the term ‘music therapy’ sometimes refers to any kind of use of music as an intervention in health care settings, music therapy should be offered by a trained music therapist, who is a licensed and qualified therapist with the required knowledge in psychology, medicine, and music (Agres et al., Citation2020; AMTA, Citation2018; Bradt et al., Citation2015; Magee, Citation2019).
Music therapists use the unique qualities of music (e.g., melody, rhythm, tempo, dynamics, pitch) within the therapeutic relationship to access patient's emotions and memories, to address social experiences or influence behavior (Bruscia, Citation1987; Wheeler, Citation2015). This specific kind of responsivity to the patient's needs can be regarded as the key competencies of the music therapist, referring to the processes that take place between therapist and patient supporting coordination, empathy and shared perspectives (Agres et al., Citation2020). More specifically, during music therapy the music therapist attunes to the patient by adjusting the music created as an immediate response to the patient's needs (Aalbers et al., Citation2019; Magee, Citation2019).
To work on patient-therapist attunement, the music therapist synchronizes with the patient moment-by-moment, which may be considered as a mirroring technique. This means that the (musical) actions of the music therapist and the patient can become simultaneous and regulated through time, yielding a similar expression in movement, matching pulse, rhythm, dynamics and/or melody (Aalbers et al., Citation2019; Bruscia, Citation1987; Schumacher & Calvet, Citation2008). For example, the music therapist may influence patients’ perceived stress during musical improvization by synchronizing with the patient's music-making, subsequently changing the musical expression by playing slower and less loudly. This specific way of patient-therapist attunement is commonly used in music therapy practice and refers to the so-called Iso Principle (e.g., Altshuler, Citation1948; Heiderscheit & Madson, Citation2015). Literature shows that the tempo and loudness are important for the experienced intensity of the music (Gabrielsson & Lindström, Citation2010), and music with a slow steady rhythm may provide stress reduction by altering inherent body rhythms, such as heart rate (Thaut et al., Citation1999; Thaut & Hoemberg, Citation2014). The music therapist uses several types of interventions, which can be offered to a group of patients as well as individually. The number, frequency, and duration of the music therapy session may vary widely, and depend on the targeted outcome, patients’ preferences, and/or the setting in which the music therapy is offered (Agres et al., Citation2020; AMTA, Citation2018). Furthermore, music therapy interventions can be subdivided in two broad categories: active and receptive interventions (Magee, Citation2019; Magee et al., Citation2017; Wheeler, Citation2015).
Active interventions involve the patient doing something with the music during the music therapy sessions, such as musical improvization, composing music or songs, movement to music, or singing or vocalizing. According to both literature and clinical practice, it seems that musical improvization is the most used intervention within music therapy, meaning that patient(s) and therapist improvize on musical instruments they have chosen and play together freely or with a given structure (Gold et al., Citation2009; Wigram, Citation2004). In receptive music therapy interventions, the patient is not actively making music, but rather responds to music provided by the music therapist, such as listening to live or prerecorded music (Bruscia, Citation1998; Magee, Citation2019; Wheeler, Citation2015). The patient listens to the music and may process verbally their own emotions and/or experiences. During both active and receptive music interventions music therapists make specific use of the unique qualities of music (also known as ‘musical components’), such as rhythm, pitch, tempo, dynamics, melody and harmony, to facilitate and promote personal contact, communication, learning, mobilization, expression and other relevant goals (Agres et al., Citation2020; Câmara et al., Citation2013; Taets et al., Citation2019; Thaut & Hoemberg, Citation2014; Wheeler, Citation2015).
Summarized, whereas music medicine does not involve a personal therapeutic process, music therapy requires such a process, characterized by personally tailored music interventions initiated by a trained/qualified music therapist (de Witte et al., Citation2020a; Leubner & Hinterberger, Citation2017). These music therapy interventions can be divided in receptive music therapy interventions (music listening) or active music therapy interventions (live music-making), and are specifically characterized by musical attunement, facilitated by the music therapist, which distinguishes music therapy from other music interventions.
Music therapy versus music medicine
Research on music therapy is fast-growing (de Witte et al., Citation2020a). The effects of music listening interventions, such as ‘music medicine’, are mainly caused by the general influence of music on the stress response, whereas the effects of music therapy may also be explained by the therapeutic relationship through patient-therapist attunement by the use of music. Dileo (Citation2006) stated that music therapy is more effective than ‘music medicine’ interventions, and attributed this difference to the fact that music therapists individualize their interventions to meet patients’ specific needs (Bradt et al., Citation2010; Dileo, Citation1999, Citation2006).
In a Cochrane review of Bradt et al. (Citation2016) it was shown that ‘music medicine’ interventions and music therapy were equally effective in decreasing (state) anxiety. Bradt et al. (Citation2015) compared ‘music medicine’ with music therapy, and also found that both types of interventions were equally effective for anxiety and stress reduction, although 77.4% of the participants expressed a preference for music therapy for future treatments. This patient's preference for music therapy was related to quality of therapeutic relationships, interactive music making and the possibility of emotional expression, which is precisely what music therapy distinguishes from music listening interventions (Bradt et al., Citation2015; Gutgsell et al., Citation2013).
In our previous meta-analytic review on Randomized Controlled Trials (RCTs) examining the effects of music interventions on stress-related outcomes (de Witte et al., Citation2020a), we showed that music therapy did have at least as much effect on physiological stress-related outcomes (d = .423) as ‘music medicine’ (d = .379). However, only 7 studies on music therapy were included against 54 studies examining music medicine. Therefore, findings on music therapy were compromised by low generalizability and lack of statistical power to examine factors that might affect the effectiveness of music therapy by means of moderator analyses. Notably, most effectiveness studies on music therapy are quasi-experimental, because it is often difficult to meet the requirements for randomization and/or masking procedures (Bradt et al., Citation2013b; de Witte et al., Citation2020a; Magee et al., Citation2017).
The present study
The present study is a systematic review and meta-analysis on the effects of music therapy on both physiological stress-related arousal (e.g., blood pressure, heart rate, hormone levels) and psychological stress-related experiences (e.g., state anxiety, restlessness or nervousness) in clinical health care settings. In our previous meta-analysis, we examined the effect of music interventions on stress-related outcomes. The included studies primarily used prerecorded music offered by medical professionals, whereas music therapy involves a trained music therapist who is responsive to the needs of the patient and can influence emotions and/or behavior of the patient by the use of music.
In the present meta-analysis, we included both RCTs and quasi-experimental designs with a control condition (Clinical Controlled Trials [CCT]), accounting for the effect of study design and quality in moderator analyses. The inclusion of quasi-experimental studies, which have been conducted under clinically representative conditions, increases external validity of meta-analytic findings and substantially increases statistical power of a meta-analysis (Shadish et al., Citation2002; Shadish et al., Citation2008).
The methodology of the present meta-analytic study is in line with our recent three-level meta-analysis (de Witte et al., Citation2020a), in which 104 randomized controlled trials were included. Results showed a significant small-to-medium effect of music interventions on physiological stress-related outcomes (d = .380; 61 trials), and a medium effect of music interventions on psychological stress-related outcomes (d = .545; 79 trials), indicating that groups receiving music intervention benefited more than the comparison groups. In the present meta-analysis, we examine the overall effect of music therapy on stress reduction, accounting for differences in physiological and psychological stress-related outcomes, and we aim to gain more insight into study, sample, outcome and intervention characteristics that might moderate the effects of music therapy on stress reduction.
Methods
Inclusion criteria
For the current meta-analysis, multiple inclusion criteria were formulated. First, only Randomized Controlled Trials (RCTs) and Clinical Controlled Trials (CCTs) that examined the effect of music therapy on the experience of stress and/or state anxiety were included. The type of intervention concerned important inclusion criteria for this meta-analysis. Only studies that offered music therapy by an educated and certified music therapist were included in this meta-analysis. Outcome measures related to quality of life (QoL) or pain were excluded, because in this study only the primary outcome measures of stress were included. The physiological effects of stress had to be measured by heart rate (HR), heart rate variability (HRV), blood pressure and hormone levels. The psychological effects of stress had to be measured by self-report instruments aiming at ‘stress' or ‘state anxiety’. Second, studies examining people with dementia or participants younger than 18 years of age were excluded. Although many studies showed cognitive and emotional benefits in dementia patients when they sing or listen to familiar songs (Särkämö et al., Citation2008, Citation2014), these findings are not directly related to ‘stress reduction’. In addition, the stress measurement instruments which are used in the included studies are not used in studies examining people with dementia or young participants.
Selection of the studies
All randomized controlled trials (RCTs) and clinical controlled trials (CCTs) available until the 8th of May 2019 that met the inclusion criteria were included in this meta-analytic review. Multiple systematic searches were performed with the help of an independent medical librarian, as librarian engagement is significantly associated with higher quality of reported search strategies (Rethlefsen et al., Citation2015). We conducted a computer-based search of the psychological and medical electronic literature databases, including Medline, Academic Search Complete, Cochrane Library, Web of Science, Embase, Wiley Online Library, Springerlink, PubMed, PiCarta, Academic Search Premier, ScienceDirect, PsycINfo and Google Scholar. The search string comprised three elements: a music therapy element, a stress-related outcome element and a study design element. For the music therapy element, the following keywords were used: ‘music therapy’, ‘musical therapy’ or ‘music-based therapy’. For the stress-related outcome element, the following keywords were used: ‘stress’, ‘anxiety’, ‘arousal’, ‘psychological stress,’ ‘occupational stress’, ‘physiological stress’, ‘mental suffer’, ‘anguish’, ‘hypertension,’ ‘relaxation’, ‘heart rate,’ ‘blood pressure’, ‘nervousness’, ‘cortical vigilance’, ‘distress’, ‘cortisol’, ‘intravascular pressure’, ‘vascular pressure’ or ‘STAI’. Concerning the study design element, the keywords: ‘randomized controlled trial’, ‘randomised controlled trial’, ‘clinical controlled trial’, ‘randomised’, ‘randomized’, ‘ RCT’, ‘review’ or ‘meta-analysis’ were used. Furthermore, reference sections of review – and meta-analytic articles about the effect of music (therapy) interventions on stress-related outcomes were inspected for qualifying studies. The search protocol of this meta-analytic review is registered at the international prospective register of systematic reviews (ref.no. CRD42020160222).
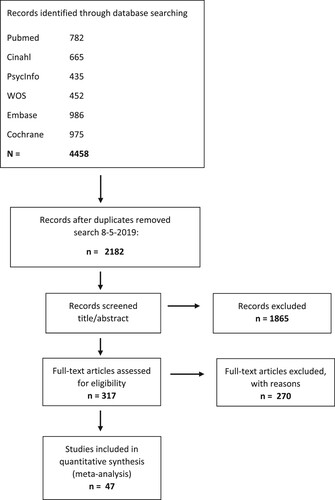
The initial search resulted in 2.182 individual studies and was conducted by an independent librarian and the first author. The first selection on title and abstract resulted in 317 individual studies that were, posteriorly, full text screened based on the inclusion criteria. Finally, 47 studies met all the inclusion criteria (see ). All the steps of the selection process were conducted by two different authors, who selected the studies blindly from each other. Concerning the selection conflicts, a third author was involved and made the final decision. Table A1 provides an overview of the included studies and their main characteristics (see Appendix 1).
Figure 1. Flow chart of the search results.
Coding and moderators
The included studies were coded by the first and second author using a coding sheet according to the guidelines of Lipsey and Wilson (Citation2001). Stress can be considered as the dependent variable and was coded into physiological or psychological stress-related outcomes, resulting in one meta-analysis. Multiple variables with a potential moderating effect on the relation between music therapy and stress were identified. These moderators were divided into outcome-, study-, sample-, and intervention characteristics.
Regarding the psychological stress-related outcomes, it was coded whether the psychological outcomes were assessed by means of questionnaires measuring stress or (state) anxiety. State anxiety can be seen as a psychological stress-related outcome, because many studies (e.g., de Witte et al., Citation2020a; Hook et al., Citation2008; Ng et al., Citation2016; Zhang et al., Citation2014) considered state anxiety to be a result of stress and outcome measures related to state anxiety or stress. Therefore, in the literature these concepts are used interchangeably (Bradt & Dileo, Citation2014; Lazarus & Folkman, Citation1984; Ozer et al., Citation2013; Pittman & Kridli, Citation2011; Wetsch et al., Citation2009). This is in line with the results of our previous meta-analysis, which showed no significant differences in effect sizes between state-anxiety self-report scales (d = .553) and stress self-report scales (d = .512). In the present study, 30% of the studies used Visual Analog Scales (VAS) to measure perceived stress or state anxiety. Overall, stress is often measured by the Perceived Stress Scale (PSS) (Cohen et al., Citation1983), the Quick Mood Scale (Woodruffe-Peacock et al., Citation1998), and the Profile of Mood States (POMS) (McNair et al., Citation1981), which instruments are used in 19% of the included studies. State anxiety is predominantly measured by the state version of the Spielberger State-Trait Anxiety Inventory (STAI) (Spielberger et al., Citation1983) and the anxiety version of the Hospital Anxiety and Depression Scale (HADS-A), which are used in 45% of the included studies.
Regarding the study characteristics, we coded the design, study quality, type of setting, type of control condition and whether the study was conducted in Western- or non-Western countries. Studies with prospective group design, such as RCTs and CCTs were considered relevant for the current research. Therefore, we coded study design as RCT when participants were allocated to treatment conditions through randomization (e.g., computer-generated randomization lists), and CCT design when authors did not explicitly mention randomization, or quasi-randomized studies. The quality of the study was coded as strong, moderate or weak after assessment with the ‘Quality Assessment Tool for Quantitative Studies’ (Effective Public Health Practice Project [EPHPP], Citation2009). This tool measures the quality of a study by providing a comprehensive and structured assessment of study quality (Armijo-Olivo et al., Citation2012). The EPHPP has been reported to have high content and construct validity (Jackson & Waters, Citation2005; Thomas et al., Citation2004). Low quality studies negatively affect the internal (causal conclusion) validity, which can lead to a biased estimation of the overall effect estimate (Higgins & Green, Citation2011; Zeng et al., Citation2015).
Regarding the setting in which the study was conducted, we coded whether the study was conducted in a mental healthcare setting or in a medical setting (e.g., during polyclinic treatments, before or after surgery, palliative care). Furthermore, the type of control condition was coded, because different control conditions can yield different effect sizes (Finney, Citation2000; Karlsson & Bergmark, Citation2015). We coded care as usual (CAU) when no stress-reducing intervention was offered, but patients did receive regular care within medical or mental healthcare, waiting list when there was no care or intervention offered, or stress intervention when another stress-reducing intervention was delivered, such as listening to prerecorded music, verbal support, or mindfulness-based therapy. Further, we coded whether the study was conducted in Western countries (European countries, Australia, USA, Canada, New Zealand) or whether the study was conducted in countries designated as non-Western countries (mainly Asiatic countries). The cultural environment has been shown to influence the way people respond to and cope with stress (Lonner, Citation2007; Tweed et al., Citation2004), which could influence the effect of music on stress. In our previous meta-analysis, the country in which the study was conducted just failed to reach the conventional level of statistical significance (p = 0.089), indicating that non-Western studies yielded larger effects on physiological stress-related outcomes than studies conducted in Western countries.
Sample characteristics were also coded, such as the percentage of men in each study. There are indications that men and women react differently to stress, both psychologically and physiologically, leading to substantiated gender differences in measured stress levels (Galanakis et al., Citation2009; Kajantie & Phillips, Citation2006; Verma et al., Citation2011). We also coded the average age of the participants per study, because research on occupational stress revealed several differences in stress levels between different age groups (Galanakis et al., Citation2009).
Additionally, we coded nine music therapy characteristics. First, we coded whether the music therapy was offered to an individual patient or whether it concerned a group music therapy. Empirical evidence shows that during group music therapy interventions people synchronize with each other, which evokes positive feelings of togetherness and bonding, and decreases stress levels (Linnemann et al., Citation2016; Tarr et al., Citation2014). Second, we coded music therapy interventions as ‘protocolized’ or ‘non-protocolized’. Music therapy protocols not only enable researchers to compare and replicate studies, but also to understand consistencies and strategies used by music therapists across sessions with participants (de Witte et al., Citation2020a; Vink & Hanser, Citation2018). Both structure as well as strategies used during the therapy session may have impact on participants’ outcomes, such as stress levels. Third, the quality of the intervention description was coded in reported detailed or reported briefly and poor. We considered the description of the therapy as detailed if authors mentioned or elaborated on components of a session of music therapy, such as the number or duration of the sessions, listening to live or recorded music, or which musical instruments or music therapeutic techniques were used. If authors did not explicitly report on most of the characteristics of the delivered music therapy (as mentioned above), the description was regarded as brief/poor.
Fourth, music style was divided into three categories: classical music offered by the music therapist, relaxation music, and selection of own-preference music by patient. Fifth, we made a distinction between the way the music was offered: whether the music therapist used live music alone, pre-recorded music alone or both. Sixth, with regard to music selection, we coded whether the music was selected based on the preferences of the patient, on the choice of the music therapist himself, or whether a pre-selected choice of music was offered. In some studies, in which the effects of music listening on stress-related outcomes was examined, it was advised to allow the subjects to choose the music themselves, because this may have a greater stress reducing impact (Brannon & Fiest, Citation2007; Juslin et al., Citation2008). However, our previous meta-analytic review showed that the term ‘self-selected music’ is used both in studies where the patient could bring her/his own preference music and in studies where the patient had to choose from a pre-selected list of music styles or songs (de Witte et al., Citation2020a). Therefore, we coded as such in the present study.
Seventh, we coded whether the tempo of the music was 60–90 bpm or whether the music had another tempo. Tempo can be considered as one of the most significant moderators of music-related arousal and relaxation effects. In the previous meta-analytic review (de Witte et al., Citation2020a) of the effects of music interventions on stress-related outcomes, larger effect sizes were found in music with a tempo of 60–90 bpm compared to music with another tempo. Music with a slow tempo, such as meditative music, has often been demonstrated to initiate reductions in heart rate, resulting in greater relaxation (e.g., Bernardi et al., Citation2005; Bringman et al., Citation2009; Chlan, Citation2000; Hilz et al., Citation2014; Nomura et al., Citation2013). Lastly, we coded the number of music intervention sessions and the frequency of the sessions per week. The number of interventions has been shown to be positively correlated with stress and anxiety regulation (Cassileth et al., Citation2003; Gold et al., Citation2009; Robb et al., Citation2011).
Calculation and analyses
The effect sizes were transformed into Cohen's d by using the calculator of Wilson (Citation2013) and formulas of Lipsey and Wilson (Citation2001). Negative effect sizes indicate that music therapy had a negative effect on stress-related outcomes. Most d-values were calculated based on reported means and standard deviations. To correct for pre-treatment differences, pre-test effects were subtracted from post-test effects. The effect size was coded as zero when a study reported that an effect was not significant without providing any statistics (Lipsey & Wilson, Citation2001). For both meta-analyses, the continuous moderators (age of the participants, gender of the participants, duration of the music intervention and frequency of the music intervention) were centered on their means. For categorical variables, dichotomous dummy variables were created. Extreme outliers in effect sizes were identified using box plots (Tabachnick & Fidell, Citation2013), and were winsorized (i.e., replaced by the highest or lowest acceptable score falling within the normal range) for both meta-analyses. Standard errors were estimated using formulas of Lipsey and Wilson (Citation2001).
In some of the studies, it was possible to calculate more than one effect size, as most studies reported on multiple stress-related outcome variables, multiple scales or measurement instruments. It is possible that the effect sizes from the same study are more alike than effect sizes from other studies. The assumption of independent effect sizes underlying traditional meta-analytic methods was therefore violated (Hox, Citation2010; Lipsey & Wilson, Citation2001). We applied a multilevel approach to meta-analysis in order to account for the interdependency of effect sizes (see Assink et al., Citation2015; Cheung, Citation2014; de Witte et al., Citation2020a; Houben et al., Citation2015; Spruit et al., Citation2016).
A three-level meta-analytic model was used to calculate the combined effect sizes and to perform the moderator analyses. Three sources of variance were modeled, including the sampling variance for each effect sizes (level-one), the variance between effect sizes within studies (level-two), and the variance between studies (level-three) (Assink & Wibbelink, Citation2016). The meta-analysis was conducted in R (version 3.4.3) with the metafor-package, employing a multilevel random effects model (Houben et al., Citation2015; Van den Bussche et al., Citation2009; Viechtbauer, Citation2010). This model is often used for multilevel meta-analyses and, in general, it is superior to the fixed-effects approaches used in traditional meta-analyses (Van Den Noortgate & Onghena, Citation2003). We used likelihood-ratio-tests to compare the deviance scores of the full model and the models without variance parameters on level two or three to determine if the level-two and -three variances were significant, indicating heterogeneity of effect sizes. A heterogeneous effect size distribution indicates that the effect sizes cannot be treated as estimates of a common overall effect size. In that case, we conducted moderator analyses, because the differences among effect sizes may be explained by outcome, study, sample, and/or intervention characteristics.
Publication bias
A common problem in conducting a meta-analysis is that studies with non-significant or negative results are less likely to be published than studies with positive and significant results. The studies included in this meta-analysis may therefore not be an adequate representation of all studies that have been conducted, which is called the ‘file drawer problem’ (Rosenthal, Citation1995).
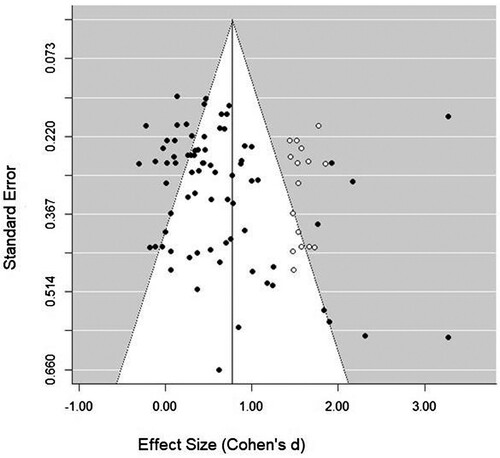
In order to check the presence of publication bias in the current meta-analysis, a trim and fill procedure was performed (Duval & Tweedie, Citation2000a, Citation2000b). In case of publication bias, the funnel plot of the distribution of effect sizes is asymmetric. We tested if effect sizes were missing on the left and right side of the distribution. Publication bias would only be likely to occur in case of non-significant or unfavorable (i.e., negative) results, resulting in left-sided funnel plot asymmetry. Right-sided funnel plot asymmetry is indicative of selection bias. We imputed estimations of effect sizes of missing studies through trim and fill analyses in the case of left or right-sided asymmetry, and subsequently computed an overall effect size that would take the influence of publication bias or selection bias into account (Duval & Tweedie, Citation2000a, Citation2000b), providing an estimate of the degree to which publication bias or selection bias might have affected the overall mean effect size.
Results
Overall effect of music therapy on stress-related outcomes
The present meta-analytic review on the effects of music therapy on both physiological and psychological stress-related outcomes, included 47 independent studies (s), reporting on 76 effect sizes (k), and a total sample of N = 2.747 subjects, of which n = 1.405 subjects in the music therapy groups, and n = 1.342 subjects in the comparison groups. Table A1 (see Appendix 1) shows an overview of the most important characteristics of the included studies. shows the overall effect of music therapy on both physiological stress-related outcomes and psychological stress-related outcomes. We found a significant medium-to-strong effect (d = .723, [.51–.94]) of music therapy on stress-related outcomes in mental healthcare and medical settings.
Table 1. Overall effects of music therapy on stress-related outcomes.
According to the trim-and-fill plot, the presence of publication bias was unlikely (see , Appendix 2), because studies were lacking on the right side of the funnel instead of the left side of the funnel. A trim and fill analysis yielded a marginally larger effect size of d = .783 compared to the observed effect size of d = .723. The likelihood ratio test showed that significant variance was present at the between-study level (level 3) and the within study level (level 2). We therefore conducted moderator analyses on type of outcome, study, sample, and music intervention characteristics to examine the effect of music intervention on physiological stress-related outcomes. The results are presented in .
Table 2. Moderator effects of music therapy on stress-related outcomes.
Results of moderator analyses of music therapy on stress-related outcomes
Outcome characteristics. Both the domain of outcomes (physiological or psychological stress-related outcomes) and the type psychological measure (stress or state-anxiety measurements) did not influence the effects of music therapy on stress-related outcomes.
Study characteristics. Firstly, the strongest effects of music therapy on stress-related outcomes were measured by CCTs (d = 1.449, [1.01–1.89]) compared to RCTs (d = .555, [.35–.76]). Secondly, the continent in which the study was conducted did also moderate the overall effect. Studies from non-Western countries had a stronger influence on the overall effect of music therapy on stress-related outcomes (d = 1.306, [.79–1.82]) compared to studies from Western countries (d = .611, [.39–.83]). Thirdly, a significant moderating effect was found for type of control condition. Studies with a waiting list control condition yielded a larger effect (d = 1.415, [.95–1.88]) than studies with CAU (d = .561, [.33–.79]) or another stress-reducing intervention (d = .594, [.29–.90]). The clinical setting in which the study was conducted, did not moderate the effect. No significant differences were found between the effects of music therapy on stress-related outcomes in mental health care settings and medical settings. Furthermore, we observed that study quality moderated the overall effect with low quality studies (d = 1.056, [.71–1.40]) yielding larger effects compared to studies with a moderate (d = .589, [.28–.90]) or strong (d = .444, [.02–.87]) study quality.
Sample characteristics. The age (d = .718, [.50–.94]) and gender (d = .728, [.51–.94]) of the samples did not show to have a moderating effect on stress symptoms.
Intervention characteristics. Music tempo between 60 and 90 bpm yielded a larger effect (d = .900 [.54–1.26]) compared to music with no specific tempo (d = .631 [.37–.90]). Similarly, more than one session of music therapy had a larger effect (d = .894 [.56–1.23]) than one session (d = .594 [.17–1.02]). The effect size of preselected choice was larger (d = 1.059 [.66–1.46]) than music selection by the music therapist (d = .695 [.37–1.02]) and by the patient (d = .766 [.47–1.06]). With respect to music style, relaxation had a greater effect (d = .826 [.49–1.16]) compared to own preference music (d = .688 [.40–.97]) and classical music (d = .562 [−.07 to 1.19]). Additionally, group music therapy yielded a larger effect (d = .927 [.54–1.32]) than individual music therapy (d = .679 [.41–.95]). However, due to the small number of studies in certain categories (see ), these differences were not statistically significant, and further studies are necessary to estimate these differences with more precision. Other differences had similar effect sizes (e.g., treatment protocol (d = .683 [.33–1.04]) or not (d = .747 [.48–1.02]); detailed intervention description (d = .775 [.52–1.03]) or brief/poor description (d = .637 [.31–96]); and the way the music therapist induced the music – live music (d = .726 [.46–.99]), prerecorded music (d = .664 [.26–1.07]) and both (d = .767 [.37–1.16]). Lastly, the effect of frequency of sessions per week (d = .746 [.49–1.01]) was not significant.
Discussion
Overall effects
Overall, we found a significant medium-to-strong effect (d = 0.723, [0.51, 0.94]) of music therapy on stress-related outcomes, indicating that participants receiving music therapy benefited more than controls. We conclude that music therapy is effective in reducing stress-related symptoms in both mental healthcare and medical settings. In our previous meta-analytic review, we found positive small-to-medium effects of music interventions on stress-related outcomes (see for more details: de Witte et al., Citation2020a), while the findings of the present study demonstrate that music therapy yields a medium-to-strong effect on stress reduction. The difference in the strength of overall effect sizes may be explained by the different way both types of interventions are offered. The active involvement of a music therapist who is specifically trained to tailor interventions to the needs of patients and their musical preferences might give a reasonable explanation for the larger effect size for music therapy compared to music interventions (Bradt & Dileo, Citation2014; Dileo, Citation1999, Citation2006; Magee, Citation2019; Magee et al., Citation2017; Stegemann et al., Citation2019). Music therapists are especially trained to deliver music therapy sessions to meet participants/patients’ needs at the individual or group level (Rafieyan & Ries, Citation2007).
The overall findings of the present meta-analysis are consistent with the findings of previous reviews and/or meta-analyses on the effects of music therapy on stress- and anxiety-related outcomes (Bradt & Dileo, Citation2014; Bradt et al., Citation2013a; Bradt et al., Citation2013b; Bradt et al., Citation2016; Carr et al., Citation2013; de Witte et al., Citation2020a; Gold et al., Citation2009; Kamioka et al., Citation2014). In addition, the promising results of music therapy established in the current meta-analysis are in line with the findings of previous systematic reviews and meta-analyses on the effects of music interventions on the reduction of stress and/or (state) anxiety (Bradt & Dileo, Citation2014; Bradt et al., Citation2013a; Bradt et al., Citation2013b; Bradt et al., Citation2016; de Witte et al., Citation2020a; Gillen et al., Citation2008; Kim et al., Citation2015; Pelletier, Citation2004; Rudin et al., Citation2007).
Both the present meta-analysis and previous reviews show a growth in controlled clinical studies testing the effects of music therapy and/or music interventions on stress-related outcomes, which is important in order to formulate valid conclusions on the effects of non-pharmaceutical interventions for stress reduction (Casey, Citation2017; de Witte et al., Citation2020a). The demand for more non-pharmaceutical interventions, such as music therapy, may be explained by the increasing awareness of the negative side effects of tranquilizing medication, such as substance dependence and abuse (Casey, Citation2017; World Health Organization [WHO], Citation2010). Although a considerable number of people around the world use tranquilizing medications to cope with daily life stressors or anxiety (e.g., Bandelow et al., Citation2015; Olfson et al., Citation2015; Puetz et al., Citation2015), previous studies show no convincing evidence for the short-term effectiveness of pharmacological treatment in the reduction of stress-related problems (Donovan et al., Citation2019; Olfson et al., Citation2015).
Effect moderating variables
Results of the present meta-analysis indicate that moderators explain differences in the strength of the effect size. Significant larger effects were found for studies using quasi-experimental CCTs compared to RCTs. Regardless of ethical concerns about the randomization of patients, the results of RCTs are still considered to provide the most robust evidence, because RCT designs can better exclude alternative explanations for established intervention effects than non-randomized designs. Selection bias in non-randomized effect studies can lead to overestimations of treatment effects (Page et al., Citation2018; Valentine & Thompson, Citation2013). In addition, we also found a significant moderating effect on the type of control condition: comparisons with a waiting list control group showed larger effects than comparisons with CAU or another stress-reducing intervention. This finding is in line with our expectation that CAU or another intervention would lead to reduction of stress, and thus to more stress reduction compared to a waiting list group. In addition, participants on a waiting list may also show a reduction in the stress level of symptomatology, which is shown in previous research in psychiatric populations (Arrindell, Citation2001; Haeyen et al., Citation2018). Specifically, Crawford et al. (Citation2013) found that in spite of the positive scores of subjects of the music therapy group on stress reduction compared to subjects of the wait-list control group, the control participants also showed an improvement on stress reduction compared to baseline.
The overall effect size proved to be strongly moderated by the country in which the study was conducted (i.e., non-Western versus Western countries). Larger effects were found in non-Western studies (n = 8), including studies conducted in Asian countries, such as China, Korea, and Taiwan, but also studies conducted in Iran, Brazil and Nigeria. It has been shown that the cultural environment influences how people respond to stress (Lonner, Citation2007; Tweed et al., Citation2004), which might explain differences between Western and non-Western countries. On the other hand, the non-Western countries show great heterogeneity in culture, socioeconomic characteristics or topographical region. Moreover, Western countries with large proportions of immigrants – such as the USA, Canada, and Australia – make it difficult to equate country with culture (Morales & Ladhari, Citation2011). Additionally, post-hoc analyses showed a weak correlation between Non-Western countries and study design (r = .34, p = <.01), which indicates that the CCT design was more frequently used in Non-Western countries than in Western studies. Further research is needed to test particular explanations for cultural differences in effects between studies in Western and non-Western countries. Not only culture should be taken into account in future research, but also socioeconomic characteristics of study samples and the delivery of care in different health care systems, because of great heterogeneity both within and between countries.
Contrary to our expectations, we did not find evidence for a moderating effect of studies using a specific therapy protocol compared to studies without such a protocol. This can be explained by the fact that most studies included in our meta-analysis did not report on the use of such a therapy protocol, but still showed an adequate and rich description of the content of music therapy interventions. From the perspective of the music therapist, who is trained to tune in to the patient by adjusting the way of music-making as an immediate response to the patient's needs (Aalbers et al., Citation2019; Magee, Citation2019), music therapy protocols might often equal the flexibility of non-protocolled treatment in order to deliver personalized treatment, which increases the comparability or sameness of protocolled and non-protocolled treatment.
Notwithstanding we believe that there is a need for developing music therapy protocols and intervention descriptions that facilitate further replication of music therapy interventions and, subsequently, will better inform clinicians and practitioners in both mental health care and medical settings (de Witte et al., Citation2020a). In addition, in future trials we strongly recommend examining treatment integrity as well, because music therapists may choose not to offer some of the elements specified in the protocol or to add new treatment elements. Having information on treatment integrity allows for the examination of the degree to which the implemented intervention approximates the intended intervention, and possible effects of treatment integrity on client outcomes (Perepletchikova, Citation2011; Vermilyea et al., Citation1984).
Study quality just failed to reach the conventional level of statistical significance, which indicates that low quality studies may yield larger effects compared to studies with a moderate or strong study quality. An explanation for this result could be that the degree of ‘masking’ was an important factor in assessing study quality. Masking of participants in music therapy studies is usually not possible unless two types of music therapy interventions are compared, such as receptive music therapy versus active music therapy (Bradt et al., Citation2013b). Masking procedures in which only the investigator is masked to the allocation of the intervention is much more feasible in music therapy trials (Day & Altman, Citation2000). Nevertheless, the present meta-analysis contained several studies in which the way of masking was not reported at all (n = 12), which is in line with the findings of Magee et al. (Citation2017), who conclude in their Cochrane review that in future research reporting on the masking of participants and outcome assessors requires improvement. The lack of participant masking is problematic when studies examine subjective outcomes, such as mood or quality of life. Masking of therapists is often not possible in music therapy studies when active music-making is examined. When due to setting constrains the interventions cannot assure masking procedures, they should at least be masked to the purpose of the study where possible. In either case, masking procedures should be reported or discussed (Bradt et al., Citation2013b; Magee et al., Citation2017).
Statistical analyses showed that the selected music therapy characteristics do not seem to moderate the overall effects of music therapy on stress-related outcomes. This could be explained by the diversity of the music therapeutic approaches and/or the applied interventions of the included music therapy studies, which is also mentioned in several previous reviews (Carr et al., Citation2013; Gold et al., Citation2009; Mössler et al., Citation2011; Silverman, Citation2003). On the other hand, this diversity in the content of music therapy can also be related to the core competence of a qualified music therapist, which means that the interventions are often tailored to what the patient needs or shows at that moment. Precisely this aspect of music therapy is the main difference with music interventions without a music therapist and could therefore have resulted in a larger effect size.
The selected intervention characteristics did not have a statistically significant impact on the effectiveness of music therapy. However, some substantial differences in effect sizes were found (d = .30 or larger) in moderator analyses that did not reach the conventional level of significance due to lack of statistical power, mostly caused by an unequal distribution of studies (and effect sizes) among moderator categories (see ). We discuss some of these findings because they may be of particular theoretical interest, and probably should be addressed in future research.
First, there was a difference of d = .30 between the impact of only one session of music therapy (d = .594, [.17–1.02]) and more than one session (d = .894, [.56–1.23]), indicating that the effect of music therapy on stress-related outcomes increases with the use of multiple sessions. The larger effect size for more than one session is in line with the study of Gold et al. (Citation2009), which showed more substantial benefits in patients who took a longer course of music therapy or more frequent sessions. However, Gold's study examined the effects of music therapy in patients with severe mental disorders, whereas the present meta-analysis mostly included studies with patients suffering from much milder mental problems or patients with stress due to medical conditions. This does not diminish the importance of stress reduction, since stress is globally recognized as a major risk factor for the development of serious health problems (American Psychological Association [APA], Citation2017; Australian Psychological Society [APS], Citation2015).
Notably, the effect of the number of sessions seems to be related to the type of setting (medical healthcare versus mental healthcare). In our meta-analysis, only studies conducted in medical healthcare settings measured one-session effects of music therapy on stress-related outcomes, which of course does not exclude the possibility that positive effects can just as well be measured within mental healthcare settings after only one session of music therapy. Nevertheless, our meta-analysis found empirical evidence for the short-term effectiveness of music therapy (i.e., a single session of music therapy) in reducing stress, and therefore puts the assumption that pharmacological treatment should be started due to its immediate and rapid effect in a critical light (Bandelow et al., Citation2015; de Witte et al., Citation2020a; Fedoroff & Taylor, Citation2001). Moreover, the shown efficacy of only one single session may facilitate the implementation of music therapy in cases where for logistic reasons or in more complicated settings (e.g., during chemotherapy in the treatment of cancer, before or after surgery, or in palliative care) multiple sessions of music therapy would not be possible.
Second, the large effect of music with a tempo of 60–90 bpm (d = .900, n = 16) is worth mentioning. It is larger than the effect obtained in our previous meta-analytic review (de Witte et al., Citation2020a), showing a medium effect (d = .625, n = 36). The larger effect size found in the current meta-analysis may be ascribed to a lower amount of studies using prerecorded music than in our previous meta-analysis, which included mostly ‘music medicine’ interventions. Interestingly, a post-hoc analysis showed a significant strong correlation between music tempo of 60–90 bpm and prerecorded music (r = .61, p = <.01). Unfortunately, several studies did not report on the tempo used due to the fact that (1) interventions could vary across the music therapy session depending on participants’ needs, and (2) the use of musical instruments varied considerably within and across the music therapy sessions. Moreover, the music tempo is usually not measured during a music therapy session of live improvised music are. We strongly recommend to investigate the influence of music tempo as a component of music therapy interventions, especially when targeting stress reduction. Moreover, literature also shows that music with a slow tempo and steady rhythm may provide stress reduction by altering inherent body rhythms, such as heart rate (Thaut et al., Citation1999; Thaut & Hoemberg, Citation2014).
Lastly, the moderator ‘therapy setting’ revealed a large effect for group music therapy (d = .927, [.54–1.32]). There is empirical evidence showing that group music activities stimulate the release of the stress-reducing neurotransmitters endorphin and oxytocin as a result of positive feelings of togetherness and bonding among group members (Linnemann et al., Citation2016; Tarr et al., Citation2014). In group music therapy, feelings of togetherness and bonding may be the result of non-verbal synchronization with each other by making music or listening to music, which offers a different experience of communicating and relating to others in a medium that has been shown to be motivating for people who otherwise find it difficult to share or engage (Carr et al., Citation2017; Gold et al., Citation2013; Stern, Citation2010). Moreover, research shows that achieving synchronization by musical attunement is considered one of the most important (pre-)conditions in music therapy for eventually reaching stress reduction (Aalbers et al., Citation2019; de Witte et al., Citation2020b). Facilitating synchronization as the basis for further interventions in music therapy is therefore regarded as one of the key competencies of a music therapist (e.g., Aalbers et al., Citation2019; Bruscia, Citation1987; Schumacher & Calvet, Citation2008; Wheeler, Citation2015). Finally, a post-hoc analysis showed a significant moderate correlation (r = .45, p = <.01) between individual music therapy and medical settings, which indicates that individual music therapy is relatively more used in medical setting compared other settings.
Limitations of the present study
The current study has some limitations that need to be mentioned. Firstly, a significant number (n = 16) of the studies included in this meta-analysis had a small sample size (10–25 participants). Studies with small sample sizes are fairly common in meta-analyses (Davey et al., Citation2011), particularly when studies are conducted in medical or palliative settings where time and logistic constraints occur. It is important to highlight that small sample sizes in primary studies may result in great heterogeneity in treatment effects due to relatively large standard errors. Studies with small samples may also show greater clinical heterogeneity among patients compared to studies with large sample sizes, which may affect the outcome of the experimental treatment (IntHout et al., Citation2015; Schwarzer et al., Citation2015). Furthermore, the findings from small sample size studies tend to be less generalizable compared to studies with large number of participants. Furthermore, a limitation of any meta-analysis is that there is not a completely satisfactory way to test the presence of publication bias (Carter et al., Citation2019). The presence of publication bias can therefore never be ruled out, even if formal tests indicate that publication bias is unlikely. In fact, it is imperative that all clinical trials be preregistered in effectiveness research, including publication of the research protocols. In the present study, we chose to conduct a funnel-plot-based trim and fill method (Duval & Tweedie, Citation2000a, Citation2000b), which is commonly used in three-level meta-analyses in the domain of psychological studies (see Assink et al., Citation2019; Assink & Wibbelink, Citation2016; Zeegers et al., Citation2017), which seems a sufficiently sensitive method to detect publication bias in the current meta-analysis given the substantial number of studies and effect sizes, the magnitude of the effect sizes, and the degree of level 2 (within studies) and level 3 (between studies) heterogeneity of the overall effect size (See Assink & Wibbelink, Citation2016; Carter et al., Citation2019).
Although a clear search strategy to identify relevant studies has been performed, by for instance excluding observational and retrospective studies, most studies included in our meta-analysis lack masking procedure to participants. This particularly occurred in medical settings where due to the clinical condition of the participants the treatment group was disclosed. The majority of studies with small sample sizes and without a masking procedure were conducted in medical care. This might have influenced some of the study outcomes. Specifically, the lack of masking may have contributed to therapist expectancy (leading to therapist bias) and/or a patient expectancy-effect (also known as placebo effect), eliciting a desirable therapeutic outcome (Tambling, Citation2012). In future studies, efforts need to be made to reduce expectancy or placebo effects, for example, by measuring expectation and/or adopting alternative experimental designs to control for these effects (Atwood et al., Citation2020; Boot et al., Citation2013). Notwithstanding the ethical reasons to refrain from a masking procedure and waiting-list design in anxiety and stress studies, it is important to further improve study quality and use larger samples. Next, we strongly recommend that future trials report on power analyses.
Concluding remarks
The current meta-analytic review provides evidence that music therapy can be effective in reducing stress and provides justifications for the increasing use of music therapy carried out by a qualified music therapist in both mental health care practice and medical settings. Given the added value of the presence of a well-trained and qualified music therapist who offers music therapy, it is advisable to carefully consider whether music therapy is needed, or whether music listening interventions, mostly offered by healthcare professionals, are sufficient. In addition, low costs and lack of side effects of music therapy, and the moderate-to-strong stress-relieving effects of music therapy are very important for the prevention and treatment of stress-related problems. Nevertheless, with respect to the methodology of future trials, we strongly recommend reducing the risk of selection bias by aligning with the conditions of RCTs. Finally, the development of standardized music therapy protocols is necessary to conduct more robust research on the effects of music therapy, and to gain more insight into the moderating effects of characteristics of music therapy for stress reduction.
Acknowledgements
Special thanks are due to Arjan Doolaar and Thomas Pelgrim from HAN university of applied sciences (Nijmegen, The Netherlands), for their advice and assist with the systematic search.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Aalbers, S., Vink, A., Freeman, R. E., Pattiselanno, K., Spreen, M., & van Hooren, S. (2019). Development of an improvisational music therapy intervention for young adults with depressive symptoms: An intervention mapping study. The Arts in Psychotherapy, 65, 101584. https://doi.org/https://doi.org/10.1016/j.aip.2019.101584
- Agres, K., Schaefer, R., Volk, A., Van Hooren, S., Holzapfel, A., Dalla Bella, Müller, M., De Witte, M., Herremans, D., Ramirez Melendez, R., Neerincx, M., Ruiz, S., Meredith, D., Dimitriadis, T., & Magee, W. (2020). Music, computing, and health: A roadmap for the current and future roles of music technology for healthcare and well-being. Music & Science.
- Akin, A., & Iskender, M. (2011). Internet addiction and depression, anxiety and stress. International Online Journal of Educational Sciences, 3, 138–148. Retrieved September 2020, from https://files.eric.ed.gov/fulltext/EJ944970.pdf [Google Scholar]
- Aldwin, C. M. (2007). Stress, coping, and development, second edition: An integrative perspective. Guilford Press.
- Altshuler, I. M. (1948). The past, present, and future of musical therapy. In E. Podolsky (Ed.), Music therapy (pp. 24–35). Philosophical Library.
- American Music Therapy Association. (2018). Definition and quotes about music therapy. What is music therapy? https://www.musictherapy.org/about/quotes/
- American Psychological Association. (2017). Stress in America: Coping with Change. https://www.apa.org/news/press/releases/stress/2016/coping-with-change.pdf
- Amir, S., Brown, Z. W., & Amit, Z. (1980). The role of endorphins in stress: Evidence and speculations. Neuroscience & Biobehavioral Reviews, 4(1), 77–86. https://doi.org/https://doi.org/10.1016/0149-7634(80)90027-5
- Armijo-Olivo, S., Stiles, C. R., Hagen, N. A., Biondo, P. D., & Cummings, G. G. (2012). Assessment of study quality for systematic reviews: A comparison of the Cochrane collaboration risk of bias tool and the effective public health practice project quality assessment tool. Journal of Evaluation in Clinical Practice, 18(1), 12–18. https://doi.org/https://doi.org/10.1111/j.1365-2753.2010.01516.x
- Arrindell, W. A. (2001). Changes in waiting-list patients over time: Data on some commonly-used measures. Beware!. Behaviour Research and Therapy, 39(10), 1227–1247. https://doi.org/https://doi.org/10.1016/S0005-7967(00)00104-2
- Assink, M., van der Put, C. E., Hoeve, M., de Vries, S. L., Stams, G. J. J., & Oort, F. J. (2015). Risk factors for persistent delinquent behavior among juveniles: A meta-analytic review. Clinical Psychology Review, 42, 47–61. https://doi.org/https://doi.org/10.1016/j.cpr.2015.08.002
- Assink, M., van der Put, C. E., Meeuwsen, M. W., de Jong, N. M., Oort, F. J., Stams, G. J. J., & Hoeve, M. (2019). Risk factors for child sexual abuse victimization: A meta-analytic review. Psychological Bulletin, 145(5), 459–489. https://doi.org/https://doi.org/10.1037/bul0000188
- Assink, M., & Wibbelink, C. J. M. (2016). Fitting three-level meta-analytic models in R: A step-by-step tutorial. The Quantitative Methods for Psychology, 12(3), 154–174. https://doi.org/https://doi.org/10.20982/tqmp.12.3.p154
- Atwood, S., Mehr, S. A., & Schachner, A. 2020. Expectancy effects threaten the inferential validity of synchrony-prosociality research. https://doi.org/https://doi.org/10.31234/osf.io/zjy8u
- Australian Psychological Society. (2015). Stress and wellbeing: How Australians are coping with life. Retrieved June 2017, from http://www.psychology.org.au/Assets/Files/PW15-SR.pdf
- Bainbridge, C., Youngers, J., Bertolo, M., Atwood, S., Lopez, K., Xing, F., Martin, A., & Mehr, S. (2020). Infants relax in response to unfamiliar foreign lullabies. Nature Human Behaviour.
- Bandelow, B., Reitt, M., Röver, C., Michaelis, S., Görlich, Y., & Wedekind, D. (2015). Efficacy of treatments for anxiety disorders: A meta-analysis. International Clinical Psychopharmacology, 30(4), 183–192. https://doi.org/https://doi.org/10.1097/YIC.0000000000000078
- Bernardi, L., Porta, C., & Sleight, P. (2005). Cardiovascular, cerebrovascular, and respiratory changes induced by different types of music in musicians and nonmusicians: The importance of silence. Heart, 92(4), 445–452. https://doi.org/https://doi.org/10.1136/hrt.2005.064600
- Bernatzky, G., Presch, M., Anderson, M., & Panksepp, J. (2011). Emotional foundations of music as a non-pharmacological pain management tool in modern medicine. Neuroscience & Biobehavioral Reviews, 35(9), 1989–1999. https://doi.org/https://doi.org/10.1016/j.neubiorev.2011.06.005
- Blood, A. J., & Zatorre, R. J. (2001). Intensely pleasurable responses to music correlate with activity in brain regions implicated in reward and emotion. Proceedings of the National Academy of Sciences, 98(20), 11818–11823. https://doi.org/https://doi.org/10.1073/pnas.191355898
- Boot, W. R., Simons, D. J., Stothart, C., & Stutts, C. (2013). The pervasive problem with placebos in psychology: Why active control groups are not sufficient to rule out placebo effects. Perspectives on Psychological Science, 8(4), 445–454. https://doi.org/https://doi.org/10.1177/1745691613491271
- Bradt, J., & Dileo, C. (2014). Music interventions for mechanically ventilated patients. The Cochrane Database Of Systematic Reviews, 12, CD006902. https://doi.org/https://doi.org/10.1002/14651858.CD006902.pub3
- Bradt, J., Potvin, N., Kesslick, A., Shim, M., Radl, D., Schriver, E., Gracely, E.J., & Komarnicky-Kocher, L. T. (2015). The impact of music therapy versus music medicine on psychological outcomes and pain in cancer patients: a mixed methods study. Supportive Care in Cancer, 23(5), 1261–1271. https://doi.org/https://doi.org/10.1007/s00520-014-2478-7
- Bradt, J., Dileo, C., Magill, L., & Teague, A. (2016). Music interventions for improving psychological and physical outcomes in cancer patients. Cochrane Database of Systematic Reviews, 8, CD006911. https://doi.org/https://doi.org/10.1002/14651858.CD006911.pub3
- Bradt, J., Dileo, C., & Potvin, N. (2013a). Music for stress and anxiety reduction in coronary heart disease patients. Cochrane Database of Systematic Reviews, 12, CD006577. https://doi.org/https://doi.org/10.1002/14651858.CD006577.pub3
- Bradt, J., Dileo, C., & Shim, M. (2013b). Music interventions for preoperative anxiety. Cochrane Database of Systematic Reviews, 6, CD006908. https://doi.org/https://doi.org/10.1002/14651858.CD006908.pub2
- Bradt, J., Magee, W. L., Dileo, C., Wheeler, B. L., & McGilloway, E. (2010). Music therapy for acquired brain injury. Cochrane Database of Systematic Reviews, 2010, CD006787. https://doi.org/https://doi.org/10.1002/14651858.CD006787.pub2
- Brannon, L., & Fiest, J. (2007). Health psychology: An introduction to behavior and health (6th ed.). Thomson-Worth.
- Bringman, H., Giesecke, K., Thörne, A., & Bringman, S. (2009). Relaxing music as pre-medication before surgery: A randomised controlled trial. Acta Anaesthesiologica Scandinavica, 53(6), 759–764. https://doi.org/https://doi.org/10.1111/j.1399-6576.2009.01969.x
- Bruscia, K. E. (1987). Improvisational models of music therapy. Charles C Thomas Pub Ltd.
- Bruscia, K. E. (1998). Defining music therapy. Barcelona Publishers.
- Burrai, F., Hasan, W., Fancourt, D., Luppi, M., & DiSomma, S. (2016). A randomized controlled trial of listening to recorded music for heart failure patients: Study protocol. Holistic Nursing Practice, 30(2), 102–115. https://doi.org/https://doi.org/10.1097/HNP.0000000000000135
- Carr, C. E., O’Kelly, J., Sandford, S., & Priebe, S. (2017). Feasibility and acceptability of group music therapy vs wait-list control for treatment of patients with long-term depression (the SYNCHRONY trial): study protocol for a randomised controlled trial. Trials, 18(1), 1–15. https://doi.org/https://doi.org/10.1186/s13063-016-1752-z
- Carr, C., Odell-Miller, H., & Priebe, S. (2013). A systematic review of music therapy practice and outcomes with acute adult psychiatric in-patients. PloS one, 8(8), e70252. https://doi.org/https://doi.org/10.1371/journal.pone.0070252
- Carter, E. C., Schönbrodt, F. D., Gervais, W. M., & Hilgard, J. (2019). Correcting for bias in psychology: A comparison of meta-analytic methods. Advances in Methods and Practices in Psychological Science, 2(2), 115–144. https://doi.org/https://doi.org/10.1177/2515245919847196
- Casey, G. (2017). Stress and disease. Kai Tiaki Nursing New Zealand, 23, 20–24.
- Cassileth, B. R., Vickers, A. J., & Magill, L. A. (2003a). Music therapy for mood disturbance during hospitalization for autologous stem cell transplantation: A randomized controlled trial. Cancer, 98(12), 2723–2729. https://doi.org/https://doi.org/10.1002/cncr.11842
- Câmara, Y. M. R., Campo, M. R. M., & Câmara, Y. R. (2013). Music therapy as a therapeutic resource for mental health. Braz J Mental Health, 94–117.
- Chanda, M. L., & Levitin, D. J. (2013). The neurochemistry of music. Trends in Cognitive Sciences, 17(4), 179–193. https://doi.org/https://doi.org/10.1016/j.tics.2013.02.007
- Cheung, M. W. L. (2014). Modeling dependent effect sizes with three-level meta-analyses: A structural equation modeling approach. Psychological Methods, 19(2), 211–229. https://doi.org/https://doi.org/10.1037/a0032968
- Chlan, L. L. (2000). Music therapy as a nursing intervention for patients supported by mechanical ventilation. AACN Advanced Critical Care, 11, 128–138. https://doi.org/https://doi.org/10.1097/00044067-200002000-00014
- Cohen, S., Kamarck, T., & Mermelstein, R. (1983). A global measure of psychological stress. Journal of Health and Social Behavior, 24(4), 385–396. https://doi.org/https://doi.org/10.2307/2136404
- Davey, J., Turner, R., Clarke, M., & Higgins, J. (2011). Characteristics of meta-analyses and their component studies in the Cochrane Database of systematic reviews: A cross-sectional, descriptive analysis. BMC Medical Research Methodology, 11(1), 1–11. https://doi.org/https://doi.org/10.1186/1471-2288-11-160
- Day, S. J., & Altman, D. G. (2000). Statistics Notes: Blinding in clinical trials and other studies. BMJ, 321(7259), 504. https://doi.org/https://doi.org/10.1136/bmj.321.7259.504
- de Witte, M., Lindelauf, E., Moonen, X. M. H., Stams, G. J. J. M., & van Hooren, S. (2020b). Music therapy interventions for stress reduction in Adults with Mild Intellectual Disabilities: Perspectives from clinical practice. Frontiers in Psychology. https://doi.org/https://doi.org/10.3389/fpsyg.2020.572549
- de Witte, M., Spruit, A., van Hooren, S., Moonen, X., & Stams, G. J. (2020a). Effects of music interventions on stress-related outcomes: A systematic review and two meta-analyses. Health Psychology Review, 14(2), 294–324. https://doi.org/https://doi.org/10.1080/17437199.2019.1627897
- Dief, A. E., Sivukhina, E. V., & Jirikowski, G. F. (2018). Oxytocin and stress response. Open Journal of Endocrine and Metabolic Diseases, 08((03|3)), 93–104. https://doi.org/https://doi.org/10.4236/ojemd.2018.83010
- Dileo, C. (1999). Music therapy and medicine: Theoretical and clinical applications. American Music Therapy Association.
- Dileo, C. (2006). Effects of music and music therapy on medical patients: A meta-analysis of the research and implications for the future. Journal of The Society for Integrative Oncology, 4, 67–70. https://doi.org/https://doi.org/10.2310/7200.2006.002
- Donovan, L. M., Malte, C. A., Spece, L. J., Griffith, M. F., Feemster, L. C., Zeliadt, S. B., Au, D. H., & Hawkins, E. J. (2019). Risks of benzodiazepines in chronic obstructive pulmonary disease with comorbid posttraumatic stress disorder. Annals of the American Thoracic Society, 16(1), 82–90. https://doi.org/https://doi.org/10.1513/AnnalsATS.201802-145OC
- Duval, S., & Tweedie, R. (2000a). A nonparametric ‘trim and fill’ method of accounting for publication bias in meta-analysis. Journal of the American Statistical Association, 95, 89–99. https://doi.org/https://doi.org/10.2307/2669529
- Duval, S., & Tweedie, R. (2000b). Trim and fill: A simple funnel-plot based method of testing and adjusting for publication bias in meta-analysis. Biometrics, 56(2), 455–463. https://doi.org/https://doi.org/10.1111/j.0006-341X.2000.00455.x
- Effective Public Health Practice Project. (2009). Quality assessment tool for quantitative studies. http://www.ephpp.ca/tools.html
- Fedoroff, I. C., & Taylor, S. (2001). Psychological and pharmacological treatments of social phobia: A meta-analysis. Journal of Clinical Psychopharmacology, 21(3), 311–324. https://doi.org/https://doi.org/10.1097/00004714-200106000-00011
- Finney, J. (2000). Limitations in using existing alcohol treatment trials to develop practice guidelines. Addiction, 95(10), 1491–1500. https://doi.org/https://doi.org/10.1046/j.1360-0443.2000.951014914.x
- Gabrielsson, A., & Lindström, E. (2010). The role of structure in the musical expression of emotions. In P. N. Juslin, & J. A. Sloboda (Eds.), Series in affective science. Handbook of music and emotion: Theory, research, applications (pp. 367–400). Oxford University Press.
- Galanakis, M., Stalikas, A., Kallia, H., Karagianni, C., & Karela, C. (2009). Gender differences in experiencing occupational stress: The role of age, education and marital status. Stress & Health, 25(5), 397–404. https://doi.org/https://doi.org/10.1002/smi.1248
- Gillen, E., Biley, F., & Allen, D. (2008). Effects of music listening on adult patients’ pre-procedural state anxiety in hospital. International Journal of Evidence-Based Healthcare, 6, 24–49. https://doi.org/https://doi.org/10.1111/j.1744–1609.2007.00097.x
- Gold, C., Solli, H. P., Krüger, V., & Lie, S. A. (2009). Dose–response relationship in music therapy for people with serious mental disorders: Systematic review and meta-analysis. Clinical Psychology Review, 29(3), 193–207. https://doi.org/https://doi.org/10.1016/j.cpr.2009.01.001
- Gutgsell, K. J., Schluchter, M., Margevicius, S., DeGolia, P. A., McLaughlin, B., Harris, M., Mecklenburg, J., & Wiencek, C. (2013). Music therapy reduces pain in palliative care patients: A randomized controlled trial. Journal of Pain and Symptom Management, 45(5), 822–831. https://doi.org/https://doi.org/10.1016/j.jpainsymman.2012.05.008
- Haeyen, S., van Hooren, S., van der Veld, W., & Hutschemaekers, G. (2018). Efficacy of art therapy in individuals with personality disorders cluster B/C: A randomized controlled trial. Journal of Personality Disorders, 32(4), 527–542. https://doi.org/https://doi.org/10.1521/pedi_2017_31_312
- Heiderscheit, A., & Madson, A. (2015). Use of the iso principle as a central method in mood management: A music psychotherapy clinical case study. Music Therapy Perspectives, 33(1), 45–52. https://doi.org/https://doi.org/10.1093/mtp/miu042
- Higgins, J., & Green, S. (Eds.). (2011). Cochrane handbook for systematic reviews of interventions: Version 5.1.0 [updated March 2011]. Wiley-Blackwell.
- Hilz, M. J., Stadler, P., Gryc, T., Nath, J., Habib-Romstoeck, L., Stemper, B., Buechner, S., Wong, S., & Koehn, J. (2014). Music induces different cardiac autonomic arousal effects in young and older persons. Autonomic Neuroscience, 183, 83–93. https://doi.org/https://doi.org/10.1016/j.autneu.2014.02.004
- Hook, L., Songwathana, P., & Petpichetchian, W. (2008). Music therapy with female surgical patients: Effect on anxiety and pain. Pacific Rim International Journal of Nursing Research, 12, 259–271.
- Houben, M., Van Den Noortgate, W., & Kuppens, P. (2015). The relation between short-term emotion dynamics and psychological well-being: A meta-analysis. Psychological Bulletin, 141(4), 901–930. https://doi.org/https://doi.org/10.1037/a0038822
- Hox, J. (2010). Multilevel analysis: Techniques and applications. Routledge.
- IntHout, J., Ioannidis, J. P., Borm, G. F., & Goeman, J. J. (2015). Small studies are more heterogeneous than large ones: A meta-meta-analysis. Journal of Clinical Epidemiology, 68(8), 860–869. https://doi.org/https://doi.org/10.1016/j.jclinepi.2015.03.017
- Jackson, N., & Waters, E. (2005). Criteria for the systematic review of health promotion and public health interventions. Health Promotion International, 20(4), 367–374. https://doi.org/https://doi.org/10.1093/heapro/dai022
- Jäncke, L. (2008). Music, memory and emotion. Journal of Biology, 7(6), 21. https://doi.org/https://doi.org/10.1186/jbiol82
- Juslin, P. N., Liljeström, S., Västfjäll, D., Barradas, G., & Silva, A. (2008). An experience sampling study of emotional reactions to music: Listener, music, and situation.. Emotion, 8(5), 668–683. https://doi.org/https://doi.org/10.1037/a0013505
- Juslin, P. N., & Västfjäll, D. (2008). Emotional responses to music: The need to consider underlying mechanisms. Behavioral and Brain Sciences, 31(5), 559–575. https://doi.org/https://doi.org/10.1017/S0140525X08005293
- Kajantie, E., & Phillips, D. I. (2006). The effects of sex and hormonal status on the physiological response to acute psychosocial stress. Psychoneuroendocrinology, 31(2), 151–178. https://doi.org/https://doi.org/10.1016/j.psyneuen.2005.07.002
- Kamioka, H., Tsutani, K., Yamada, M., Park, H., Okuizumi, H., Tsuruoka, K., Honda, T., Okada, S., Park, S. J., Kitayuguchi, J., & Abe, T. (2014). Effectiveness of music therapy: A summary of systematic reviews based on randomised controlled trials of music interventions. Patient Preference and Adherence, 8, 727–754. https://doi.org/https://doi.org/10.2147/PPA.S61340
- Karlsson, P., & Bergmark, A. (2015). Compared with what? An analysis of control-group types in Cochrane and Campbell reviews of psychosocial treatment efficacy with substance use disorders. Addiction, 110(3), 420–428. https://doi.org/https://doi.org/10.1111/add.12799
- Kemper, K. J., & Danhauer, S. C. (2005). Music as therapy. Southern Medical Journal, 98(3), 282–288. https://doi.org/https://doi.org/10.1097/01.SMJ.0000154773.11986.39
- Kim, Y., Evangelista, L. S., & Park, Y. G. (2015). Anxiolytic effects of music interventions in patients receiving incenter hemodialysis: A systematic review and meta-analysis. Nephrology Nursing Journal, 42, 339–347. https://doi.org/https://doi.org/10.1037/1099-9809.11.3.187
- Koelsch, S. (2012). Brain and music. John Wiley.
- Koelsch, S. (2015). Music-evoked emotions: Principles, brain correlates, and implications for therapy. Annals of the New York Academy of Sciences, 1337(1), 193–201. https://doi.org/https://doi.org/10.1111/nyas.12684
- Koelsch, S., Boehlig, A., Hohenadel, M., Nitsche, I., Bauer, K., & Sack, U. (2016). The impact of acute stress on hormones and cytokines, and how their recovery is affected by music-evoked mood. Scientific Reports, 6(1), 23008. https://doi.org/https://doi.org/10.1038/srep23008
- Kreutz, G., Murcia, C. Q., & Bongard, S. (2012). Psychoneuroendocrine research on music and health: An overview. In R. A. R. MacDonald, D. Kreutz, & L. Mitchell (Eds.), Music, health, and wellbeing (pp. 457–476). Oxford University Press.
- Landis-Shack, N., Heinz, A. J., & Bonn-Miller, M. O. (2017). Music therapy for posttraumatic stress in adults: A theoretical review. Psychomusicology: Music, Mind, and Brain, 27(4), 334–342. https://doi.org/https://doi.org/10.1037/pmu0000192
- Lazarus, R. S., & Folkman, S. (1984). Stress, appraisal, and coping. Springer.
- Leubner, D., & Hinterberger, T. (2017). Reviewing the effectiveness of music interventions in treating depression. Frontiers in Psychology, 8, 1109. https://doi.org/https://doi.org/10.3389/fpsyg.2017.01109
- Levitin, D. J. (2009). The Neural Correlates of Temporal structure in music. Music and Medicine, 1(1), 9–13. https://doi.org/https://doi.org/10.1177/1943862109338604
- Linnemann, A., Ditzen, B., Strahler, J., Doerr, J. M., & Nater, U. M. (2015). Music listening as a means of stress reduction in daily life. Psychoneuroendocrinology, 60, 82–90. https://doi.org/https://doi.org/10.1016/j.psyneuen.2015.06.008
- Linnemann, A., Strahler, J., & Nater, U. M. (2016). The stress-reducing effect of music listening varies depending on the social context. Psychoneuroendocrinology, 72, 97–105. https://doi.org/https://doi.org/10.1016/j.psyneuen.2016.06.003
- Linnemann, A., Strahler, J., & Nater, U. M. (2017). Assessing the effects of music listening on Psychobiological stress in daily life. Journal of Visualized Experiments, 120, e54920–e54920. https://doi.org/https://doi.org/10.3791/54920
- Lipsey, M. W., & Wilson, D. B. (2001). Practical meta-analysis. Sage.
- Lonner, W. J. (2007). Foreword. In P. T. Wong, & L. C. Wong (Eds.), Handbook of multicultural perspectives on stress and coping (pp. v–vii). Springer.
- Magee, W. L. (2019). Why include music therapy in a neuro-rehabilitation team. Advances in Clinical Neuroscience & Rehabilitation, 19(2), 10–12.
- Magee, W. L., Clark, I., Tamplin, J., & Bradt, J. (2017). Music interventions for acquired brain injury. Cochrane Database of Systematic Reviews, 1, CD006787. https://doi.org/https://doi.org/10.1002/14651858.CD006787.pub3
- Martin, L., Oepen, R., Bauer, K., Nottensteiner, A., Mergheim, K., Gruber, H., & Koch, S. C. (2018). Creative arts interventions for stress management and prevention—a systematic review. Behavioral Sciences, 8(2), 28. https://doi.org/https://doi.org/10.3390/bs8020028
- McEwen, B. S., & Gianaros, P. J. (2010). Central role of the brain in stress and adaptation: Links to socioeconomic status, health, and disease. Annals of The New York Academy of Sciences, 1186(1), 190–222. https://doi.org/https://doi.org/10.1111/j.1749-6632.2009.05331.x
- McNair, D. M., Lorr, M., & Droppleman, L. (1981). Profile of mood states questionnaire. EDITS.
- Mehr, S. A., Singh, M., Knox, D., Ketter, D. M., Pickens–Jones, D., Atwood, S., Lucas, C., Jacoby, N., Egner, A. A., Hopkins, E. J., & Howard, R. M. (2019). Universality and diversity in human song. Science, 366), https://doi.org/https://doi.org/10.1126/science.aax0868
- Ming Wu, S. (2002). Effects of music therapy on anxiety, depression and self-esteem of undergraduates. Psychologia, 45(2), 104–114. https://doi.org/https://doi.org/10.2117/psysoc.2002.104
- Moore, K. S. (2013). A systematic review on the neural effects of music on emotion regulation: Implications for music therapy practice. Journal of Music Therapy, 50(3), 198–242. https://doi.org/https://doi.org/10.1093/jmt/50.3.198
- Morales, M., & Ladhari, R. (2011). Comparative cross-cultural service quality: An assessment of research methodology. Journal of Service Management. https://www.emerald.com/insight/publication/issn/1757-5818
- Mössler, K., Chen, X., Heldal, T. O., & Gold, C. (2011). Music therapy for people with schizophrenia and schizophrenia-like disorders. Cochrane Database of Systematic Reviews, 12, 1–84. https://doi.org/https://doi.org/10.1002/14651858.CD004025.pub4
- Myint, K., Jayakumar, R., Hoe, S. Z., Kanthimathi, M. S., & Lam, S. K. (2017). Cortisol, β-endorphin and oxidative stress markers in healthy medical students in response to examination stress. Biomedical Research, 28, 3774–3779.
- Ng, M. Y., Karimzad, Y., Menezes, R. J., Wintersperger, B. J., Li, Q., Forero, J., … Nguyen, E. T. (2016). Randomized controlled trial of relaxation music to reduce heart rate in patients undergoing cardiac CT. European Radiology, 26(10), 3635–3642. https://doi.org/https://doi.org/10.1007/s00330-016-4215-8
- Nomura, S., Yoshimura, K., & Kurosawa, Y. (2013). A pilot study on the effect of music-heart beat feedback system on human heart activity. Journal of Medical Informatics & Technologies, 22, 251–256. http://jmit.us.edu.pl/cms/jmitjrn/22/14_Nomura_3.pdf
- Olfson, M., King, M., & Schoenbaum, M. (2015). Benzodiazepine use in the United States. JAMA Psychiatry, 72(2), 136–142. https://doi.org/https://doi.org/10.1001/jamapsychiatry.2014.1763
- Ozer, N., Karaman Ozlu, Z., Arslan, S., & Gunes, N. (2013). Effect of music on postoperative pain and physiologic parameters of patients after open heart surgery. Pain Management Nursing, 14(1), 20–28. https://doi.org/https://doi.org/10.1016/j.pmn.2010.05.002
- Page, M. J., Boutron, I., Hansen, C., Altman, D. G., & Hróbjartsson, A. (2018). Assessing risk of bias in studies that evaluate health care interventions: Recommendations in the misinformation age. Journal of Clinical Epidemiology, 97, 133–136. https://doi.org/https://doi.org/10.1016/j.jclinepi.2018.01.004
- Pelletier, C. (2004). The effect of music on decreasing arousal due to stress: A meta-analysis. Journal of Music Therapy, 41(3), 192–214. https://doi.org/https://doi.org/10.1093/jmt/41.3.192
- Perepletchikova, F. (2011). On the topic of treatment integrity. Clinical Psychology: Science and Practice, 18(2), 148–153. https://doi.org/https://doi.org/10.1111/j.1468-2850.2011.01246.x
- Pittman, S., & Kridli, S. (2011). Music intervention and preoperational anxiety: An integrative review. International Nursing Review, 58(2), 157–163. https://doi.org/https://doi.org/10.1111/j.1466-7657.2011.00888.x
- Pritchard, M. J. (2009). Identifying and assessing anxiety in pre-operative patients. Nursing Standard, 23(51), 35–40. https://doi.org/https://doi.org/10.7748/ns.23.51.35.s46
- Puetz, T. W., Youngstedt, S. D., & Herring, M. P. (2015). Effects of pharmacotherapy on combat-related PTSD, anxiety, and depression: A systematic review and meta-regression analysis. PloS One, 10(5), 1–18. https://doi.org/https://doi.org/10.1371/journal.pone.0126529
- Rafieyan, R., & Ries, R. (2007). A description of the use of music therapy in consultation-liaison psychiatry. Psychiatry (Edgmont), 1, 47–52. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2922391/
- Raglio, A., Attardo, L., Gontero, G., Rollino, S., Groppo, E., & Granieri, E. (2015). Effects of music and music therapy on mood in neurological patients. World Journal of Psychiatry, 5(1), 68–78. https://doi.org/https://doi.org/10.5498/wjp.v5.i1.68
- Rethlefsen, M. L., Farrell, A. M., Trzasko, L. C. O., & Brigham, T. J. (2015). Librarian co-authors correlated with higher quality reported search strategies in general internal medicine systematic reviews. Journal of Clinical Epidemiology, 68(6), 617–626. https://doi.org/https://doi.org/10.1016/j.jclinepi.2014.11.025
- Robb, S. L., Carpenter, J. S., & Burns, D. S. (2011). Reporting guidelines for music-based interventions. Journal of Health Psychology, 16(2), 342–352. https://doi.org/https://doi.org/10.1177/1359105310374781
- Rosenthal, R. (1995). Writing meta-analytic reviews. Psychological Bulletin, 118(2), 183–192. https://doi.org/https://doi.org/10.1037/0033-2909.118.2.183
- Rudin, D., Kiss, A., Wetz, R. V., & Sottile, V. M. (2007). Music in the endoscopy suite: A meta-analysis of randomised controlled studies. Endoscopy, 39, 507–510. https://doi.org/https://doi.org/10.1055/s-2007-966362
- Salimpoor, V. N., van den Bosch, I., Kovacevic, N., McIntosh, A. R., Dagher, A., & Zatorre, R. J. (2013). Interactions between the nucleus accumbens and auditory cortices predict music reward value. Science, 340(6129), 216–219. https://doi.org/https://doi.org/10.1126/science.1231059
- Särkämö, T., Tervaniemi, M., Laitinen, S., Forsblom, A., Soinila, S., Mikkonen, M., Autti, T., Silvennoinen, H. M., Erkkilä, J., Laine, M., & Peretz, I. (2008). Music listening enhances cognitive recovery and mood after middle cerebral artery stroke. Brain, 131(3), 866–876. https://doi.org/https://doi.org/10.1093/brain/awn013
- Särkämö, T., Tervaniemi, M., Laitinen, S., Numminen, A., Kurki, M., Johnson, J. K., & Rantanen, P. (2014). Cognitive, emotional, and social benefits of regular musical activities in early dementia: Randomized controlled study. The Gerontologist, 54(4), 634–650. https://doi.org/https://doi.org/10.1093/geront/gnt100
- Schumacher, K., & Calvet, C. (2008). Synchronization. Music therapy with children on the autistic spectrum. Vandenhoeck & Ruprecht.
- Schwarzer, G., Carpenter, J., & Rücker, G. (2015). Small-study effects in meta-analysis. Springer.
- Shadish, W. R., Clark, M. H., & Steiner, P. M. (2008). Can Nonrandomized Experiments yield Accurate Answers? A randomized Experiment Comparing random and Nonrandom Assignments. Journal of the American Statistical Association, 103(484), 1334–1344. https://doi.org/https://doi.org/10.1198/016214508000000733
- Shadish, W. R., Cook, T. D., & Campbell, D. T. (2002). Experimental and quasi-experimental designs for generalized causal inference. Houghton Mifflin.
- Silverman, M. J. (2003). The influence of music on the symptoms of psychosis: A meta-analysis. Journal of Music Therapy, 40(1), 27–40. https://doi.org/https://doi.org/10.1093/jmt/40.1.27
- Spielberger, C. D., Gorsuch, R. L., Lushene, R., Vagg, P. R., & Jacobs, G. A. (1983). Manual for the state-trait anxiety inventory. Consulting Psychologists Press.
- Spruit, A., Assink, M., van Vugt, E., van der Put, C., & Stams, G. J. (2016). The effects of physical activity interventions on psychosocial outcomes in adolescents: A meta-analytic review. Clinical Psychology Review, 45, 56–71. https://doi.org/https://doi.org/10.1016/j.cpr.2016.03.006
- Stegemann, T., Geretsegger, M., Phan Quoc, E., Riedl, H., & Smetana, M. (2019). Music therapy and other music-based interventions in pediatric health care: An overview. Medicines, 6(1), 25. https://doi.org/https://doi.org/10.3390/medicines6010025
- Steptoe, A., & Kivimäki, M. (2012). Stress and cardiovascular disease. Nature Reviews Cardiology, 9(6), 360–370. https://doi.org/https://doi.org/10.1038/nrcardio.2012.45
- Stern, D. N. (2010). Forms of vitality: Exploring dynamic experience in psychology, the arts, psychotherapy, and development. Oxford University Press.
- Tabachnick, B. G., & Fidell, L. S. (2013). Using multivariate statistics (6th ed.). Pearson.
- Taets, G. G. D. C., Jomar, R. T., Abreu, A. M. M., & Capella, M. A. M. (2019). Effect of music therapy on stress in chemically dependent people: A quasi-experimental study. Revista Latino-Americana de Enfermagem, 27. https://doi.org/https://doi.org/10.1590/1518-8345.2456.3115
- Tambling, R. B. (2012). A literature review of therapeutic expectancy effects. Contemporary Family Therapy, 34(3), 402–415. https://doi.org/https://doi.org/10.1007/s10591-012-9201-y
- Tarr, B., Launay, J., & Dunbar, R. I. (2014). Music and social bonding: Self-other merging and neurohormonal mechanisms. Frontiers in Psychology, 5, 1096. https://doi.org/https://doi.org/10.3389/fpsyg.2014.01096
- Thaut, M. H., & Hoemberg, V. (2014). Handbook of neurologic music therapy. Oxford University Press.
- Thaut, M. H., Kenyon, G. P., Schauer, M. L., & McIntosh, G. C. (1999). The connection between rhythmicity and brain function. IEEE Engineering in Medicine and Biology Magazine, 18(2), 101–108. https://doi.org/https://doi.org/10.1109/51.752991
- Thomas, B. H., Ciliska, D., Dobbins, M., & Micucci, S. (2004). A process for systematically reviewing the literature: Providing the research evidence for public health nursing interventions. Worldviews on Evidence-Based Nursing, 1(3), 176–184. https://doi.org/https://doi.org/10.1111/j.1524-475X.2004.04006.x
- Tweed, R. G., White, K., & Lehman, D. R. (2004). Culture, stress, and coping: Internally- and externally-targeted control strategies of European Canadians, East Asian Canadians, and Japanese. Journal of Cross-Cultural Psychology, 35(6), 652–668. https://doi.org/https://doi.org/10.1177/0022022104270109
- Valentine, J. C., & Thompson, S. G. (2013). Issues relating to confounding and meta-analysis when including non-randomized studies in systematic reviews on the effects of interventions. Research Synthesis Methods, 4(1), 26–35. https://doi.org/https://doi.org/10.1002/jrsm.1064
- Van den Bussche, E., Van den Noortgate, W., & Reynvoet, B. (2009). Mechanisms of masked priming: A meta-analysis. Psychological Bulletin, 135(3), 452–477. https://doi.org/https://doi.org/10.1037/a0015329
- Van Den Noortgate, W., & Onghena, P. (2003). Estimating the mean effect size in meta-analysis: Bias, precision, and mean squared error of different weighting methods. Behavior Research Methods, Instruments, & Computers, 35, 504–511. https://doi.org/https://doi.org/10.3758/BF03195529
- Verma, R., Balhara, Y. P. S., & Gupta, C. S. (2011). Gender differences in stress response: Role of developmental and biological determinants. Industrial Psychiatry Journal, 20, 4–10. https://doi.org/https://doi.org/10.4103/0972-6748.98407
- Vermilyea, B. B., Barlow, D. H., & O’Brien, G. T. (1984). The importance of assessing treatment integrity: An example in the anxiety disorders. Journal of Behavioral Assessment, 6(1), 1–11. https://doi.org/https://doi.org/10.1007/BF01321456
- Viechtbauer, W. (2010). Conducting meta-analyses in R with the metafor package. Journal of Statistical Software, 36(3), 1–48. https://doi.org/https://doi.org/10.18637/jss.v036.i03
- Vink, A., & Hanser, S. (2018). Music-based therapeutic interventions for people with dementia: A mini-review. Medicines, 5(4), 109. https://doi.org/https://doi.org/10.3390/medicines5040109
- Wetsch, W. A., Pircher, I., & Lederer, W. (2009). Preoperative stress and anxiety in day-care patients and inpatients undergoing fast-track surgery. British Journal of Anaesthesia, 103(2), 199–205. https://doi.org/https://doi.org/10.1093/bja/aep136
- Wheeler, B. L. (2015). Music therapy handbook. Guilford Publications.
- Wigram, T. (2004). Improvisation: Methods and techniques for music therapy clinicians, educators and students. Jessica Kingsley Publishers.
- Wilson, D. B. (2013). Practical meta-analysis effect size calculator. http://www.campbellcollaboration.org/escalc/html/EffectTable 1SizeCalculator-Home.php
- Woodruffe-Peacock, C., Turnbull, G. M., Johnson, M. A., Elahi, N., & Preston, G. C. (1998). The quick mood scale: Development of a simple mood assessment scale for clinical pharmacology studies. Human Psychopharmacology: Clinical and Experimental, 13(1), 53–58. https://doi.org/https://doi.org/10.1002/(SICI)1099-1077(199801)13:1<53::AID-HUP955>3.0.CO;2-S
- World Health Organization. (2010). Global health diplomacy: Negotiating health in the 21st century. Retrieved October 12, 2017, from http://www.who.int/dg/speeches/2008/20081021/en/
- Zatorre, R. J. (2015). Musical pleasure and reward: Mechanisms and dysfunction. Annals of the New York Academy of Sciences, 1337(1), 202–211. https://doi.org/https://doi.org/10.1111/nyas.12677
- Zeegers, M. A. J., Colonnesi, C., Stams, G. J. J. M., & Meins, E. (2017). Mind Matters: A meta-analysis on Parental Mentalization and Sensitivity as Predictors of Infant-Parent Attachment. Psychological Bulletin, 143(12), 1245–1272. https://doi.org/https://doi.org/10.1037/bul0000114
- Zeng, X., Zhang, Y., Kwong, J. S., Zhang, C., Li, S., Sun, F., Niu, Y., & Du, L. (2015). The methodological quality assessment tools for preclinical and clinical studies, systematic review and meta-analysis, and clinical practice guideline: A systematic review. Journal of Evidence-Based Medicine, 8(1), 2–10. https://doi.org/https://doi.org/10.1111/jebm.12141
- Zhang, Z. S., Wang, X. L., Xu, C. L., Zhang, C., Cao, Z., Xu, W. D., Wei, R. C., & Sun, Y. H. (2014). Music reduces panic: An initial study of listening to preferred music improves male patient discomfort and anxiety during flexible cystoscopy. Journal of Endourology, 28(6), 739–744. https://doi.org/https://doi.org/10.1089/end.2013.0705
Studies included in the meta-analysis
- Aldridge, D., Schmid, W., Kaeder, M., Schmidt, C., & Ostermann, T. (2005). Functionality or aesthetics? A pilot study of music therapy in the treatment of multiple sclerosis patients. Complementary Therapies in Medicine, 13(1), 25–33. https://doi.org/https://doi.org/10.1016/j.ctim.2005.01.004
- Argstatter, H., Haberbosch, W., & Bolay, H. V. (2006). Study of the effectiveness of musical stimulation during intracardiac catheterization. Clinical Research in Cardiology, 95(10), 514–522. https://doi.org/https://doi.org/10.1007/s00392-006-0425-4
- Bradt, J., Potvin, N., Kesslick, A., Shim, M., Radl, D., Schriver, E., … Komarnicky-Kocher, L. T. (2015). The impact of music therapy versus music medicine on psychological outcomes and pain in cancer patients: A mixed methods study. Supportive Care in Cancer, 23(5), 1261–1271. https://doi.org/https://doi.org/10.1007/s00520-014-2478-7
- Browning, C. A. (2001). Music therapy in Childbirth: Research in practice. Music Therapy Perspectives, 19(2), 74–81. https://doi.org/https://doi.org/10.1093/mtp/19.2.74
- Burns, D. S., Azzouz, F., Sledge, R., Rutledge, C., Hincher, K., Monahan, P. O., & Cripe, L. D. (2008). Music imagery for adults with acute leukemia in protective environments: A feasibility study. Supportive Care in Cancer, 16(5), 507–513. https://doi.org/https://doi.org/10.1007/s00520-007-0330-z
- Cassileth, B. R., Vickers, A. J., & Magill, L. A. (2003b). Music therapy for Mood Disturbance during Hospitalization for Autologous Stem Cell Transplantation: A randomized controlled trial. Cancer, 98(12), 2723–2729. https://doi.org/https://doi.org/10.1002/cncr.11842
- Chang, B. H., Chen, B. W., Beckstead, J. W., & Yang, C. Y. (2018). Effects of a music-creation programme on the anxiety, self-esteem, and quality of life of people with severe mental illness: A quasi-experimental design. International Journal of Mental Health Nursing, 27(3), 1066–1076. https://doi.org/https://doi.org/10.1111/inm.12414
- Chen, X. J., Hannibal, N., & Gold, C. (2016). Randomized trial of group music therapy with Chinese prisoners: Impact on anxiety, depression, and self-esteem. International Journal of Offender Therapy and Comparative Criminology, 60(9), 1064–1081. https://doi.org/https://doi.org/10.1177/0306624X15572795
- Choi, A. N., Lee, M. S., & Lim, H. J. (2008). Effects of group music intervention on depression, anxiety, and relationships in psychiatric patients: A pilot study. Journal of Alternative and Complementary Medicine, 14(5), 567–570. https://doi.org/https://doi.org/10.1089/acm.2008.0006
- Clark, M., Isaacks-Downton, G., Wells, N., Redlin-Frazier, S., Eck, C., Hepworth, J. T., & Chakravarthy, B. (2006). Use of preferred music to reduce emotional distress and symptom activity during radiation therapy. Journal of Music Therapy, 43(3), 247–265. https://doi.org/https://doi.org/10.1093/jmt/43.3.247
- Crawford, I., Hogan, T., & Silverman, M. J. (2013). Effects of music therapy on perception of stress, relaxation, mood, and side effects in patients on a solid organ transplant unit: A randomized effectiveness study. Arts in Psychotherapy, 40(2), 224–229. https://doi.org/https://doi.org/10.1016/j.aip.2013.02.005
- Domingo, J. P., Matamoros, N. E., Danés, C. F., Abelló, H. V., Carranza, J. M., Ripoll, A. I. R., Garcia, S. M., & Rossetti, A. (2015). Effectiveness of music therapy in advanced cancer patients admitted to a palliative care unit: A nonrandomized controlled, clinical trial. Music and Medicine, 7(1), 23–31.
- Dóro, C. A., Neto, J. Z., Cunha, R., & Dóro, M. P. (2017). Music therapy improves the mood of patients undergoing hematopoietic stem cells transplantation (controlled randomized study). Supportive Care in Cancer, 25(3), 1013–1018. https://doi.org/https://doi.org/10.1007/s00520-016-3529-z
- Erkkilä, J., Punkanen, M., Fachner, J., Ala–Ruona, E., Pöntiö, I., Tervaniemi, M., Vanhala, M., & Gold, C. (2011). Individual music therapy for depression: Randomised controlled trial. British Journal of Psychiatry, 199(2), 132–139. https://doi.org/https://doi.org/10.1192/bjp.bp.110.085431
- Ezegbe, B. N., Ede, M. O., Eseadi, C., Nwaubani, O. O., Akaneme, I. N., Aye, E. N., Ede, K. R., Omeje, J. C., Ezurike, C., Onyishi, C. N., & Ali, R. B. (2018). Effect of music therapy combined with cognitive restructuring therapy on emotional distress in a sample of Nigerian married couples. Medicine (United States), 34, 1–7. https://doi.org/https://doi.org/10.1097/MD.0000000000011637
- Ferrer, A. J. (2007). The effect of live music on decreasing anxiety in patients undergoing chemotherapy treatment. Journal of Music Therapy, 44(3), 242–255. https://doi.org/https://doi.org/10.1093/jmt/44.3.242
- Gallagher, L. M., Gardner, V., Bates, D., Mason, S., Nemecek, J., DiFiore, J. B., Bena, J., Li, M., & Bethoux, F. (2018). Impact of music therapy on Hospitalized patients post-Elective Orthopaedic surgery: A randomized controlled trial. Orthopaedic Nursing, 37(2), 124–133. https://doi.org/https://doi.org/10.1097/NOR.0000000000000432
- Ghetti, C. M. (2013). Effect of music therapy with emotional – approach coping on preprocedural anxiety in cardiac catheterization: A randomized controlled trial. Journal of Music Therapy, 50(2), 93–122. https://doi.org/https://doi.org/10.1093/jmt/50.2.93
- Gold, C., Assmus, J., Hjørnevik, K., Qvale, L. G., Brown, F. K., Hansen, A. L., Waage, L., & Stige, B. (2014). Music therapy for prisoners: Pilot randomised controlled trial and implications for evaluating psychosocial interventions. International Journal of Offender Therapy and Comparative Criminology, 58(12), 1520–1539. https://doi.org/https://doi.org/10.1177/0306624X13498693
- Gold, C., Erkkilä, J., Bonde, L. O., Trondalen, G., Maratos, A., & Crawford, M. J. (2011). Music therapy or music medicine? Psychotherapy and Psychosomatics, 80(5), 304. https://doi.org/https://doi.org/10.1159/000323166
- Gold, C., Mössler, K., Grocke, D., Heldal, T. O., Tjemsland, L., Aarre, T., Aarø, L. E., Rittmannsberger, H., Stige, B., Assmus, J., & Rolvsjord, R. (2013). Individual music therapy for mental health care clients with low therapy motivation: Multicentre randomised controlled trial. Psychotherapy and Psychosomatics, 82(5), 319–331. https://doi.org/https://doi.org/10.1159/000348452
- Haack, B., & Silverman, M. J. (2017). Effects of guitar accompaniment style within patient preferred live music on mood and pain with hospitalized patients on a solid organ transplant unit: A three group randomized pilot study. Arts in Psychotherapy, 52, 32–40. https://doi.org/https://doi.org/10.1016/j.aip.2016.09.005
- Hammer, S. E. (1996). The effects of Guided Imagery through music on state and Trait Anxiety. Journal of Music Therapy, 33(1), 47–70. https://doi.org/https://doi.org/10.1093/jmt/33.1.47
- Hanser, S. B., Bauer-Wu, S., Kubicek, L., Healey, M., Manola, J., Hernandez, M., & Bunnell, C. (2006). Effects of a music therapy intervention on quality of life and distress in women with metastatic breast cancer. Journal of the Society for Integrative Oncology, 04((02|2)), 62–66. https://doi.org/https://doi.org/10.2310/7200.2006.003
- Hernández-Ruiz, E. (2005). Effect of music therapy on the anxiety levels and sleep patterns of abused women in shelters. Journal of Music Therapy, 42(2), 140–158. https://doi.org/https://doi.org/10.1093/jmt/42.2.140
- Horne-Thompson, A., & Grocke, D. (2008). The effect of music therapy on anxiety in patients who are terminally ill. Journal of Palliative Medicine, 11(4), 582–590. https://doi.org/https://doi.org/10.1089/jpm.2007.0193
- Kim, D. S., Park, Y. G., Choi, J. H., Im, S. H., Jung, K. J., Cha, Y. A., Jung, C. O., & Yoon, Y. H. (2011). Effects of music therapy on mood in stroke patients. Yonsei Medical Journal, 52(6), 977–981. https://doi.org/https://doi.org/10.3349/ymj.2011.52.6.977
- Mandel, S. E., Hanser, S. B., Secic, M., & Davis, B. A. (2007). Effects of music therapy on health-related outcomes in cardiac rehabilitation: A randomized controlled trial. Journal of Music Therapy, 44(3), 176–197. https://doi.org/https://doi.org/10.1093/jmt/44.3.176
- McKinney, C. H., Antoni, M. H., Kumar, M., Tims, F. C., & McCabe, P. M. (1997). Effects of Guided Imagery and music (GIM) therapy on Mood and cortisol in Healthy Adults. Health Psychology, 16(4), 390–400. https://doi.org/https://doi.org/10.1037/0278-6133.16.4.390
- Mohammadi, A. Z., Shahabi, T., & Panah, F. M. (2011). An evaluation of the effect of group music therapy on stress, anxiety, and depression levels in nursing home residents [Evaluation des effets de la musicothérapie de groupe sur les niveaux de stress, d ‘ anxiété et de dépression auprès de résidents d ‘]. Journal of Music Therapy, 1, 55–69.
- Mondanaro, J. F., Homel, P., Lonner, B., Shepp, J., Lichtensztein, M., & Loewy, J. V. (2017). Music therapy increases Comfort and Reduces pain in patients Recovering from Spine surgery. American Journal of Orthopedics (Belle Mead, N.J.), 1, 13–22.
- Morgan, K., Bartrop, R., Telfer, J., & Tennant, C. (2011). A controlled trial investigating the effect of music therapy during an acute psychotic episode. Acta Psychiatrica Scandinavica, 124(5), 363–371. https://doi.org/https://doi.org/10.1111/j.1600-0447.2011.01739.x
- Palmer, J. B., Lane, D., Mayo, D., Schluchter, M., & Leeming, R. (2015). Effects of music therapy on anesthesia requirements and anxiety in women undergoing ambulatory breast surgery for cancer diagnosis and treatment: A randomized controlled trial. Journal of Clinical Oncology, 33(28), 3162–3168. https://doi.org/https://doi.org/10.1200/JCO.2014.59.6049
- Pitts, S. E., & Silverman, M. J. (2015). Effects of verbal Processing on psychiatric patients’ Proactive Coping Skills using Recreational music therapy. Journal of Creativity in Mental Health, 10(2), 181–199. https://doi.org/https://doi.org/10.1080/15401383.2014.984097
- Raglio, A., Giovanazzi, E., Pain, D., Baiardi, P., Imbriani, C., Imbriani, M., & Mora, G. (2016). Active music therapy approach in amyotrophic lateral sclerosis: A randomized-controlled trial. International Journal of Rehabilitation Research, 39(4), 365–367. https://doi.org/https://doi.org/10.1097/MRR.0000000000000187
- Raglio, A., Zaliani, A., Baiardi, P., Bossi, D., Sguazzin, C., Capodaglio, E., Imbriani, C., Gontero, G., & Imbriani, M. (2017). Active music therapy approach for stroke patients in the post-acute rehabilitation. Neurological Sciences, 38(5), 893–897. https://doi.org/https://doi.org/10.1007/s10072-017-2827-7
- Ribeiro, M .K., Alcântara–Silva, T. R., Oliveira, J. C., Paula, T. C., Dutra, J. B., Pedrino, G. R., Simões, K., Sousa, R. B., & Rebelo, A. C. (2018). Music therapy intervention in cardiac autonomic modulation, anxiety, and depression in mothers of preterms: Randomized controlled trial. BMC Psychology, 57, 1–10. https://doi.org/https://doi.org/10.1186/s40359-018-0271-y
- Romito, F., Lagattolla, F., Costanzo, C., Giotta, F., & Mattioli, V. (2013). Music therapy and emotional expression during chemotherapy. How do breast cancer patients feel? European Journal of Integrative Medicine, 5(5), 438–442. https://doi.org/https://doi.org/10.1016/j.eujim.2013.04.001
- Rosenow, S. C., & Silverman, M. J. (2014). Effects of single session music therapy on hospitalized patients recovering from a bone marrow transplant: Two studies. Arts in Psychotherapy, 41(1), 65–70. https://doi.org/https://doi.org/10.1016/j.aip.2013.11.003
- Rossetti, A., Chadha, M., Torres, B. N., Lee, J. K., Hylton, D., Loewy, J. V., & Harrison, L. B. (2017). The impact of music therapy on Anxiety in cancer patients Undergoing Simulation for Radiation therapy. International Journal of Radiation Oncology Biology Physics, 99(1), 103–110. https://doi.org/https://doi.org/10.1016/j.ijrobp.2017.05.003
- Schmid, W., & Aldridge, D. (2004). Active music therapy in the treatment of multiple sclerosis patients: A matched control study. Journal of Music Therapy, 41(3), 225–240. https://doi.org/https://doi.org/10.1093/jmt/41.3.225
- Selle, E. W., & Silverman, M. J. (2017). A randomized feasibility study on the effects of music therapy in the form of patient-preferred live music on mood and pain in patients on a cardiovascular unit. Arts and Health, 9(3), 213–223. https://doi.org/https://doi.org/10.1080/17533015.2017.1334678
- Smith, M. (2008). The effects of a single music relaxation session on state Anxiety levels of Adults in a Workplace environment. Australian Journal of Music Therapy, 19, 45–66. https://www.austmta.org.au/journal/article/effects-single-music-relaxation-session-state-anxiety-levels-adults-workplace
- Teckenberg-Jansson, P., Turunen, S., Pölkki, T., Lauri-Haikala, M. J., Lipsanen, J., Henelius, A., Aitokallio-Tallberg, A., Pakarinen, S., Leinikka, M., & Huotilainen, M. (2019). Effects of live music therapy on heart rate variability and self-reported stress and anxiety among hospitalized pregnant women: A randomized controlled trial. Nordic Journal of Music Therapy, 28(1), 7–26. https://doi.org/https://doi.org/10.1080/08098131.2018.1546223
- Verstegen, A. L., & Silverman, M. J. (2018). Effects of music therapy on mood and pain with patients hospitalized for bone marrow transplantation: A randomized effectiveness pilot study. Journal of Creativity in Mental Health, 4, 132–139. https://doi.org/https://doi.org/10.1080/15401383.2018.1486257
- Volpe, U., Gianoglio, C., Autiero, L., Marino, M. L., Facchini, D., Mucci, A., & Galderisi, S. (2018). Acute effects of music therapy in subjects With Psychosis during Inpatient treatment. Psychiatry (New York), 3, 218–227. https://doi.org/https://doi.org/10.1080/00332747.2018.1502559
- Warth, M., Keßler, J., Bardenheuer, H. J., & Hillecke, T. K. (2015). Music therapy in palliative care. Deutsches Arzteblatt International, 46, 788–794. https://doi.org/https://doi.org/10.3238/arztebl.2015.0788
- Yates, G. J., & Silverman, M. J. (2015). Immediate effects of single-session music therapy on affective state in patients on a post-surgical oncology unit: A randomized effectiveness study. Arts in Psychotherapy, 44, 57–61. https://doi.org/https://doi.org/10.1016/j.aip.2014.11.002
Appendix 1
Table A1. Characteristics of included studies.
Appendix 2
Figure A1. Trim-and-fill plot.